Mother-to-Infant Bonding in Women with Postpartum Psychosis and Severe Postpartum Depression: A Clinical Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection and Procedures
2.3. Treatment
2.4. Statistical Analysis
3. Results
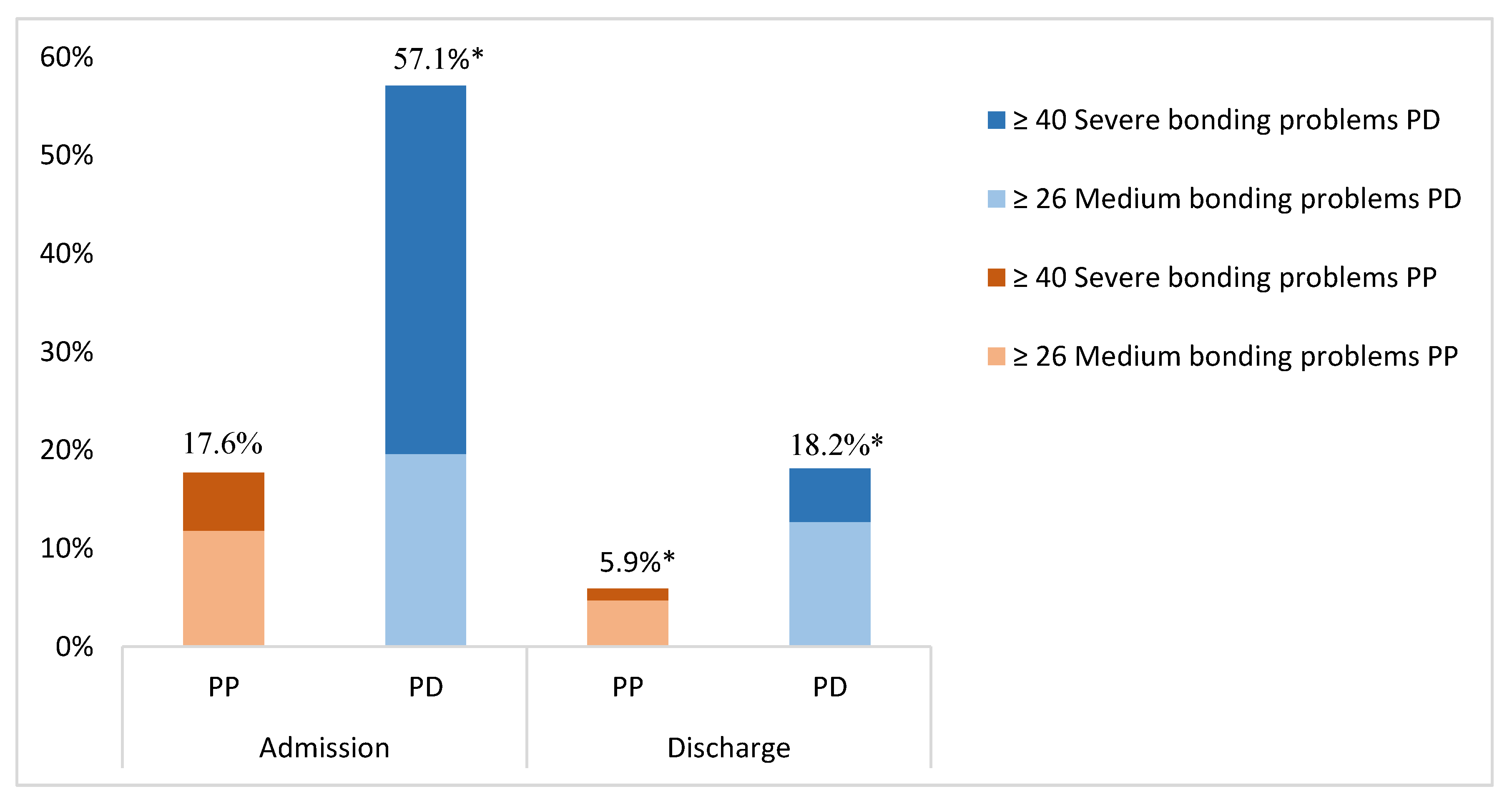
3.1. Prevalence of Impaired Mother-to-Infant Bonding at Admission and Discharge
3.2. Persistent Impaired Bonding at Discharge
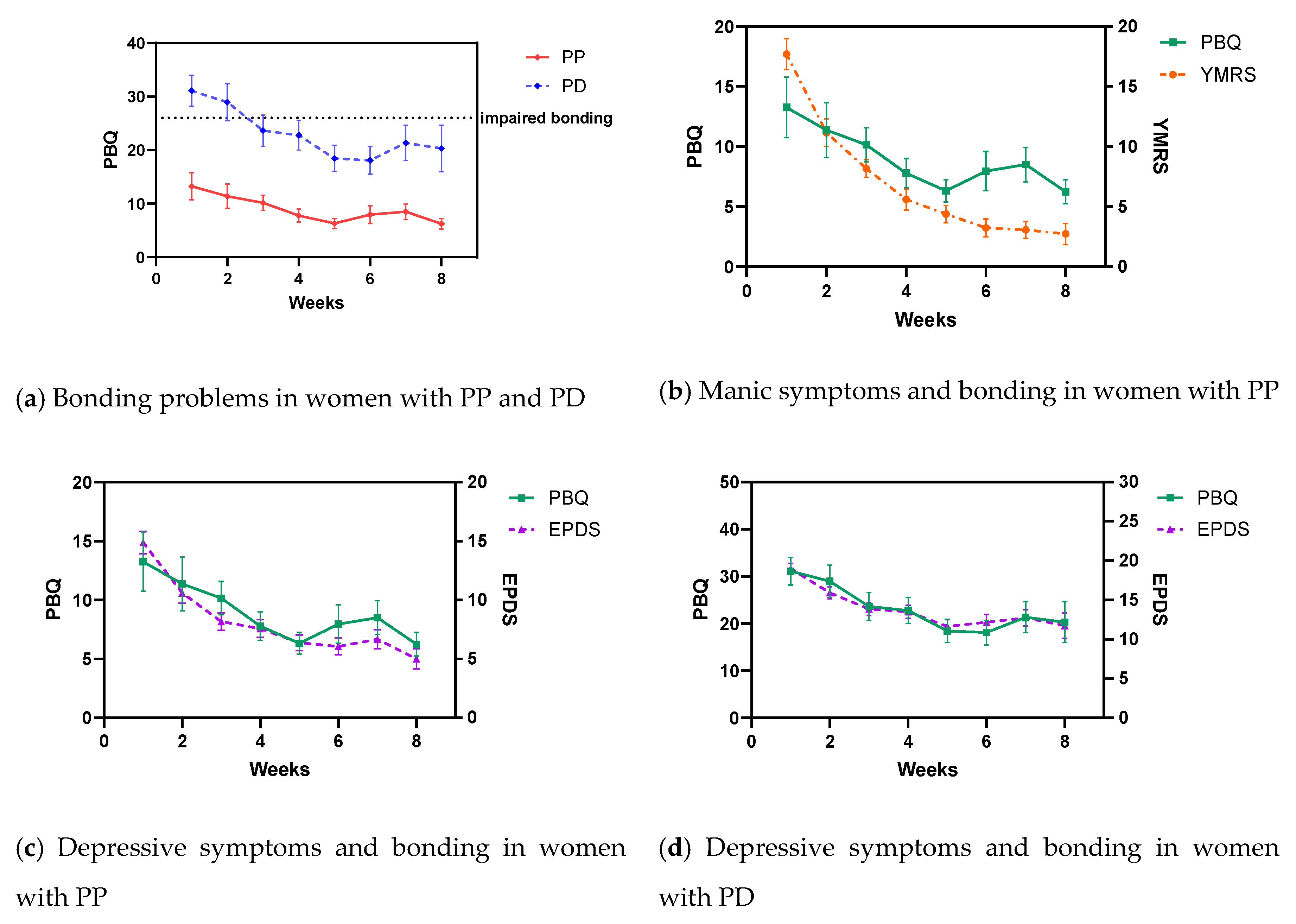
3.3. Postpartum Depressive and Manic Symptoms and the Association with Mother-to-Infant Bonding
4. Discussion
4.1. Differences in Bonding Problems between PP and PD
4.2. The Effect of Treating Depressive and Manic Symptoms on Mother-to-Infant Bonding
4.3. Strengths and Limitations
4.4. Clinical Implications
4.5. Implications for Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Laxton-Kane, M.; Slade, P. The role of maternal prenatal attachment in a woman’s experience of pregnancy and implications for the process of care. J. Reprod. Infant Psychol. 2002, 20, 253–266. [Google Scholar] [CrossRef]
- Siddiqui, A.; Hägglöf, B. Does maternal prenatal attachment predict postnatal mother-infant interaction? Early Hum. Dev. 2000, 59, 13–25. [Google Scholar] [CrossRef]
- O’Higgins, M.; Roberts, I.S.J.; Glover, V.; Taylor, A. Mother-child bonding at 1 year; associations with symptoms of postnatal depression and bonding in the first few weeks. Arch. Women’s Ment. Health 2013, 16, 381–389. [Google Scholar] [CrossRef]
- Kinsey, C.B.; Hupcey, J.E. State of the science of maternal–infant bonding: A principle-based concept analysis. Midwifery 2013, 29, 1314–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, A.; Möhler, E.; Reck, C.; Resch, F.; Kaess, M. The Early Mother-to-Child Bond and Its Unique Prospective Contribution to Child Behavior Evaluated by Mothers and Teachers. Psychopatholgy 2016, 49, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Enns, M.W.; Cox, B.J.; Clara, I. Parental bonding and adult psychopathology: Results from the US National Comorbidity Survey. Psychol. Med. 2002, 32, 997–1008. [Google Scholar] [CrossRef]
