The Influence of Electron Beam Sterilization on In Vivo Degradation of β-TCP/PCL of Different Composite Ratios for Bone Tissue Engineering


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Fabrication
2.1.1. Pre-E-Beam Surface Treatment
2.1.2. E-Beam Specification
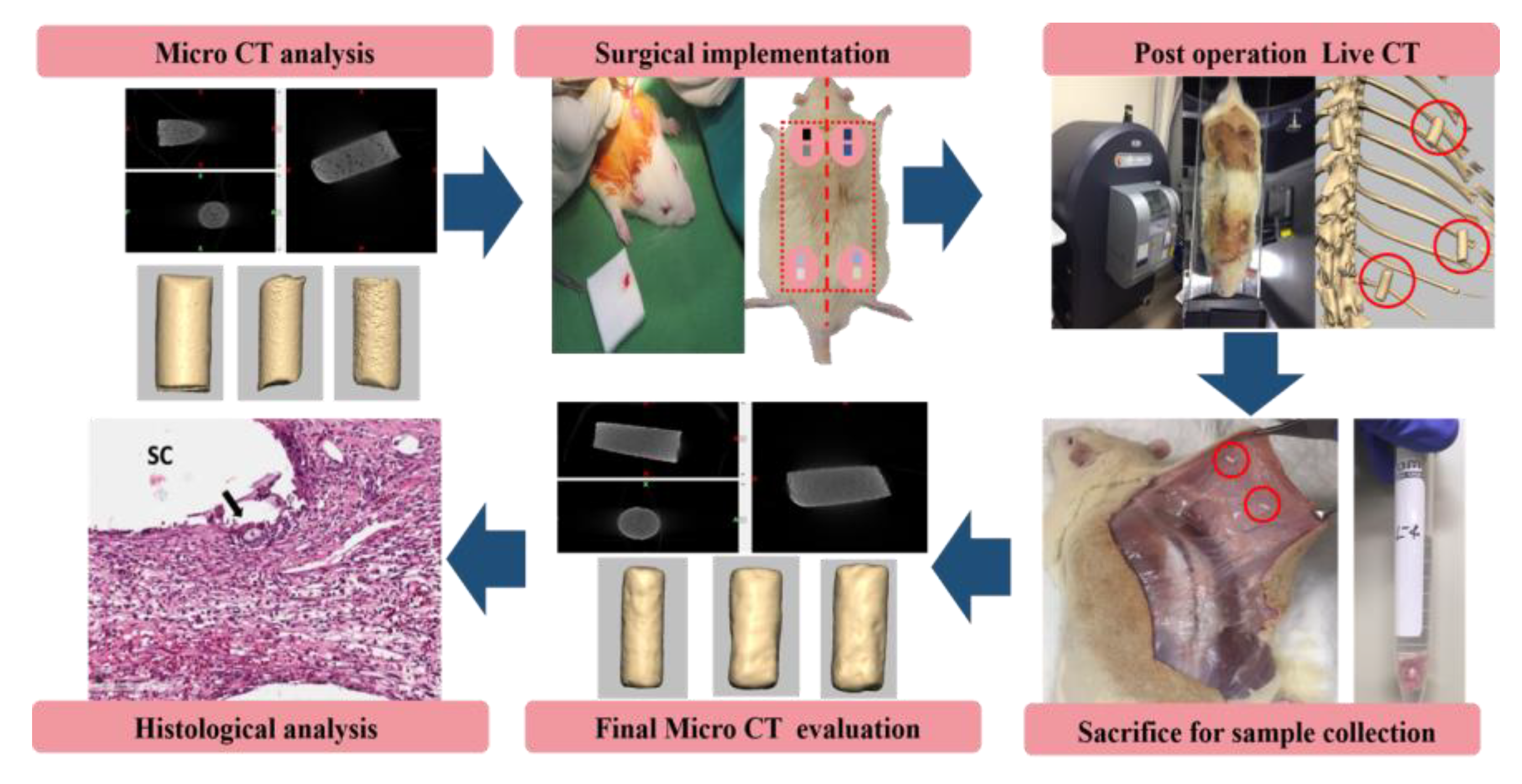
2.2. The Subcutaneous Implantation of Samples into Rats
2.3. Micro-CT and In Vivo Live-CT
2.4. Histological Examination
2.5. Statistics
3. Results and Discussion
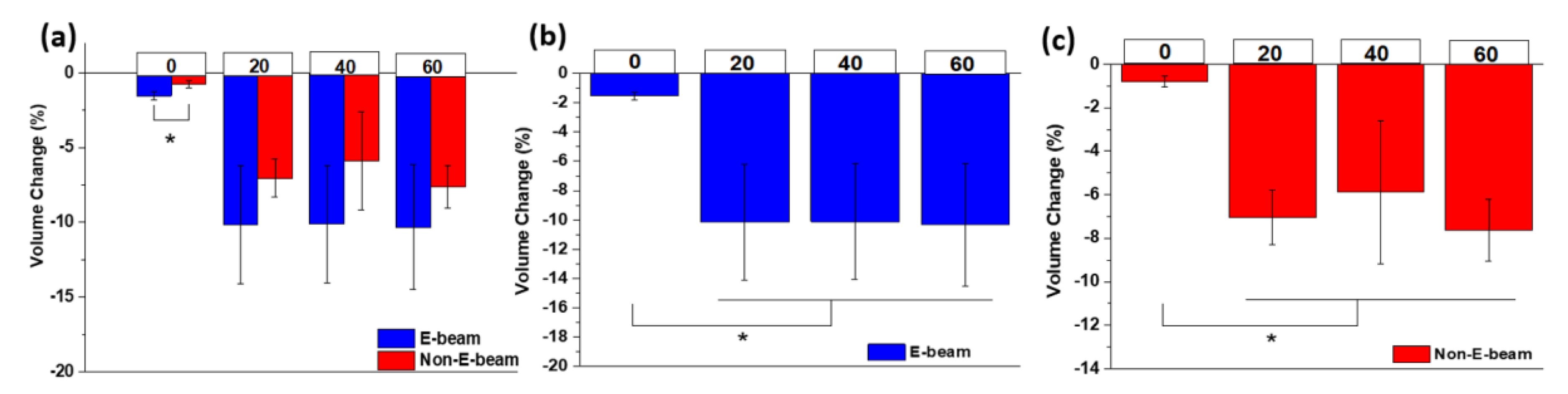
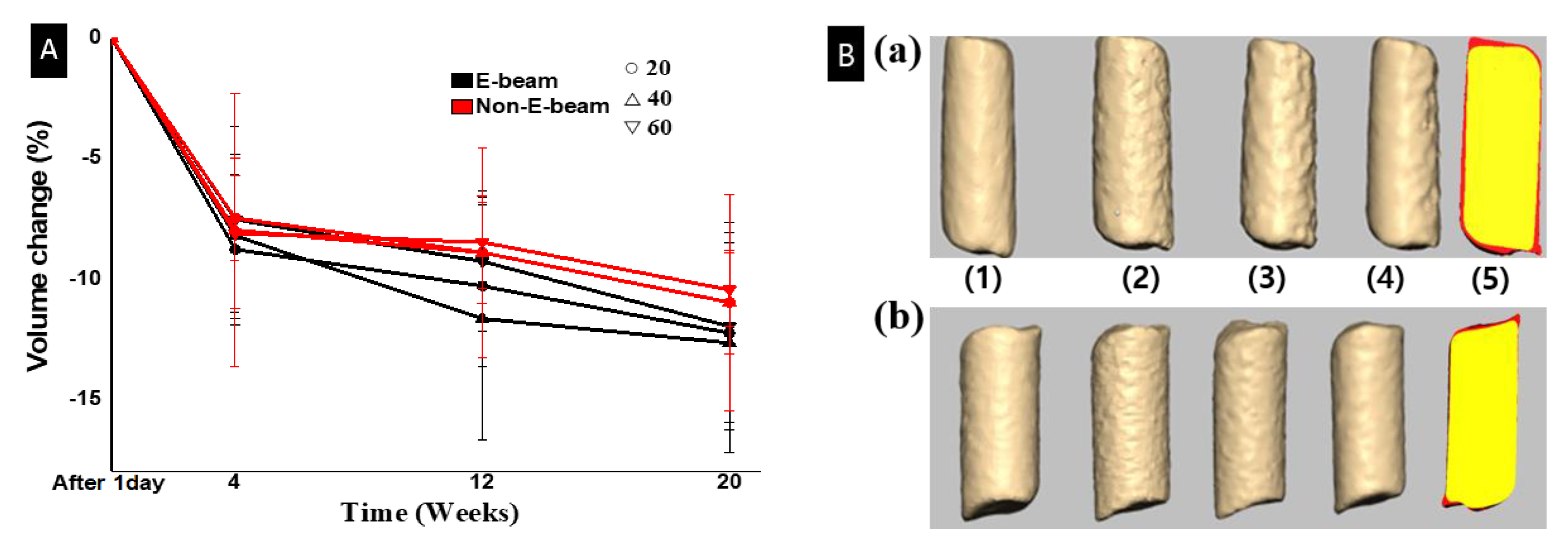
3.1. Evaluation of Filament Degradation in the Subcutaneous
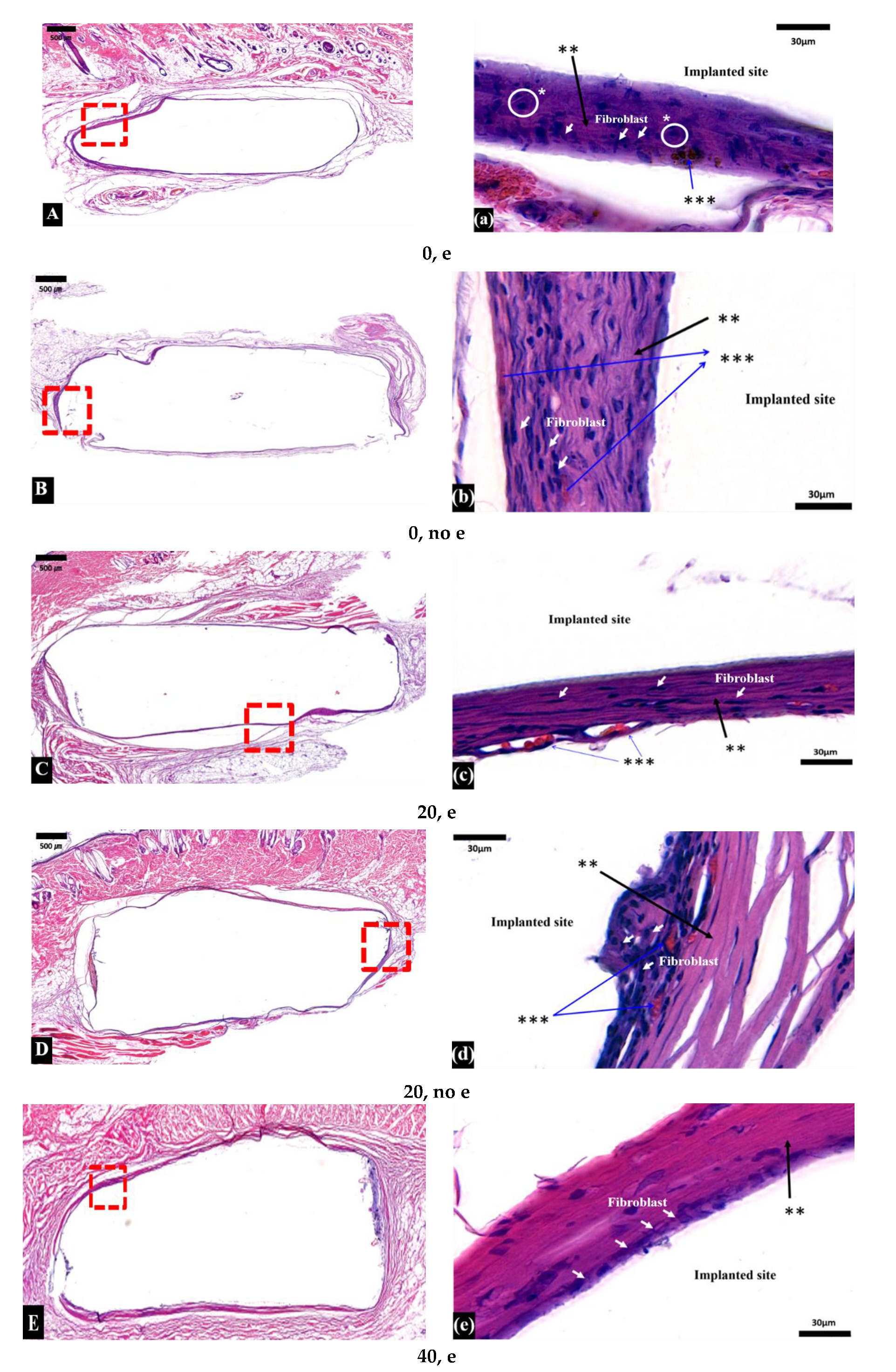
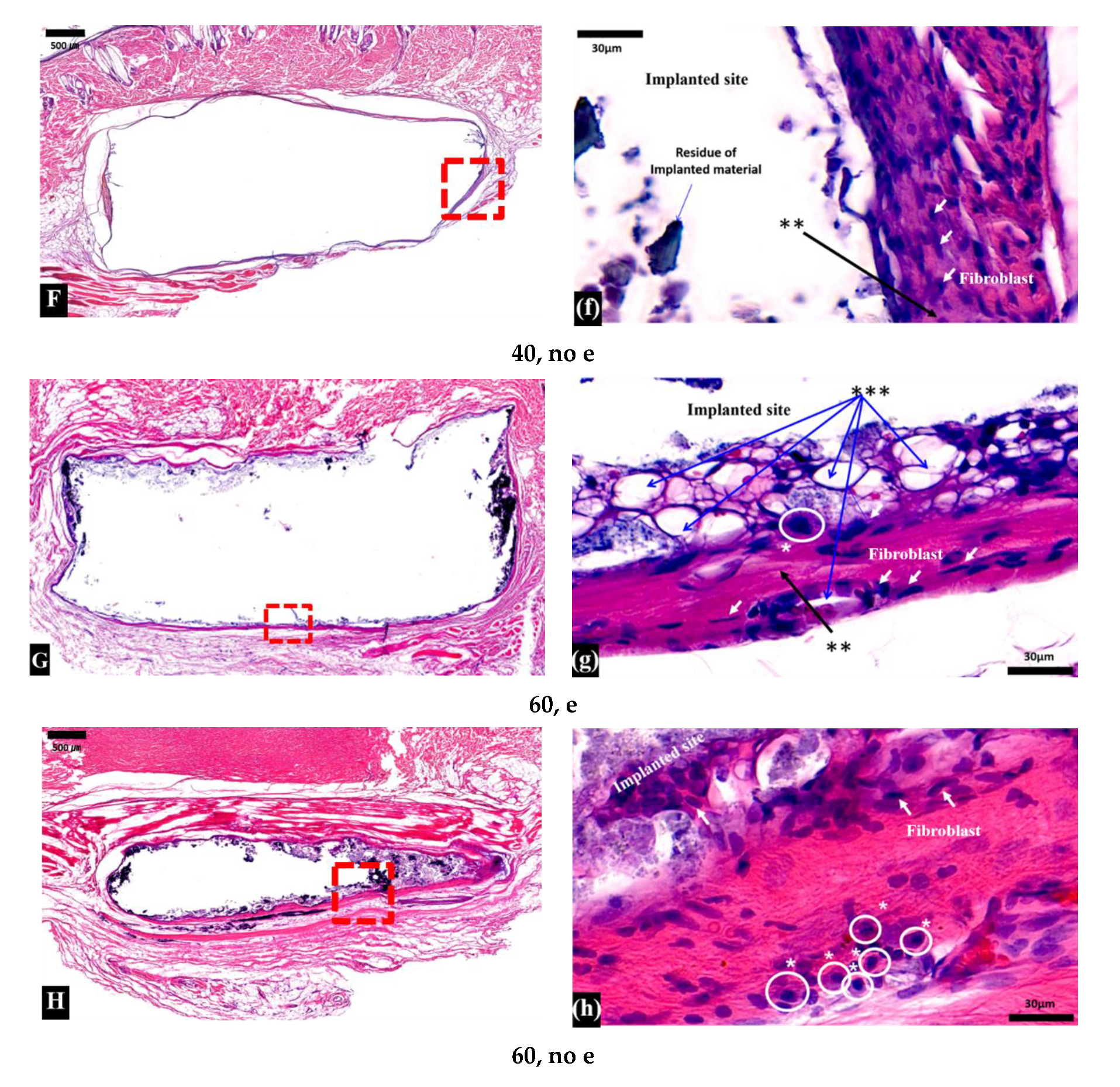
3.2. Histological Examination
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lichte, P.; Pape, H.C.; Pufe, T.; Kobbe, P.; Fischer, H. Scaffolds for bone healing: Concepts, materials and evidence. Injury 2011, 42, 569–573. [Google Scholar] [CrossRef]
- Stevens, B.; Yang, Y.; Mohandas, A.; Stucker, B.; Nguyen, T.K. A review of materials, fabrication methods, and strategies used to enhance bone regeneration in engineered bone tissues. J. Biomed. Mater. Res. Part B 2011, 85, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Mercado-Pagán, Á.E.; Stahl, A.; Shanjani, Y.; Yang, Y. Vascularization in bone tissue engineering constructs. Ann. Biomed. Eng. 2015, 43, 718–729. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Kang, Y.; Sen, M.; Park, S. Bioceramics in Tissue Engineering. In Biomaterials for Tissue Engineering Applications; Burdick, J., Mauck, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Hutmacher, D.W. Scaffolds in tissue engineering bone and cartilage. Biomaterials 2000, 24, 2529–2543. [Google Scholar] [CrossRef]
