Electroencephalographic Abnormalities in Autism Spectrum Disorder: Characteristics and Therapeutic Implications

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. SEAs in Non-Epileptic Patients with ASD
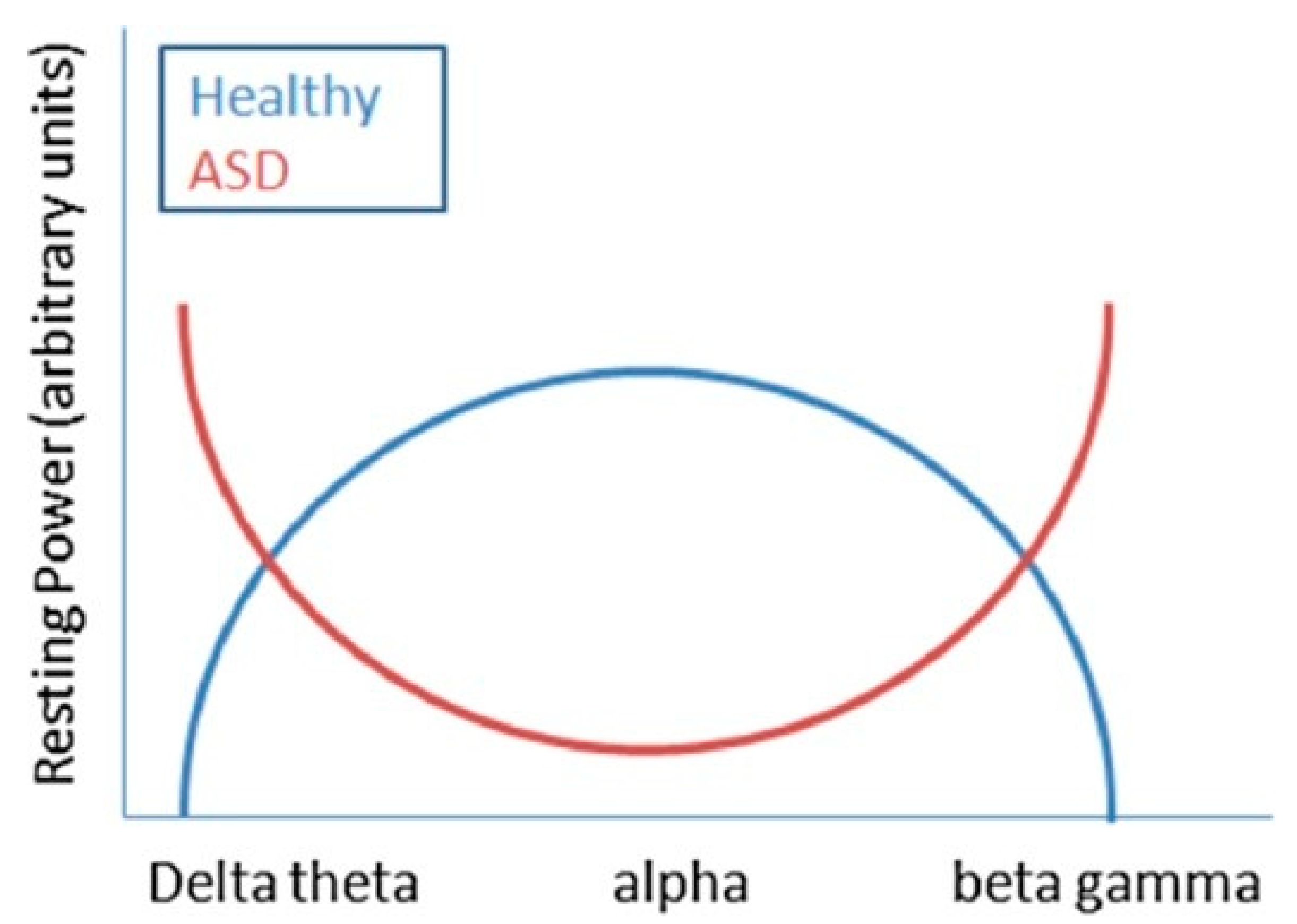
3. Electroencephalographic Patterns
4. Treatment Implications in Patients with ASD and SEAs
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kanner, L. Autistic disturbances of affective contact. Acta Paedopsychiatr. 1968, 35, 100–136. [Google Scholar] [PubMed]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- Amiet, C.; Gourfinkel-An, I.; Bouzamondo, A.; Tordjman, S.; Baulac, M.; Lechat, P.; Mottron, L.; Cohen, D. Epilepsy in autism is associated with intellectual disability and gender: Evidence from a meta-analysis. Biol. Psychiatry 2008, 64, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.R.; Melyn, M. EEG and seizures in autistic children and adolescents: Further findings with therapeutic implications. Clin. EEG Neurosci. 2005, 36, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Viscidi, E.W.; Triche, E.W.; Pescosolido, M.F.; McLean, R.L.; Joseph, R.M.; Spence, S.J.; Morrow, E.M. Clinical characteristics of children with autism spectrum disorder and co-occurring epilepsy. PLoS ONE 2013, 8, e67797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuhara, A. Correlation between EEG abnormalities and symptoms of autism spectrum disorder (ASD). Brain Dev. 2010, 32, 791–798. [Google Scholar] [CrossRef]
- Shubrata, K.S.; Sinha, S.; Seshadri, S.P.; Girimaji, S.; Subbakrishna, D.K.; Srinath, S. Childhood autism spectrum disorders with and without epilepsy: Clinical implications. J. Child Neurol. 2015, 30, 476–482. [Google Scholar] [CrossRef]
- Parmeggiani, A.; Barcia, G.; Posar, A.; Raimondi, E.; Santucci, M.; Scaduto, M.C. Epilepsy and EEG paroxysmal abnormalities in autism spectrum disorders. Brain Dev. 2010, 32, 783–789. [Google Scholar] [CrossRef]
- Pavone, P.; Incorpora, G.; Fiumara, A.; Parano, E.; Trifiletti, R.R.; Ruggieri, M. Epilepsy is not a prominent feature of primary autism. Neuropediatrics 2004, 35, 207–210. [Google Scholar] [CrossRef]
- Woolfenden, S.; Sarkozy, V.; Ridley, G.; Coory, M.; Williams, K. A systematic review of two outcomes in autism spectrum disorder—Epilepsy and mortality. Dev. Med. Child Neurol. 2012, 54, 306–312. [Google Scholar] [CrossRef]
- Volkmar, F.R.; Nelson, D.S. Seizure disorders in autism. J. Am. Acad. Child Adolesc. Psychiatry 1990, 29, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Operto, F.F.; Pastorino, G.M.G.; Mazza, R.; Roccella, M.; Carotenuto, M.; Margari, L.; Verrotti, A. Cognitive profile in BECTS treated with levetiracetam: A 2-year follow-up. Epilepsy Behav. 2019, 97, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Carotenuto, M.; Parisi, P.; Esposito, M.; Cortese, S.; Elia, M. Sleep alterations in children with refractory epileptic encephalopathies: A polysomnographic study. Epilepsy Behav. 2014, 35, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Spence, S.J.; Schneider, M.T. The role of epilepsy and epileptiform EEGs in autism spectrum disorders. Pediatr. Res. 2009, 65, 599–606. [Google Scholar] [CrossRef]
