Dietary Habits of Saharawi Type II Diabetic Women Living in Algerian Refugee Camps: Relationship with Nutritional Status and Glycemic Profile

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Clinical Investigation
2.3. Anthropometric Assessment
2.4. Dietary Assessment
2.5. Laboratory Evaluations
2.6. Statistical Analysis
3. Results
3.1. Socialdemographic Characteristics
3.2. Clinical History, Nutritional Status, and Metabolic Profile
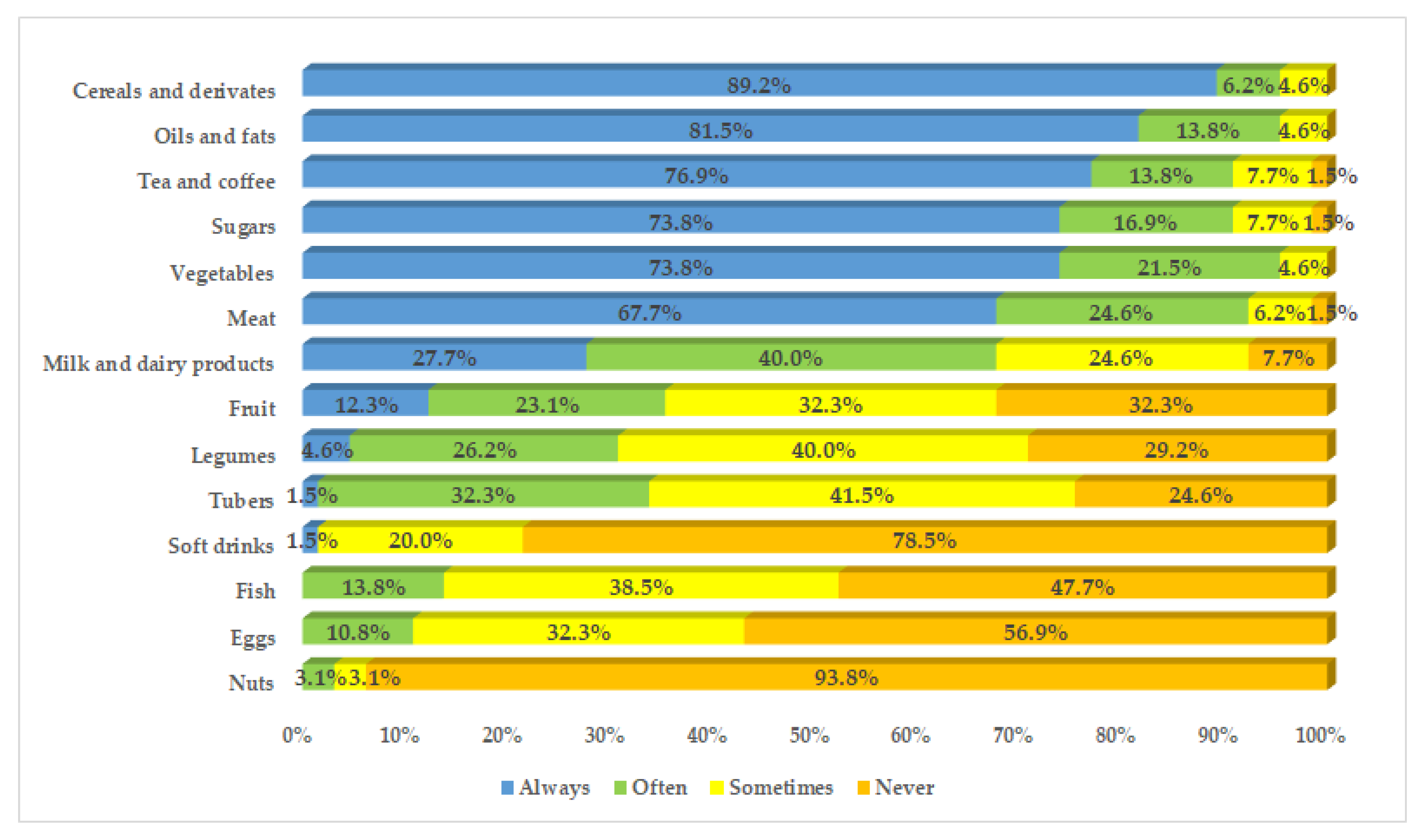
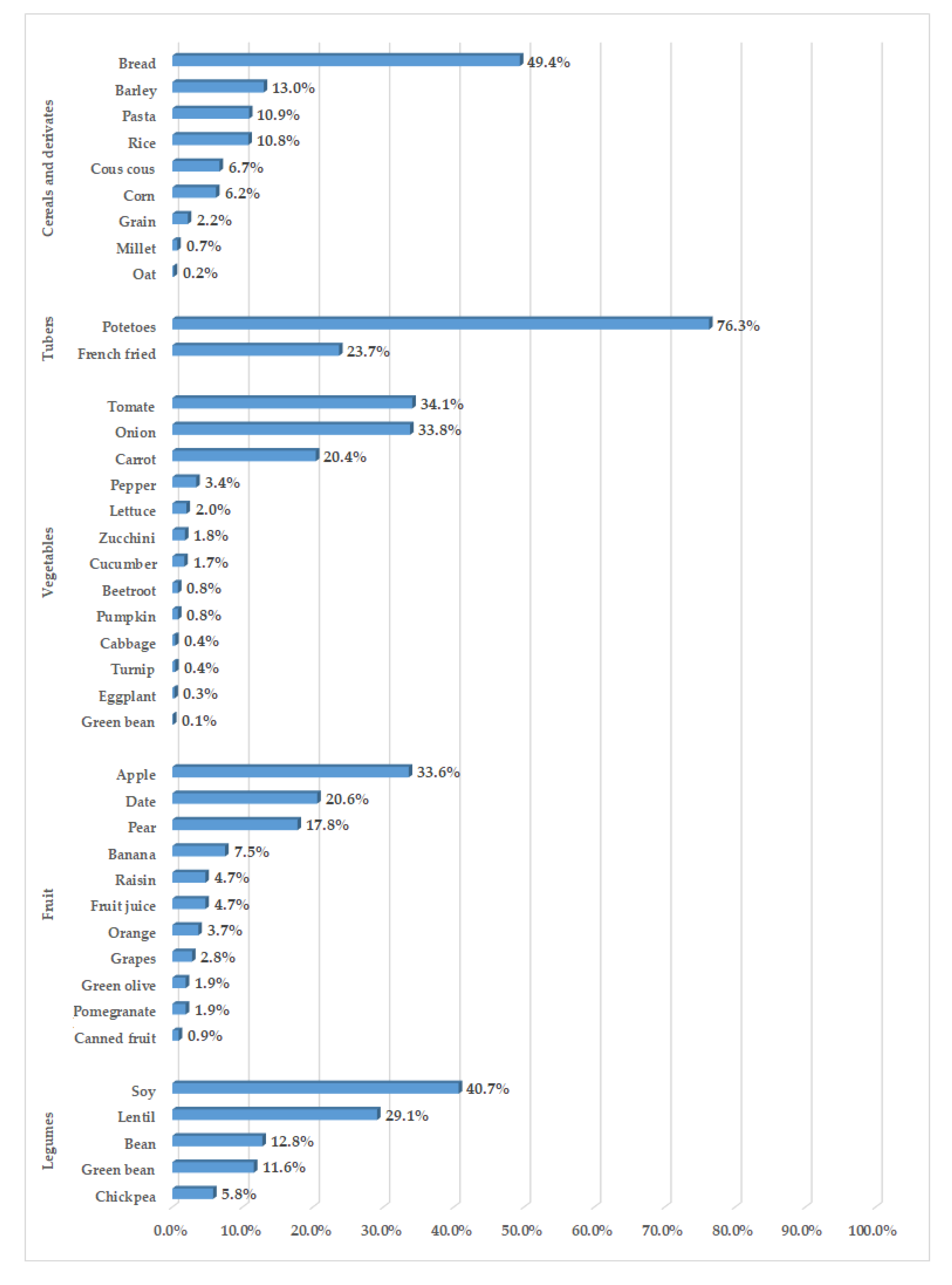
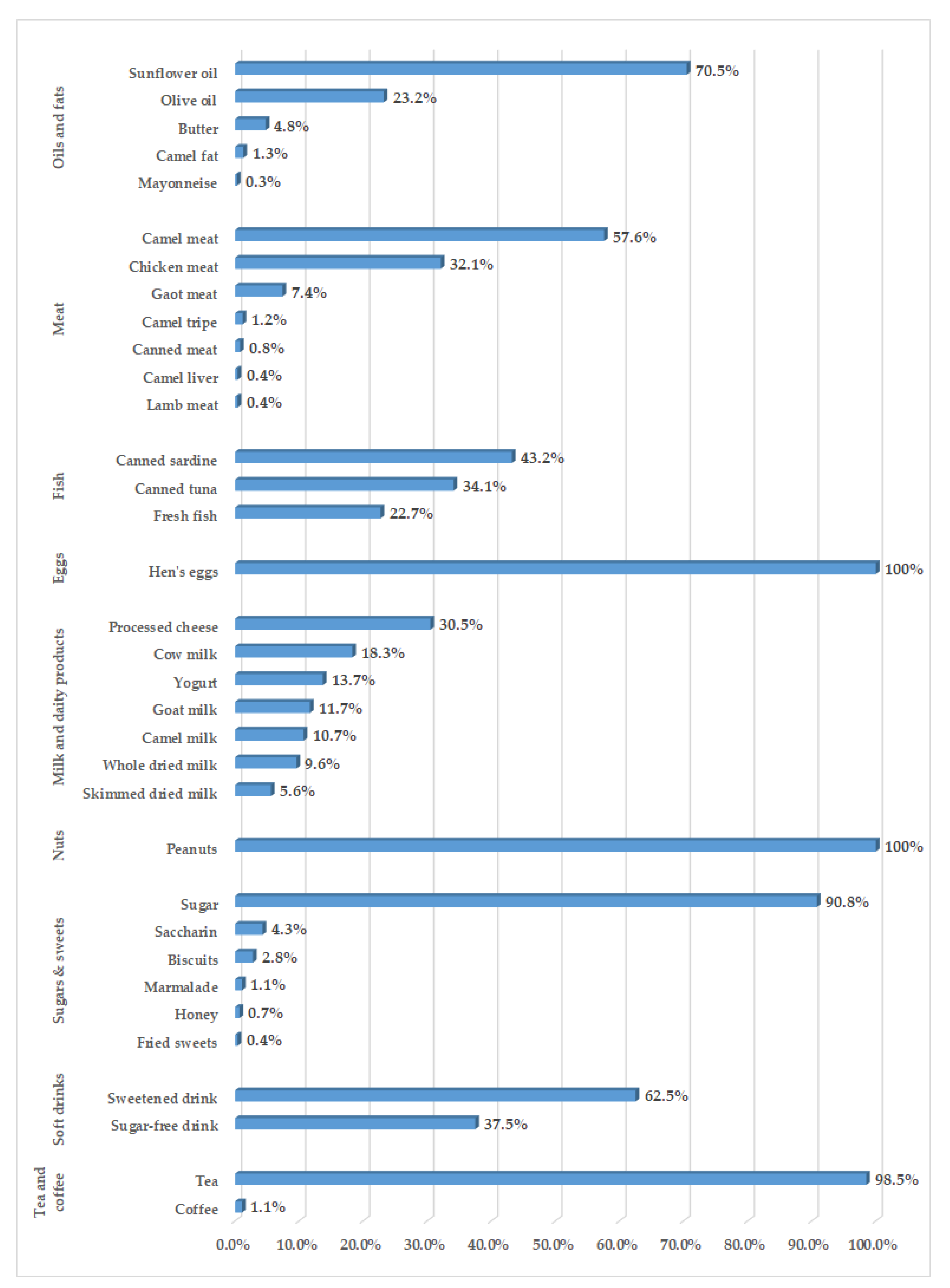
3.3. Dietary Habits
3.4. Relationship between Dietary Habits and Nutritional and Metabolic Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Misra, A.; Gopalan, H.; Jayawardena, R.; Hills, A.P.; Soares, M.; Reza-Albarrán, A.A.; Ramaiya, K.L. Diabetes in developing countries. J. Diabetes 2019, 11, 522–539. [Google Scholar] [CrossRef] [PubMed]