- Zhao, P.; Gu, H.; Mi, H.; Rao, C.; Fu, J.; Turing, L. Fabrication of scaffolds in tissue engineering: A review. Mech. Eng. 2018, 13, 107–119. [Google Scholar] [CrossRef]
- Winkler, T.; Sass, F.A.; Duda, G.N.; Schmidt-Bleek, K. A review of biomaterials in bone defect healing, remaining shortcomings and future opportunities for bone tissue engineering. Bone Joint Res. 2018, 7, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone substitutes: An update. Injury 2005, 36, S20–S27. [Google Scholar] [CrossRef]
- McAndrew, M.P.; Gorman, P.W.; Lange, T.A. Tricalcium phosphate as a bone graft substitute in trauma: Preliminary report. J. Orthop. Trauma 1988, 2, 333–339. [Google Scholar] [CrossRef]
- Li, W.; Cooper, J.A.J.r.; Mauck, R.L.; Tuan, R.S. Fabrication and characterization of six electrospun poly (α-hydroxy ester)-based fibrous scaffolds for tissue engineering applications. Acta Biomater. 2006, 2, 377–385. [Google Scholar] [CrossRef]
- Albrektsson, T.; Johansson, C. Osteoinduction, osteoconduction and osteointegration. Eur. Spine J. 2001, 10, S96–S101. [Google Scholar] [CrossRef] [Green Version]
- Shanjani, Y.; Kang, Y.; Zarnescu, L.; Ellerbee Bowden, A.K.; Koh, J.T.; Ker, D.F.E.; Yang, Y. Endothelial pattern formation in hybrid constructs of additive manufactured porous rigid scaffolds and cell-laden hydrogels. J. Mech. Behav. Biomed. 