Cytotoxicity and Bioactivity of Dental Pulp-Capping Agents towards Human Tooth-Pulp Cells: A Systematic Review of In-Vitro Studies and Meta-Analysis of Randomized and Controlled Clinical Trials

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Study Selection and Data Collection Process
2.6. Risk of Bias in Individual Studies
2.7. Data Analysis
2.7.1. Data Synthesis
2.7.2. Heterogeneity Assessment
2.7.3. Assessment of Publication Bias
2.7.4. Summary Measures
2.8. Statistical Analysis
2.9. Risk of Bias Across Studies (Certainty in the Evidence)
3. Results
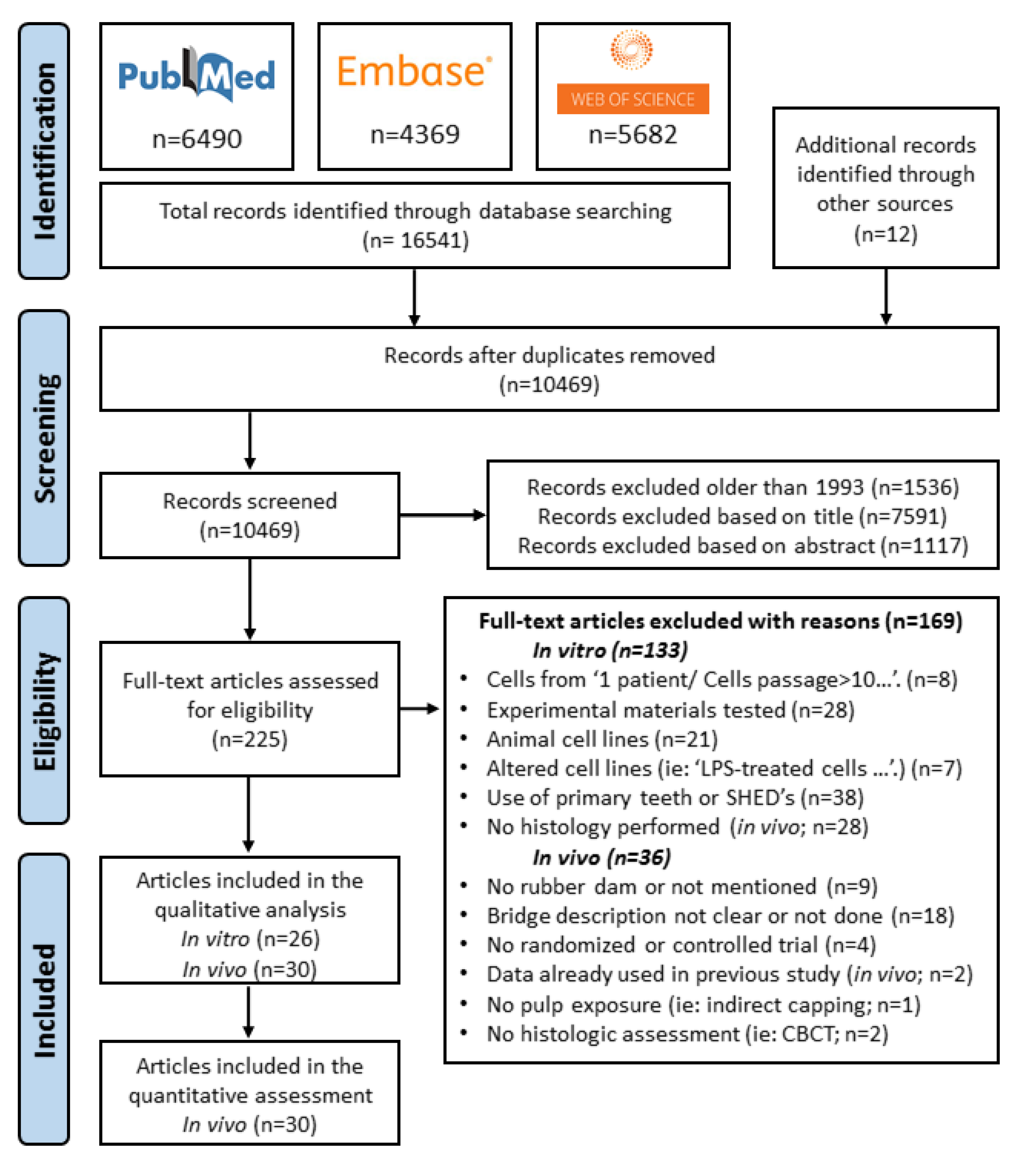
3.1. Search Results and Study Selection
3.2. Study Characteristics
Risk of Bias within Studies
3.3. Synthesis of Results
3.3.1. Qualitative Analysis of In Vitro Studies
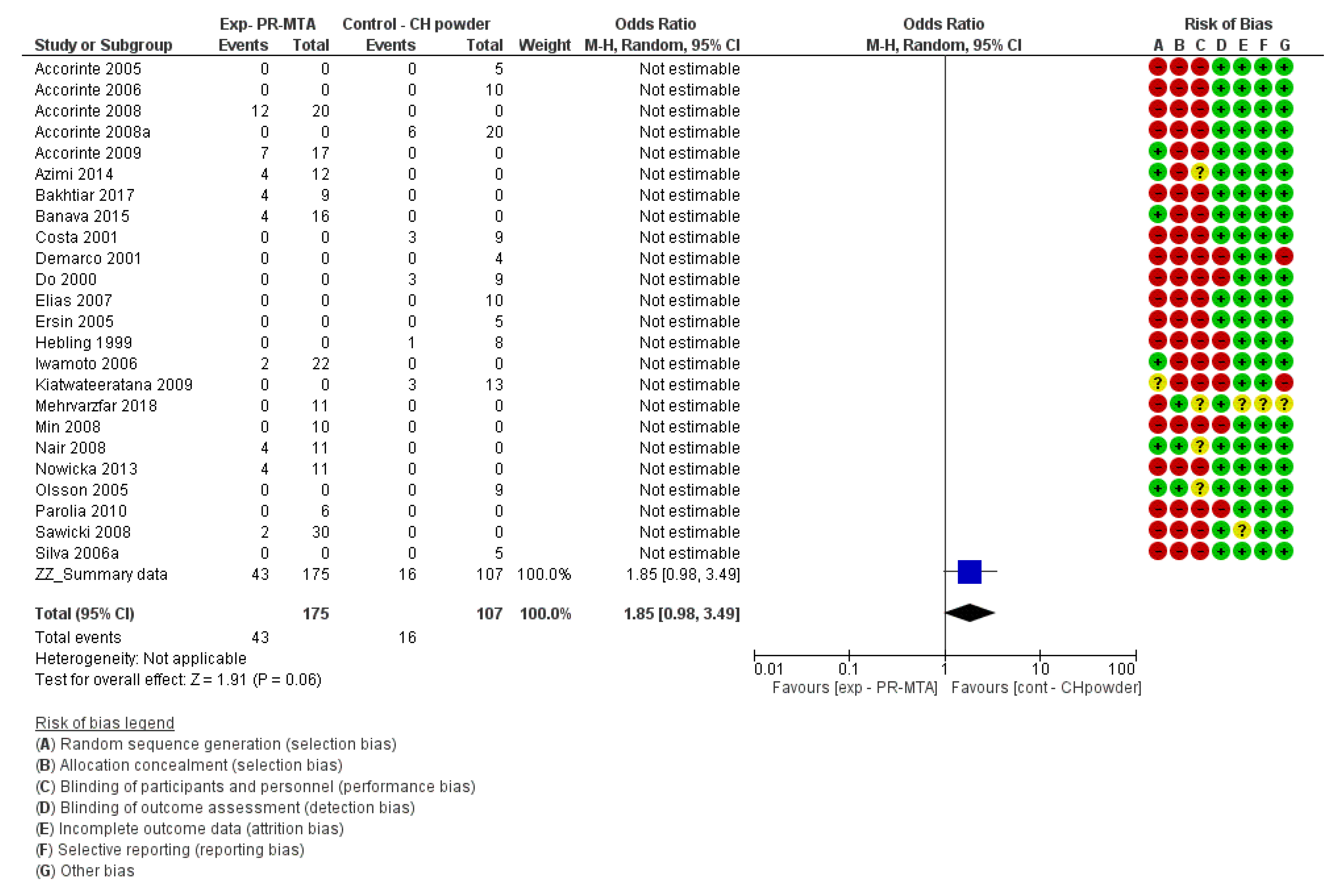
3.3.2. Meta-Analysis of the Effect of Pulp-Capping Agents on the Inflammatory Reaction Induced in Human Pulp Tissue
Inflammatory Reaction at Day 30
Inflammatory Reaction at Day 15
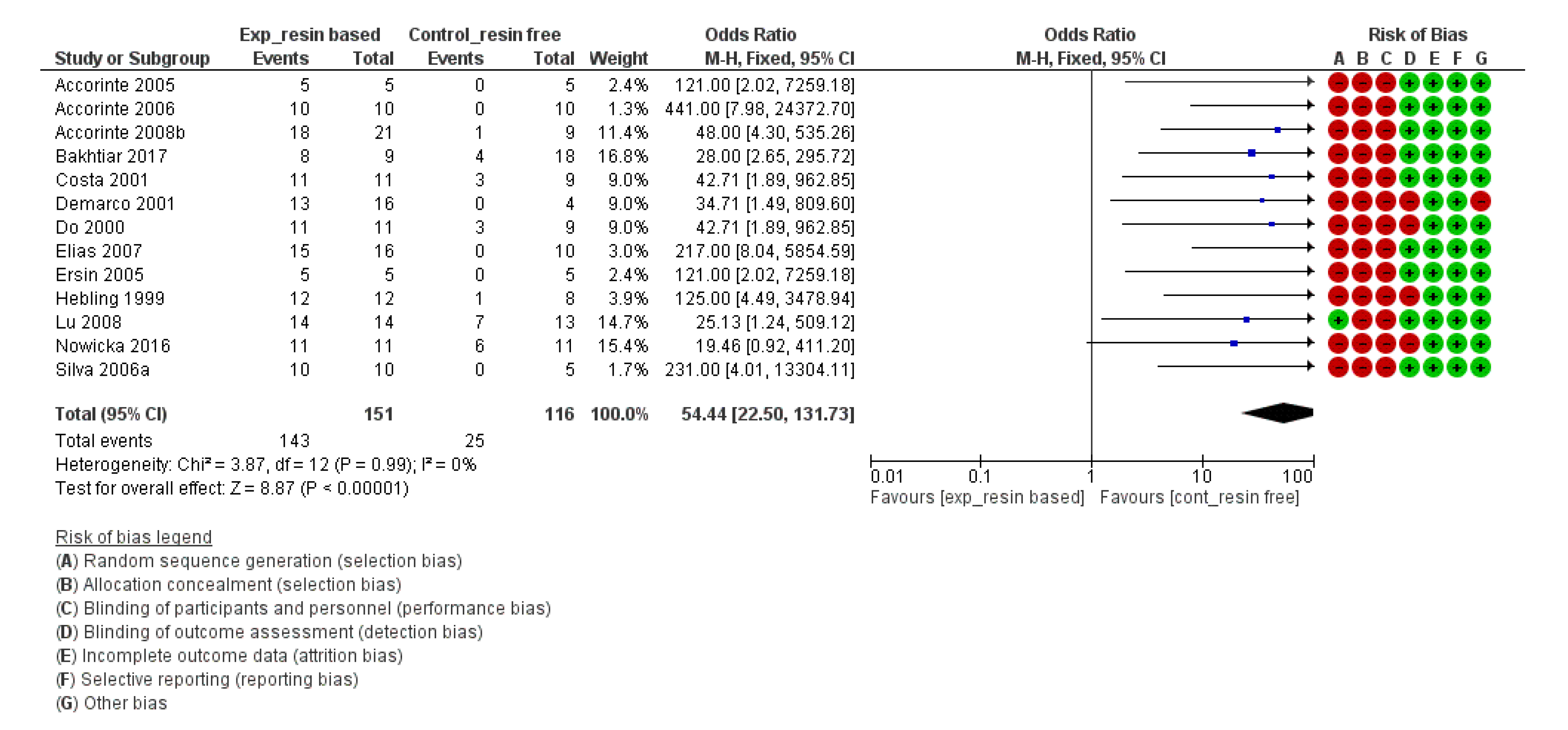
Inflammatory Reaction up to Day 7
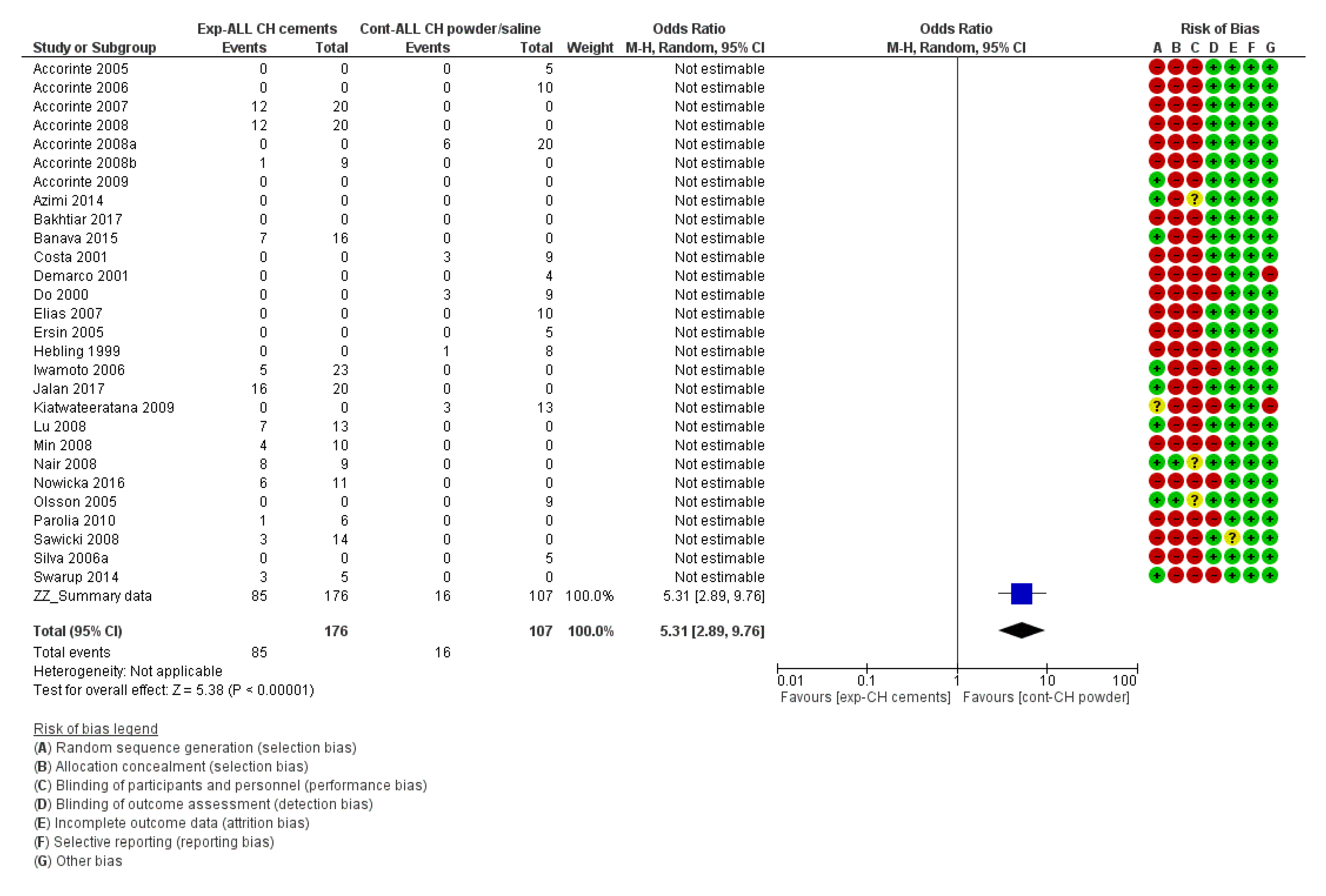
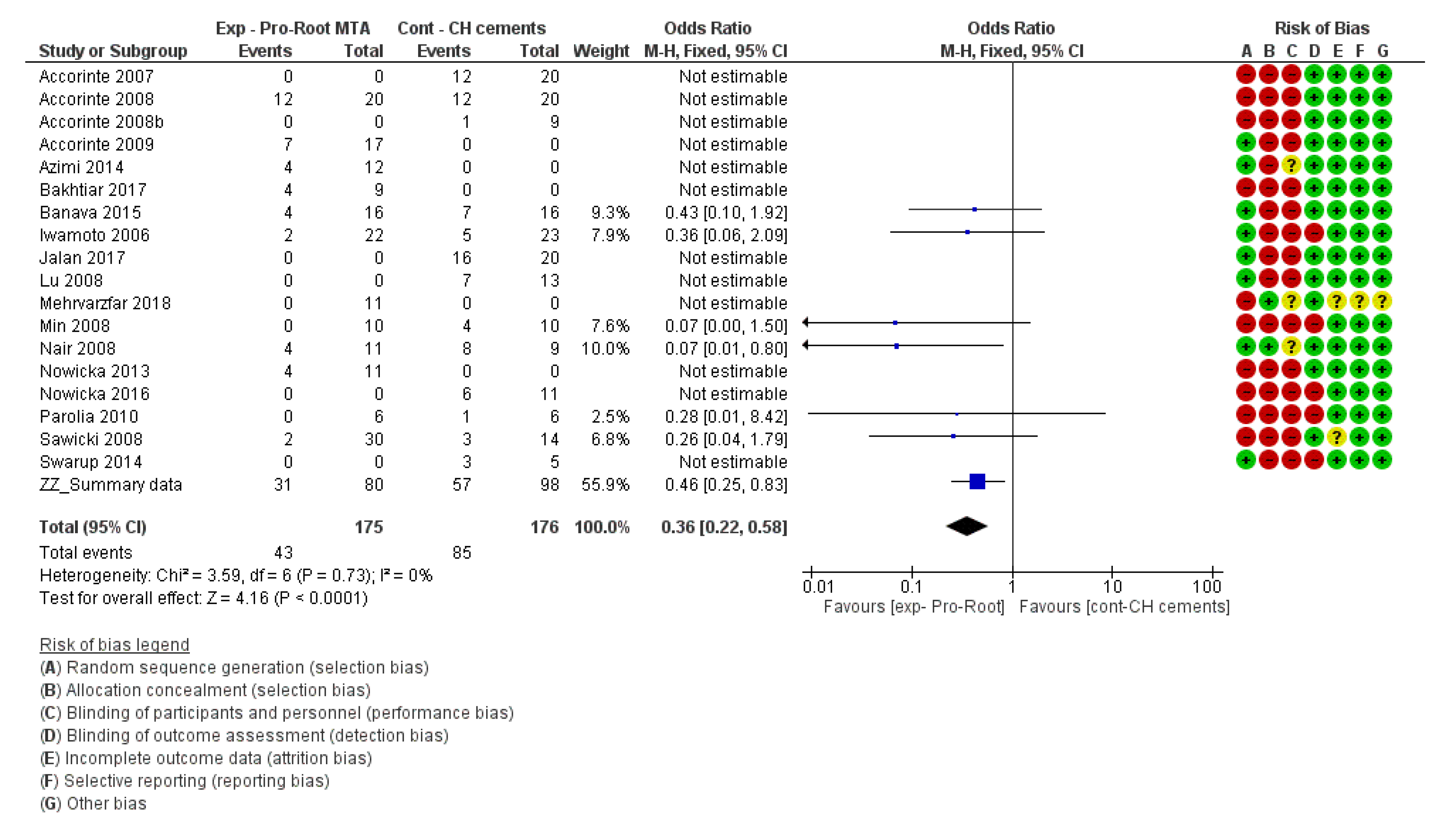
Meta-Analysis of the Effect of Pulp-Capping Materials on Hard-Tissue Formation upon Capping Exposed Human Pulp Tissue
3.4. Risk of Bias Across Studies
4. Discussion
4.1. Summary of Results
4.1.1. Systematic Review of In Vitro Studies
4.1.2. Systematic Review and Meta-Analysis of In Vivo Studies
Inflammatory Reaction
Complete Reparative Bridge Formation
4.2. Comparison with Previous Studies and Limitations
5. Conclusions and Recommendations for Future Research
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALP | Alkaline Phosphatase |
| ARS | Alizarin Red S |
| BMP-2 | Bone Morphogenetic Protein-2 |
| BSP | Bone Sialoprotein |
| CCK-8 | Cell Counting Kit-8 |
| Col I A1 | Collagen I A-1 |
| DMP-1 | Dentin Matrix acidic Phosphoprotein-1 |
| DSPP | Dentin Sialophosphoprotein |
| ELISA | Enzyme-Linked Immuno Sorbent Assay |
| FGF-2 | Fibroblast Growth Factor–2 |
| HO-1 | Heme Oxygenase-1 |
| IBSP | Bone Sialoprotein (gene name) |
| IL-8 | Interleukine-8 |
| MTS | Colorimetric assay based on the reduction of:3-(4,5-dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium |
| MTT | Colorimetric assay based on the reduction of:3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| OCN | Osteocalcin |
| ON | Osteonectin |
| OPN | Osteopontin |
| qRT-PCR | Quantitative Real Time–Polymerase Chain Reaction |
| RT-PCR | Real Time–Polymerase Chain Reaction |
| RunX-2 | Runt related transcription factor 2 |
| SEM | Scanning Electron Microscopy |
| SEM-EDX | Scanning Electron Microscope coupled with Electron Dispersive X-ray Spectroscopy |
| SPP1 | Osteopontin (gene name) |
| TEM | Transmission Electron Microscopy |
| VEGF | Vascular Endothelial Growth Factor |
| WST-1 | Water Soluble Tetrazolium salt–1–Colorimetric assay based on the reduction of:2-(4-Iodophenyl)-3-(4-nitrophenyl)-5-(2,4-disulfophenyl)-2H-tetrazolium, monosodium salt |
| XTT | Colorimetric assay based on the reduction of:2,3-Bis-(2-Methoxy-4-Nitro-5-Sulfophenyl)-2H-Tetrazolium-5-Carboxanilide |
References
- Pulp Capping and Pulpotomy Agents. 2020. Available online: https://www.ncbi.nlm.nih.gov/mesh?Db=mesh&Term=%22Dental%20Pulp%20Capping%20%22[MESH] (accessed on 15 May 2020).
- Olsson, H.; Petersson, K.; Rohlin, M. Formation of a Hard Tissue Barrier after Pulp Cappings in Humans. A Systematic Review. Int. Endod. J. 2006, 39, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Schröder, U. Effects of Calcium Hydroxide-Containing Pulp-Capping Agents on Pulp Cell Migration, Proliferation, and Differentiation. J. Dent. Res. 1985, 64, 541–548. [Google Scholar] [CrossRef] [PubMed]
- About, I. Dentin Regeneration in Vitro: The Pivotal Role of Supportive Cells. Adv. Dent. Res. 2011, 23, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, D.; Lamont, T.; Innes, N.P.T.; Kidd, E.; Clarkson, J.E. Operative Caries Management in Adults and Children. Cochrane Database Syst. Rev. 2013, 3, CD003808. [Google Scholar] [CrossRef]
- Schwendicke, F.; Frencken, J.E.; Bjørndal, L.; Maltz, M.; Manton, D.J.; Ricketts, D.; van Landuyt, K.; Banerjee, A.; Campus, G.; Doméjean, S.; et al. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv. Dent. Res. 2016, 28, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Bjorndal, L.; Fransson, H.; Bruun, G.; Markvart, M.; Kjaeldgaard, M.; Nasman, P.; Hedenbjork-Lager, A.; Dige, I.; Thordrup, M. Randomized Clinical Trials on Deep Carious Lesions: 5-Year Follow-Up. J. Dent. Res. 2017, 96, 747–753. [Google Scholar] [CrossRef]
- Dummer, P.M.H.; Franco, V.; Gambarini, G.; Orstavik, D.; Tjaderhane, L.; Whitworth, J.; Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; et al. European Society of Endodontology Position Statement: Management of Deep Caries and the Exposed Pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar]
- Ricucci, D.; Loghin, S.; Siqueira, J.F., Jr. Correlation between Clinical and Histologic Pulp Diagnoses. J. Endod. 2014, 40, 1932–1939. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Lin, L.M.; Spangberg, L.S.; Tay, F.R. Is Hard Tissue Formation in the Dental Pulp after the Death of the Primary Odontoblasts a Regenerative or a Reparative Process? J. Dent. 2014, 42, 1156–1170. [Google Scholar] [CrossRef]
- Taha, N.A.; Khazali, M.A. Partial Pulpotomy in Mature Permanent Teeth with Clinical Signs Indicative of Irreversible Pulpitis: A Randomized Clinical Trial. J. Endod. 2017, 43, 1417–1421. [Google Scholar] [CrossRef]
- Schwendicke, F.; Stotpe, M. Direct Pulp Capping after a Carious Exposure Versus Root Canal Treatment: A Cost-Effectiveness Analysis. J. Endod. 2014, 40, 1764–1770. [Google Scholar] [CrossRef]
- Darvell, B.W.; Wu, R.C.T. Mta-an Hydraulic Silicate Cement: Review Update and Setting Reaction. Dent. Mater. 2011, 27, 407–422. [Google Scholar] [CrossRef]
- Prati, C.; Gandolfi, M.G. Calcium Silicate Bioactive Cements: Biological Perspectives and Clinical Applications. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef]
- Lee, S.J.; Monsef, M.; Torabinejad, M. Sealing Ability of a Mineral Trioxide Aggregate for Repair of Lateral Root Perforations. J. Endod. 1993, 19, 541–544. [Google Scholar] [CrossRef]
- Hilton, T.J.; Ferracane, J.L.; Mancl, L. Comparison of Caoh with Mta for Direct Pulp Capping: A Pbrn Randomized Clinical Trial. J. Dent. Res. 2013, 92 (Suppl. S7), 16s–22s. [Google Scholar] [CrossRef] [Green Version]
- Mente, J.; Hufnagel, S.; Leo, M.; Michel, A.; Gehrig, H.; Panagidis, D.; Saure, D.; Pfefferle, T. Treatment Outcome of Mineral Trioxide Aggregate or Calcium Hydroxide Direct Pulp Capping: Long-Term Results. J. Endod. 2014, 40, 1746–1751. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral Trioxide Aggregate and Other Bioactive Endodontic Cements: An Updated Overview—Part I: Vital Pulp Therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Parirokh, M.; Torabinejad, M. Mineral Trioxide Aggregate: A Comprehensive Literature Review-Part Iii: Clinical Applications, Drawbacks, and Mechanism of Action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J.; Laurent, P.; About, I. Hydration of Biodentine, Theracal Lc, and a Prototype Tricalcium Silicate-Based Dentin Replacement Material after Pulp Capping in Entire Tooth Cultures. J. Endod. 2014, 40, 1846–1854. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Siboni, F.; Prati, C. Chemical-Physical Properties of Theracal, a Novel Light-Curable Mta-Like Material for Pulp Capping. Int. Endod. J. 2012, 45, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Sauro, S.; Babbar, A.; Gharibi, B.; Feitosa, V.P.; Carvalho, R.M.; Rodrigues, L.K.A.; Banerjee, A.; Watson, T. Cellular Differentiation, Bioactive and Mechanical Properties of Experimental Light-Curing Pulp Protection Materials. Dent. Mater. Off. Publ. Acad. Dent. Mate. 2018, 34, 868–878. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, S.B.; Collares, F.M.; Leitune, V.C.; Schneider, L.F.; Ogliari, F.A.; Petzhold, C.L.; Samuel, S.M. Influence of Hydroxyethyl Acrylamide Addition to Dental Adhesive Resin. Dent. Mater. 2015, 31, 1579–1586. [Google Scholar] [CrossRef]
- Rodrigues, S.B.; Petzhold, C.L.; Gamba, D.; Leitune, V.C.B.; Collares, F.M. Acrylamides and Methacrylamides as Alternative Monomers for Dental Adhesives. Dent. Mater. 2018, 34, 1634–1644. [Google Scholar] [CrossRef]
- Yoshihara, K.; Nagaoka, N.; Okihara, T.; Irie, M.; Matsukawa, A.; Pedano, M.S.; Maruo, Y.; Yoshida, Y.; van Meerbeek, B. Development of Self-Adhesive Pulp-Capping Agents Containing a Novel Hydrophilic and Highly Polymerizable Acrylamide Monomer. J. Mater. Chem. B 2000. [Google Scholar] [CrossRef]
- Meraji, N.; Camilleri, J. Bonding over Dentin Replacement Materials. J. Endod. 2017, 43, 1343–1349. [Google Scholar] [CrossRef]
- Giraud, T.; Jeanneau, C.; Bergmann, M.; Laurent, P.; About, I. Tricalcium Silicate Capping Materials Modulate Pulp Healing and Inflammatory Activity in Vitro. J. Endod. 2018, 44, 1686–1691. [Google Scholar] [CrossRef] [Green Version]
- Jeanneau, C.; Laurent, P.; Rombouts, C.; Giraud, T.; About, I. Light-Cured Tricalcium Silicate Toxicity to the Dental Pulp. J. Endod. 2017, 43, 2074–2080. [Google Scholar] [CrossRef]
- Schertl, P.; Volk, J.; Perduns, R.; Adam, K.; Leyhausen, G.; Bakopoulou, A.; Geurtsen, W. Impaired Angiogenic Differentiation of Dental Pulp Stem Cells During Exposure to the Resinous Monomer Triethylene Glycol Dimethacrylate. Dent. Mater. 2019, 35, 144–155. [Google Scholar] [CrossRef]
- Yu, L.; Katherine, D.; Lin, L. Polymer Blends and Composites from Renewable Resources. Prog. Polym. Sci. 2006, 31, 576–602. [Google Scholar] [CrossRef]
- Pillai, C.K.S. Challenges for Natural Monomers and Polymers: Novel Design Strategies and Engineering to Develop Advanced Polymers. Des. Monomers Polym. 2010, 13, 87–121. [Google Scholar] [CrossRef]
- Poulopoulou, N.; Smyrnioti, D.; Nikolaidis, G.N.; Tsitsimaka, I.; Christodoulou, E.; Bikiaris, D.N.; Charitopoulou, M.A.; Achilias, D.S.; Kapnisti, M.; Papageorgiou, G.Z. Sustainable Plastics from Biomass: Blends of Polyesters Based on 2,5-Furandicarboxylic Acid. Polymers 2020, 12, 225. [Google Scholar] [CrossRef] [Green Version]
- Steven-Friso, K.; Ruijten, D.; Trullemans, L.; Renders, T.; van Puyvelde, P.; Witters, H.; Sels, B.F. Regioselective Synthesis, Isomerisation, in Vitro Oestrogenic Activity, and Copolymerisation of Bisguaiacol F (Bgf) Isomers. Green Chem. 2019, 21, 6622–6633. [Google Scholar]
- Zamboulis, A.; Nakiou, E.A.; Christodoulou, E.; Bikiaris, D.N.; Kontonasaki, E.; Liverani, L.; Boccaccini, A.R. Polyglycerol Hyperbranched Polyesters: Synthesis, Properties and Pharmaceutical and Biomedical Applications. Int. J. Mol. Sci. 2019, 20, 6210. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Gillispie, G.J.; Copus, J.S.; Zhang, W.; Atala, A.; Yoo, J.J.; Yelick, P.C.; Lee, S.J. The Effect of Bmp-Mimetic Peptide Tethering Bioinks on the Differentiation of Dental Pulp Stem Cells (Dpscs) in 3d Bioprinted Dental Constructs. Biofabrication 2020. [Google Scholar] [CrossRef]