- Manne-Goehler, J.; Atun, R.; Stokes, A.; Goehler, A.; Houinato, D.; Houehanou, C.; Hambou, M.M.; Mbenza, B.L.; Sobngwi, E.; Balde, N.; et al. Diabetes diagnosis and care in sub-Saharan Africa: Pooled analysis of individual data from 12 countries. Lancet Diabetes Endocrinol. 2016, 4, 903–912. [Google Scholar] [CrossRef]
- Misra, A.; Sattar, N.; Tandon, N.; Shrivastava, U.; Vikram, N.K.; Khunti, K.; Hills, A.P. Clinical management of type 2 diabetes in south Asia. Lancet Diabetes Endocrinol. 2018, 6, 979–991. [Google Scholar] [CrossRef]
- MacLeod, J.; Franz, M.J.; Handu, D.; Gradwell, E.; Brown, C.; Evert, A.; Reppert, A.; Robinson, M. Academy of Nutrition and Dietetics Nutrition Practice Guideline for Type 1 and Type 2 Diabetes in Adults: Nutrition Intervention Evidence Reviews and Recommendations. J. Acad. Nutr. Diet. 2017, 117, 1637–1658. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; MacLeod, J.; Evert, A.; Brown, C.; Gradwell, E.; Handu, D.; Reppert, A.; Robinson, M. Academy of Nutrition and Dietetics Nutrition Practice Guideline for Type 1 and Type 2 Diabetes in Adults: Systematic Review of Evidence for Medical Nutrition Therapy Effectiveness and Recommendations for Integration into the Nutrition Care Process. J. Acad. Nutr. Diet. 2017, 117, 1659–1679. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Humanitarian Needs of Sahrawi Refugees in Algeria. Available online: http://reporting.unhcr.org/sites/default/files/Humanitarian%20Needs%20of%20Sahrawi%20Refugees%20in%20Algeria%202016-2017%20-%20June%202016.pdf (accessed on 13 July 2018).