2017, 65, 356–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawai, T.; Shanjani, Y.; Fazeli, S.; Behn, A.W.; Okuzu, Y.; Goodman, S.B.; Yang, Y.P. Customized, degradable, functionally graded scaffold for potential treatment of early stage osteonecrosis of the femoral head. J. Orthop. Res. 2018, 36, 1002–1011. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, M.; Nabeshima, A.; Pan, C.C.; Behn, A.W.; Thio, T.; Lin, T.; Pajarinen, J.; Kawai, T.; Takagi, M.; Goodman, S.B.; et al. The effects of a functionally-graded scaffold and bone marrow-derived mononuclear cells on steroid-induced femoral head osteonecrosis. Biomaterials 2018, 187, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Legeros, R.Z. Calcium phosphate-based osteoinductive materials. Chem. Rev. 2008, 108, 4742–4753. [Google Scholar] [CrossRef]
- Woodruff, M.A.; Hutmacher, D.W. The return of a forgotten polymer—Polycaprolactone in the 21st century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar] [CrossRef] [Green Version]
- Bose, S.; Vahabzadeh, S.; Bandyopadhyay, A. Bone tissue engineering using 3D printing. Mater. Today 2013, 16, 496–504. [Google Scholar] [CrossRef]
- Derakhshanfar, S.; Mbeleck, R.; Xu, K.; Zhang, X.; Zhong, W.; Xing, M. 3D bioprinting for biomedical devices and tissue engineering: A review of recent trends and advances. Bioact. Mater. 2018, 3, 144–156. [Google Scholar] [CrossRef]
- Lam, C.X.; Hutmacher, D.W.; Schantz, J.T.; Woodruff, M.A. Evaluation of polycaprolactone scaffold degradation for 6 months in vitro and in vivo. J. Biomed. Mater. Res. Part A 2009, 90, 906–919. [Google Scholar] [CrossRef]