- De Cock, E.S.A.; Henrichs, J.; Klimstra, T.A.; Maas, A.J.B.M.; Vreeswijk, C.M.J.M.; Meeus, W.H.J.; Van Bakel, H.J.A. Longitudinal Associations Between Parental Bonding, Parenting Stress, and Executive Functioning in Toddlerhood. J. Child. Fam. Stud. 2017, 26, 1723–1733. [Google Scholar] [CrossRef] [Green Version]
- Brockington, I. Postpartum psychiatric disorders. Lancet 2004, 363, 1078. [Google Scholar] [CrossRef]
- Di Florio, A.; Forty, L.; Gordon-Smith, K.; Heron, J.; Jones, L.; Craddock, N.; Jones, I. Perinatal Episodes Across the Mood Disorder Spectrum. Jama Psychiatry 2013, 70, 168–175. [Google Scholar] [CrossRef] [Green Version]
- Woody, C.; Ferrari, A.; Siskind, D.; Whiteford, H.A.; Harris, M. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Bergink, V.; Rasgon, N.; Wisner, K.L. Postpartum Psychosis: Madness, Mania, and Melancholia in Motherhood. Am. J. Psychiatry 2016, 173, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Munk-Olsen, T.; Laursen, T.M.; Pedersen, C.B.; Mors, O.; Mortensen, P.B. New Parents and Mental Disorders. JAMA 2006, 296, 2582–2589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brockington, I.F. What Is Worth Knowing about Puerperal Psychosis; Eyry Press: Dubai, UK, 2014. [Google Scholar]
- Valdimarsdóttir, U.; Hultman, C.M.; Harlow, B.L.; Cnattingius, S.; Sparén, P. Psychotic Illness in First-Time Mothers with No Previous Psychiatric Hospitalizations: A Population-Based Study. PLoS Med. 2009, 6, e1000013. [Google Scholar] [CrossRef] [PubMed]
- Wesseloo, R.; Kamperman, A.M.; Munk-Olsen, T.; Pop, V.; Kushner, S.A.; Bergink, V. Risk of Postpartum Relapse in Bipolar Disorder and Postpartum Psychosis: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2016, 173, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Bergink, V.; Kushner, S.A.; Berg, M.P.L.-V.D.; Koorengevel, K.M.; Kupka, R. First-Onset Psychosis Occurring in the Postpartum Period. J. Clin. Psychiatry 2011, 72, 1531–1537. [Google Scholar] [CrossRef]
- Wisner, K.L.; Peindl, K.; Hanusa, B.H. Symptomatology of affective and psychotic illnesses related to childbearing. J. Affect. Disord. 1994, 30, 77–87. [Google Scholar] [CrossRef]
- Kendell, R.E.; Chalmers, J.C.; Platz, C. Epidemiology of Puerperal Psychoses. Br. J. Psychiatry 1987, 150, 662–673. [Google Scholar] [CrossRef]
