Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
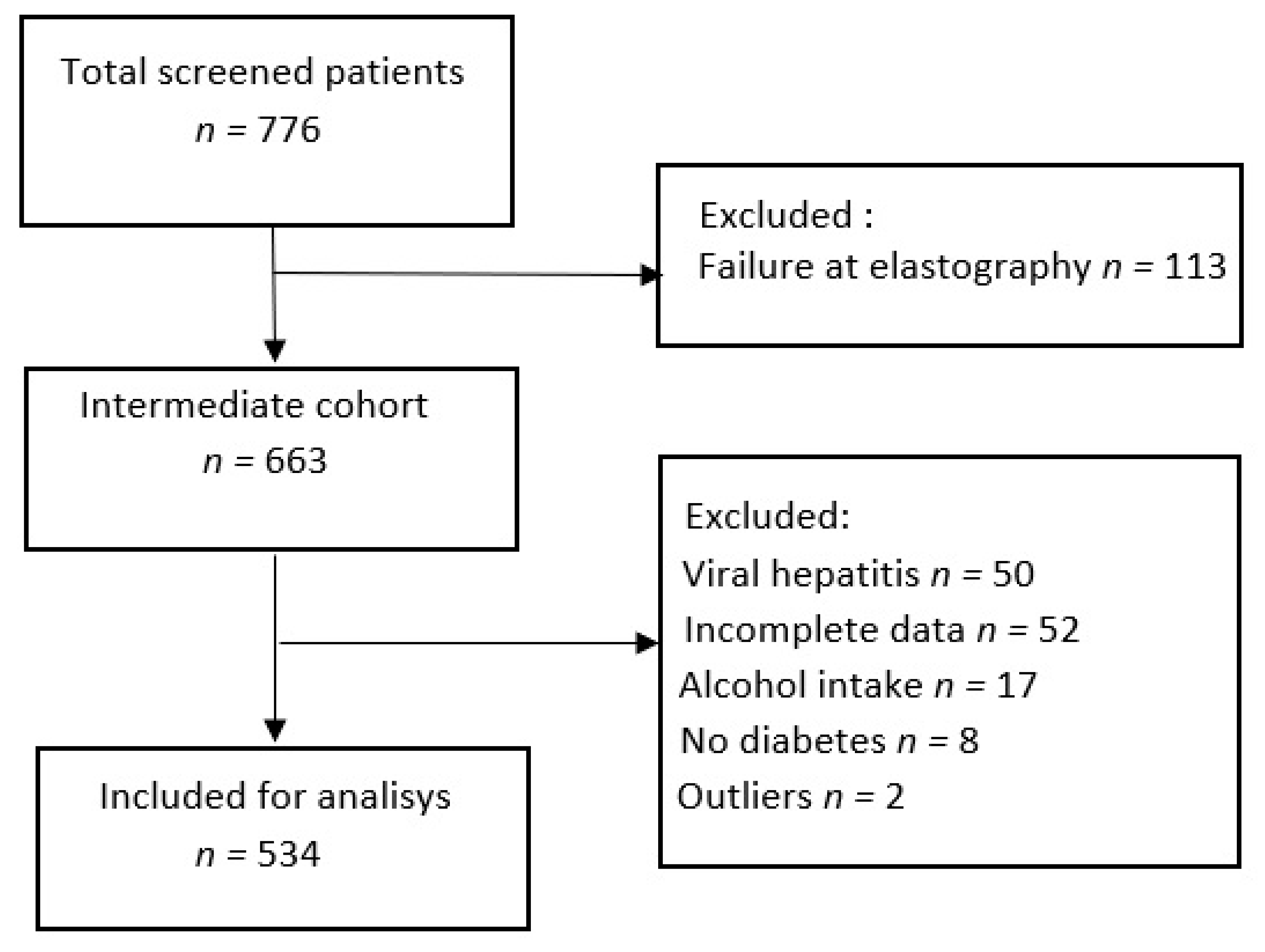
2.1. Study Population
2.2. Clinical Assessment
2.3. Vibration Controlled Transient Elastography (VTCE) and Controlled Attenuation Parameter (CAP) Measurements
2.4. Surogate Serum Fibrosis Markers
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Factors Associated with Severe Steatosis at CAP
3.3. Factors Associated with Advanced Fibrosis (F3) by VCTE
3.4. Factors Associated with Significant Fibrosis (F2) by VCTE
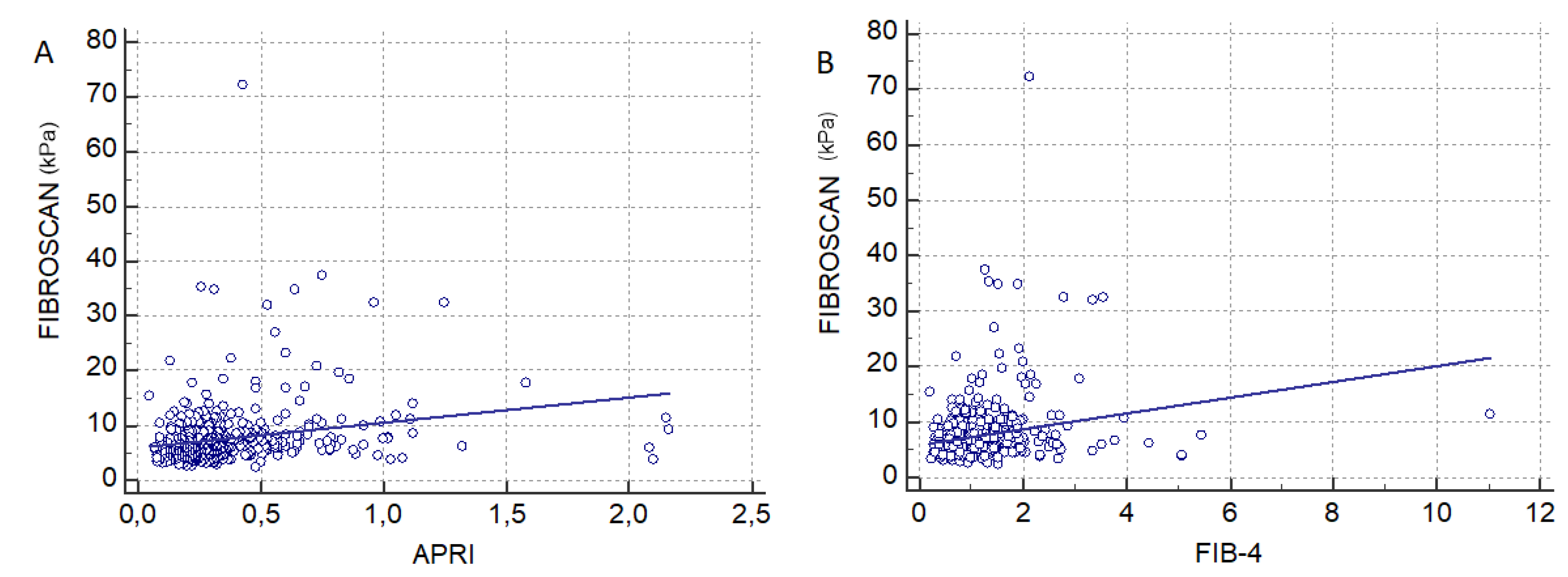
3.5. Comparison of Transient Elastography with FIB-4 and APRI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Younossi, Z.; Koenig, A.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perumpail, B.; Khan, M.; Yoo, E.; Cholankeril, G.; Kim, D.; Ahmed, A. Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J. Gastroenterol. 2017, 23, 8263–8276. [Google Scholar] [CrossRef] [PubMed]
- Björkström, K.; Franzén, S.; Eliasson, B.; Miftaraj, M.; Gudbjörnsdottir, S.; Trolle-Lagerros, Y.; Svensson, A.M.; Hagström, H. Risk factors for severe liver disease in patients with type 2 diabetes. Clin. Gastroenterol. Hepatol. 2019, 17, 2769–2775.e4. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Hossain, F.; Horsfall, L.; Banh, X.; Hayward, K.L.; Williams, S.; Johnson, T.; Bernard, A.; Brown, N.N.; Lampe, G.; et al. A pragmatic approach identifies a high rate of nonalcoholic fatty liver disease with advanced fibrosis in diabetes clinics and at-risk populations in primary care. Hepatol. Commun. 2018, 2, 897–909. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.; Tampi, R.; Racila, A.; Qiu, Y.; Burns, L.; Younossi, I.; Nader, F. Economic and clinical burden of nonalcoholic steatohepatitis in patients with type 2 diabetes in the U.S. Diabetes Care 2020, 43, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Roulot, D.; Roudot-Thoraval, F.; NKontchou, G.; Kouacou, N.; Costes, J.L.; Elourimi, G.; Le Clesiau, H.; Ziot, M.; Beaugrand, M. Concomitant screening for liver fibrosis and steatosis in French type 2 diabetic patients using Fibroscan. Liver Int. 2017, 37, 1897–1906. [Google Scholar] [CrossRef]