- Lam, C.X.; Teoh, S.H.; Hutmacher, D.W. Comparison of the degradation of polycaprolactone and polycaprolactone–(b-tricalcium phosphate) scaffolds in alkaline medium. Polym. Int. 2007, 56, 718–728. [Google Scholar] [CrossRef]
- Ker, D.F.E.; Wang, D.; Behn, A.W.; Wang, E.T.H.; Zhang, X.; Zhou, B.Y.; Mercado-Pagán, Á.E.; Kim, S.; Kleimeyer, J.; Gharaibeh, B.; et al. Functionally Graded, Bone- and Tendon-Like Polyurethane for Rotator Cuff Repair. Adv. Funct. Mater. 2018, 28, 1–16. [Google Scholar] [CrossRef]
- Baume, A.S.; Boughton, P.C.; Coleman, N.V.; Ruys, A.J. Sterilization of tissue scaffolds. In Characterisation and Design of Tissue Scaffolds, 1st ed.; Tomlins, P., Ed.; Woodhead Publishing: Cambridge, UK, 2016. [Google Scholar]
- Bruyas, A.; Moeinzadeh, S.; Kim, S.; Lowenberg, D.W.; Yang, Y.P. Effect of Electron Beam Sterilization on Three-Dimensional-Printed Polycaprolactone/Beta-Tricalcium Phosphate Scaffolds for Bone Tissue Engineering. Tissue Eng. Part A 2019, 25, 1–9. [Google Scholar] [CrossRef]
- Cottam, E.; Hukins, D.W.; Lee, K.; Hewitt, C.; Jenkins, M.J. Effect of sterilisation by gamma irradiation on the ability of polycaprolactone (PCL) to act as a scaffold material. Med. Eng. Phys. 2009, 31, 221–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz, E.; Sandonis, I.; Valle, M.B. In Vitro Degradation of Poly(caprolactone)/nHA Composites. J. Nanomater. 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Yeo, A.; Rai, B.; Sju, E.; Cheong, J.J.; Teoh, S.H. The degradation profile of novel, bioresorbable PCL-TCP scaffolds: An in vitro and in vivo study. J. Biomed. Mater. Res. Part. A 2007, 84, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Rai, B.; Ho, K.H.; Teoh, S.H. In vitro degradation of novel bioactive polycaprolactone—20% tricalcium phosphate composite scaffolds for bone engineering. Mater. Sci. Eng. C 2007, 27, 293–298. [Google Scholar] [CrossRef]