- Glangeaud-Freudenthal, N.M.-C.; Sutter, A.-L.; Thieulin, A.-C.; Dagens-Lafont, V.; Zimmermann, M.-A.; Debourg, A.; Massari, B.; Cazas, O.; Cammas, R.; Rainelli, C.; et al. Inpatient mother-and-child postpartum psychiatric care: Factors associated with improvement in maternal mental health. Eur. Psychiatry 2011, 26, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, M.C.; Lara-Cinisomo, S.; Melvin, K.; Di Florio, A.; Brandon, A.; Meltzer-Brody, S. Treatment of severe perinatal mood disorders on a specialized perinatal psychiatry inpatient unit. Arch. Women’s Ment. Health 2016, 19, 645–653. [Google Scholar] [CrossRef]
- Chandra, P.S.; Desai, G.; Reddy, D.; Thippeswamy, H.; Saraf, G. The establishment of a mother-baby inpatient psychiatry unit in India: Adaptation of a Western model to meet local cultural and resource needs. Indian J. Psychiatry 2015, 57, 290–294. [Google Scholar] [CrossRef]
- Bergink, V.; Burgerhout, K.M.; Koorengevel, K.M.; Kamperman, A.M.; Hoogendijk, W.J.; Berg, M.L.-V.D.; Kushner, S.A. Treatment of Psychosis and Mania in the Postpartum Period. Am. J. Psychiatry 2015, 172, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Dubber, S.; Reck, C.; Müller, M.; Gawlik, S. Postpartum bonding: The role of perinatal depression, anxiety and maternal–fetal bonding during pregnancy. Arch. Women’s Ment. Health 2014, 18, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Moehler, E.; Brunner, R.; Wiebel, A.; Reck, C.; Resch, F. Maternal depressive symptoms in the postnatal period are associated with long-term impairment of mother–child bonding. Arch. Women’s Ment. Health 2006, 9, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Tietz, A.; Zietlow, A.-L.; Reck, C. Maternal bonding in mothers with postpartum anxiety disorder: The crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch. Women’s Ment. Health 2014, 17, 433–442. [Google Scholar] [CrossRef]
- Milgrom, J.; Westley, D.T.; Gemmill, A.W. The mediating role of maternal responsiveness in some longer term effects of postnatal depression on infant development. Infant Behav. Dev. 2004, 27, 443–454. [Google Scholar] [CrossRef]
- Tichelman, E.; Westerneng, M.; Witteveen, A.B.; Van Baar, A.L.; Van Der Horst, H.E.; De Jonge, A.; Berger, M.Y.; Schellevis, F.G.; Burger, H.; Peters, L.L. Correlates of prenatal and postnatal mother-to-infant bonding quality: A systematic review. PLoS ONE 2019, 14, e0222998. [Google Scholar] [CrossRef] [Green Version]
