A Single Dose of Beetroot Juice Does Not Change Blood Pressure Response Mediated by Acute Aerobic Exercise in Hypertensive Postmenopausal Women

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
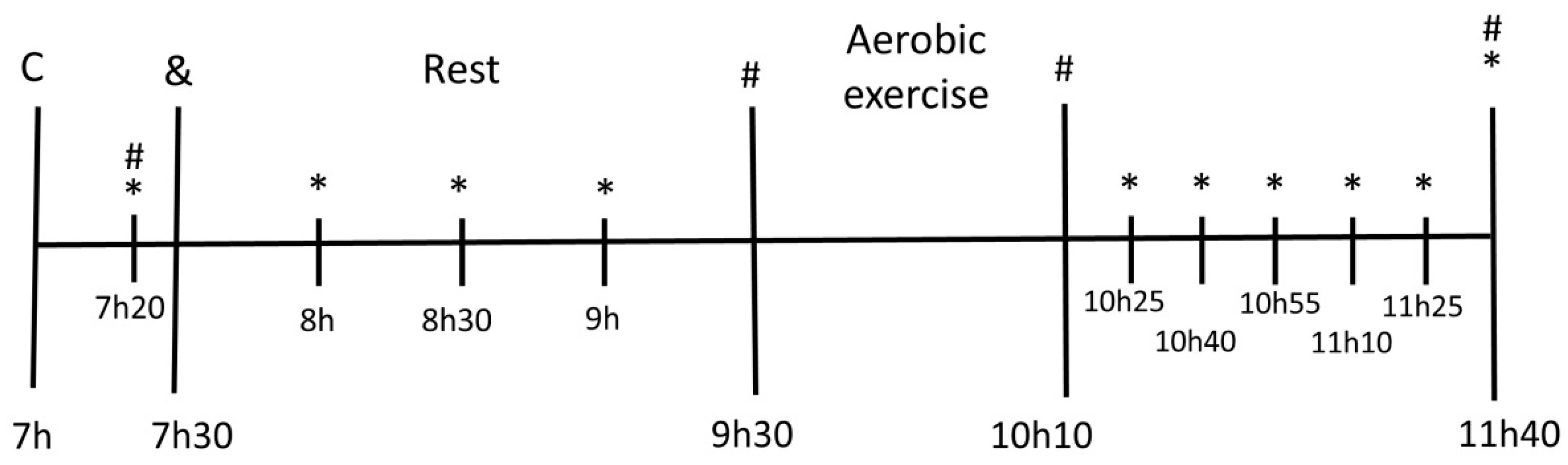
2.2. Study Design
2.3. Physical Exercise
2.4. Intake of Beetroot Juice and Placebo
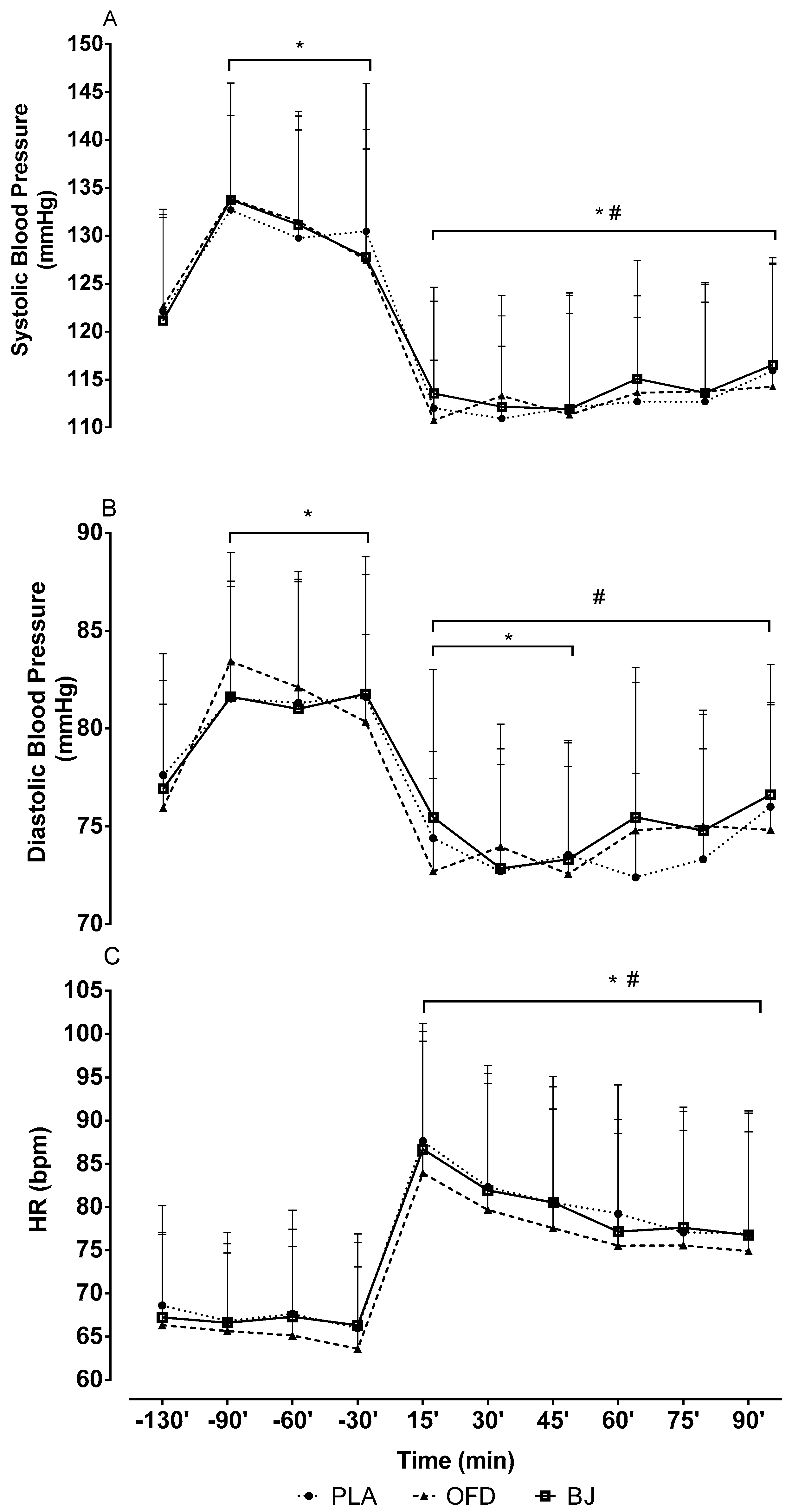