- Bruyas, A.; Lou, F.; Stahl, A.M.; Gardner, M.; Maloney, W.; Goodman, S.; Yang, Y.P. Systemic characterization of 3D-printed PCL/β-TCP scaffolds for biomedical devices and bone tissue engineering: Influence of composition and porosity. J. Mater. Res. 2018, 0, 1–12. [Google Scholar] [CrossRef]
- Schantz, J.T.; Teoh, S.H.; Lim, T.C.; Endres, M.; Lam, C.X.; Hutmacher, D.W. Repair of calvarial defects with customized tissue-engineered bone grafts 1. Evaluation of osteogenesis in a three-dimensional culture system. Tissue Eng. 2003, 9, S113–S126. [Google Scholar] [CrossRef]
- Darwis, D.; Mitomo, H.; Yoshii, F. Degradability of radiation crosslinked PCL in the supercooled state under various environments. Polym. Degrad. Stab. 1999, 65, 279–285. [Google Scholar] [CrossRef]
- Sung, H.J.; Meredith, C.; Johnson, C.; Galis, Z.S. The effect of scaffold degradation rate on three-dimensional cell growth and angiogenesis. Biomaterials 2004, 25, 5735–5742. [Google Scholar] [CrossRef]
- Thuaksuban, N.; Pannak, R.; Boonyaphiphat, P.; Monmaturapoj, N. In vivo biocompatibility and degradation of novel Polycaprolactone-Biphasic Calcium phosphate scaffolds used as a bone substitute. Biomed. Mater. Eng. 2018, 29, 253–267. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, J. Computed Tomography: Principles, Design, Artifacts, and Recent Advances, 2nd ed.; SPIE: Bellingham, WA, USA, 2009. [Google Scholar]