- Marotta, R.; Risoleo, M.C.; Messina, G.; Parisi, L.; Carotenuto, M.; Vetri, L.; Roccella, M. The Neurochemistry of Autism. Brain Sci. 2020, 10, 163. [Google Scholar] [CrossRef] [Green Version]
- Keller, R.; Basta, R.; Salerno, L.; Elia, M. Autism, epilepsy, and synaptopathies: A not rare association. Neurol. Sci. 2017, 38, 1353–1361. [Google Scholar] [CrossRef]
- Resendiz-Aparicio, J.C.; Coiscou-Dominguez, N.R.; Yanez-Acosta, L.; Rodriguez-Rodriguez, E.; Rivera-Quintero, J.; Aguirre-Garcia, E.; Cruz-Martinez, E. Epileptiform activity in psychiatric disorders in children. Rev. Neurol. 2008, 46, 660–663. [Google Scholar]
- Capdevila, O.S.; Dayyat, E.; Kheirandish-Gozal, L.; Gozal, D. Prevalence of epileptiform activity in healthy children during sleep. Sleep Med. 2008, 9, 303–309. [Google Scholar] [CrossRef]
- Binnie, C.D. Cognitive impairment during epileptiform discharges: Is it ever justifiable to treat the EEG? Lancet Neurol. 2003, 2, 725–730. [Google Scholar] [CrossRef]
- Aldenkamp, A.; Arends, J. The relative influence of epileptic EEG discharges, short nonconvulsive seizures, and type of epilepsy on cognitive function. Epilepsia 2004, 45, 54–63. [Google Scholar] [CrossRef]
- Smirni, D.; Smirni, P.; Di Martino, G.; Operto, F.F.; Carotenuto, M. Emotional Awareness and Cognitive Performance in Borderline Intellectual Functioning Young Adolescents. J. Nerv. Ment. Dis. 2019, 207, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Ghacibeh, G.A.; Fields, C. Interictal epileptiform activity and autism. Epilepsy Behav. 2015, 47, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Akshoomoff, N.; Farid, N.; Courchesne, E.; Haas, R. Abnormalities on the neurological examination and EEG in young children with pervasive developmental disorders. J. Autism Dev. Disord. 2007, 37, 887–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulligan, C.K.; Trauner, D.A. Incidence and behavioral correlates of epileptiform abnormalities in autism spectrum disorders. J. Autism Dev. Disord. 2014, 44, 452–458. [Google Scholar] [CrossRef]
- Rossi, P.G.; Posar, A.; Parmeggiani, A. Epilepsy in adolescents and young adults with autistic disorder. Brain Dev. 2000, 22, 102–106. [Google Scholar] [CrossRef]
- Cavazzuti, G.B.; Cappella, L.; Nalin, A. Longitudinal study of epileptiform EEG patterns in normal children. Epilepsia 1980, 21, 43–55. [Google Scholar] [CrossRef]
- Swatzyna, R.J.; Tarnow, J.D.; Turner, R.P.; Roark, A.J.; MacInerney, E.K.; Kozlowski, G.P. Integration of EEG Into Psychiatric Practice: A Step Toward Precision Medicine for Autism Spectrum Disorder. J. Clin. Neurophysiol. 2017, 34, 230–235. [Google Scholar] [CrossRef]