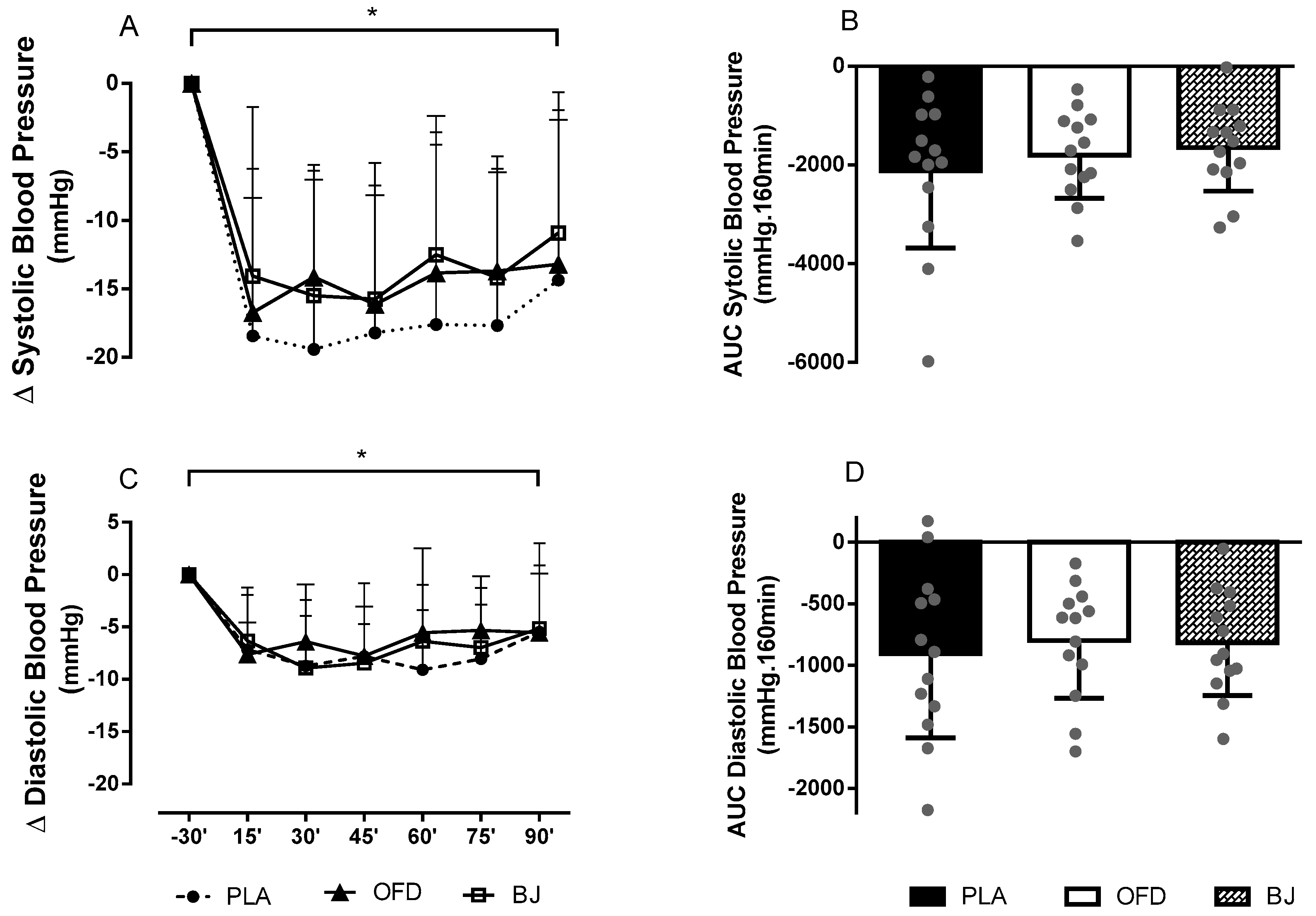
2.5. Measurements of Blood Pressure
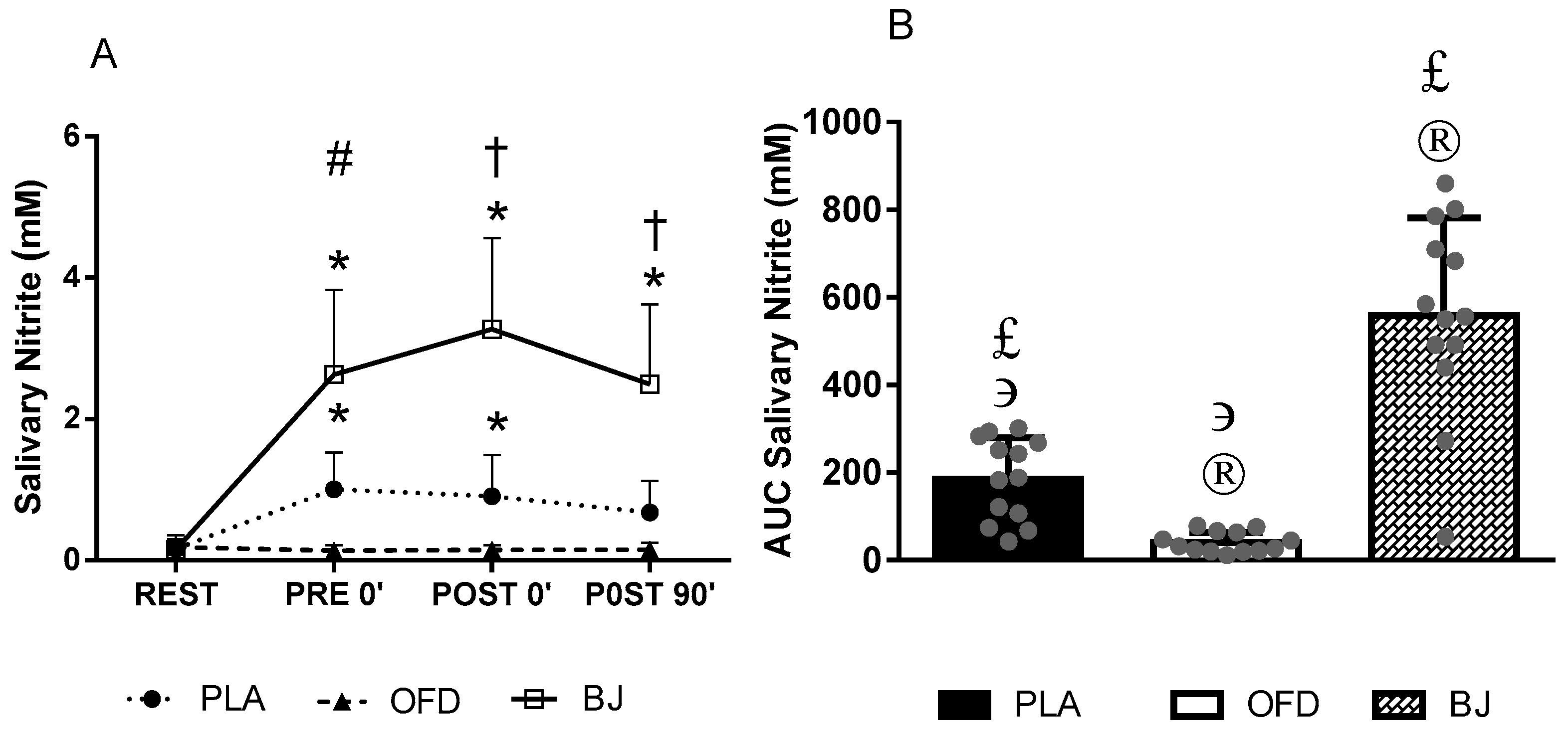
2.6. Salivary Samples Collection and Analysis
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lagranha, C.J.; Silva, T.L.A.; Silva, S.C.A.; Braz, G.R.F.; da Silva, A.I.; Fernandes, M.P.; Sellitti, D.F. Protective effects of estrogen against cardiovascular disease mediated via oxidative stress in the brain. Life Sci. 2018, 192, 190–198. [Google Scholar] [CrossRef]
- Coylewright, M.; Reckelhoff, J.F.; Ouyang, P. Menopause and Hypertension An Age-Old Debate. Hypertension 2008, 51, 952–959. [Google Scholar] [CrossRef]
- Malachias, M.; Souza, W.; Plavnik, F.; Rodrigues, C.; Brandão, A.; Neves, M.; Bortolotto, L.; Franco, R.; Poli-de-Figueiredo, C.; Jardim, P.; et al. 7a Diretriz Brasileira De Hipertensão Arterial. In Arquivos Brasileiros de Cardiologia; 2016; Volume 107, ISBN 1435-232X (Electronic)r1434-5161 (Linking). Available online: http://publicacoes.cardiol.br/2014/diretrizes/2016/05_HIPERTENSAO_ARTERIAL.pdf (accessed on 3 November 2018).