- Lizarraga Valderrama, L.D.R.; Nigmatullin, R.; Ladino, B.; Taylor, C.S.; Boccaccini, A.R.; Knowles, J.C.; Claeyssens, F.; Haycock, J.W.; Roy, I. Modulation of Neuronal Cell Affinity of Composites Scaffolds Based on Polyhydroxyalkanoates and Bioactive Glasses. Biomed. Mater. 2020. [Google Scholar] [CrossRef]
- Okamoto, M.; Matsumoto, S.; Sugiyama, A.; Kanie, K.; Watanabe, M.; Huang, H.; Ali, M.; Ito, Y.; Miura, J.; Hirose, Y.; et al. Performance of a Biodegradable Composite with Hydroxyapatite as a Scaffold in Pulp Tissue Repair. Polymers 2020, 12, 937. [Google Scholar] [CrossRef] [Green Version]
- Asgary, S.; Eghbal, M.J. Treatment Outcomes of Pulpotomy in Permanent Molars with Irreversible Pulpitis Using Biomaterials: A Multi-Center Randomized Controlled Trial. Acta Odontol. Scand. 2013, 71, 130–136. [Google Scholar] [CrossRef]
- Eghbal, M.J.; Asgary, S.; Baglue, R.A.; Parirokh, M.; Ghoddusi, J. Mta Pulpotomy of Human Permanent Molars with Irreversible Pulpitis. Aust. Endod. J. 2009, 35, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Eghbal, M.J.; Fazlyab, M.; Baghban, A.A.; Ghoddusi, J. Five-Year Results of Vital Pulp Therapy in Permanent Molars with Irreversible Pulpitis: A Non-Inferiority Multicenter Randomized Clinical Trial. Clin. Oral Investig. 2015, 19, 335–341. [Google Scholar] [CrossRef]
- Taha, N.A.; Ahmad, M.B.; Ghanim, A. Assessment of Mineral Trioxide Aggregate Pulpotomy in Mature Permanent Teeth with Carious Exposures. Int. Endod. J. 2017, 50, 117–125. [Google Scholar] [CrossRef]
- Caliskan, M.K. Pulpotomy of Carious Vital Teeth with Periapical Involvement. Int. Endod. J. 1995, 28, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S. Calcium-Enriched Mixture Pulpotomy of a Human Permanent Molar with Irreversible Pulpitis and Condensing Apical Periodontitis. J. Conserv. Dent. 2011, 14, 90–93. [Google Scholar] [CrossRef] [Green Version]
- Asgary, S.; Eghbal, M.J.; Bagheban, A.A. Long-Term Outcomes of Pulpotomy in Permanent Teeth with Irreversible Pulpitis: A Multi-Center Randomized Controlled Trial. Am. J. Dent. 2017, 30, 151–155. [Google Scholar] [PubMed]
- Ricucci, D.; Siqueira, J.F., Jr.; Li, Y.; Tay, F.R. Vital Pulp Therapy: Histopathology and Histobacteriology-Based Guidelines to Treat Teeth with Deep Caries and Pulp Exposure. J. Dent. 2019, 86, 41–52. [Google Scholar] [CrossRef]
- Schwendicke, F.; Brouwer, F.; Schwendicke, A.; Paris, S. Different Materials for Direct Pulp Capping: Systematic Review and Meta-Analysis and Trial Sequential Analysis. Clin. Oral Investig. 2016, 20, 1121–1132. [Google Scholar] [CrossRef]
- Sangwan, P.; Sangwan, A.; Duhan, J.; Rohilla, A. Tertiary Dentinogenesis with Calcium Hydroxide: A Review of Proposed Mechanisms. Int. Endod. J. 2013, 46, 3–19. [Google Scholar] [CrossRef]
- Emara, R.; Elhennawy, K.; Schwendicke, F. Effects of Calcium Silicate Cements on Dental Pulp Cells: A Systematic Review. J. Dent. 2018, 77, 18–36. [Google Scholar] [CrossRef]
- Paula, A.B.; Laranjo, M.; Marto, C.M.; Paulo, S.; Abrantes, A.M.; Casalta-Lopes, J.; Marques-Ferreira, M.; Botelho, M.F.; Carrilho, E. Direct Pulp Capping: What Is the Most Effective Therapy?-Systematic Review and Meta-Analysis. J. Evid. Based. Dent. Pract. 2018, 18, 298–314. [Google Scholar] [CrossRef]
- Li, Z.; Cao, L.; Fan, M.; Xu, Q. Direct Pulp Capping with Calcium Hydroxide or Mineral Trioxide Aggregate: A Meta-Analysis. J. Endod. 2015, 41, 1412–1417. [Google Scholar] [CrossRef]
- Sanz, J.L.; Forner, L.; Almudéver, A.; Guerrero-Gironés, J.; Llena, C. Viability and Stimulation of Human Stem Cells from the Apical Papilla (Hscaps) Induced by Silicate-Based Materials for Their Potential Use in Regenerative Endodontics: A Systematic Review. Materials 2020, 13, 974. [Google Scholar] [CrossRef] [Green Version]
- Accorinte, M.L.R.; Loguercio, A.D.; Reis, A.; Carneiro, E.; Grande, R.H.M.; Murata, S.S.; Holland, R. Response of Human Dental Pulp Capped with Mta and Calcium Hydroxide Powder. Oper Dent. 2008, 33, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Accorinte, M.D.R.; Holland, R.; Reis, A.; Bortoluzzi, M.C.; Murata, S.S.; Dezan, E.; Souza, V.; Alessandro, L.D. Evaluation of Mineral Trioxide Aggregate and Calcium Hydroxide Cement as Pulp-Capping Agents in Human Teeth. J. Endod. 2008, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The Prisma Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The Prisma Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alliotlicht, B.; Jean, A.; Gregoire, M. Comparative Effect of Calcium Hydroxide and Hydroxyapatite on the Cellular-Activity of Human Pulp Fibroblasts in-Vitro. Arch. Oral Biol. 1994, 39, 481–489. [Google Scholar] [CrossRef]
- Min, K.S.; Chang, H.S.; Bae, J.M.; Park, S.H.; Hong, C.U.; Kim, E.C. The Induction of Heme Oxygenase-1 Modulates Bismuth Oxide-Induced Cytotoxicity in Human Dental Pulp Cells. J. Endod. 2007, 33, 1342–1346. [Google Scholar] [CrossRef]
- Min, K.S.; Kim, H.I.; Park, H.J.; Pi, S.H.; Hong, C.U.; Kim, E.C. Human Pulp Cells Response to Portland Cement in Vitro. J. Endod. 2007, 33, 163–166. [Google Scholar] [CrossRef]
- Laurent, P.; Camps, J.; de Meo, M.; Dejou, J.; About, I. Induction of Specific Cell Responses to a Ca(3)Sio(5)-Based Posterior Restorative Material. Dent. Mater. 2008, 24, 1486–1494. [Google Scholar] [CrossRef]
- Min, K.S.; Lee, S.I.; Lee, Y.; Kim, E.C. Effect of Radiopaque Portland Cement on Mineralization in Human Dental Pulp Cells. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e82–e86. [Google Scholar] [CrossRef]
- Lee, J.B.; Park, S.J.; Kim, H.H.; Kwon, Y.S.; Lee, K.W.; Min, K.S. Physical Properties and Biological/Odontogenic Effects of an Experimentally Developed Fast-Setting Alpha-Tricalcium Phosphate-Based Pulp Capping Material. BMC Oral Health 2014, 14, 87. [Google Scholar] [CrossRef] [Green Version]
- Bortoluzzi, E.A.; Niu, L.N.; Palani, C.D.; El-Awady, A.R.; Hammond, B.D.; Pei, D.D.; Tian, F.C.; Cutler, C.W.; Pashley, D.H.; Tay, F.R. Cytotoxicity and Osteogenic Potential of Silicate Calcium Cements as Potential Protective Materials for Pulpal Revascularization. Dent. Mater. 2015, 31, 1510–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, L.N.; Watson, D.; Thames, K.; Primus, C.M.; Bergeron, B.E.; Jiao, K.; Bortoluzzi, E.A.; Cutler, C.W.; Chen, J.H.; Pashley, D.H.; et al. Effects of a Discoloration-Resistant Calcium Aluminosilicate Cement on the Viability and Proliferation of Undifferentiated Human Dental Pulp Stem Cells. Sci. Rep. 2015, 5, 17177. [Google Scholar] [CrossRef] [PubMed]
- Oncel Torun, Z.; Torun, D.; Demirkaya, K.; Yavuz, S.T.; Elci, M.P.; Sarper, M.; Avcu, F. Effects of Iroot Bp and White Mineral Trioxide Aggregate on Cell Viability and the Expression of Genes Associated with Mineralization. Int. Endod. J. 2015, 48, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhu, L.X.; Cheng, X.; Lin, Y.; Yan, P.; Peng, B. Promotion of Dental Pulp Cell Migration and Pulp Repair by a Bioceramic Putty Involving Fgfr-Mediated Signaling Pathways. J. Dent. Res. 2015, 94, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.J.; Kim, E.; Song, M.; Park, J.W.; Shin, S.J. Effects of Two Fast-Setting Calcium-Silicate Cements on Cell Viability and Angiogenic Factor Release in Human Pulp-Derived Cells. Odontology 2016, 104, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Daltoe, M.O.; Paula-Silva, F.W.; Faccioli, L.H.; Gaton-Hernandez, P.M.; de Rossi, A.; Silva, L.A.B. Expression of Mineralization Markers During Pulp Response to Biodentine and Mineral Trioxide Aggregate. J. Endod. 2016, 42, 596–603. [Google Scholar] [CrossRef] [Green Version]
- Widbiller, M.; Lindner, S.R.; Buchalla, W.; Eidt, A.; Hiller, K.A.; Schmalz, G.; Galler, K.M. Three-Dimensional Culture of Dental Pulp Stem Cells in Direct Contact to Tricalcium Silicate Cements. Clin. Oral Investig. 2016, 20, 237–246. [Google Scholar] [CrossRef]
- Jun, S.K.; Lee, J.H.; Lee, H.H. The Biomineralization of a Bioactive Glass-Incorporated Light-Curable Pulp Capping Material Using Human Dental Pulp Stem Cells. Biomed Res. Int. 2017, 2017, 2495282. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.N.; Lee, B.G.; Chang, H.S.; Hwang, Y.C.; Hwang, I.N.; Oh, W.M. Effects of a Novel Light-Curable Material on Odontoblastic Differentiation of Human Dental Pulp Cells. Int. Endod. J. 2017, 50, 464–471. [Google Scholar] [CrossRef]
- Mestieri, L.B.; Gomes-Cornelio, A.L.; Rodrigues, E.M.; Faria, G.M.; Guerreiro-Tanomaru, J.; Tanomaru-Filho, M. Cytotoxicity and Bioactivity of Calcium Silicate Cements Combined with Niobium Oxide in Different Cell Lines. Braz. Dent. J. 2017, 28, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, E.M.; Cornelio, A.L.G.; Mestieri, L.B.; Fuentes, A.S.C.; Salles, L.P.; Rossa-Junior, C.; Faria, G.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M. Human Dental Pulp Cells Response to Mineral Trioxide Aggregate (Mta) and Mta Plus: Cytotoxicity and Gene Expression Analysis. Int. Endod. J. 2017, 50, 780–789. [Google Scholar] [CrossRef]
- Sun, Y.; Luo, T.; Shen, Y.; Haapasalo, M.; Zou, L.; Liu, J. Effect of Iroot Fast Set Root Repair Material on the Proliferation, Migration and Differentiation of Human Dental Pulp Stem Cells in Vitro. PLoS ONE 2017, 12, e0186848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomas-Catala, C.J.; Collado-Gonzalez, M.; Garcia-Bernal, D.; Onate-Sanchez, R.E.; Forner, L.; Llena, C.; Lozano, A.; Castelo-Baz, P.; Moraleda, J.M.; Rodriguez-Lozano, F.J. Comparative Analysis of the Biological Effects of the Endodontic Bioactive Cements Mta-Angelus, Mta Repair Hp and Neomta Plus on Human Dental Pulp Stem Cells. Int. Endod. J. 2017, 50 (Suppl. S2), e63–e72. [Google Scholar] [CrossRef] [Green Version]
- Collado-Gonzalez, M.; Pecci-Lloret, M.R.; Tomas-Catala, C.J.; Garcia-Bernal, D.; Onate-Sanchez, R.E.; Llena, C.; Forner, L.; Rosa, V.; Rodriguez-Lozano, F.J. Thermo-Setting Glass Ionomer Cements Promote Variable Biological Responses of Human Dental Pulp Stem Cells. Dent. Mater. 2018, 34, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Pedano, M.S.; Li, X.; Li, S.; Sun, Z.; Cokic, S.M.; Putzeys, E.; Yoshihara, K.; Yoshida, Y.; Chen, Z.; van Landuyt, K.; et al. Freshly-Mixed and Setting Calcium-Silicate Cements Stimulate Human Dental Pulp Cells. Dent. Mater. 2018, 34, 797–808. [Google Scholar] [CrossRef]
- Tomas-Catala, C.J.; Collado-Gonzalez, M.; Garcia-Bernal, D.; Onate-Sanchez, R.E.; Forner, L.; Llena, C.; Lozano, A.; Moraleda, J.M.; Rodriguez-Lozano, F.J. Biocompatibility of New Pulp-Capping Materials Neomta Plus, Mta Repair Hp, and Biodentine on Human Dental Pulp Stem Cells. J. Endod. 2018, 44, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.M.; Kim, S.Y.; Kim, J.H.; Jun, S.K.; Kim, H.W.; Lee, J.H.; Lee, H.H. Depth-Dependent Cellular Response from Dental Bulk-Fill Resins in Human Dental Pulp Stem Cells. Stem Cells Int. 2019, 2019, 1251536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Garcia, S.; Pecci-Lloret, M.P.; Pecci-Lloret, M.R.; Onate-Sanchez, R.E.; Garcia-Bernal, D.; Castelo-Baz, P.; Rodriguez-Lozano, F.J.; Guerrero-Girones, J. In Vitro Evaluation of the Biological Effects of Activa Kids Bioactive Restorative, Ionolux, and Riva Light Cure on Human Dental Pulp Stem Cells. Materials 2019, 12, 3694. [Google Scholar] [CrossRef] [Green Version]