- Buzug, T.M. Computed Tomography. In Springer Handbook of Medical Technology; Kramme, R., Hoffmann, K.P., Pozos, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Wang, Y.; Garcea, S.C.; Withers, P.J. 7.6 Computed tomography of composites. Compr. Comp. Mater. 2018, 7, 101–118. [Google Scholar]
- Davis, G.R.; Elliott, J.C. Artefacts in X-ray microtomography of materials. Mater. Sci. Technol. Ser. 2006, 22, 1011–1018. [Google Scholar] [CrossRef]
- Fadaie, M.; Mirzaei, E. Nanofibrillated chitosan/polycaprolactone bionanocomposite scaffold with improved tensile strength and cellular behavior. Nanomed. J. 2019, 5, 77–89. [Google Scholar] [CrossRef]
- Kim, J.J.; Singh, R.K.; Seo, S.J.; Kim, T.H.; Kim, J.H.; Lee, E.J.; Kim, H.W. Magnetic scaffolds of polycaprolactone with functionalized magnetite nanoparticles: Physicochemical, mechanical, and biological properties effective for bone regeneration. RSC Adv. 2014, 4, 17325–17336. [Google Scholar] [CrossRef]
- Wypych, G. Microscopic Mechanisms of Damage Caused by Degradants. In Atlas of Material Damage, 2nd ed.; ChemTec Publishing: Toronto, ON, Canada, 2017. [Google Scholar]
- Vohra, S.; Hennessy, K.M.; Sawyer, A.A.; Zhuo, Y.; Bellis, S.L. Comparison of mesenchymal stem cell and osteosarcoma cell adhesion to hydroxyapatite. J. Mater. Sci. Mater. Med. 2008, 19, 3567. [Google Scholar] [CrossRef] [Green Version]
- Pêgo, A.; Van Luyn, M.; Brouwer, L.; Van Wachem, P.; Poot, A.A.; Grijpma, D.W.; Feijen, J. In vivo behavior of poly (1,3-trimethylene carbonate) and copolymers of 1,3-trimethylene carbonate with D,L-lactide or ϵ-caprolactone: Degradation and tissue response. J. Biomed. Mater. Res. Part A 2003, 67, 1044–1054. [Google Scholar] [CrossRef]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [Green Version]