- Valvo, G.; Baldini, S.; Brachini, F.; Apicella, F.; Cosenza, A.; Ferrari, A.R.; Guerrini, R.; Muratori, F.; Romano, M.F.; Santorelli, F.M.; et al. Somatic overgrowth predisposes to seizures in autism spectrum disorders. PLoS ONE 2013, 8, e75015. [Google Scholar] [CrossRef] [Green Version]
- Rossi, P.G.; Parmeggiani, A.; Bach, V.; Santucci, M.; Visconti, P. EEG features and epilepsy in patients with autism. Brain Dev. 1995, 17, 169–174. [Google Scholar] [CrossRef]
- Tuchman, R.F.; Rapin, I. Regression in pervasive developmental disorders: Seizures and epileptiform electroencephalogram correlates. Pediatrics 1997, 99, 560–566. [Google Scholar] [CrossRef]
- Hrdlicka, M.; Komarek, V.; Propper, L.; Kulisek, R.; Zumrova, A.; Faladova, L.; Havlovicova, M.; Sedlacek, Z.; Blatny, M.; Urbanek, T. Not EEG abnormalities but epilepsy is associated with autistic regression and mental functioning in childhood autism. Eur. Child Adolesc. Psychiatry 2004, 13, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Canitano, R.; Luchetti, A.; Zappella, M. Epilepsy, electroencephalographic abnormalities, and regression in children with autism. J. Child Neurol. 2005, 20, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Chez, M.G.; Chang, M.; Krasne, V.; Coughlan, C.; Kominsky, M.; Schwartz, A. Frequency of epileptiform EEG abnormalities in a sequential screening of autistic patients with no known clinical epilepsy from 1996 to 2005. Epilepsy Behav. 2006, 8, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Hara, H. Autism and epilepsy: A retrospective follow-up study. Brain Dev. 2007, 29, 486–490. [Google Scholar] [CrossRef]
- Baird, G.; Robinson, R.O.; Boyd, S.; Charman, T. Sleep electroencephalograms in young children with autism with and without regression. Dev. Med. Child Neurol. 2006, 48, 604–608. [Google Scholar] [CrossRef]
- Hartley, S.L.; Barker, E.T.; Seltzer, M.M.; Floyd, F.; Greenberg, J.; Orsmond, G.; Bolt, D. The relative risk and timing of divorce in families of children with an autism spectrum disorder. J. Fam. Psychol. 2010, 24, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Capal, J.K.; Carosella, C.; Corbin, E.; Horn, P.S.; Caine, R.; Manning-Courtney, P. EEG endophenotypes in autism spectrum disorder. Epilepsy Behav. 2018, 88, 341–348. [Google Scholar] [CrossRef]
- Milovanovic, M.; Radivojevic, V.; Radosavljev-Kircanski, J.; Grujicic, R.; Toskovic, O.; Aleksic-Hil, O.; Pejovic-Milovancevic, M. Epilepsy and interictal epileptiform activity in patients with autism spectrum disorders. Epilepsy Behav. 2019, 92, 45–52. [Google Scholar] [CrossRef]
- Nicotera, A.G.; Hagerman, R.J.; Catania, M.V.; Buono, S.; Di Nuovo, S.; Liprino, E.M.; Stracuzzi, E.; Giusto, S.; Di Vita, G.; Musumeci, S.A. EEG Abnormalities as a Neurophysiological Biomarker of Severity in Autism Spectrum Disorder: A Pilot Cohort Study. J. Autism Dev. Disord. 2019, 49, 2337–2347. [Google Scholar] [CrossRef]
- Trauner, D.A. Behavioral correlates of epileptiform abnormalities in autism. Epilepsy Behav. 2015, 47, 163–166. [Google Scholar] [CrossRef]