- Leone, A.; Bertoli, S.; Di Lello, S.; Bassoli, A.; Ravasenghi, S.; Borgonovo, G.; Forlani, F.; Battezzati, A. Effect of Moringa oleifera Leaf Powder on Postprandial Blood Glucose Response: In Vivo Study on Saharawi People Living in Refugee Camps. Nutrients 2018, 10, 1494. [Google Scholar] [CrossRef] [Green Version]
- Morseth, M.S.; Grewal, N.K.; Kaasa, I.S.; Hatloy, A.; Barikmo, I.; Henjum, S. Dietary diversity is related to socioeconomic status among adult Saharawi refugees living in Algeria. BMC Public Health 2017, 17, 621. [Google Scholar] [CrossRef] [Green Version]
- Grijalva-Eternod, C.S.; Wells, J.C.; Cortina-Borja, M.; Salse-Ubach, N.; Tondeur, M.C.; Dolan, C.; Meziani, C.; Wilkinson, C.; Spiegel, P.; Seal, A.J. The double burden of obesity and malnutrition in a protracted emergency setting: A cross-sectional study of Western Sahara refugees. PLoS Med. 2012, 9, e1001320. [Google Scholar] [CrossRef]
- Carretero-Anibarro, E.; Hamud-Uedha, M. Prevalence of undiagnosed type 2 diabetes mellitus in the sahrawi population of the sahrawi refugee camps of Tindouf, Algeria. Med. Clin. 2019, in press. [Google Scholar] [CrossRef]
- Henjum, S.; Hjellset, V.T.; Kjollesdal, M.K.R.; Flaaten, M.; Andersen, E.; Morseth, M.S. Prevalence of Type 2 Diabetes and Associated Risk Factors Among Saharawi Refugees (P10-071-19). Curr. Dev. Nutr. 2019, 3, 10. [Google Scholar] [CrossRef] [Green Version]
- Dagenais, G.R.; Gerstein, H.C.; Zhang, X.; McQueen, M.; Lear, S.; Lopez-Jaramillo, P.; Mohan, V.; Mony, P.; Gupta, R.; Kutty, V.R.; et al. Variations in Diabetes Prevalence in Low-, Middle-, and High-Income Countries: Results From the Prospective Urban and Rural Epidemiological Study. Diabetes Care 2016, 39, 780–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th ed. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.J.T.; et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureThe JNC 7 Report. JAMA 2003, 289, 2560–2571. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.; Roche, A.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Book: Champaign, IL, USA, 1988. [Google Scholar]
- NHLBI. Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults (US). In Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998. [Google Scholar]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durnin, J.V.; Womersley, J. Body fat assessed from total body density and its estimation from skinfold thickness: Measurements on 481 men and women aged from 16 to 72 years. Br. J. Nutr. 1974, 32, 77–97. [Google Scholar] [CrossRef] [Green Version]
- Siri, W.E. Body composition from fluid spaces and density: Analysis of methods. In Techniques for Measuring Body Compositon; Brozek, J., Henschel, A., Eds.; National Academy of Sciences-National Research Council: Washington, WA, USA, 1961; pp. 223–244. [Google Scholar]
- Agodi, A.; Maugeri, A.; Kunzova, S.; Sochor, O.; Bauerova, H.; Kiacova, N.; Barchitta, M.; Vinciguerra, M. Association of Dietary Patterns with Metabolic Syndrome: Results from the Kardiovize Brno 2030 Study. Nutrients 2018, 10, 898. [Google Scholar] [CrossRef] [Green Version]
- Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Favara, G.; La Rosa, M.C.; La Mastra, C.; Quattrocchi, A.; Agodi, A. Dietary Patterns are Associated with Leukocyte LINE-1 Methylation in Women: A Cross-Sectional Study in Southern Italy. Nutrients 2019, 11, 1843. [Google Scholar] [CrossRef] [Green Version]
- Castello, A.; Lope, V.; Vioque, J.; Santamarina, C.; Pedraz-Pingarron, C.; Abad, S.; Ederra, M.; Salas-Trejo, D.; Vidal, C.; Sanchez-Contador, C.; et al. Reproducibility of data-driven dietary patterns in two groups of adult Spanish women from different studies. Br. J. Nutr. 2016, 116, 734–742. [Google Scholar] [CrossRef] [Green Version]
- Markussen, M.S.; Veierod, M.B.; Ursin, G.; Andersen, L.F. The effect of under-reporting of energy intake on dietary patterns and on the associations between dietary patterns and self-reported chronic disease in women aged 50–69 years. Br. J. Nutr. 2016, 116, 547–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naigaga, D.A.; Jahanlu, D.; Claudius, H.M.; Gjerlaug, A.K.; Barikmo, I.; Henjum, S. Body size perceptions and preferences favor overweight in adult Saharawi refugees. Nutr. J. 2018, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Rguibi, M.; Belahsen, R. Fattening practices among Moroccan Saharawi women. East. Mediterr. Health J. 2006, 12, 619–624. [Google Scholar]
- Rguibi, M.; Belahsen, R. Metabolic syndrome among Moroccan Sahraoui adult Women. Am. J. Hum. Biol. 2004, 16, 598–601. [Google Scholar] [CrossRef]
- Hao, M.; Ding, L.; Xuan, L.; Wang, T.; Li, M.; Zhao, Z.; Lu, J.; Xu, Y.; Chen, Y.; Wang, W.; et al. Urinary bisphenol A concentration and the risk of central obesity in Chinese adults: A prospective study. J. Diabetes 2018, 10, 442–448. [Google Scholar] [CrossRef]
- Ranciere, F.; Botton, J.; Slama, R.; Lacroix, M.Z.; Debrauwer, L.; Charles, M.A.; Roussel, R.; Balkau, B.; Magliano, D.J. Exposure to Bisphenol A and Bisphenol S and Incident Type 2 Diabetes: A Case-Cohort Study in the French Cohort D.E.S.I.R. Environ. Health Perspect. 2019, 127, 107013. [Google Scholar] [CrossRef] [Green Version]
- Ranciere, F.; Lyons, J.G.; Loh, V.H.; Botton, J.; Galloway, T.; Wang, T.; Shaw, J.E.; Magliano, D.J. Bisphenol A and the risk of cardiometabolic disorders: A systematic review with meta-analysis of the epidemiological evidence. Environ. Health 2015, 14, 46. [Google Scholar] [CrossRef] [Green Version]
- Geens, T.; Aerts, D.; Berthot, C.; Bourguignon, J.P.; Goeyens, L.; Lecomte, P.; Maghuin-Rogister, G.; Pironnet, A.M.; Pussemier, L.; Scippo, M.L.; et al. A review of dietary and non-dietary exposure to bisphenol-A. Food Chem. Toxicol. 2012, 50, 3725–3740. [Google Scholar] [CrossRef]