- Dou, L.; Yan, Q.; Yang, D. Effect of Five Dental Pulp Capping Agents on Cell Proliferation, Viability, Apoptosis and Mineralization of Human Dental Pulp Cells. Exp. Ther. Med. 2020, 19, 2377–2383. [Google Scholar] [CrossRef]
- Hebling, J.; Giro, E.M.A.; Costa, C.A.D. Biocompatibility of an Adhesive System Applied to Exposed Human Dental Pulp. J. Endod. 1999, 25, 676–682. [Google Scholar] [CrossRef]
- Do Nascimento, A.B.L.; Fontana, U.F.; Teixeira, H.M.; Costa, C.A.D. Biocompatibility of a Resin-Modified Glass-Ionomer Cement Applied as Pulp Capping in Human Teeth. Am. J. Dent. 2000, 13, 28–34. [Google Scholar] [PubMed]
- Costa, C.A.D.; Nascimento, A.B.L.d.; Teixeira, H.M.; Fontana, U.F. Response of Human Pulps Capped with a Self-Etching Adhesive System. Dent. Mater. 2001, 17, 230–240. [Google Scholar] [CrossRef]
- Ersin, N.K.; Eronat, N. The Comparison of a Dentin Adhesive with Calcium Hydroxide as a Pulp-Capping Agent on the Exposed Pulps of Human and Sheep Teeth. Quintessence Int. 2005, 36, 271–280. [Google Scholar]
- Olsson, H.; Davies, J.R.; Holst, K.E.; Schroder, U.; Petersson, K. Dental Pulp Capping: Effect of Emdogain Gel on Experimentally Exposed Human Pulps. Int. Endod. J. 2005, 38, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.A.B.; Lanza, L.D.; Lopes, N., Jr.; Moreira, A.; Alves, J.B. Direct Pulp Capping with a Dentin Bonding System in Human Teeth: A Clinical and Histological Evaluation. Oper. Dent. 2006, 31, 297–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawicki, L.; Pameijer, C.H.; Emerich, K.; Adamowicz-Klepalska, B. Histological Evaluation of Mineral Trioxide Aggregate and Calcium Hydroxide in Direct Pulp Capping of Human Immature Permanent Teeth. Am. J. Dent. 2008, 21, 262–266. [Google Scholar] [PubMed]
- Azimi, S.; Fazlyab, M.; Sadri, D.; Saghiri, M.A.; Khosravanifard, B.; Asgary, S. Comparison of Pulp Response to Mineral Trioxide Aggregate and a Bioceramic Paste in Partial Pulpotomy of Sound Human Premolars: A Randomized Controlled Trial. Int. Endod. J. 2014, 47, 873–881. [Google Scholar] [CrossRef]
- Swarup, S.J.; Rao, A.; Boaz, K.; Srikant, N.; Shenoy, R. Pulpal Response to Nano Hydroxyapatite, Mineral Trioxide Aggregate and Calcium Hydroxide When Used as a Direct Pulp Capping Agent: An in Vivo Study. J. Clin. Pediatr. Dent. 2014, 38, 201–206. [Google Scholar] [CrossRef]
- Banava, S.; Fazlyab, M.; Heshmat, H.; Mojtahedzadeh, F.; Motahhary, P. Histological Evaluation of Single and Double-Visit Direct Pulp Capping with Different Materials on Sound Human Premolars: A Randomized Controlled Clinical Trial. Iran. Endod. J. 2015, 10, 82–88. [Google Scholar]
- Demarco, F.F.; Tarquinio, S.B.; Jaeger, M.M.; de Araújo, V.C.; Matson, E. Pulp Response and Cytotoxicity Evaluation of 2 Dentin Bonding Agents. Quintessence Int. (Berlin, Germany: 1985) 2001, 32, 211–220. [Google Scholar]
- Accorinte Mde, L.; Loguercio, A.D.; Reis, A.; Muench, A.; de Araujo, V.C. Adverse Effects of Human Pulps after Direct Pulp Capping with the Different Components from a Total-Etch, Three-Step Adhesive System. Dent. Mater. 2005, 21, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Accorinte, M.D.L.R.; Reis, A.; Loguercio, A.D.; de Araújo, V.C.; Muench, A. Influence of Rubber Dam Isolation on Human Pulp Responses after Capping with Calcium Hydroxide and an Adhesive System. Quintessence Int. 2006, 37, 205–212. [Google Scholar]
- Iwamoto, C.E.; Adachi, E.; Pameijer, C.H.; Barnes, D.; Romberg, E.E.; Jefferies, S. Clinical and Histological Evaluation of White Proroot Mta in Direct Pulp Capping. Am. J. Dent. 2006, 19, 85–90. [Google Scholar] [PubMed]
- Accorinte, M.D.R.; Loguercio, A.D.; Reis, A.; Holland, R. Effects of Hemostatic Agents on the Histomorphologic Response of Human Dental Pulp Capped with Calcium Hydroxide. Quintessence Int. 2007, 38, 843–852. [Google Scholar]
- Elias, R.V.; Demarco, F.F.; Tarquinio, S.B.; Piva, E. Pulp Responses to the Application of a Self-Etching Adhesive in Human Pulps after Controlling Bleeding with Sodium Hypochlorite. Quintessence Int. 2007, 38, e67–e77. [Google Scholar] [PubMed]
- Accorinte, M.L.R.; Loguercio, A.D.; Reis, A.; Costa, C.A.S. Response of Human Pulps Capped with Different Self-Etch Adhesive Systems. Clin. Oral Investig. 2008, 12, 119–127. [Google Scholar] [CrossRef]
- Lu, Y.; Liu, T.; Li, H.; Pi, G. Histological Evaluation of Direct Pulp Capping with a Self-Etching Adhesive and Calcium Hydroxide on Human Pulp Tissue. Int. Endod. J. 2008, 41, 643–650. [Google Scholar] [CrossRef]
- Min, K.S.; Park, H.J.; Lee, S.K.; Park, S.H.; Hong, C.U.; Kim, H.W.; Lee, H.H.; Kim, E.C. Effect of Mineral Trioxide Aggregate on Dentin Bridge Formation and Expression of Dentin Sialoprotein and Heme Oxygenase-1 in Human Dental Pulp. J. Endod. 2008, 34, 666–670. [Google Scholar] [CrossRef]
- Nair, P.N.R.; Duncan, H.F.; Ford, T.R.P.; Luder, H.U. Histological, Ultrastructural and Quantitative Investigations on the Response of Healthy Human Pulps to Experimental Capping with Mineral Trioxide Aggregate: A Randomized Controlled Trial. Int. Endod. J. 2008, 41, 128–150. [Google Scholar]
- Accorinte, M.L.; Loguercio, A.D.; Reis, A.; Bauer, J.R.; Grande, R.H.; Murata, S.S.; Souza, V.; Holland, R. Evaluation of Two Mineral Trioxide Aggregate Compounds as Pulp-Capping Agents in Human Teeth. Int. Endod. J. 2009, 42, 122–128. [Google Scholar] [CrossRef]
- Kiatwateeratana, T.; Kintarak, S.; Piwat, S.; Chankanka, O.; Kamaolmatyakul, S.; Thearmontree, A. Partial Pulpotomy on Caries-Free Teeth Using Enamel Matrix Derivative or Calcium Hydroxide: A Randomized Controlled Trial. Int. Endod. J. 2009, 42, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Parolia, A.; Kundabala, M.; Rao, N.N.; Acharya, S.R.; Agrawal, P.; Mohan, M.; Thomas, M. A Comparative Histological Analysis of Human Pulp Following Direct Pulp Capping with Propolis, Mineral Trioxide Aggregate and Dycal. Aust. Dent. J. 2010, 55, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, A.; Lipski, M.; Parafiniuk, M.; Sporniak-Tutak, K.; Lichota, D.; Kosierkiewicz, A.; Kaczmarek, W.; Buczkowska-Radlinska, J. Response of Human Dental Pulp Capped with Biodentine and Mineral Trioxide Aggregate. J. Endod. 2013, 39, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, A.; Lagocka, R.; Lipski, M.; Parafiniuk, M.; Grocholewicz, K.; Sobolewska, E.; Witek, A.; Buczkowska-Radlinska, J. Clinical and Histological Evaluation of Direct Pulp Capping on Human Pulp Tissue Using a Dentin Adhesive System. Biomed Res. Int. 2016, 2016, 2591273. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiar, H.; Nekoofar, M.H.; Aminishakib, P.; Abedi, F.; Moosavi, F.N.; Esnaashari, E.; Azizi, A.; Esmailian, S.; Ellini, M.R.; Mesgarzadeh, V.; et al. Human Pulp Responses to Partial Pulpotomy Treatment with Theracal as Compared with Biodentine and Proroot Mta: A Clinical Trial. J. Endod. 2017, 43, 1786–1791. [Google Scholar] [CrossRef]
- Jalan, A.L.; Warhadpande, M.M.; Dakshindas, D.M. A Comparison of Human Dental Pulp Response to Calcium Hydroxide and Biodentine as Direct Pulp-Capping Agents. J. Conserv. Dent. 2017, 20, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Mehrvarzfar, P.; Abbott, P.V.; Mashhadiabbas, F.; Vatanpour, M.; Savadkouhi, S.T. Clinical and Histological Responses of Human Dental Pulp to Mta and Combined Mta/Treated Dentin Matrix in Partial Pulpotomy. Aust. Endod. J. 2018, 44, 46–53. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version. 6.0.; Cochrane: London, UK, 2019. [Google Scholar]
- The Cochrane Collaboration. Review Manager (Revman) [Computer Program]. Version 5.3.; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What Is Quality of Evidence and Why Is It Important to Clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Accorinte Mde, L.; Loguercio, A.D.; Reis, A.; Muench, A.; de Araujo, V.C. Response of Human Pulp Capped with a Bonding Agent after Bleeding Control with Hemostatic Agents. Oper. Dent. 2005, 30, 147–155. [Google Scholar] [PubMed]
- Fransson, H.; Petersson, K.; Davies, J.R. Dentine Sialoprotein and Collagen I Expression after Experimental Pulp Capping in Humans Using Emdogain (R) Gel. Int. Endod. J. 2011, 44, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Madani, Z.S.; Haddadi, A.; Mesgarani, A.; Seyedmajidi, M.; Mostafazadeh, A.; Bijani, A.; Ashraphpour, M. Histopathologic Responses of the Dental Pulp to Calcium-Enriched Mixture (Cem) and Mineral Trioxide Aggregate (Mta) in Diabetic and Non-Diabetic Rats. Int. J. Mol. Cell. Med. 2014, 3, 263–271. [Google Scholar] [PubMed]
- Leite, M.F.; Ganzerla, E.; Marques, M.M.; Nicolau, J. Diabetes Induces Metabolic Alterations in Dental Pulp. J. Endod. 2008, 34, 1211–1214. [Google Scholar] [CrossRef]
- Kakehashi, S.; Stanley, H.R.; Fitzgerald, R.J. The Effects of Surgical Exposures of Dental Pulps in Germ-Free and Conventional Laboratory Rats. Oral Surg. Oral Med. Oral Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef]
- Nyborg, H. Healing Processes in the Pulp on Capping; a Morphologic Study; Experiments on Surgical Lesions of the Pulp in Dog and Man. Acta Odontol. Scand. 1955, 13 (Suppl. S16), 1–130. [Google Scholar]
- Martignoni, M.; Groothuis, G.M.; de Kanter, R. Species Differences between Mouse, Rat, Dog, Monkey and Human Cyp-Mediated Drug Metabolism, Inhibition and Induction. Expert Opin. Drug Metab. Toxicol. 2006, 2, 875–894. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Siqueira, J.F.; Ricucci, D.; Siqueira, J.F., Jr. Pulp Response to Caries and Restorative Procedures. In Endodontology: An Integrated Biological and Clinical View; Edizioni Martina: Bologna, Italy, 2013. [Google Scholar]
- Schweikl, H.; Spagnuolo, G.; Schmalz, G. Genetic and Cellular Toxicology of Dental Resin Monomers. J. Dent. Res. 2006, 85, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Caldas, I.P.; Alves, G.G.; Barbosa, I.B.; Scelza, P.; de Noronha, F.; Scelza, M.Z. In Vitro Cytotoxicity of Dental Adhesives: A Systematic Review. Dent. Mater. 2019, 35, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Van Landuyt, K.L.; Krifka, S.; Hiller, K.A.; Bolay, C.; Waha, C.; van Meerbeek, B.; Schmalz, G.; Schweikl, H. Evaluation of Cell Responses toward Adhesives with Different Photoinitiating Systems. Dent. Mater. 2015, 31, 916–927. [Google Scholar] [CrossRef]
- Schneider, T.R.; Hakami-Tafreshi, R.; Tomasino-Perez, A.; Tayebi, L.; Lobner, D. Effects of Dental Composite Resin Monomers on Dental Pulp Cells. Dent. Mater. J. 2019, 38, 579–583. [Google Scholar] [CrossRef] [Green Version]
- Costa, C.A.D.; Teixeira, H.M.; Nascimento, A.B.L.d.; Hebling, J. Biocompatibility of an Adhesive System and 2-Hydroxyethylmethacrylate. J. Dent. Child. 1999, 66, 337–342. [Google Scholar]