- Halliwill, J.R.; Buck, T.M.; Lacewell, A.N.; Romero, S.A. Postexercise hypotension and sustained postexercise vasodilatation: What happens after we exercise? Exp. Physiol. 2013, 98, 7–18. [Google Scholar] [CrossRef]
- Farah, C.; Nascimento, A.; Bolea, G.; Meyer, G.; Gayrard, S.; Lacampagne, A.; Cazorla, O.; Reboul, C. Key role of endothelium in the eNOS-dependent cardioprotection with exercise training. J. Mol. Cell. Cardiol. 2017, 102, 26–30. [Google Scholar] [CrossRef]
- Ocampo, D.A.B.; Paipilla, A.F.; Marín, E.; Vargas-Molina, S.; Petro, J.L.; Pérez-Idárraga, A. Dietary Nitrate from Beetroot Juice for Hypertension: A Systematic Review. Biomolecules 2018, 8, 134. [Google Scholar] [CrossRef]
- Eggebeen, J.; Kim-Shapiro, D.B.; Haykowsky, M.; Morgan, T.M.; Basu, S.; Brubaker, P.; Rejeski, J.; Kitzman, D.W. One Week of Daily Dosing With Beetroot Juice Improves Submaximal Endurance and Blood Pressure in Older Patients With Heart Failure and Preserved Ejection Fraction. JACC Heart Fail. 2016, 4, 428–437. [Google Scholar] [CrossRef]
- Kenjale, A.A.; Ham, K.L.; Stabler, T.; Robbins, J.L.; Johnson, J.L.; VanBruggen, M.; Privette, G.; Yim, E.; Kraus, W.E.; Allen, J.D. Dietary nitrate supplementation enhances exercise performance in peripheral arterial disease. J. Appl. Physiol. 2011, 110, 1582–1591. [Google Scholar] [CrossRef]
- Kelly, J.; Fulford, J.; Vanhatalo, A.; Blackwell, J.R.; French, O.; Bailey, S.J.; Gilchrist, M.; Winyard, P.G.; Jones, A.M. Effects of short-term dietary nitrate supplementation on blood pressure, O2 uptake kinetics, and muscle and cognitive function in older adults. AJP Regul. Integr. Comp. Physiol. 2013, 304, R73–R83. [Google Scholar] [CrossRef]
- Bock, J.M.; Treichler, D.P.; Norton, S.L.; Ueda, K.; William, E.; Casey, D.P. Inorganic nitrate supplementation enhances functional capacity and lower-limb microvascular reactivity in patients with peripheral artery disease. Nitric Oxide 2018, 80, 45–51. [Google Scholar] [CrossRef]
- Siervo, M.; Oggioni, C.; Mathers, J.C.; Celis-Morales, C.; Ashor, A.W.; Jakovljevic, D.G.; Trenell, M.; Houghton, D.; Trenell, M.; Mathers, J.C.; et al. Dietary nitrate does not affect physical activity or outcomes in healthy older adults in a randomized, cross-over trial. Nutr. Res. 2016, 36, 1361–1369. [Google Scholar] [CrossRef] [Green Version]
- Woessner, M.; VanBruggen, M.D.; Pieper, C.F.; Sloane, R.; Kraus, W.E.; Gow, A.J.; Allen, J.D. Beet the Best? Circ. Res. 2018, 123, 654–659. [Google Scholar] [CrossRef]
- Bahadoran, Z.; Mirmiran, P.; Kabir, A.; Azizi, F.; Ghasemi, A. The Nitrate-Independent Blood Pressure-Lowering Effect of Beetroot Juice: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 830–838. [Google Scholar] [CrossRef]
- Jackson, J.K.; Patterson, A.J.; Macdonald-wicks, L.K.; Oldmeadow, C.; Mcevoy, M.A. The role of inorganic nitrate and nitrite in cardiovascular disease risk factors: A systematic review and meta-analysis of human evidence. Nutr. Rev. 2018, 76, 348–371. [Google Scholar] [CrossRef]
- Stanaway, L.; Rutherfurd-Markwick, K.; Page, R.; Ali, A. Performance and health benefits of dietary nitrate supplementation in older adults: A systematic review. Nutrients 2017, 9, 1171. [Google Scholar] [CrossRef]
- Curtis, K.J.; O’Brien, A.K.; Tanner, R.J.; Polkey, J.I.; Minnion, M.; Feelisch, M.; Polkey, M.I.; Edwards, M.; Hopkinson, N.S. Acute dietary nitrate supplementation and exercise performance in COPD: A double-blind, placebo-controlled, randomised controlled pilot study. PLoS ONE 2015, 10, e0144504. [Google Scholar] [CrossRef]