- Barbeck, M.; Kubesch, A.; Booms, P.; Boehm, N.; Choukroun, J.; Sader, R.; Kirkpatrick, C.J.; Lorenz, J.; Ghanaati, S. Porcine dermis-derived collagen membranes induce implantation bed vascularization via multinucleated giant cells: A physiological reaction? J. Oral Implantol. 2015, 41, 238–251. [Google Scholar] [CrossRef]
- Barbeck, M.; Lorenz, J.; Holthaus, M.G.; Raetscho, N.; Kubesch, A.; Booms, P.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. Porcine Dermis and Pericardium-Based, Non–Cross-Linked Materials Induce Multinucleated Giant Cells After Their In Vivo Implantation: A Physiological Reaction? J. Oral Implantol. 2015, 41, 267–281. [Google Scholar] [CrossRef]
- Barbeck, M.; Najman, S.; Stojanović, S.; Mitić, Ž.; Živković, J.M.; Choukroun, J.; Kovačević, P.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. Addition of blood to a phycogenic bone substitute leads to increased in vivo vascularization. Biomed. Mater. 2015, 10, 1–15. [Google Scholar] [CrossRef] [Green Version]
- DeBaun, M.R.; Stahl, A.M.; Daoud, A.I.; Pan, C.C.; Bishop, J.A.; Gardner, M.J.; Yang, Y.P. Preclinical Induced Membrane Model to Evaluate Synthetic Implants for Healing Critical Bone Defects Without Autograft. J. Orthop. Res. 2019, 37, 60–68. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Filament Group | Code | Quantity | |
|---|---|---|---|
| E-beam | 100% PCL | 0, e | 5 |
| 20% TCP/80% PCL | 20, e | 5 | |