- Teixeira, H.M.; Nascimento, A.B.L.D.; Hebling, J.; Costa, C.A.D. In Vivo Evaluation of the Biocompatibility of Three Current Bonding Agents. J. Oral Rehabil. 2006, 33, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D. Patologia E Clinica Endodontica; Edizione Martina: Bologna, Italy, 2009. [Google Scholar]
- Bjorndal, L.; Reit, C.; Bruun, G.; Markvart, M.; Kjaeldgaard, M.; Nasman, P.; Thordrup, M.; Dige, I.; Nyvad, B.; Fransson, H.; et al. Treatment of Deep Caries Lesions in Adults: Randomized Clinical Trials Comparing Stepwise Vs. Direct Complete Excavation, and Direct Pulp Capping Vs. Partial Pulpotomy. Eur. J. Oral Sci. 2010, 118, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Barthel, C.R.; Rosenkranz, B.; Leuenberg, A.; Roulet, J.F. Pulp Capping of Carious Exposures: Treatment Outcome after 5 and 10 Years: A Retrospective Study. J. Endod. 2000, 26, 525–528. [Google Scholar] [CrossRef]
- Holland, R.; de Souza, V.; de Mello, W.; Nery, M.J.; Bernabe, P.F.; Filho, J.A.O. Healing Process after Pulpotomy and Covering with Calcium Hydroxide, Dycal or Mpc. Histological Study in Dog Teeth. Rev. Fac. Odontol. Aracatuba 1978, 7, 185–191. [Google Scholar] [PubMed]
- Holland, R.; de Mello, W.; Nery, M.J.; de Souza, V.; Bernabe, P.F.; Filho, J.A.O. Healing Process of Dog Dental Pulp after Pulpotomy and Pulp Covering with Calcium Hydroxide in Powder or Paste Form. Acta Odontol. Pediatr. 1981, 2, 47–51. [Google Scholar] [PubMed]
- Nowicka, A.; Wilk, G.; Lipski, M.; Kolecki, J.; Buczkowska-Radlinska, J. Tomographic Evaluation of Reparative Dentin Formation after Direct Pulp Capping with Ca(Oh)2, Mta, Biodentine, and Dentin Bonding System in Human Teeth. J. Endod. 2015, 41, 1234–1240. [Google Scholar] [CrossRef]
- Glass, R.L.; Zander, H.A. Pulp Healing. J. Dent. Res. 1949, 28, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Dammaschke, T. The History of Direct Pulp Capping. J. Hist. Dent. 2008, 56, 9–23. [Google Scholar] [PubMed]
- Shovelton, D.S.; Friend, L.A.; Kirk, E.E.; Rowe, A.H. The Efficacy of Pulp Capping Materials. A Comparative Trial. Br. Dent. J. 1971, 130, 385–391. [Google Scholar] [CrossRef]
- Sanz, J.L.; Rodríguez-Lozano, F.J.; Llena, C.; Sauro, S.; Forner, L. Bioactivity of Bioceramic Materials Used in the Dentin-Pulp Complex Therapy: A Systematic Review. Materials 2019, 12, 1015. [Google Scholar] [CrossRef] [Green Version]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; et al. Nonrestorative Treatments for Caries: Systematic Review and Network Meta-Analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Briso, A.L.F.; Rahal, V.; Mestrener, S.R.; Dezan, E., Jr. Biological Response of Pulps Submitted to Different Capping Materials. Braz. Oral Res. 2006, 20, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gronthos, S.; Mankani, M.; Brahim, J.; Robey, P.G.; Shi, S. Postnatal Human Dental Pulp Stem Cells (Dpscs) in Vitro and in Vivo. Proc. Natl. Acad. Sci. USA 2000, 97, 13625–13630. [Google Scholar] [CrossRef] [Green Version]
- About, I.; Bottero, M.J.; de Denato, P.; Camps, J.; Franquin, J.C.; Mitsiadis, T.A. Human Dentin Production in Vitro. Exp. Cell Res. 2000, 258, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- About, I.; Laurent-Maquin, D.; Lendahl, U.; Mitsiadis, T.A. Nestin Expression in Embryonic and Adult Human Teeth under Normal and Pathological Conditions. Am. J. Pathol. 2000, 157, 287–295. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eligibility criteria for in vitro studies | ||
| Characteristics | Inclusion Criteria | Exclusion Criteria |
| Publication year | Studies published from 1993 | Studies published before 1993 |
| Language | English | Other languages different than English |
| Population | Human dental pulp cells from a primary source Cells from more than 1 patient | Other type of oral/dental cells or cells not from primary source (i.e.,: immortalized cells, commercial cell lines, …) Cells obtained from one single patient |
| Tests performed | At least 2 different tests were performed | Only 1 test was performed (i.e.,: cytotoxicity, mineralization ability, ...) |
| Materials tested | Commercially available materials Resin-based or resin-free pulp-capping materials | Experimental materials or modification of an existing material Materials for other purposes (sealers, fixation cements, monomers, …) |
| Analysis | At least 2 different materials compared between each other | Materials compared only to the control |
| Eligibility criteria for in vivo studies | ||
| Publication year | Studies published from 1993 | Studies published before 1993 |
| Language | English | Other languages different than English |
| Ethical Committee | Mentioned | No ethical committee mentioned in the text |
| Population | Permanent teeth Healthy teeth (free from caries or infection) Patients’ age and amount of teeth should be provided | Primary teeth Teeth exhibiting caries or periodontal disease Sample size and age of the participants not mentioned |
| Materials tested | Commercially available materials Resin-based or resin-free pulp-capping materials Clear description and brand of the materials used | Experimental materials or modification of an existing material Materials for other purposes (sealers, fixation cements, monomers, …) No clear description and brand of the materials used |
| Analysis | Histology Inflammation and hard-tissue formation | Studies where “only” clinical parameters were evaluated No bridge formation evaluated |
| Type of study | Randomized or controlled clinical trials (RCT or CCT) | Other type of studies (case reports, case series, …) |
| Studies | Materials | Type of Exposure | Parameters | Methods | Results |
| Alliot-Licht et al. (1994) [56] | Calcium hydroxide (CH) Hydroxyapatite (HAp) | CH particles sterilized by heating (180 °C-1 h); direct contact (materials powder in culture medium) | Cell morphology | Light microscopy (at 3 & 5 days) | CH inhibited pulp fibroblasts growth (<cell density than control; subjective observation) HAp did not affect the cell density (≈cell density as the control; subjective observation) |
| Phagocytotic activity | SEM (at day 5) | Close contact of CH particles with fibroblasts’ membrane. HAp particles were closely bound to cell membrane or internalized by the cells. | |||
| TEM (at day 5) | Cells cultured in the presence of CH exhibited ghost cells and electron-dense spherical vesicles in the cytoplasm of living cells. TEM revealed HAp particles within the cells. | ||||
| Cell proliferation | DNA synthesis (at 1, 2, 3 & 4 days) | CH and HAp delayed the proliferation of cells at all time points. | |||
| Protein synthetic activity (at 6 days) | CH < incorporation of [3H]-leucine and [3H]-proline by pulp fibroblasts at day 6. HAp > incorporation of [3H]-leucine and [3H]-proline by the pulp fibroblasts at day 6. | ||||
| Cell differentiation | ALP activity (at 8 days for CH; at 5 & 8 days for HAp) | CH inhibited ALP activity of pulp fibroblasts at day 8. HAp inhibited ALP activity of pulp fibroblasts at 5 and 8 days. | |||
| Min et al. (2007) [57] | Portland cement (PC) Portland cement with bismuth oxide (BPC) | Indirect contact (SET materials) | Cell viability | MTT assay (at 12, 24, 48 & 72 h) | PC > BPC at 12 and 24 h PC ≈ BPC at 48 and 72 h |
| Nitric oxide production | Griess reaction(at 12, 24, 48 & 72 h) | BPC > nitrite production than PC at 12 and 24 h. PC ≈ BPC nitrite production at 48 and 72 h. | |||
| Ho-1 and iNOS | RT-PCR (at 12, 24, 48 & 72 h) | Ho-1: PC < BPC at all study periods iNOS: PC < BPC at all study points | |||
| Min et al. (2007) [58] | Portland cement (PC) Fuji-II LC (Fuji-II, GC) Zinc-oxide Eugenol (IRM; Dentsply-Sirona) CH cement Dycal (Dentsply-Sirona) | Direct and indirect contact (SET materials) | Cell morphology | SEM (at 24 h) | PC: showed flattened cells close to one another and spreading across the substrate. Fuji-II, IRM, and Dycal: no living cells were seen. |
| Cell viability | MTT assay (at 12, 24, 48 & 72 h) | PC ≈ control at all study periods. PC > Fuji-II, Dycal and IRM at all study periods. Control > Fuji II LC, IRM, and Dycal at all study points. | |||
| Cell differentiation | RT-PCR (ON, DSPP) (at 7 days) | ON: PC ≈ positive control group. DSPP: PC stimulated mineralization but less than the positive control. | |||
| Laurent et al. (2008) [59] | Ca3SiO5 cement (CS) Dycal (Dentsply-Sirona) Pro-Root MTA (MTA; Dentsply-Sirona) | Indirect contact * (SET materials) [ISO-Standard–(Nr. Not mentioned)] | Cell viability | MTT assay (at 24 h) | No contact (disk diffusion): CS ≈ MTA ≈ Dyc Indirect contact (eluates from materials): Cs ≈ MTA > Dycal |
| Cell differentiation | Immunohistochemistry (at 4 weeks) | MTA and CS expressed Nestin and Collagen I at a similar level as the control group. Both materials generated mineral deposits at a similar level as the control group. | |||
| Genotoxicity | Ames test | CS does not induce reverse mutations with/without the S9 metabolic activation system. | |||
| Micronuclei test Comet assay | CS generated lymphocytes with micronuclei ≈ as the negative control. | ||||
| CS generated DNA in the tail ≈ as the negative control and < than the cytotoxic control. | |||||
| Min et al. (2009) [60] | Radiopaque Portland cement (RPC) Portland cement (PC) IRM (Dentsply-Sirona) | Direct and indirect contact (SET materials) | Cell morphology | SEM (at 48 h) | PC and RPC: Spread and flattened HDPCs. The density and characteristics of the HDPCs in both groups were similar to that on control samples. IRM: no living cells were seen in contact with the |
| Cell differentiation | ALP activity (at 1, 3, 7 & 14 days) | 1d: PC and RPC > control; 3d, 7d, 14d: control > PC and RPC 2wk and 3wk: PC and PCR > control DSPP: PC and RPC > control at day 14; OCN: control ≈ Pc and RPC at all study periods. | |||
| ARS staining (1, 2 & 3 wk) | |||||
| RT-PCR (DSPP, ON) (at 1, 3, 7 & 14 days) | |||||
| Lee et al. (2014) [61] | ProRoot MTA (MTA; Dentsply-Sirona) α-tricalcium phosphate-based cement (α-TCP) | Direct and indirect contact (SET materials) | Cell morphology | SEM (at 72 h) | hDPCs in contact with MTA and α-TCP were well-spread and flattened. |
| Cell viability | MTT assay (at 1, 2, 3, 7 & 14 days) | MTA and α-TCP ≈ control until day 7 α-TCP > MTA at 14d; α-TCP ≈ control | |||
| Cell differentiation | Western blot (DSPP, DMP-1 and ON) (at 3 days) | α-TCP ≈ MTA for DSPP, DMP-1 and ON. | |||
| ARS staining (at 14 days) | α-TCP ≈ MTA for DSPP, DMP-1 and ON. | ||||
| Immunofluorescence (DSPP, DMP-1 and ON) (at 7 days) | α-TCP and MTA induced higher protein signals than the control group. | ||||
| Bortoluzzi et al. (2015) [62] | Biodentine (Bd; Septodont) Theracal LC (Th; Bisco) MTA Angelus (MTA-A; Angelus) | Indirect contact * (SET materials) | Cell viability | XTT assay (direct and indirect eluate evaluations) Flow cytometry– Annexin V-PI (4 weekly cycles) | Direct evaluation: 1st cycle: control > Bd > MTA-A and Th 2nd cycle: control > Bd ≈ MTA-A > Th 3rd cycle: control ≥ MTA-A ≥ Bd > Th 4th cycle: control ≈ Bd ≈ MTA-A > Th Indirect eluate evaluation: 1:1&1:10 dilutions: control > MTA-A ≈ Bd > Th; 1:100 dilution: control ≈ MTA-A ≈ Bd > Th Percentage of healthy, non-apoptotic and non-necrotic cells: control > MTA-A ≈ Bd > Th Th was the most cytotoxic material causing apoptosis and necrosis. |