- Coppola, G.; Operto, F.F.; Auricchio, G.; D’Amico, A.; Fortunato, D.; Pascotto, A. Temporal lobe dual pathology in malignant migrating partial seizures in infancy. Epileptic Disord. 2007, 9, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kang, H.C.; Kim, S.W.; Kim, Y.K.; Chung, H.J. Characteristics of late-onset epilepsy and EEG findings in children with autism spectrum disorders. Korean J. Pediatr. 2011, 54, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Smirni, D.; Precenzano, F.; Magliulo, R.M.; Romano, P.; Bonifacio, A.; Gison, G.; Bitetti, I.; Terracciano, M.; Ruberto, M.; Sorrentino, M. Inhibition, set-shifting and working memory in Global Developmental Delay preschool children. Life Span Disabil. 2018, 21, 191–206. [Google Scholar]
- Blume, J.; Wittke, K.; Naigles, L.; Mastergeorge, A.M. Language Growth in Young Children with Autism: Interactions Between Language Production and Social Communication. J. Autism Dev. Disord. 2020. [Google Scholar] [CrossRef]
- Carotenuto, M.; Ruberto, M.; Fontana, M.L.; Catania, A.; Misuraca, E.; Precenzano, F.; Lanzara, V.; Messina, G.; Roccella, M.; Smirni, D. Executive functioning in autism spectrum disorders: A case-control study in preschool children. Curr. Pediatric Res. 2019, 23, 112–116. [Google Scholar]
- Unal, O.; Ozcan, O.; Oner, O.; Akcakin, M.; Aysev, A.; Deda, G. EEG and MRI findings and their relation with intellectual disability in pervasive developmental disorders. World J. Pediatr. 2009, 5, 196–200. [Google Scholar] [CrossRef] [Green Version]
- Ekinci, O.; Arman, A.R.; Isik, U.; Bez, Y.; Berkem, M. EEG abnormalities and epilepsy in autistic spectrum disorders: Clinical and familial correlates. Epilepsy Behav. 2010, 17, 178–182. [Google Scholar] [CrossRef]
- Lado, F.A.; Rubboli, G.; Capovilla, G.; Avanzini, G.; Moshe, S.L. Pathophysiology of epileptic encephalopathies. Epilepsia 2013, 54 (Suppl. 8), 6–13. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Barstein, J.; Ethridge, L.E.; Mosconi, M.W.; Takarae, Y.; Sweeney, J.A. Resting state EEG abnormalities in autism spectrum disorders. J. Neurodev. Disord. 2013, 5, 24. [Google Scholar] [CrossRef] [Green Version]
- Tallon-Baudry, C. Oscillatory synchrony and human visual cognition. J. Physiol. 2003, 97, 355–363. [Google Scholar] [CrossRef]
- Cantor, D.S.; Thatcher, R.W.; Hrybyk, M.; Kaye, H. Computerized EEG analyses of autistic children. J. Autism Dev. Disord. 1986, 16, 169–187. [Google Scholar] [CrossRef] [PubMed]
- Leno, V.C.; Tomlinson, S.B.; Chang, S.A.; Naples, A.J.; McPartland, J.C. Resting-state alpha power is selectively associated with autistic traits reflecting behavioral rigidity. Sci. Rep. 2018, 8, 11982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Diessen, E.; Senders, J.; Jansen, F.E.; Boersma, M.; Bruining, H. Increased power of resting-state gamma oscillations in autism spectrum disorder detected by routine electroencephalography. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 537–540. [Google Scholar] [CrossRef] [Green Version]