| 40% TCP/60% PCL | 40, e | 5 | |
| 60% TCP/40% PCL | 60, e | 5 | |
| Non-E-beam | 100% PCL | 0, no e | 5 |
| 20% TCP/80% PCL | 20, no e | 5 | |
| 40% TCP/60% PCL | 40, no e | 5 | |
| 60% TCP/40% PCL | 60, no e | 5 | |
| Time/Group | 20, e | 40, e | 60, e | 20, no e | 40, no e | 60, no e |
|---|---|---|---|---|---|---|
| Before surgery (micro-CT) (%) | 28.05 | 21.30 | 27.73 | 26.13 | 22.00 | 26.24 |
| 1 day after implantation (live-CT) (%) | 28.83 | 22.64 | 29.23 | 26.93 | 23.74 | 27.25 |
| Volume change (%) | +2.78 | +6.29 | +5.4 | +3.09 | +7.88 | +3.84 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, J.-H.; Kaneda, J.; Jang, J.-G.; Sakthiabirami, K.; Lui, E.; Kim, C.; Wang, A.; Park, S.-W.; Yang, Y.P. The Influence of Electron Beam Sterilization on In Vivo Degradation of β-TCP/PCL of Different Composite Ratios for Bone Tissue Engineering. Micromachines 2020, 11, 273. https://doi.org/10.3390/mi11030273
Kang J-H, Kaneda J, Jang J-G, Sakthiabirami K, Lui E, Kim C, Wang A, Park S-W, Yang YP. The Influence of Electron Beam Sterilization on In Vivo Degradation of β-TCP/PCL of Different Composite Ratios for Bone Tissue Engineering. Micromachines. 2020; 11(3):273. https://doi.org/10.3390/mi11030273
Chicago/Turabian StyleKang, Jin-Ho, Janelle Kaneda, Jae-Gon Jang, Kumaresan Sakthiabirami, Elaine Lui, Carolyn Kim, Aijun Wang, Sang-Won Park, and Yunzhi Peter Yang. 2020. "The Influence of Electron Beam Sterilization on In Vivo Degradation of β-TCP/PCL of Different Composite Ratios for Bone Tissue Engineering" Micromachines 11, no. 3: 273. https://doi.org/10.3390/mi11030273