- Kamperman, A.M.; Veldman-Hoek, M.J.; Wesseloo, R.; Blackmore, E.R.; Bergink, V. Phenotypical characteristics of postpartum psychosis: A clinical cohort study. Bipolar Disord. 2017, 19, 450–457. [Google Scholar] [CrossRef]
- Chasson, G.S.; Williams, M.T.; Davis, D.M.; Combs, J.Y. Missed diagnoses in African Americans with obsessive-compulsive disorder: The structured clinical interview for DSM-IV Axis I disorders (SCID-I). BMC Psychiatry 2017, 17, 258. [Google Scholar] [CrossRef] [Green Version]
- Brockington, I.F.; Oates, J.; George, S.; Turner, D.; Vostanis, P.; Sullivan, M.; Loh, C.; Murdoch, C. A Screening Questionnaire for mother-infant bonding disorders. Arch. Women’s Ment. Health 2001, 3, 133–140. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Pop, V.J.; Komproe, I.H.; Van Son, M.J. Characteristics of the Edinburgh post natal depression scale in The Netherlands. J. Affect. Disord. 1992, 26, 105–110. [Google Scholar] [CrossRef]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Tohen, M.; Jacobs, T.G.; Grundy, S.L.; McElroy, S.L.; Banov, M.C.; Janicak, P.G.; Sanger, T.; Risser, R.; Zhang, F.; Toma, V.; et al. Efficacy of olanzapine in acute bipolar mania: A double-blind, placebo-controlled study. The Olanzipine HGGW Study Group. Arch. Gen. Psychiatry 2000, 57, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Noorlander, Y.; Bergink, V.; Berg, M.P.V.D. Perceived and observed mother–child interaction at time of hospitalization and release in postpartum depression and psychosis. Arch. Women’s Ment. Heal. 2008, 11, 49–56. [Google Scholar] [CrossRef]
- Fox, J. Applied Regression Analysis and Generalized Linear Models; Sage Publications: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Upadhyaya, S.K.; Sharma, A.; Raval, C.M. Postpartum Psychosis: Risk Factors Identification. N. Am. J. Med. Sci. 2014, 6, 274–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, I.; Craddock, N. Familiality of the puerperal trigger in bipolar disorder: Results of a family study. Am. J. Psychiatry 2001, 158, 913–917. [Google Scholar] [CrossRef]