| Cell differentiation | qRT-PCR (DSPP, OCN, BSP, RUNX 2, DMP-1 and ALP) (at 7 days) | ALP; OCN; BSP; DSPP; DMP-1: Bd and MTA-A > control ≈ Th RUNX 2: Bd ≈ MTA-A ≈ control ≈ Th | |||
| ALP activity (at 14 days) | Bd ≈ control > MTA-A > Th | ||||
| ARS and TEM (at 21 days) | Bd > control > MTA-A > Th | ||||
| Niu et al. (2015) [63] | ProRoot MTA (MTA; Dentsply-Sirona) Quick-Set2 (Qs; Avalon Biomed Inc) | Direct and indirect contact (SET materials) | Cell viability | Flow cytometry– Annexin V-PI (3 weekly cycles) Leakage of cytosolic enzyme (3 weekly cycles) Caspase-3 acitivity (3 weekly cycles) Oxidative stress (3 weekly cycles) | Number of healthy cells: 1st cycle: control > Qs > MTA (p < 0.001) > IRM 2nd cycle: control > Qs ≈ MTA > IRM; 3rd cycle: control ⩾ MTA ⩾ Qs > IRM Percentage of cytotoxicity: 1st cycle: IRM > MTA > Qs > control; 2nd and 3rd cycles: IRM > MTA ≈ Qs > control Relative caspase-3 activity: 1st cycle: IRM > MTA > Qs > control; 2nd cycle: IRM > MTA > Qs > control 3rd cycle: IRM > MTA ≈ Qs > control Oxidative stress: 1st cycle: IRM > MTA > Qs > control; 2nd cycle: IRM > MTA ≈ Qs > control 3rd cycle: IRM > MTA ≈ Qs ≈ control |
| Cell proliferation | MTT assay (3 weekly cycles)Cellular DNA content (3 weekly cycles) | 1st cycle: control > Qs > MTA > IRM 2nd cycle: control > Qs ≈ MTA > IRM 3rd cycle: control > Qs > MTA > IRM DNA content: 1st cycle: control > Qs > MTA > IRM 2nd cycle: control > Qs ≈ MTA > IRM 3rd cycle: control > Qs ≈ MTA > IRM | |||
| Öncel Torun et al. (2015) [64] | iRoot BP Plus (iBP; Innovative Bioceramix) White MTA Angelus (MTA-A; Angelus) | Indirect contact (SET materials) | Cell viability | XTT assay (24, 48 & 72 h) | 24 h; 1:1 and 1:2 dilutions: iBP > W-MTA-A; 1:5 and 1:10 dilutions: iBP ≈ MTA-A 48 h; 1:1 dilution: iBP > W-MTA-A; 1:2, 1:5 and 1:10 dilutions: iBP ≈ MTA-A 72 h; all concentrations: iBP ≈ MTA-A |
| Cell differentiation | qRT-PCR (BMP-2, ON, BSP, OPN, DSPP, Col I A1, HO-1 at 24 & 72 h) | BMP-2: 24 h 1:1 and 1:5 dilutions MTA-A > iBP; 1:2 dilution: iBP ≈ MTA-A 72 h 1:1, 1:2 and 1:5 dilutions MTA-A > iBPON: 24 h 1:1 and 1:5 dilutions iBP > MTA-A; 1:2 diution: iBP ≈ MTA-A 72 h: 1:1 dilution iBP > MTA-A; 1:2 and 1:5 dilutions MTA-A > iBP BSP: 24 h: 1:1 dilution MTA-A > iBP; 1:2 and 1:5 diutions: iBP ≈ MTA-A 72 h: 1:1 and 1:2 dilutions MTA-A > iBP; 1:5 diution: iBP ≈ MTA-AOPN: 24 h: 1:2 dilution iBP > MTA-A; 1:1 and 1:5 dilutions: iBP ≈ MTA-A 72 h: 1:1 and 1:5 dilutions MTA-A > iBP; 1:2 dilution: iBP ≈ MTA-A DSPP: 24 h: 1:1 dilution iBP > MTA-A; 1:2 and 1:5 dilutions: iBP ≈ MTA-A 72 h: 1:2 dilution iBP> MTA-A; 1:1 dilution MTA-A > iBP; 1:5 dilution: iBP ≈ MTA-ACol I A1: 24 h: 1:1 dilution iBP > MTA-A; 1:2 and 1:5 dilutions: iBP ≈ MTA-A 72 h: 1:1 and 1:2 dilutions iBP > MTA-A; 1:5 dilution: iBP ≈ MTA-AHO-1: 24 h 1:1 and 1:2 dilutions MTA-A > iBP; 1:5 dilution: iBP ≈ MTA-A 72 h: 1:1, 1:2 and 1:5 dilutions MTA-A > iBP | |||
| Zhang et al.(2015) [65] | iRoot BP Plus (iBP; Innovative Bioceramix) ProRoot MTA (MTA; Dentsply-Sirona) | Indirect contact (SET materials) (ISO 10993-5) | Cell Viability | Flow cytometry– Annexin V-PI | iBP ≈ MTA ≈control |
| Cell Migration | Wound-healing at 24 h | iBP ≈ MTA > control | |||
| Transwell assay at 24 h | iBP = MTA > control | ||||
| Cellular adhesion and motility | Western-Blot (at 5, 10, 30 & 60 min) Cell Immunofluorescence assay (at 1 h) | iBP led to phosphorylation of p38 MAPK, ERK 1/2, JNK, Akt, and FGFR | |||
| iBP significantly increased p–focal adhesion kinase (p-FAK), p-paxillin, and vinculin Cells treated with iBP showed highly organized and stretched stress fiber assembly | |||||
| Chung CJ et al. (2016) [66] | Dycal (Dy; Dentsply-Sirona) Endocem Zr (E-Zr, Maruchi) White ProRoot MTA (MTA; Dentsply-Sirona) Retro-MTA (R-MTA; Bio MTA) | Indirect and direct contact; SET (s) and FRESH (f) materials | Cell morphology/attachment | Phase microscopy (at 3 & 7 days) SEM (at 3 & 7 days) | 3d: MTA > cell morphology and attachement than R-MTA and E-Zr 7d: MTA, R-MTA and E-Zr sowed good cell morphology and attachement Dycal treated cells were dead after 3 and 7 days. Dycal was not further used |
| Cell viability | XTT assay (at 3 & 7 days) | 3 d: control ≈ MTA (s) ≈ MTA (f) > R-MTA (s) ≈ R-MTA (f) > E-Zr (s) ≈ E-Zr (f) 7 d: MTA(f) > control ≈ MTA (s) ≈ R-MTA (s) ≈ R-MTA (f) ≈ E-Zr (f) > E-Zr (s) | |||
| Angiogenic properties | ELISA (VEGF, angiogenin, FGF-2) (at 3 & 7 days) | VEGF24 h: control ≈ MTA (s) ≈ R-MTA (s) ≈ R-MTA (f) ≥ MTA (f) ≈ E-Zr (s) > E-Zr (f) VEGF72 h: MTA (s) ≈ MTA (f) ≈ R-MTA (s) ≈ E-Zr (s) ≥ control ≥ R-MTA (f) ≈ E-Zr (f) Angiogenin 24 h: control≈ MTA(s) ≥ R-MTA (s) > MTA(f) > R-MTA (f) ≈ E-Zr(s)>E-Zr (f) Angiogenin 72 h: R-MTA (s) ≈ R-MTA (f) ≈ control > MTA(s) ≈ MTA (f) > E-Zr (s) ≈ E-Zr (f) FGF-2 24 h and 72 h: no difference among materials and control | |||
| Daltoé M et al. (2016) [67] | Biodentine (Bd; Septodont) White ProRoot MTA (MTA; Dentsply-Sirona) | Indirect contact (SET materials) (ISO 10993-5) | Cell Viability | MTT assay (at 24 & 48 h) | 24 h: control ≈ MTA_1:100 ≈ Bd_1:100 > MTA_1:10, Bd_1:10, Bd_1:1 and MTA_1:1 48 h: control ≈ MTA_1:100 ≈ Bd_1:100 > MTA_1:10, Bd_1:10, MTA_1:1 and Bd_1:1 |
| Cell differentiation | qRT-PCR (SPP1, IBSP, DSPP, ALP 1, DMP-1 and RUNX 2 (at 24 & 48 h) | SPP1 & ALP1 & RUNX2 at 24 h: Bd and MTA ≈ control SPP1 & ALP1 & RUNX2 48 h: Bd and MTA > control IBSP & DSPP & DMP1: 24 h and 48 h: no expression | |||
| Widbiller M et al. (2016) [68] | Biodentine (Bd; Septodont) GI Ketac-Molar (KM; 3M) ProRoot MTA (MTA; Dentsply-Sirona) | Indirect and direct contact (SET materials) | Cell morphology/attachement (only Bd) | SEM (at 24 h) | Biodentine: cells showed adhesion to and spreading onto the cement surface * Not done for the other materials. |
| Cell viability | MTT assay (at 1, 3, 5, 7, 10 & 14 days) | Bd > other materials and control at 1, 3, 5 and 7 d; Bd ≈ MTA > control > KM at 10 and 14 d MTA < viability than the control at 1d; MTA ≈ cell viability as the control at 3-5-7d; KM < cell viability than all the materials tested and the control at all time points | |||
| Cell differentiation Not performed on KM | RT-qPCR (ALP, Col-I A1, DSPP, RUNX 2) (at 7, 14 & 21 days) | Col-I A1 & ALP: upregulated at 7d, especially for MTA, and decreased steadily until 21d DSPP: upregulated for MTA and BD at 14 and 21d RUNX2: downregulated for MTA and BF throughout the whole study period | |||
| ALP activity (at 3, 7 & 14 days) | ALP activity was downregulated for Bd at all times: MTA ≈ control > Bd | ||||
| Jeanneau C et al. (2017) [28] | Biodentine (Bd; Septodont) Theracal LC (Th; Bisco) Xeno III (Dentsply-Sirona) | Indirect contact (SET materials) | Cell proliferation | MTT assay (3, 5, & 7 days) | Bd_0.05 cm2/mL > Th_ 0.05 cm2/mL (p < 0.05) ≈ control at 3, 5 and 7 days Bd_0.5 cm2/mL > Th_ 0.5 cm2/mL (p < 0.05) ≈ control at 3, 5 and 7 days |
| Cell differentiation | Immunofluorescence (DSP and Nestin at day 7) | Bd increased the expression of both markers, while Th had no effect | |||
| Inflammatory effect | ELISA (IL-8; 24 and 48 h) | IL-8 expression at 24 h: Th_0.05 cm2/mL > Bd_0.05 cm2/mL ≈ control IL-8 expression at 48 h: Th_0.05 cm2/mL > Bd_0.05 cm2/mL > control | |||
| Jun S-K et al. (2017) [69] | Activa Bioactive (Activa; Pulpdent) Dycal (Dy; Dentsply-Sirona) Theracal LC (Th; Bisco) | Indirect contact (SET materials) (ISO 10993-12) | Cell viability | MTS assay (at 24 h) Live/dead assay (at 24 h) | 3.125% eluates: Dy > Th > Activa ≈ control; 6.25% eluates: Dy > Th ≈ Activa ≈ control 12.5% eluates: Dy ≈ Th ≈ Activa ≈ control; 25% eluates: Dy < Activa < Th < control 50% eluates: Dy ≈ Activa < Th < control 50% eluates: Dy < Activa < Th < control |
| Cell differentiation | ALP (at days 14 and 21) | 14 d: Th > Dy > Activa ≈ Osteogenic medium 21 d: Th ≈ Dy > Activa > Osteogenic medium | |||
| ARS (at 21 days) | Th ≈ Dy > Activa ≈ Osteogenic medium | ||||
| Lee B-N et al. (2017) [70] | ProRoot MTA (MTA; Dentsply-Sirona) Theracal LC (Th; Bisco) | Indirect contact (SET materials) | Cell viability | WST-1 assay (at 24 h) | 100% concentration: Th > MTA; At 50%, 25% and 10% dilutions: Th ≈ MTA At 100% MTA: cell viability < 70% and significantly lower than Th. |
| Cell differentiation | RT-PCR (DSPP, DMP-1 at 1 & 3d) Q-PCR(DSPP, DMP-1 at 2, 5 & 7d) ALP staining (at day 7) ARS (at day 14) | DSPP 1 d: MTA > Th ≈ control; 3 d: MTA ≈ Th > control DMP-1 at 1 and 3d: MTA ≈ Th ≈ control DSPP & DMP-1: upregulated for both materials, especially at day 7. MTA > Th ≈ control MTA > Th > control | |||
| Mestieri LB et al. (2017) [71] | White MTA Angelus (MTA-A; Angelus) White Portland Cement (PC; Votoran) | Indirect contact (SET materials) | Cell viability | MTT assay | 1:2, 1:3, 1:4 and 1:8 dilutions: control > W-MTA-A >W-PC 1:6 dilution: MTA-A ≈ control > PC |
| Trypan blue assay | 1:2 dilution: control > MTA-A > PC 1:3 dilution: control > PC > MTA-A 1:4 and 1:6 dilutions: control > PC > MTA-A 1:8 dilution: control > PC ≈ MTA-A | ||||
| Cell Differentiation | ALP activity (at 1, 3 & 7d) | 1, 3 and 7 d: MTA-A ≈ PC ≈ control | |||
| Rodrigues EM et al. (2017) [72] | MTA-Plus (MTA-P; Prevest Denpro) White MTA Angelus (MTA-A; Angelus) | Indirect contact (SET materials)(ISO-10993) | Cell viability | MTT Assay Flow cytometry– Annexin V-PI | 1:2 concentration: MTA-P > MTA-A ≈ control 1:4 and 1:8 concentrations: MTA-P ≈ MTA-A > control MTA-A > live cells than MTA-P ≈ control MTA-A > necrotic cells than MTA-P > control |
| Cell differentiation | ALP activity (at 1, 3 & 7 days) | MTA-A < control < MTA-P after 7 days. | |||
| ARS (14d) | MTA-A > MTA-P > control | ||||
| qRT-PCR (BMP2, OC, ALP) | Day 1_BMP2 & OC: MTA-A > MTA-P > control; ALP: MTA-A ≈ MTA-P < control Day 3_ BMP2: MTA-A > MTA-P > control; OC & ALP: MTA-A ≈ MTA-P < control | ||||
| Sun Y et al. (2017) [73] | Biodentine (Bd; Septodont) iRoot FS (iFS; Innovative Bioceramix) | Indirect contact (SET materials) | Cell proliferation | CCK-8 assay (1, 3 & 7 days) | 1 d: Bd_0.2 mg/mL ≈ Bd_2 mg/mL ≈ iFS_0.2 mg/mL ≈ iFS_2 mg/mL ≈ control (p ≥ 0.05) 3 d: Bd_0.2 mg/mL ≈ Bd_2 mg/mL ≈ iFS_0.2 mg/mL ≈ iFS_2 mg/mL > control 7 d: Bd_0.2 mg/mL ≈ iFS_0.2 mg/mL > Bd_2 mg/mL ≈ iFS_2 mg/mL > control |
| Cell migration (24 h) | Wound healing assay Transwell migration assay | iFS_0.2 mg/mL > iFS_2 mg/mL > control > Bd_0.2 mg/mL > Bd_2 mg/mL | |||
| iFS_0.2 mg/mL > iFS_2 mg/mL > control > Bd_0.2 mg/mL > Bd_2 mg/mL | |||||
| Cell differentiation | ALP activity (at 7, 14 d) | 7 d: iFS_0.2 mg/mL ≈ iFS_2 mg/mL ≈ Bd_0.2 mg/mL > Bd_2 mg/mL > control | |||
| 14 d: iFS_0.2 mg/mL > Bd_0.2 mg/mL > Bd_2 mg/mL ≈ iFS_2 mg/mL > control | |||||
| ARS (at 21 d) | 21 d: iFS_0.2 mg/mL > Bd_0.2 mg/mL ≈ Bd_2 mg/mL ≈ iFS_2 mg/mL ≈ control | ||||