- Tierney, A.L.; Gabard-Durnam, L.; Vogel-Farley, V.; Tager-Flusberg, H.; Nelson, C.A. Developmental trajectories of resting EEG power: An endophenotype of autism spectrum disorder. PLoS ONE 2012, 7, e39127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, C.L.; Levin, A.R.; Gabard-Durnam, L.J.; Tager-Flusberg, H.; Nelson, C.A. Reduced frontal gamma power at 24 months is associated with better expressive language in toddlers at risk for autism. Autism Res. 2019, 12, 1211–1224. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, T.J.; Oeltzschner, G.; Hoogenboom, N.; Wittsack, H.J.; Schnitzler, A.; Lange, J. Beta Peak Frequencies at Rest Correlate with Endogenous GABA+/Cr Concentrations in Sensorimotor Cortex Areas. PLoS ONE 2016, 11, e0156829. [Google Scholar] [CrossRef]
- Uhlhaas, P.J.; Singer, W. Neural synchrony in brain disorders: Relevance for cognitive dysfunctions and pathophysiology. Neuron 2006, 52, 155–168. [Google Scholar] [CrossRef] [Green Version]
- Casanova, M.F.; van Kooten, I.A.; Switala, A.E.; van Engeland, H.; Heinsen, H.; Steinbusch, H.W.; Hof, P.R.; Trippe, J.; Stone, J.; Schmitz, C. Minicolumnar abnormalities in autism. Acta Neuropathol. 2006, 112, 287–303. [Google Scholar] [CrossRef]
- Levitt, P. Disruption of interneuron development. Epilepsia 2005, 46 (Suppl. 7), 22–28. [Google Scholar] [CrossRef]
- Casanova, M.F.; Buxhoeveden, D.P.; Switala, A.E.; Roy, E. Minicolumnar pathology in autism. Neurology 2002, 58, 428–432. [Google Scholar] [CrossRef]
- Casanova, M.F.; Buxhoeveden, D.P.; Gomez, J. Disruption in the inhibitory architecture of the cell minicolumn: Implications for autism. Neuroscientist 2003, 9, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.Q.; Whitehead, P.L.; Menold, M.M.; Martin, E.R.; Ashley-Koch, A.E.; Mei, H.; Ritchie, M.D.; Delong, G.R.; Abramson, R.K.; Wright, H.H.; et al. Identification of significant association and gene-gene interaction of GABA receptor subunit genes in autism. Am. J. Hum. Genet. 2005, 77, 377–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosconi, M.W.; Kay, M.; D’Cruz, A.M.; Seidenfeld, A.; Guter, S.; Stanford, L.D.; Sweeney, J.A. Impaired inhibitory control is associated with higher-order repetitive behaviors in autism spectrum disorders. Psychol. Med. 2009, 39, 1559–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, N.H.; Elliott, A.J.; Isler, J.R.; Rodriguez, C.; Friedrich, C.; Shuffrey, L.C.; Fifer, W.P. Neonatal EEG linked to individual differences in socioemotional outcomes and autism risk in toddlers. Dev. Psychobiol. 2019, 61, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- Gabard-Durnam, L.J.; Wilkinson, C.; Kapur, K.; Tager-Flusberg, H.; Levin, A.R.; Nelson, C.A. Longitudinal EEG power in the first postnatal year differentiates autism outcomes. Nat. Commun. 2019, 10, 4188. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, D.; Giuffre, M. The Coat-Hanger Angle Sign. J. Pediatr. 2016, 177, 325. [Google Scholar] [CrossRef] [Green Version]