- Lansley, K.E.; Winyard, P.G.; Bailey, S.J.; Vanhatalo, A.; Wilkerson, D.P.; Blackwell, J.R.; Gilchrist, M.; Benjamin, N.; Jones, A.M. Acute dietary nitrate supplementation improves cycling time trial performance. Med. Sci. Sports Exerc. 2011, 43, 1125–1131. [Google Scholar] [CrossRef]
- Thompson, C.; Vanhatalo, A.; Jell, H.; Fulford, J.; Carter, J.; Nyman, L.; Bailey, S.J.; Jones, A.M. Dietary nitrate supplementation improves sprint and high-intensity intermittent running performance. Nitric Oxide 2016, 61, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Clifford, T.; Berntzen, B.; Davison, G.W.; West, D.J.; Howatson, G.; Stevenson, E.J. Effects of beetroot juice on recovery of muscle function and performance between bouts of repeated sprint exercise. Nutrients 2016, 8, 506. [Google Scholar] [CrossRef]
- Coggan, A.R.; Leibowitz, J.L.; Spearie, C.A.; Kadkhodayan, A.; Thomas, D.P.; Ramamurthy, S.; Mahmood, K.; Park, S.; Waller, S.; Farmer, M.; et al. Acute Dietary Nitrate Intake Improves Muscle Contractile Function in Patients with Heart Failure: A Double-Blind, Placebo-Controlled, Randomized Trial. Circ. Heart Fail. 2015, 8, 914–920. [Google Scholar] [CrossRef]
- Barbosa, C.D.; Costa, J.G.; Giolo, J.S.; Rossato, L.T.; Nahas, P.C.; Mariano, I.M.; Batista, J.P.; Puga, G.M.; de Oliveira, E.P. Isoflavone supplementation plus combined aerobic and resistance exercise do not change phase angle values in postmenopausal women: A randomized placebo-controlled clinical trial. Exp. Gerontol. 2019, 117, 31–37. [Google Scholar] [CrossRef]
- Karvonen, M.J.; Kentala, E.; Mustala, O. The effects of training on heart rate; a longitudinal study. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- De Castro, T.F.; Manoel, F.D.A.; Figueiredo, D.H.; Figueiredo, D.H.; Machado, F.A. Effect of beetroot juice supplementation on 10-km performance in recreational runners. Appl. Physiol. Nutr. Metab. 2018, 44, 90–94. [Google Scholar] [CrossRef]
- Bondonno, C.P.; Liu, A.H.; Croft, K.D.; Ward, N.C.; Shinde, S.; Moodley, Y.; Lundberg, J.O.; Puddey, I.B.; Woodman, R.J.; Hodgson, J.M. Absence of an effect of high nitrate intake from beetroot juice on blood pressure in treated hypertensive individuals: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 368–375. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for Collecting Saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Kurose, I.; Wolf, R.; Grisham, M.B.; Granger, D.N. Effects of an endogenous inhibitor of nitric oxide synthesis on postcapillary venules. Am. J. Physiol. 1995, 268, H2224–H2231. [Google Scholar] [CrossRef]
- Vanhatalo, A.; Bailey, S.J.S.; Blackwell, J.R.J.; DiMenna, F.J.F.; Pavey, T.G.; Wilkerson, D.P.; Benjamin, N.; Winyard, P.G.P.; Jones, A.M. Acute and chronic effects of dietary nitrate supplementation on blood pressure and the physiological responses to moderate-intensity and incremental exercise. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 299, R1121–R1131. [Google Scholar] [CrossRef] [Green Version]
- Betteridge, S.; Bescós, R.; Martorell, M.; Pons, A.; Garnham, A.P.; Stathis, C.C.; McConell, G.K. No effect of acute beetroot juice ingestion on oxygen consumption, glucose kinetics, or skeletal muscle metabolism during submaximal exercise in males. J. Appl. Physiol. 2016, 120, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-K.; Moore, D.J.; Maurer, D.G.; Kim-Shapiro, D.B.; Basu, S.; Flanagan, M.P.; Skulas-Ray, A.C.; Kris-Etherton, P.; Proctor, D.N. Acute dietary nitrate supplementation does not augment submaximal forearm exercise hyperemia in healthy young men. Appl. Physiol. Nutr. Metab. 2015, 40, 122–128. [Google Scholar] [CrossRef]