- Farré-Sender, B.; Andrés, S.; Roca, A.; Lasheras, G.; Valdés, M.; Garcia-Esteve, L.; Torres, A.; Gelabert, E. Mother–infant bonding in the postpartum period: Assessment of the impact of pre-delivery factors in a clinical sample. Arch. Women’s Ment. Health 2017, 21, 287–297. [Google Scholar] [CrossRef]
- Hornstein, C.; Trautmann-Villalba, P.; Hohm, E.; Rave, E.; Wortmann-Fleischer, S.; Schwarz, M. Maternal bond and mother–child interaction in severe postpartum psychiatric disorders: Is there a link? Arch. Women’s Ment. Health 2006, 9, 279–284. [Google Scholar] [CrossRef]
- Bienfait, M.; Maury, M.; Haquet, A.; Faillie, J.-L.; Franc, N.; Combes, C.; Daudé, H.; Picaud, J.-C.; Rideau, A.; Cambonie, G. Pertinence of the self-report mother-to-infant bonding scale in the neonatal unit of a maternity ward. Early Hum. Dev. 2011, 87, 281–287. [Google Scholar] [CrossRef]
- Reck, C.; Klier, C.M.; Pabst, K.; Stehle, E.; Steffenelli, U.; Struben, K.; Backenstrass, M. The German version of the Postpartum Bonding Instrument: Psychometric properties and association with postpartum depression. Arch. Women’s Ment. Health 2006, 9, 265–271. [Google Scholar] [CrossRef]
- Taylor, A.; Atkins, R.; Kumar, R.; Adams, D.; Glover, V. A new Mother-to-Infant Bonding Scale: Links with early maternal mood. Arch. Women’s Ment. Health 2005, 8, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Klier, C.M. Mother–infant bonding disorders in patients with postnatal depression: The Postpartum Bonding Questionnaire in clinical practice. Arch. Women’s Ment. Health 2006, 9, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.; Heron, J.; Francomb, H.; Oke, S.; Golding, J. Cohort study of depressed mood during pregnancy and after childbirth. BMJ 2001, 323, 257–260. [Google Scholar] [CrossRef] [Green Version]
- Limlomwongse, N.; Liabsuetrakul, T. Cohort study of depressive moods in Thai women during late pregnancy and 6–8 weeks of postpartum using the Edinburgh Postnatal Depression Scale (EPDS). Arch. Women’s Ment. Health 2005, 9, 131–138. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Postpartum Psychosis (n = 91) | Postpartum Depression (n = 64) | p-Value | |
|---|---|---|---|
| Maternal age at admission (yr), mean (SD) | 31.0 (4.7) | 30.0 (8.0) | 0.32 |