- Newson, J.J.; Thiagarajan, T.C. EEG Frequency Bands in Psychiatric Disorders: A Review of Resting State Studies. Front. Hum. Neurosci. 2018, 12, 521. [Google Scholar] [CrossRef]
- Burnette, C.P.; Henderson, H.A.; Inge, A.P.; Zahka, N.E.; Schwartz, C.B.; Mundy, P.C. Anterior EEG asymmetry and the Modifier Model of Autism. J. Autism Dev. Disord. 2011, 41, 1113–1124. [Google Scholar] [CrossRef] [Green Version]
- Stroganova, T.A.; Nygren, G.; Tsetlin, M.M.; Posikera, I.N.; Gillberg, C.; Elam, M.; Orekhova, E.V. Abnormal EEG lateralization in boys with autism. Clin. Neurophysiol. 2007, 118, 1842–1854. [Google Scholar] [CrossRef]
- Sutton, S.K.; Burnette, C.P.; Mundy, P.C.; Meyer, J.; Vaughan, A.; Sanders, C.; Yale, M. Resting cortical brain activity and social behavior in higher functioning children with autism. J. Child Psychol. Psychiatry 2005, 46, 211–222. [Google Scholar] [CrossRef]
- McVoy, M.; Lytle, S.; Fulchiero, E.; Aebi, M.E.; Adeleye, O.; Sajatovic, M. A systematic review of quantitative EEG as a possible biomarker in child psychiatric disorders. Psychiatry Res. 2019, 279, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Coben, R.; Clarke, A.R.; Hudspeth, W.; Barry, R.J. EEG power and coherence in autistic spectrum disorder. Clin. Neurophysiol. 2008, 119, 1002–1009. [Google Scholar] [CrossRef]
- Kanemura, H.; Sano, F.; Tando, T.; Sugita, K.; Aihara, M. Can EEG characteristics predict development of epilepsy in autistic children? Eur. J. Paediatr. Neurol. 2013, 17, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Cetin, O.E.; Korkmaz, B.; Alev, G.; Demirbilek, V. EEG abnormalities and long term seizure outcome in high functioning autism. Acta Neurol. Belg. 2017, 117, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Danielsson, S.; Gillberg, I.C.; Billstedt, E.; Gillberg, C.; Olsson, I. Epilepsy in young adults with autism: A prospective population-based follow-up study of 120 individuals diagnosed in childhood. Epilepsia 2005, 46, 918–923. [Google Scholar] [CrossRef]
- Aarts, J.H.; Binnie, C.D.; Smit, A.M.; Wilkins, A.J. Selective cognitive impairment during focal and generalized epileptiform EEG activity. Brain 1984, 107 Pt 1, 293–308. [Google Scholar] [CrossRef] [Green Version]
- Binnie, C.D. Significance and management of transitory cognitive impairment due to subclinical EEG discharges in children. Brain Dev. 1993, 15, 23–30. [Google Scholar] [CrossRef]
- Plioplys, A.V. Autism: Electroencephalogram abnormalities and clinical improvement with valproic acid. Arch. Pediatr. Adolesc. Med. 1994, 148, 220–222. [Google Scholar] [CrossRef]
- Gordon, K.; Bawden, H.; Camfield, P.; Mann, S.; Orlik, P. Valproic acid treatment of learning disorder and severely epileptiform EEG without clinical seizures. J. Child Neurol. 1996, 11, 41–43. [Google Scholar] [CrossRef]