- Demir, M.; Deyneli, O.; Yilmaz, Y. Screening for hepatic fibrosis and steatosis in Turkish patients with type 2 diabetes mellitus: A transient elastography study. Turk. J. Gastroenterol. 2019, 30, 266–270. [Google Scholar] [CrossRef] [Green Version]
- Castéra, L.; Foucher, J.; Bernard, P.H.; Carvalho, F.; Allaix, D.; Merrouche, W.; Couzigou, P.; de Lédinghen, V. Pitfalls of liver stiffness measurement: A 5-year prospective study of 13,369 examinations. Hepatology 2010, 51, 828–835. [Google Scholar] [CrossRef]
- Sporea, I.; Șirli, R.; Mare, R.; Popescu, A.; Ivascu, C. Feasibility of Transient Elastography with M and XL probes in real life. Med. Ultrason. 2016, 18, 7. [Google Scholar] [CrossRef] [Green Version]
- Sasso, M.; Beaugrand, M.; de Ledinghen, V.; Douvin, C.; Marcellin, P.; Poupon, R.; Sandrin, L.; Miette, V. Controlled Attenuation Parameter (CAP): A novel VCTE™ guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: Preliminary study and validation in a cohort of patients with chronic liver disease from various causes. Ultrasound Med. Biol. 2010, 36, 1825–1835. [Google Scholar] [CrossRef]
- Ekstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019. Diabetes Care 2018, 42 (Suppl. 1), S13–S28. [CrossRef] [Green Version]
- EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [CrossRef] [PubMed] [Green Version]
- Dietrich, C.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H. EFSUMB guidelines and recommendations on the clinical use of liver ultrasound elastography, update 2017 (long version). Ultraschall Med. Eur. J. Ultrasound 2017, 38, e16–e47. [Google Scholar] [CrossRef] [Green Version]
- Sandrin, L.; Fourquet, B.; Hasquenoph, J.; Yon, S.; Fournier, C.; Mal, F.; Christidis, C.; Ziol, M.; Poulet, B.; Kazemi, F.; et al. Transient elastography: A new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med. Biol. 2003, 29, 1705–1713. [Google Scholar] [CrossRef]