- Bond, V., Jr.; Curry, B.H.; Adams, R.G.; Haddad, G.E. Cardiorespiratory function associated with dietary nitrate supplementation. Appl. Physiol. Nutr. Metab. 2014, 39, 168–172. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos Baião, D.; Conte-Junior, C.A.; Paschoalin, V.M.F.; Alvares, T.S. Beetroot juice increase nitric oxide metabolites in both men and women regardless of body mass. Int. J. Food Sci. Nutr. 2016, 67, 40–46. [Google Scholar] [CrossRef]
- Berry, M.J.; Justus, N.W.; Hauser, J.I.; Case, A.H.; Helms, C.C.; Basu, S.; Rogers, Z.; Lewis, M.T.; Miller, G.D. Dietary nitrate supplementation improves exercise performance and decreases blood pressure in COPD patients. Nitric Oxide-Biol. Chem. 2015, 48, 22–30. [Google Scholar] [CrossRef]
- Hohensinn, B.; Haselgrübler, R.; Müller, U.; Stadlbauer, V.; Lanzerstorfer, P.; Lirk, G.; Höglinger, O.; Weghuber, J. Sustaining elevated levels of nitrite in the oral cavity through consumption of nitrate-rich beetroot juice in young healthy adults reduces salivary pH. Nitric Oxide-Biol. Chem. 2016, 60, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Siervo, M.; Lara, J.; Jajja, A.; Sutyarjoko, A.; Ashor, A.W.; Brandt, K.; Qadir, O.; Mathers, J.C.; Benjamin, N.; Winyard, P.G.; et al. Ageing modifies the effects of beetroot juice supplementation on 24-h blood pressure variability: An individual participant meta-analysis. Nitric Oxide-Biol. Chem. 2015, 47, 97–105. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Smart, N.A. Exercise Training for Blood Pressure: A Systematic Review and Meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef]
- Wylie, L.J.; Kelly, J.; Bailey, S.J.; Blackwell, J.R.; Skiba, P.F.; Winyard, P.G.; Jeukendrup, A.E.; Vanhatalo, A.; Jones, A.M. Beetroot juice and exercise: Pharmacodynamic and dose-response relationships. J. Appl. Physiol. 2013, 115, 325–336. [Google Scholar] [CrossRef]
- Quillon, A.; Fromy, B.; Debret, R. Endothelium microenvironment sensing leading to nitric oxide mediated vasodilation: A review of nervous and biomechanical signals. Nitric Oxide-Biol. Chem. 2015, 45, 20–26. [Google Scholar] [CrossRef]
- Gomes Anunciação, P.; Doederlein Polito, M. A review on post-exercise hypotension in hypertensive individuals. Arq. Bras. Cardiol. 2011, 96, 100–109. [Google Scholar]
- Reboussin, D.M.; Allen, N.B.; Griswold, M.E.; Guallar, E.; Hong, Y.; Lackland, D.T.; Miller, E.P.R.; Polonsky, T.; Thompson-Paul, A.M.; Vupputuri, S. Systematic Review for the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association. J. Am. Coll. Cardiol. 2018, 71, 2176–2198. [Google Scholar] [CrossRef]
- Jarrete, A.P.; Novais, I.P.; Nunes, H.A.; Puga, G.M.; Delbin, M.A.; Zanesco, A. Influence of aerobic exercise training on cardiovascular and endocrine-inflammatory biomarkers in hypertensive postmenopausal women. J. Clin. Transl. Endocrinol. 2014, 1, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Korsager Larsen, M.; Matchkov, V.V. Hypertension and physical exercise: The role of oxidative stress. Medicina 2016, 52, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Clifford, T.; Howatson, G.; West, D.J.; Stevenson, E.J. The potential benefits of red beetroot supplementation in health and disease. Nutrients 2015, 7, 2801–2822. [Google Scholar] [CrossRef] [PubMed]