- Hollander, E.; Dolgoff-Kaspar, R.; Cartwright, C.; Rawitt, R.; Novotny, S. An open trial of divalproex sodium in autism spectrum disorders. J. Clin. Psychiatry 2001, 62, 530–534. [Google Scholar] [CrossRef]
- Pressler, R.M.; Robinson, R.O.; Wilson, G.A.; Binnie, C.D. Treatment of interictal epileptiform discharges can improve behavior in children with behavioral problems and epilepsy. J. Pediatr. 2005, 146, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.S.; Knutsson, E.; Nergardh, A. The effect of lamotrigine on epileptiform discharges in young patients with drug-resistant epilepsy. Epilepsia 2001, 42, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Jiang, L.; Tang, X. Levetiracetam is associated with decrease in subclinical epileptiform discharges and improved cognitive functions in pediatric patients with autism spectrum disorder. Neuropsychiatr. Dis. Treat. 2017, 13, 2321–2326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mordekar, S.R.; Prendergast, M.; Chattopadhyay, A.K.; Baxter, P.S. Corticosteroid treatment of behaviour, language and motor regression in childhood disintegrative disorder. Eur. J. Paediatr. Neurol. 2009, 13, 367–369. [Google Scholar] [CrossRef]
- Duffy, F.H.; Shankardass, A.; McAnulty, G.B.; Eksioglu, Y.Z.; Coulter, D.; Rotenberg, A.; Als, H. Corticosteroid therapy in regressive autism: A retrospective study of effects on the Frequency Modulated Auditory Evoked Response (FMAER), language, and behavior. BMC Neurol. 2014, 14, 70. [Google Scholar] [CrossRef] [Green Version]
- Lewine, J.D.; Andrews, R.; Chez, M.; Patil, A.A.; Devinsky, O.; Smith, M.; Kanner, A.; Davis, J.T.; Funke, M.; Jones, G.; et al. Magnetoencephalographic patterns of epileptiform activity in children with regressive autism spectrum disorders. Pediatrics 1999, 104, 405–418. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, I.S.; Loddenkemper, T.; Galanopoulou, A.S.; Moshe, S.L. Should epileptiform discharges be treated? Epilepsia 2015, 56, 1492–1504. [Google Scholar] [CrossRef]


{kind=link}
| Subjects | Mean Age (Years) | % SEAs | EEG Findings | Other Findings | |
|---|---|---|---|---|---|
| Rossi et al. (1995) [29] | 106 | 12.5 | 18.9% | Focal SEAs were mainly localized on centro-parieto-temporal regions | Higher incidence of severe intellectual disability |
| Tuchman and Rapin (1997) [30] | 335 | Not reported | 8% | Centrotemporal SEAs (~50%) | Higher incidence of Regression |
| Hrdlicka et al. (2004) [31] | 77 | 9.1 ± 5.3 | 48% | Non-epileptiform abnormality (18%); Epileptiform discharges (30%) | Abnormal early development |
| Canitano et al. (2005) [32] | 46 | 7.8 ± 2.7 | 22% | Focal 50%; Multifocal 50%; Diffuse 20% | No difference in regression rate |
| Chez et al. (2006) [33] | 889 | 5.3 | 60.7% | Right temporal region (21.5%), bilateral temporal central spikes (20.2%). Generalized spike–wave activity (16.2%) left temporal activity (15.2%) | No difference in regression rate |
| Hara (2007) [34] | 97 | 18–35 | 21% | Temporal region SEAs (60%) | Lower IQ and social skills in the epileptics rather than in patients with SEAs |