- Bertoli, S.; Leone, A.; Battezzati, A. Human Bisphenol A Exposure and the "Diabesity Phenotype". Dose-Response 2015, 13, 1559325815599173. [Google Scholar] [CrossRef] [Green Version]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Fernandez-Montero, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Bertoli, S.; Battezzati, A.; Bes-Rastrollo, M. Adherence to the Mediterranean Dietary Pattern and Incidence of Nephrolithiasis in the Seguimiento Universidad de Navarra Follow-up (SUN) Cohort. Am. J. Kidney Dis. 2017, 70, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Manley, S.E.; Stratton, I.M.; Cull, C.A.; Frighi, V.; Eeley, E.A.; Matthews, D.R.; Holman, R.R.; Turner, R.C.; Neil, H.A. Effects of three months’ diet after diagnosis of Type 2 diabetes on plasma lipids and lipoproteins (UKPDS 45). UK Prospective Diabetes Study Group. Diabet. Med. 2000, 17, 518–523. [Google Scholar] [CrossRef] [Green Version]
- Franz, M.J.; Monk, A.; Barry, B.; McClain, K.; Weaver, T.; Cooper, N.; Upham, P.; Bergenstal, R.; Mazze, R.S. Effectiveness of medical nutrition therapy provided by dietitians in the management of non-insulin-dependent diabetes mellitus: A randomized, controlled clinical trial. J. Am. Diet. Assoc. 1995, 95, 1009–1017. [Google Scholar] [CrossRef]
- Andrews, R.C.; Cooper, A.R.; Montgomery, A.A.; Norcross, A.J.; Peters, T.J.; Sharp, D.J.; Jackson, N.; Fitzsimons, K.; Bright, J.; Coulman, K.; et al. Diet or diet plus physical activity versus usual care in patients with newly diagnosed type 2 diabetes: The Early ACTID randomised controlled trial. Lancet 2011, 378, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Barikmo, I.; Henjum, S.; Dahl, L.; Oshaug, A.; Torheim, L.E. Environmental implication of iodine in water, milk and other foods used in Saharawi refugees camps in Tindouf, Algeria. J. Food Compos. Anal. 2011, 24, 637–641. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Wilaya (Province) | Daira (Town) | ||
| Smara | 44 | 67.7 | |
| Eydaria | 12 | 18.5 | |
| Bir Lehlu | 10 | 15.4 | |
| Mahbes | 11 | 16.9 | |
| Farsia | 11 | 16.9 | |
| Bojador | 21 | 32.3 | |
| 27Febrero | 10 | 15.4 | |
| Lamsid | 11 | 16.9 | |
| Education | |||
| None | 25 | 38.5 | |
| Primary level | 18 | 27.7 | |
| Secondary level | 20 | 30.8 | |
| University | 2 | 3.1 | |
| Marital status | |||
| Unmarried | 1 | 1.5 | |
| Married | 38 | 58.5 | |
| Divorced | 12 | 18.5 | |
| Widow | 14 | 21.5 | |
| Occupation | |||
| Housewife | 29 | 44.6 | |
| Retired | 4 | 6.2 | |
| Worker | 32 | 49.2 |
| P25 | P50 | P75 | |
|---|---|---|---|
| Nutritional status | |||
| BMI (kg/m2) | 25.6 | 28.7 | 31.8 |
| Waist circumference (cm) | 97.0 | 101.8 | 108.5 |
| Hip circumference (cm) | 95.8 | 101.0 | 108.5 |
| Waist-to-hip ratio | 0.9 | 1.0 | 1.1 |
| Arm circumference (cm) | 31.0 | 34.0 | 36.0 |
| Tricipital SKF (mm) | 30.0 | 34.0 | 41.0 |
| Bicipital SKF (mm) | 21.0 | 25.5 | 33.0 |
| Subscapular SKF (mm) | 32.5 | 36.0 | 41.0 |
| Suprailiac SKF (mm) | 32.0 | 36.5 | 41.0 |
| Body fat (%) | 43.7 | 45.4 | 47.3 |
| Metabolic parameters | |||
| Glucose (mg/dL) | 163 | 207 | 243 |
| Insulin (mU/mL) | 4.9 | 8.8 | 13.9 |
| HOMA | 2.4 | 4.5 | 7.1 |
| HbA1c (%) | 7.9 | 9.4 | 10.3 |
| Systolic blood pressure (mm Hg) | 120 | 135 | 145 |
| Diastolic blood pressure (mm Hg) | 75 | 80 | 89 |
| Total cholesterol (mg/dL) | 165 | 188 | 219 |
| Triglycerides (mg/dL) | 98 | 126 | 166 |
| AST (U/L) | 20 | 24 | 30 |
| ALT (U/L) | 17 | 21 | 26 |
| Hemoglobin (g/dL) | 12.7 | 14.0 | 14.6 |
| Healthy Dietary Pattern | Unhealthy Dietary Pattern | |