- Bedale, W.; Sindelar, J.J.; Milkowski, A.L. Dietary nitrate and nitrite: Benefits, risks, and evolving perceptions. Meat Sci. 2016, 120, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Bondonno, N.P.; Liu, A.H.; Ward, N.C.; Prince, R.L.; Lewis, J.R. Nitrate, the oral microbiome, and cardiovascular health: A systematic literature review of human and animal studies. Am. J. Clin. Nutr. 2018, 107, 504–522. [Google Scholar] [CrossRef] [PubMed]
- Bondonno, C.P.; Liu, A.H.; Croft, K.D.; Considine, M.J.; Puddey, I.B.; Woodman, R.J.; Hodgson, J.M. Antibacterial Mouthwash Blunts Oral Nitrate Reduction and Increases Blood Pressure in Treated Hypertensive Men and Women. Am. J. Hypertens. 2015, 28, 572–575. [Google Scholar] [CrossRef] [PubMed]
- Duncan, C.; Dougall, H.; Ohnston, P.; Green, S.; Brogan, R.; Leifer, C.; Smith, L.; Gowen, M.; Benjamin, N. Chemical generation of nitric oxide in the mouth from the enterosalivary circulation of dietary nitrate. Nat. Med. 1995, 1, 546. [Google Scholar] [CrossRef] [PubMed]
- Kim-Shapiro, D.B.; Gladwin, M.T. Mechanisms of Nitrite Bioactivation. Nitric Oxide 2014, 38, 58–68. [Google Scholar] [CrossRef]
- Förstermann, U. Nitric oxide and oxidative stress in vascular disease. Eur. J. Physiol. 2010, 459, 923–939. [Google Scholar] [CrossRef]
- Naci, H.; Salcher-konrad, M.; Dias, S.; Blum, M.R.; Sahoo, S.A.; Nunan, D.; Ioannidis, J.P.A. How does exercise treatment compare with antihypertensive medications ? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Brith J. Sprots Med. 2018, 1–12. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Characteristics | (Mean ± SD) |
| Age (years) | 58.1 ± 4.6 |
| Body mass (kg) | 69.9 ± 9.2 |
| Height (m) | 1.57 ± 0.05 |
| BMI (kg/m²) | 27.4 ± 4.2 |
| Waist circumference (cm) | 92.9 ± 11.7 |
| Body fat (%) | 37.3 ± 6.2 |
| Fat mass (kg) | 26.1 ± 6.9 |
| Lean mass (kg) | 29.9 ± 9.2 |
| Physical activity level | (n (%)) |
| Very Active | 2 (15%) |
| Active | 8 (62%) |
| Irregularly Active | 3 (23%) |
| Drugs | (n (%)) |
| Angiotensin 1 Receptor Blockers + Diuretic | 6 (46%) |
| Angiotensin 1 Receptor Blockers | 4 (31%) |
| Diuretic | 1 (8%) |
| Angiotensin Converting Enzyme Inhibitor | 1 (8%) |
| Angiotensin Converting Enzyme Inhibitor + Diuretic | 1 (8%) |
| Statins | 3 (23%) |
| Levothyroxine | 4 (31%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amaral, A.L.; Mariano, I.M.; Carrijo, V.H.V.; de Souza, T.C.F.; Batista, J.P.; Mendonça, A.M.; de Souza, A.V.; Caixeta, D.C.; Teixeira, R.R.; Espindola, F.S.; et al. A Single Dose of Beetroot Juice Does Not Change Blood Pressure Response Mediated by Acute Aerobic Exercise in Hypertensive Postmenopausal Women. Nutrients 2019, 11, 1327. https://doi.org/10.3390/nu11061327
Amaral AL, Mariano IM, Carrijo VHV, de Souza TCF, Batista JP, Mendonça AM, de Souza AV, Caixeta DC, Teixeira RR, Espindola FS, et al. A Single Dose of Beetroot Juice Does Not Change Blood Pressure Response Mediated by Acute Aerobic Exercise in Hypertensive Postmenopausal Women. Nutrients. 2019; 11(6):1327. https://doi.org/10.3390/nu11061327
Chicago/Turabian StyleAmaral, Ana Luiza, Igor M. Mariano, Victor Hugo V. Carrijo, Tállita Cristina F. de Souza, Jaqueline P. Batista, Anne M. Mendonça, Adriele V. de Souza, Douglas C. Caixeta, Renata R. Teixeira, Foued S. Espindola, and et al. 2019. "A Single Dose of Beetroot Juice Does Not Change Blood Pressure Response Mediated by Acute Aerobic Exercise in Hypertensive Postmenopausal Women" Nutrients 11, no. 6: 1327. https://doi.org/10.3390/nu11061327