| Baird (2006) [35] | 64 | 3 ± 0.7 | ~31% | Not specified | No difference in regression rate |
| Akshoomoff et al. (2007) [23] | 60 | 2–6 | ~32% | 78% epileptiform abnormalities and 22% focal slowing | SEAs are more frequent in low-functioning autism (72%) |
| Hartley et al. (2010) [36] | 123 | Not reported | 31% | No significant abnormal discharge location | No differences in behavior between children with ASD with or without SEAs |
| Yasuhara (2010) [6] | 1014 | 9.3 ± 3.4 | ~49% | SEAs in frontal lobe (65.6%) | Lower IQ in patient with SEAs |
| Parmeggiani et al. (2010) [8] | 345 | mean age 10.5 years | 23.5% | SEAs in temporal and central areas (31.4%). | SEAs were not related to autistic regression |
| Valvo et al. (2013) [28] | 206 | 7.1 ± 3.8 | 51% | EEG abnormalities were not specified | Tall stature was significantly associated with SEAs |
| Mulligan and Trauner (2014) [24] | 101 | 7.06 ± 3.74 | 50% | The most frequent location was frontal with multifocal or generalized epileptiform abnormalities | Higher incidence of SEAs in children with stereotypies and aggressive behavior |
| Swatzyna et al. (2017) [27] | 140 | 4–25 | 36% | EEG abnormalities were not specified | SEAs are regardless of age or gender |
| Capal et al. (2018) [37] | 372 | 45 ± 16.4 (months at ASD diagnosis) | 25.5% | 67.4% epileptiform, 36.8% other abnormalities. 83% Focal and more frequent in the left temporal region | Impaired adaptive functioning |
| Milovanovic et al. (2019) [38] | 112 | 6.58 ± 3.72 | 12.5% | Slow background activity, abnormal sleep architecture | Better motor skills in patient without SEAs |
| Nicotera et al. (2019) [39] | 69 | 6.5 ± 4.01 | 39.13% | Non-epileptiform abnormalities 13%; epileptiform abnormalities 26% | SEAs significantly higher in patients with severer forms of ASD. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Precenzano, F.; Parisi, L.; Lanzara, V.; Vetri, L.; Operto, F.F.; Pastorino, G.M.G.; Ruberto, M.; Messina, G.; Risoleo, M.C.; Santoro, C.; et al. Electroencephalographic Abnormalities in Autism Spectrum Disorder: Characteristics and Therapeutic Implications. Medicina 2020, 56, 419. https://doi.org/10.3390/medicina56090419
Precenzano F, Parisi L, Lanzara V, Vetri L, Operto FF, Pastorino GMG, Ruberto M, Messina G, Risoleo MC, Santoro C, et al. Electroencephalographic Abnormalities in Autism Spectrum Disorder: Characteristics and Therapeutic Implications. Medicina. 2020; 56(9):419. https://doi.org/10.3390/medicina56090419
Chicago/Turabian StylePrecenzano, Francesco, Lucia Parisi, Valentina Lanzara, Luigi Vetri, Francesca Felicia Operto, Grazia Maria Giovanna Pastorino, Maria Ruberto, Giovanni Messina, Maria Cristina Risoleo, Claudia Santoro, and et al. 2020. "Electroencephalographic Abnormalities in Autism Spectrum Disorder: Characteristics and Therapeutic Implications" Medicina 56, no. 9: 419. https://doi.org/10.3390/medicina56090419