| qRT-PCR (Col I and OCN) (at 1, 7 & 14 d) | 1 d: Col I control ≥ all materials OCN iFS_2 mg/mL ≥ iFS_0.2 mg/mL ≈ Bd_0.2 mg/mL ≈ Bd_2 mg/mL ≈ control 7 d: Col I control > iFS_0.2 mg/mL > Bd_0.2 mg/mL > Bd_2 mg/mL > iFS_2 mg/mL OCN iFS_0.2 mg/mL > control ≈ iFS_2 mg/mL > Bd_2 mg/mL ≥ Bd_0.2 mg/mL | ||||
| 14 d: Col I iFS_0.2 mg/mL > Bd_0.2 mg/mL ≈ Bd_2 mg/mL ≥ control ≥ iFS_2 mg/mL OCN iFS_0.2 mg/mL ≈ iFS_2 mg/m ≥ control ≥ Bd_0.2 mg/mL ≥ Bd_2 mg/mL | |||||
| Tomás -Catalá et al. (2017) [74] | MTA-repair HP Angelus (MTA-HP; Angelus) NeoMTA-Plus (N-MTA-P; Avalon Biomed Inc) White MTA Angelus (W-MTA; Angelus) | Indirect and direct contact (SET materials) (ISO 10993-5) | Cell morphology | SEM-EDX (direct contact, 72 h) | Cells attached and merged in all three materials, more cell monolayer structures were evident on the surface of W-MTA. EDX revealed MTA-HP ≈ N-MTA-P ≈ W-MTA in %weight of Ca, C and O. |
| Cell Viability (24, 48 & 72 h) | MTT assay | 24 h all dilutions: MTA-HP ≈ N-MTA-P ≈ W-MTA ≈ control 48 h undiluted extract: MTA-HP ≈ W-MTA > control 48 h 1:2 dilution: MTA-HP ≈ N-MTA-P ≈ W-MTA ≈ control 48 h 1:4 dilution: W-MTA > control ≈ MTA-HP > N-MTA-P 72 h undiluted extract: W-MTA > N-MTA-P > MTA-HP > control 72 h 1:2 dilution: MTA-HP ≈ N-MTA-P ≈ W-MTA ≈ control 72 h 1:4 dilution: MTA-HP < control ≈ N-MTA-P ≈ W-MTA | |||
| Cell migration (24 & 48 h) | Wound healing–scratch assay | N-MTA-P < control for all dilutions and time points MTA-HP-A > control at 24 h_1:1/1:2 dilutions but < control at 48 h W-MTA-A > control at 24 h_all dilutions but < control at 48 h | |||
| Collado-González M et al. (2018) [75] | GI Equia Forte (EF; GC) GI Ionostar Molar (IoM;Voco) | Indirect and direct contact (SET materials) (ISO 10993-5) | Cell morphology (indirect contact, 24 h) | Confocal microscopy (cytoskeletal F-actin) | 1:1 extracts EF ≈ control (an organized and stretched stress fiber) 1:1 extracts IoM < control (cell numbers and stretched stress fiber) |
| Cell morphology (direct contact, 72 h) | SEM | EF > IoM (cell attachment, morphology and growth) | |||
| Cell Viability (at 24, 48 & 72 h) | MTT assay | 24 h all concentrations: Control > EF ≈ IoM 48 h 1:1 dilution: Control ≈ IoM > EF; 48 h 1:2 dilution: IoM ≈ EF ≈ control 48 h 1:4 dilution: IoM ≈ EF ≈ control 72 h 1:1 dilution: EF ≈ control > IoM 72 h 1:2 dilution: control > IoM ≈ EF 72 h 1:4 dilution: control > EF > IoM | |||
| Cell migration (24 and 48 h) | Scratch assay | Control > EF > IoM for all concentrations and study periods | |||
| Cell differentiation | Flow cytometry– Annexin V/7-AAD staining | IoM and EF ≈ control (the percentage of positive expression of mesenchymal markers) | |||
| Pedano MS et al. (2018) [76] | Exp-PPL (PPL) Biodentine (Bd; Septodont) Nex-Cem MTA (Nex-MTA; GC) Zinc-oxide eugenol Alganol (ZnO; Kemdent) | Indirect contact (FRESH materials) | Cell viability (24 h) | XTT assay | 10% eluates: Bd > PPL ≈ Nex-MTA > ZnO 25% eluates: PPL > Nex-MTA > Bd > ZnO 50% eluates: PPL ≈ Nex-MTA > Bd > ZnO 100% eluates: Nex-MTA > PPL > Bd > ZnO |
| Cell proliferation (1, 4 & 7 d) | XTT assay | 10% eluates 7d: PPL ≈ Bd ≈ control > Nex-MTA > ZnO 25% eluates 7d: control > Bd > PPL > Nex-MTA > ZnO 50% eluates 7d: control > Bd > PPL > Nex-MTA > ZnO 100% eluates 7d: control > PPL ≈ Bd ≈ Nex-MTA > ZnO | |||
| Cell migration (24 h) | Scratch-wound healing assay | 10% and 25% eluates: control ≈ PPL ≈ Nex-MTA > Bd 50% eluates: control ≈Nex-MTA ≈ PPL > Bd 100% eluates: control > PPL > Nex-MTA > Bd | |||
| Cell differentiation (4, 10 & 14 d) | RT-PCR (ALP, OCN, DSPP) | ALP 4 d: differentiation medium > PPL ≈ Bd ≈ Nex-MTA 10 d: differentiation medium ≈ PPL ≈ Bd ≈ Nex-MTA 14 d: differentiation medium > PPL > Bd ≈ Nex-MTA OCN 14d: PPL ≈ Bd > Nex-MTA ≈ differentiation medium DSPP 10 d: PPL ≈ Bd ≈ Nex-MTA ≈ differentiation medium 14 d: Bd > PPL > differentiation medium > Nex-MTA | |||
| Tomás-Catalá CJ et al. (2018) [77] | Biodentine (Bd; Septodont)MTA Repair HP Angelus (MTA-HP-A; Angelus) NeoMTA Plus (N-MTA-P; Avalon Biomed Inc) | Indirect and direct contact (SET materials) (ISO 10993-5) | Cell attachment | SEM-EDX (direct contact, 72 h) | SEM showed Bd revealed more cells and with better morphology than MTA-HP-A and N-MTA-P. The EDX revealed that Bd, MTA-HP-A and N-MTA-P had similar percentages of Ca, C and O. |
| Cell viability | MTT assay (24, 48 & 72 h) | Undiluted extract: Bd > MTA-HP-A > N-MTA-P > control at 48 h and 72 h 1:2 dilution: Bd > MTA-HP-A ≈ N-MTA-P ≈ control (p < 0.01) at 48 h and 72 h 1:4 dilution: Bd > N-MTA-P ≈ control > MTA-HP-A at 72 h | |||
| Cell migration | Scratch assay (at 24 & 48 h) | 24 h: Bd > MTA-HP-A ≈ N-MTA-P ≈ control (p < 0.01) 48 h: Bd > control for all dilutions; control > N-MTA-P > MTA-HP-A | |||
| Lee S-M et al. (2019) [78] | Smart Dentin Replacement (SDR; Dentsply-Sirona) Venus Bulk-fill (VBF; Hereaus Kulzer) Beautifil Bulk flowable (BBF; Shofu) Filtek Z350 XT Flowable (ZFF; 3M) | Indirect contact (Set materials) (ISO 10993-5) | Cell viability | WST assay (24 h) Live/dead Assay (direct visualization with confocal microscopy) | 2-mm-cured composite: ≈ 100% cell-viability except for BFF (49%) 4-mm-cured composite: SDR not cytotoxic at all dilutions. VBF & BBF statistically different values (71.05% and 64.43%, respectively) of cell viability at 100% concentration compared to control (p < 0.05) but no statistically different cell viability compared to control at 25% and 12.5% concentrations, respectively (~100%, p > 0.05) 6-mm-cured composite: SDR and BBF were ~69% and ~6% at 100% concentration (p < 0.05), and these resins did not show statistically different cell viability compared to control at 25% and 12.5% (~100%, p > 0.05), respectively. In contrast, VBF and ZFF did not reach non-cytotoxic levels (~100%) even at 12.5% dilution. |
| At 100% concentrations of SDR, VBF, and ZFF, 6-mm cured composite showed 5~60% live cell numbers compared to the 2-mm cured group. Another bulk-fill resin, BBF, had 5~35% live cells with some dead cells in all groups. At 12.5%, there were full of live cells at all groups while the 4-mm cured ZFF and the 6-mm cured VBF and ZFF revealed fewer live cells (~75%) than the control. | |||||
| Cell differentiation (7 days) | ALP staining | 6-mm-cured bulk-fill resins showed significantly lower ALP staining than the differentiation media control (p < 0.05), while all 2-mm and 4-mm cured bulk-fill resins showed similar ALP staining, except for 4-mm-cured BBF. ALP staining from the bulk-fill resins was ranked as follows: 2-mm > 4-mm > 6-mm cured. The flowable resin, ZFF, exhibited the least amount of ALP staining between the experimental groups. | |||
| López-García et al. (2019) [79] | Activa Kids (Activa; Pulpdent) GI Ionolux (Voco) Riva Light Cure (Riva; SDI) | Indirect and direct contact (Set materials) (ISO 10993-5) | Cell morphology (indirect contact) | Immunofluorescence | Activa > cell density and spreading than Riva > Inolux |
| Cell attachment/adhesion (direct contact) | SEM | Activa showed well-adhered fibroblastic cells with multiple cytoplasmic extensions. Riva showed less density and fewer cells than Activa. Ionolux induced drastic reduction in cell density and attachement. | |||
| Cell viability | MTT assay (1, 2 & 4 days) | 24 h - Undiluted extracts: Activa ≈ control > Riva > Ionolux (p < 0.01) 24 h–1:2 dilution: Activa ≈ control ≈ Riva > Ionolux 24 h–1:4 dilution: Activa ≈ control > Riva > Ionolux 48 h-Undiluted extracts: Ionolux < Activa & Riva (p < 0.01) < control (p < 0.01) 48 h–1:2 dilution: Activa & Riva & Ionolux ≈ control 48 h–1:4 dilution: Activa & Riva & Ionolux ≈ control | |||
| 72 h-Undiluted extracts: Control > Activa > Riva > Ionolux 72 h–1:2 dilution: Control > Activa > Riva > Ionolux 72 h–1:4 dilution: Activa ≈ control; Riva & Ionolux < control | |||||
| Cell migration | Wound healing assay | Activa ≈ control at all dilutions except 1:2 at 72 h Riva < migration than control except 1:4 dilution Ionolux < migration than control except 1:4 dilution at 24 h and 48 h | |||
| Dou L et al. (2020) [80] | Dycal (Dentsply-Sirona) Pro-Root MTA (MTA; Dentsply-Sirona) iRoot BP (iRoot; Innovative Bioceramix) Platelet-rich Fibrin (PRF) Concentrated Growth Factors (CGF) | Indirect contact (Set materials) | Cell viability | Trypan Blue Staining (1, 3 & 7 days) Flow cytometry– Annexin V-PI (1, 3 & 7 days) Cell Cycle(1, 3 & 7 days) | Dycal < cell viability than MTA ≈ iRoot ≈ PRF ≈ CGF ≈ control at 1, 3 & 7 days |
| Dycal > apoptotic cells than MTA ≈ iRoot ≈ CGF ≈ control at 1, 3 & 7 days Days 1 & 3: no significant differences among the groups Day 7: CGF showed less cells in G0/G1-phase compared to MTA & Dycal | |||||
| Cell proliferation | CCK-8 | Day 1: Dycal < cell proliferation than all groups; MTA ≈ iRoot ≈ PRF ≈ CGF ≈ control. Day 3: PRF & CGF > cell proliferation than control & MTA, but ≈ iRoot; Dycal < all groups Day 7: CGF > cell proliferation than iRoot & MTA, but ≈ control &PRF; Dycal < all groups | |||
| Cell differentiation (1,3 & 7 days) | ALP staining | Days 1 & 3: MTA > ALP-activity than control; Control ≈ iRoot ≈ PRF ≈ CGF ≈ Dycal Day 7: Dycal < ALP-activity than CGF; CGF ≈ control ≈ MTA ≈ iRoot ≈ PRF |
| Authors | Study Type | Hemostasia | Materials Used | Etched Pulp? | Evaluation Period(s) | Bridge Formation | Inflammation | Sample |
| Hebling J et al. (1999) [81] | CCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide saline paste (CH) + calcium-hydroxide cement (Dycal; Dentsply-Sirona) All Bond 2 (AB2; Bisco) | No (CH), Yes (AB2) | 7 days 30 days 60 days | CH: 3/4 teeth showed complete bridge formation at 30 days. 4/4 teeth showed complete bridge below exposed area at 60 days. AB2: 0/6 teeth showed completed bridge at 30 or 60 days (0/12 in total). All of them showed modest bridge formation at 60 days. | CH: 1/4 teeth showed moderate and 3/4 slight inflammation at day 7. At day 30, 4/4 teeth showed slight inflammatory reaction. No tooth showed severe inflammation AB2: 1/6 teeth showed severe inflammatory reaction, 3/6 moderate and 2/6 slight inflammation at day 7. At day 30, 3/6 showed moderate and 3/6 slight inflammatory reaction. | 32 premolars (12–15 years old patients) |
| Do Nascimento AB et al. (2000) [82] | CCT | Sterile paper cones + sterile saline | Calcium-hydroxide saline paste (CH; Pathfinder associates) + calcium hydroxide cement (Dycal; Dentsply-Sirona)Resin-modified glass-ionomer cement (Vit; Vitrebond; 3M Oral Care) | No | 5 days 30 days 120+ days | CH: 1/4 teeth showed complete bridge at 30 days. 5/5 teeth showed complete bridge at 120+ days. Vit: 0/6 teeth showed complete bridge at 30 days. 0/5 teeth showed complete bridge at 120+ days. | CH: at day 5, 0/6 teeth showed no inflammation, 4/6 teeth showed slight, 2/6 moderate and 0/6 severe inflammation. At day 30, 3/4 showed slight and 1/4 moderate inflammation. Vit: 0/5 teeth showed none inflammatory reaction, 1/5 teeth showed slight and 4/5 moderate inflammation at day 5. At day 30, 2/6 showed slight and 4/6 moderate inflammatory reaction. | 34 premolars (11–17 years old patients) |