|---|---|---|
| Grain cereals | −0.273 | 0.110 |
| Bread, pasta, rice, couscous | 0.095 | 0.807 |
| Potatoes | −0.040 | 0.006 |
| Fried potatoes | −0.043 | −0.076 |
| Onions, tomatoes, and carrots | 0.027 | 0.798 |
| Other vegetables | 0.636 | 0.101 |
| Olive oil | 0.585 | −0.220 |
| Sunflower oil | −0.191 | 0.671 |
| Animal fats | −0.365 | 0.290 |
| Fresh fruit | 0.584 | −0.156 |
| Dried fruit | 0.205 | 0.466 |
| Red meat | −0.568 | 0.466 |
| White meat | 0.705 | 0.247 |
| Eggs | 0.480 | −0.049 |
| Low-fat milk | 0.339 | −0.190 |
| Camel’s, cow’s, and goat’s milk and dairy products | 0.518 | 0.099 |
| Legumes | 0.389 | 0.232 |
| Canned fish | 0.264 | 0.108 |
| Fresh fish | −0.088 | −0.305 |
| Sugar, sweets, and beverages | −0.132 | 0.480 |
| Explained variance (%) | 15.3 | 14.3 |
| Healthy Dietary Pattern | Unhealthy Dietary Pattern | |||||
|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | |
| Nutritional status * | ||||||
| BMI | Reference | 0.76 | 1.62 | Reference | 0.66 | −0.65 |
| [−1.95, 3.47] | [−1.18, 4.43] | [−2.09, 3.40] | [−3.45, 2.15] | |||
| WC | Reference | −0.69 | 1.00 | Reference | 4.01 | −0.47 |
| [−6.66, 5.29] | [−5.17, 7.16] | [−1.94, 9.96] | [−6.50, 5.56] | |||
| WHR | Reference | 0.00 | 0.01 | Reference | 0.03 | 0.01 |
| [−0.06, 0.05] | [−0.05, 0.07] | [−0.02, 0.09] | [−0.04, 0.07] | |||
| BF% | Reference | 0.21 | −0.28 | Reference | 1.35 | 1.90 |
| [−1.76, 2.17] | [−2.35, 1.79] | [−0.61, 3.31] | [−0.12, 3.91] | |||
| Glycemic profile † | ||||||
| HbA1c (%) | Reference | 0.39 | −0.06 | Reference | −0.36 | 0.50 |
| [−0.65, 1.42] | [−1.12, 0.99] | [−1.38, 0.66] | [−0.55, 1.55] | |||
| HOMA | Reference | −0.05 | −0.49 | Reference | −0.03 | 2.49 * |
| [−2.22, 2.11] | [−2.74, 1.76] | [−2.06, 1.99] | [0.41, 4.57] | |||
| Insulin (mU/mL) | Reference | 0.00 | −0.90 | Reference | 0.89 | 4.52 * |
| [−4.18, 4.18] | [−5.24, 3.44] | [−3.08, 4.87] | [0.44, 8.60] | |||
| Glucose (mg/dL) | Reference | 1.71 | −6.93 | Reference | −17.86 | 6.58 |
| [−37.30, 40.73] | [−46.87, 33.02] | [−56.56, 20.84] | [−33.21, 46.36] | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leone, A.; Battezzati, A.; Di Lello, S.; Ravasenghi, S.; Mohamed-Iahdih, B.; Mohamed Lamin Saleh, S.; Bertoli, S. Dietary Habits of Saharawi Type II Diabetic Women Living in Algerian Refugee Camps: Relationship with Nutritional Status and Glycemic Profile. Nutrients 2020, 12, 568. https://doi.org/10.3390/nu12020568
Leone A, Battezzati A, Di Lello S, Ravasenghi S, Mohamed-Iahdih B, Mohamed Lamin Saleh S, Bertoli S. Dietary Habits of Saharawi Type II Diabetic Women Living in Algerian Refugee Camps: Relationship with Nutritional Status and Glycemic Profile. Nutrients. 2020; 12(2):568. https://doi.org/10.3390/nu12020568
Chicago/Turabian StyleLeone, Alessandro, Alberto Battezzati, Sara Di Lello, Stefano Ravasenghi, Babahmed Mohamed-Iahdih, Saleh Mohamed Lamin Saleh, and Simona Bertoli. 2020. "Dietary Habits of Saharawi Type II Diabetic Women Living in Algerian Refugee Camps: Relationship with Nutritional Status and Glycemic Profile" Nutrients 12, no. 2: 568. https://doi.org/10.3390/nu12020568