| Length of admission (wks), mean (SD) | 7.9 (4.3) | 7.5 (4.8) | 0.52 |
| Dutch nationality, n (%) | 83 (92.2) | 55 (90.2) | 0.66 |
| Relationship, yes, n (%) | 88 (97.8) | 55 (93.2) | 0.21 |
| Primary/Secondary education only, n (%) | 44 (48.4) | 33 (60.0) | 0.17 |
| Primiparous, n (%) | 68 (78.2) | 40 (64.5) | 0.09 |
| Psychiatric history, n (%) | |||
| None | 44 (48.4) | 25 (39.1) | 0.14 |
| Prior postpartum episode | 11 (12.1) | 4 (26.7) | |
| Prior non-postpartum episode | 36 (39.6) | 35 (54.7) | |
| EPDS score at admission, mean (SD) | 14.9 (6.0) | 19.0 (4.9) | 0.001 * |
| YMRS score at admission, mean (SD) | 17.7 (11.5) | n.a. | n.a. |
| Family history of psychiatric disorder, n (%) | 51 (56.0) | 20 (35.0) | 0.013 * |
| Infant age at admission (wks), median (IQR) | 2.0 (3.7) | 6.0 (5.2) | <0.001 * |
| Gender infant, male, n (%) | 45 (50.0) | 26 (43.3) | 0.51 |
| Fixed Effects | Unadjusted Estimate | Sig. | Adjusted Estimate | Sig. |
|---|---|---|---|---|
| Linear mixed effects model in PP group | ||||
| Intercept | 2.62 | 0.02 | 7.96 | 0.22 |
| EPDS | 0.76 | 0.00 | 0.76 | 0.00 |
| YMRS | 0.16 | 0.02 | 0.16 | 0.02 |
| Linear mixed effects model in PD group | ||||
| Intercept | 8.30 | 0.00 | 1.98 | 0.88 |
| EPDS | 1.05 | 0.00 | 1.05 | 0.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilden, J.; Molenaar, N.M.; Smit, A.K.; Hoogendijk, W.J.G.; Rommel, A.-S.; Kamperman, A.M.; Bergink, V. Mother-to-Infant Bonding in Women with Postpartum Psychosis and Severe Postpartum Depression: A Clinical Cohort Study. J. Clin. Med. 2020, 9, 2291. https://doi.org/10.3390/jcm9072291
Gilden J, Molenaar NM, Smit AK, Hoogendijk WJG, Rommel A-S, Kamperman AM, Bergink V. Mother-to-Infant Bonding in Women with Postpartum Psychosis and Severe Postpartum Depression: A Clinical Cohort Study. Journal of Clinical Medicine. 2020; 9(7):2291. https://doi.org/10.3390/jcm9072291
Chicago/Turabian StyleGilden, Janneke, Nina M. Molenaar, Anne K. Smit, Witte J. G. Hoogendijk, Anna-Sophie Rommel, Astrid M. Kamperman, and Veerle Bergink. 2020. "Mother-to-Infant Bonding in Women with Postpartum Psychosis and Severe Postpartum Depression: A Clinical Cohort Study" Journal of Clinical Medicine 9, no. 7: 2291. https://doi.org/10.3390/jcm9072291