| Costa CAS et al. (2001) [83] | CCT | Sterile paper cones + sterile saline | Calcium-hydroxide saline paste (CH; Pathfinder associates) + calcium hydroxide cement (Dycal; Dentsply-Sirona) Clearfil Liner Bond 2 (CLB2; Kuraray Noritake) | No | 5 days 30 days 120+ days | CH: 1/4 teeth showed complete bridge at 30 days. 5/5 teeth showed complete bridge at 120+ days. CLB2: 0/5 teeth showed complete bridge at 30 days. 0/6 teeth showed complete bridge at 120+ days. | CH: at day 5, 1/6 teeth showed none inflammatory reaction, 3/6 teeth showed slight, 2/6 moderate and 0/6 severe inflammation. At day 30, 3/4 showed slight and 1/4 moderate inflammation. CLB2: 4/6 teeth showed slight and 2/6 moderate inflammation at day 5. At day 30, 2/5 showed slight and 3/5 moderate inflammatory reaction. | 36 premolars (11–17 years old patients) |
| Ersin EK et al. (2005) [84] | CCT | 3% H2O2 | Calcium-hydroxide saline paste (CH) + calcium hydroxide cement (Dycal; Dentsply-Sirona) Prime&Bond 2.1 (P&B2.1; Dentsply-Sirona) | No | 7 days 90 days | CH: 5/5 teeth showed complete bridge after 90 days. P&B2.1: 0/5 teeth showed complete bridge after 90 days. | CH: 5/5 teeth showed slight inflammatory reaction at day 7. P&B2.1: at 7 days, 5/5 teeth showed moderate acute inflammatory reaction. 0/5 teeth showed severe inflammation or necrotic tissue. | 20 premolars (mean age 12.6 years) Age range not available |
| Olsson H et al. (2005) [85] | RCT | Continuous irrigation with sterile saline | Calcium-hydroxide saline paste (CH) Enamel matrix derivative (EMD; Emdogain, BIORA) | No | 12 weeks | CH: 9/9 teeth showed complete bridge at 12 weeks. EMD: 0/9 teeth showed complete bridge at 12 weeks. | 12 weeks | 18 premolars (12–16 years old patients) |
| Silva GAB et al. (2006) [86] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide powder (CH; PA Biodinamica) + calcium hydroxide cement (Dycal; Dentsply-Sirona) Single Bond (SB; 3M Oral Care) | No (CH), Yes (10%-37%; SB) | 1 day 3 days 7 days 30 days | CH: 5/5 teeth showed complete bridge at day 30. SB-10% Etch: 0/5 teeth showed complete bridge at day 30. SB-37% Etch: 0/5 teeth showed complete bridge at day 30. | CH: 0/20 showed severe inflammatory reaction at days 1-3-7 or 30 (5/time period). 10/20 teeth showed slight and 10/20 teeth showed moderate inflammation at 1-3-7 or 30 days. SB-10% Etch: 0/20 showed severe inflammatory reaction at days 1-3-7 or 30 (5/time period). 1/20 teeth showed none/few inflammatory cells at d1. 5/20 teeth showed slight and 14/20 moderate inflammatory reaction. SB-37% Etch: 0/20 showed severe inflammatory reaction at days 1-3-7 or 30 (5/time period). 1/20 teeth showed none/few inflammatory cells at d1. 10/20 teeth showed slight and 9/20 moderate inflammation at 1-3-7 or 30d. | 81 premolars (12–17 years old patients) |
| Sawicki L et al. (2008) [87] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Life; Kerr) White Pro-Root MTA (W-MTA; Dentsply-Sirona) | No | 47+ days | Life: 11/14 teeth showed complete bridge after 47+ days. WMTA: 28/30 teeth complete bridge. 4 teeth lost (not reported) | 47+ days! | 48 premolars (10–18 years old patients) |
| Azimi S et al. (2014) [88] | RCT | Sterile cotton pellets + sterile saline | White Pro-Root MTA (W-MTA; Dentsply-Sirona) iRoot BP (iRoot; Innovative Bioceramix) | No | 6 weeks | WMTA: 8/12 teeth showed complete bridge formation at 6 weeks. iRoot: 7/12 teeth showed complete bridge at 6 weeks. | 6 weeks!! | 24 premolars (12–16 years old) |
| Swarup SJ et al. (2014) [89] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply) MTA Angelus (MTA-A; Angelus) Nanohydroxyapatite (Hap; Orthogran) | No | 15 days 30 days | Dycal: 2/5 had a complete bridge at 30d. MTA-A: 4/5 had complete bridge 30d. Hap: 4/5 teeth had complete bridge. | Dycal: 4/5 showed moderate and 1/5 severe inflammatory reaction day 15. 1/5 teeth showed moderate and 4/5 slight inflammation at day 30. MTA-A: 3/5 teeth showed none and 2/5 teeth showed slight inflammatory reaction at day 15. At day 30, 4/5 teeth showed none or few inflammations and 1/5 showed slight inflammatory reaction. Hap: 3/5 showed moderate inflammatory reaction and 2/5 severe inflammation (day 15). 3/5 showed no inflammation and 2/5 slight inflammatory reaction at day 30. | 30 premolars (11–15 years old) |
| Banava S et al. (2015) [90] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) White-MTA (WMTA; Dentsply-Sirona)Pulpdent Multi-Cal Liner (PML; Pulpdent) | No | 6 weeks | Dycal: 7/8 teeth showed bridge at 6w. WMTA: 12/16 teeth sowed bridge formation at 6w. PML: 2/8 teeth showed bridge formation at 6w. | 6 weeks!! | 32 premolars (13–20 years old) |
| Authors | Study Type | Hemostasia | Materials Used | Etched Pulp? | Evaluation Period(s) | Bridge Formation | Inflammation | Sample |
|---|---|---|---|---|---|---|---|---|
| Demarco FF et al. (2001) [91] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide powder (CH; Labrynth Produtos) + calcium-hydroxide cement Hydro C (Dentsply-Sirona) Scotchbond Multipurpose (SBMP; 3M) Clearfil Liner Bond 2 (CLB2; Kuraray Noritake) | Yes (SBMP), No (CH and CLB2) | 30 days 90 days | CH: 2/2 complete bridges formed at 30 and 2/2 at 90 days SBMP: 0/4 teeth with bridges formed at 30 and 0/4 at 90 days. CLB2: 1/4 teeth showed bridge at 30 days. 2/4 teeth showed bridge formation at 90 days. | CH: 0/2 teeth showed severe inflammation or necrosis at 30 days. SBMP: 1/4 teeth showed severe inflammation or necrosis at 30 days. CLB2: 0/4 teeth showed severe inflammation or necrosis at 30 days. | 20 molars (20–27 years old patients) |
| Accorinte MLR et al. (2005) [92] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide powder (CH; Labrynth Produtos) + calcium-hydroxide cement (Dycal; Dentsply-Sirona) Scotchbond Multipurpose (SBMP; 3M Oral Care) | Yes (SBMP), No (CH) | 60 days | CH: 100% (5/5) of the teeth showed brige formation at day 60. SBMP: 0% (0/5) of the teeth showed bridge formation | 60 days | 25 premolars (15–25 years old patients) |
| Accorinte MLR et al. (2006) [93] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide powder (CH; Labrynth Produtos) + calcium-hydroxide cement (Dycal; Dentsply-Sirona) Scotch Bond Multipurpose (SBMP; 3M Oral Care) | Yes (SBMP), No (CH) | 30 days 60 days | CH: 100% (5/5) of the teeth showed brige formation at 30 and 60 days. SBMP: 0% (0/5) of the teeth showed bridge formation at 30 or 60 days. | CH: no to mild inflammatory reaction all teeth (5/5) at 30 days. SBMP: 2/5 teeth (40%) showed pulp necrosis at day 30. | 40 premolars (15–25 years old patients) |
| Iwamoto CE et al. (2006) [94] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) White Pro-Root MTA (W-MTA; Dentsply-Sirona) | No | 112+ days | Dycal: 18/23 teeth developed bridge formation at 110+ days. W-MTA: 20/22 teeth developed bridge formation. | 112+ days | 48 molars (18–60 years old patients) |
| Accorinte MLR et al. (2007) [95] | CCT | Sterile cotton pellets + sterile saline; sterile cotton pellets + 2.5% sodium hypochlorite | Calcium-hydroxide cement (Life; Kerr) | No | 30 days 60 days | Life: 2/10 teeth (20%) showed bridge formation at 30 days. At day 60, 6/10 teeth showed complete bridge formation. At day 60, only 1/10 teeth showed absent bridge. | Life: At day 30, 8/10 teeth showed no inflammation and 1/10 showed mild inflammatory reaction. Only 1/10 teeth showed severe inflammation. | 40 premolars (15–30 years old patients) |
| Elias RV et al. (2007) [96] | RCT | Sterile cotton pellets + 2.5% sodium hypochlorite | Calcium-hydroxide powder (CH; Labrynth Produtos) + calcium-hydroxide cement Hydro C (Dentsply-Sirona) Clearfil SE Bond (CSE; Kuraray Noritake) | No | 30 day 90 days | CH: 5/5 complete bridge after 30 days and 5/5 at 90 days. CSE: 1/8 specimens showed dentin deposition at the interface (complete bridge) at 90 days. 0/8 teeth showed complete bridge at 30 days. 3/8 specimens showed no dentin deposition at all. | CH: 5/5 teeth showed none or slight inflammation after 30 days for all specimens. CSE: 4/8 specimens showed no inflammation; 3/8 specimens slight inflamm; 1/8 severe inflammation at 30 days. | 26 molars (average 25 years) Age range not provided |
| Accorinte MLR et al. (2008) [53] | CCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Life; Kerr) Pro-Root MTA (MTA; Dentsply-Sirona) | No | 30 days 60 days | Life: 2/10 teeth showed complete bridge at 30 days and 6/10 complete bridge after 60 days MTA: 3/10 teeth showed complete bridge at 30 days and 5/10 teeth complete bridge after 60 days | Life: all teeth showed absent (8/10) or mild (2/10) inflammatory reaction at 30 days. 1/10 teeth showed slight and 1/10 moderate inflammatory reaction. No teeth showed necrosis or abscess formation at 30 days.MTA: all teeth showed absent (9/10) or mild (1/10) inflammatory reaction at 30 days. No teeth showed necrosis or abscess formation at 30 days. | 40 premolars (15–30 years old patients) |
| Accorinte MLR et al. (2008) [52] | CCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide powder (CH) + calcium-hydroxide cement (Life; Kerr) MTA Angelus (MTA-A; Angelus) | No | 30 days 60 days | CH: 6/10 teeth showed complete bridge at 30 days and 8/10 teeth showed complete bridge after 60 days MTA-A: 4/10 teeth showed complete bridge at 30 days and 7/10 complete bridge after 60 days | CH: 8/10 teeth showed absent or slight inflammatory reaction at 30 days. No teeth showed necrosis or abscess formation at 30 days. MTA-A: 8/10 teeth showed absent or slight inflammatory reaction at 30 days. 1/10 teeth showed severe inflammation (abscess formation) at 30 days. | 40 premolars (15–30 years old patients) |
| Accorinte MLR et al. (2008) [97] | CCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) Clearfil Liner Bond 2V (C2V; Kuraray Noritake) Clearfil SE Bond (CSE; Kuraray Noritake) | No | 30 days 90 days | Dycal: 8/9 teeth with complete bridge formed at day 90. No CH treated teeth extracted at 30 days. C2V: 1/4 teeth complete bridge at 30 days. 1/6 teeth with complete bridge at day 90 and 2/6 with absence or discrete bridge CSE: 0/5 teeth complete bridge at 30 days. 1/6 teeth with complete bridge at day 90 and 4/6 with absence or discrete bridge | Dycal: no teeth were extracted at 30 days for CH group. C2V: All teeth had slight (2/6) or moderate (3/6) inflammation after 30 days including 1/6 teeth with abscess. CSE: All teeth had slight (3/6) or moderate (2/6) inflammation after 30 days including 1/6 teeth with abscess. | 34 premolars (15–30 years old patients) |
| Lu Y et al. (2008) [98] | RCT | Sterile cotton pellets + 2% chlorhexidine + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) Clearfil SE Bond (CSE; Kuraray Noritake) | No | 7 days 30 days 90 days | Dycal: 1/6 teeth complete bridge at day 30. 5/7 teeth complete bridge deposits after 90 days. CSE: 0/7 teeth complete bridge after 30 and 0/7 at 90 days. | Dycal: 2/7 teeth showed slight, 4/7 moderate and 1/7 teeth showed severe inflammatory reaction at day 7. At day 30, 5/6 teeth showed slight and 1/6 moderate inflammatory reaction. CSE: 6/7 teeth showed slight and 1/7 moderate inflammatory reaction at both 7 and 30 days. | 45 molars (20–25 years old patients) |
| Min K-S et al. (2008) [99] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) Pro-Root MTA (MTA; Dentsply-Sirona) | No | 2 months | Dycal: 6/10 teeth complete bridge. 4/10 total absence of bridge. MTA: 100% complete bridge formation. Bridges were significantly thicker with MTA | 2 months!! | 20 molars (2–50 years old patients) |
| Nair PNR et al. (2008) [100] | RCT | 1% sodium hypochlorite + sterile saline + paper points | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) Pro-Root MTA (MTA; Dentsply-Sirona) | No | 7 days 30 days 90 days | Dycal: 1/5 teeth complete bridge and 3/5 partial bridge at day 30. At day 90, 2/4 teeth partial bridge and 0/4 complete bridge at 90 days. Thick bridges with tunnel defects. MTA: 3/6 teeth with complete bridge formation at day 30. 4/5 teeth complete bridge formation at day 90. MTA showed thicker and less variable bridges than Dycal. | Dycal: at day 7, 2/4 teeth showed inflammatory reaction, 1 of them with severe inflammation. At day 30, 1/5 teeth showed severe inflammatory reaction. MTA: 5/6 teeth showed absence of inflammatory reaction and 1/6 showed slight inflammation at day 7. At day 30, 6/6 samples showed no inflammatory reaction. | 33 molars (18–30 years old patients) |
| Accorinte MLR et al. (2009) [101] | RCT | Sterile cotton pellets + sterile saline | Pro-Root MTA (MTA; Dentsply-Sirona) MTA Angelus (MTA-A; Angelus) | No | 30 days 60 days | MTA: 5/8 teeth had complete bridge at day 30. 5/9 teeth showed complete bridge at day 60.MTA-A: 5/8 teeth had complete bridge at day 30. 6/10 teeth showed complete bridge at day 60. | MTA: 2/8 teeth showed no inflammation and 6/8 slight inflammatory reaction at day 30. MTA-A: 3/8 teeth showed no inflammation at day 30. 4/8 showed mild inflammatory reaction and 1 tooth showed abscess at day 30. | 35 premolars (25–42 years old patients) |
| Kiatwateeratana T et al. (2009) [102] | RCT | Moistened sterile cotton pellets | Calcium-hydroxide powder (CH) Enamel matrix derivative (EMD; Emdogain, BIORA) | No | 6 months | CH: 10/13 teeth showed complete bridge formation EMD: no tooth showed bridge formation | 6 months! | 26 premolars (13–22 years old) |
| Parolia A et al. (2010) [103] | CCT | Moistened sterile cotton pellets | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) Pro-Root MTA (MTA; Dentsply-Sirona)Propolis powder (Propolis; Ecuadorian Rainforest LLC) mixed with 70% ethanol | No | 15 days 45 days | Dycal: 5/6 teeth showed bridge formation at 45 days. MTA: 6/6 teeth showed bridge formation at day 45. Propolis: 6/6 teeth showed bridge formation at 45 days. | Dycal: 6/6 teeth showed none or mild inflammation at day 15. MTA: all teeth (6/6) showed none or mild inflammation at day 15. Propolis: 6/6 teeth showed none or mild inflammation at day 15. | 36 premolars (15–25 years old) |
| Nowicka A et al. (2013) [104] | CCT | Sterile cotton pellets + sterile saline | White Pro-Root MTA (W-MTA; Dentsply-Sirona) Biodentine (Biodentine; Septodont) | No | 6 weeks | W-MTA: 7/11 teeth had complete bridge. All teeth formed bridges. Biodentine: 6/11 teeth had complete bridge. All teeth formed bridges. | 6 weeks! | 28 molars (19–28 years old patients) |
| Nowicka A et al. (2016) [105] | RCT | Sterile cotton pellets + sterile saline | Calcium hydroxide paste (Calcipast; Cerkamed) + Calcium hydroxide cement (Life, Kerr) Single Bond Universal (SBU; 3M Oral Care) | No | 6 weeks | Calcipast: all teeth showed bridge formation with 5/11 teeth showing complete bridge at 6 wk SBU: none of the teeth showed complete bridge formation. 7/11 teeth showed no bridge formation at 6 wks. | 6 weeks! | 28 molars (19–28 years old patients) |
| Bakhtiar H et al. (2017) [106] | RCT | Sterile cotton pellets | Theracal LC (Theracal; Bisco) Biodentine (Biodentine; Septodont) Pro-Root MTA (W-MTA; Dentsply-Sirona) | No | 8 weeks | Theracal: 2/9 teeth showed no bridge formation at 8 wks. 1/9 teeth showed complete bridge at 8 wks. Biodentine: All teeth (9/9) showed a complete bridge formation at 8 wks. W-MTA: 5/9 teeth showed a complete bridge at 8 wks. 4/9 teeth showed an incomplete bridge at 8 wks. | 8 weeks! | 27 molars (18–32 years old patients) |
| Jalan AL et al. (2017) [107] | RCT | Sterile cotton pellets + sterile saline | Calcium-hydroxide cement (Dycal; Dentsply-Sirona) Biodentine (Biodentine; Septodont) | No | 45 days | Dycal: 1/20 teeth showed no bridge formation. 4/20 teeth showed a complete bridge. Biodentine: all teeth showed bridge formation. 16/20 teeth complete bridge. | 45 days | 40 premolars (15–25 years old) |
| Mehrvarzfar P et al. (2018) [108] | RCT | Sterile cotton pellets + sterile saline | White Pro-Root MTA (W-MTA; Dentsply-Sirona) W-MTA + Treated Dentin Matrix (W-MTA/TDM; Dentsply-Sirona) | No | 6 weeks | W-MTA: 11/11 complete bridge was present in all specimens at 6 wk. W-MTA/TDM: 11/11 complete bridge was present in all specimens at 6 wks. | 6 weeks! | 26 molars (15–31 years old patients) |
| Comparison | Direct Comparison | Indirect Comparison | ||
|---|---|---|---|---|
| Relative Risk (95% CIs) | Evidence Level | Relative Risk (95% CIs) | Evidence Level | |
| Pro-Root MTA vs. calcium-hydroxide (CH) powder | No studies available | Not available | No studies available 1 | Not available |
| Pro-Root MTA vs. CH cements (Dycal, Life, Calcipast, …) | 0.29 [0.01, 5.79] | VERY LOW 2 b | 0.39 [0.04, 3.47] | LOW a |
| MTA-like cements (Pro-Root MTA, Angelus MTA, …) vs. CH powder | 3.00 [0.14, 65.90] 3 | VERY LOW 3 b | 2.67 [0.29, 24.24] | LOW a |
| MTA-like cements vs. CH cements | 0.29 [0.01, 5.79] | VERY LOW b | 0.87 [0.16, 4.71] | LOW a |
| MTA-like cements vs. ALL CH-based materials (CH cements + powder) | 0.93 [0.15, 5.79] | LOW | 1.17 [0.26, 5.26] | LOW a |
| CH cements vs. CH powder | No studies available | Not available | 5.41 [0.27, 108.93] | LOW a |
| Calcium-silicate cements (Biodentine, iRoot, …) vs. MTA-like cements | No studies available 4 | Not available | No studies available 4 | Not available |
| Resin-based vs. resin-free materials | 2.41 [0.48, 12.03] | VERY LOW b | 1.33 [0.44, 4.04] | MODERATE a |
| Comparison | Direct Comparison | Indirect Comparison | ||
|---|---|---|---|---|
| Relative Risk (95% CIs) | Evidence Level | Relative Risk (95% CIs) | Evidence Level | |
| Pro-Root MTA vs. calcium-hydroxide (CH) powder | No studies available 1 | Not available 1 | No studies available 1 | Not available 1 |
| Pro-Root MTA vs. CH cements (Dycal, Life, Calcipast, …) | Not available 2 | Not available | 0.54 [0.02, 15.30] | VERY LOW a |
| MTA-like cements (Pro-Root MTA, Angelus MTA, …) vs. CH powder | No studies available 3 | Not available | No studies available 3 | Not available 3 |
| MTA-like cements vs. CH cements | 0.33 [0.02, 6.65] 3 | VERY LOW a | Not available 3 | VERY LOW a |
| MTA-like cements vs. ALL CH-based materials (CH cements + powder) | 0.33 [0.02, 6.65] 3 | VERY LOW a | Not available 3 | VERY LOW a |
| CH cements vs. CH powder | No studies available | Not available | No studies available 4 | Not available |
| Calcium-silicate cements (Biodentine, iRoot, ...) vs. MTA-like cements | No studies available 5 | Not available | No studies available 5 | Not available |
| Resin-based vs. resin-free materials | No studies available 6 | Not available | No studies available 6 | Not available |
| Comparison | Direct Comparison | Indirect Comparison | ||
|---|---|---|---|---|
| Relative Risk (95% CIs) | Evidence Level | Relative Risk (95% CIs) | Evidence Level | |
| Pro-Root MTA vs. calcium hydroxide powder | No studies available | Not available | Not available 1 | Not available 1 |
| Pro-Root MTA vs. CH cements (Dycal, Life, Calcipast, …) | 0.24 [0.01, 4.72] 2 | VERY LOW | 0.34 [0.02, 6.17] | VERY LOW b |
| MTA-like cements (Pro-Root MTA, Angelus MTA, …) vs. CH powder | No studies available | Not available | Not available 3 | Not available 3 |
| MTA-like cements vs. CH cements | 0.24 [0.01, 4.72] 2 | VERY LOW 2 | 0.34 [0.02, 6.17] | VERY LOW b |
| MTA-like cements vs. ALL CH-based materials (CH cements + powder) | 0.24 [0.01, 4.72] 2 | VERY LOW 2 | 1.37 [0.07, 25.71] | VERY LOW 2 |
| CH cements vs. CH powder | No studies available | Not available | 15.42 [0.79, 299.22] | LOW a |
| Calcium-silicate cements (Biodentine, iRoot, ...) vs. MTA-like cements | No studies available 4 | Not available | No studies available 4 | Not available |
| Resin-based vs. resin-free materials | 0.84 [0.12, 5.74] | VERY LOW b | 0.84 [0.12, 5.74] 5 | VERY LOW b |
| Comparison | Direct Comparison | Indirect Comparison | ||
|---|---|---|---|---|
| Relative Risk (95% CIs) | Evidence Level | Relative Risk (95% CIs) | Evidence Level | |
| Pro-Root MTA vs. Calcium-hydroxide (CH) powder | No studies available | Not available | 1.64 [0.98, 2.77] | MODERATE a |
| Pro-Root MTA vs. CH cements (Dycal, Life, Calcipast, …) | 0.39 [0.22, 0.67] ** | HIGH | 0.56 [0.42, 0.74] *** | HIGH |
| MTA-like cements (Pro-Root MTA, Angelus MTA, …) vs. CH powder | 1.50 [0.66, 3.43] 1 | VERY LOW 1 | 2.02 [1.21, 3.36] ** | MODERATE a |
| MTA-like cements vs. CH cements | 0.41 [0.23, 0.73] ** | HIGH | 0.59 [0.45, 0.78] *** | HIGH |
| MTA-like cements vs. ALL CH-based materials (CH cements + powder) | 0.66 [0.47, 0.92] * | HIGH | 0.80 [0.62, 1.03] | HIGH |
| CH cements vs. CH powder | Not available | Not available | 3.23 [2.00, 5.20] *** | MODERATE a |
| Calcium-silicate cements (Biodentine, iRoot, ...) vs. MTA-like cements | 0.84 [0.43, 1.65] | MODERATE a | 0.81 [0.47, 1.40] | MODERATE a |
| Biodentine vs. Pro-Root MTA | 0.50 [0.04, 6.43] | VERY LOW 3 b | 0.86 [0.36, 2.02] | LOW b |
| Calcium-silicate cements vs. CH powder | Not available | Not available | 1.80 [0.95, 3.40] | LOW a b |
| Calcium-silicate cements vs. CH cements | 0.25 [0.10, 0.62] ** 2 | VERY LOW 2 | 0.47 [0.15, 1.44] | LOW a b |
| Resin-based vs. resin-free materials | 3.69 [2.23, 6.12] *** | HIGH a | Not performed 4 | Not performed |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedano, M.S.; Li, X.; Yoshihara, K.; Landuyt, K.V.; Van Meerbeek, B. Cytotoxicity and Bioactivity of Dental Pulp-Capping Agents towards Human Tooth-Pulp Cells: A Systematic Review of In-Vitro Studies and Meta-Analysis of Randomized and Controlled Clinical Trials. Materials 2020, 13, 2670. https://doi.org/10.3390/ma13122670
Pedano MS, Li X, Yoshihara K, Landuyt KV, Van Meerbeek B. Cytotoxicity and Bioactivity of Dental Pulp-Capping Agents towards Human Tooth-Pulp Cells: A Systematic Review of In-Vitro Studies and Meta-Analysis of Randomized and Controlled Clinical Trials. Materials. 2020; 13(12):2670. https://doi.org/10.3390/ma13122670
Chicago/Turabian StylePedano, Mariano S., Xin Li, Kumiko Yoshihara, Kirsten Van Landuyt, and Bart Van Meerbeek. 2020. "Cytotoxicity and Bioactivity of Dental Pulp-Capping Agents towards Human Tooth-Pulp Cells: A Systematic Review of In-Vitro Studies and Meta-Analysis of Randomized and Controlled Clinical Trials" Materials 13, no. 12: 2670. https://doi.org/10.3390/ma13122670