- Eddowes, P.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V. Accuracy of FibroScan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [Green Version]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [Green Version]
- McPherson, S.; Stewart, S.F.; Henderson, E.; Burt, A.D.; Day, C.P. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut 2010, 59, 1265–1269. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.; Plompen, E.; Schouten, J.; Hansen, B.E.; Darwish Murad, S.; Taimr, P.; Leebeek, F.W.; Hofman, A.; Stricker, B.H.; Castera, L.; et al. Presence of diabetes mellitus and steatosis is associated with liver stiffness in a general population: The Rotterdam study. Hepatology 2015, 63, 138–147. [Google Scholar] [CrossRef] [Green Version]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [Green Version]
- Lupșor-Platon, M.; Feier, D.; Stefănescu, H.; Tamas, A.; Botan, E.; Sparchez, Z.; Maniu, A.; Badea, R. Diagnostic accuracy of CAP measurement by TE for non-invasive assessment of liver steatosis: A prospective study. J. Gastrointest. Liver Dis. 2015, 24, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Karlas, T.; Petroff, D.; Sasso, M.; Fan, J.G.; Mi, Y.Q.; de Lédinghen, V.; Kumar, M.; Lupsor-Platon, M.; Han, K.H.; Cardoso, A.C.; et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J. Hepatol. 2017, 66, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- de Lédinghen, V.; Vergniol, J.; Capdepont, M.; Chermak, F.; Hiriart, J.B.; Cassinotto, C.; Merrouche, W.; Foucher, J.; Brigitte, L.B. Controlled attenuation parameter (CAP) for the diagnosis of steatosis: A prospective study of 5323 examinations. J. Hepatol. 2014, 60, 1026–1031. [Google Scholar] [CrossRef]
- Wong, V.; Irles, M.; Wong, G.; Shili, S.; Chan, A.W.; Merrouche, W.; Shu, S.S.; Foucher, J.; Le Bail, B.; Chan, W.K.; et al. Unified interpretation of liver stiffness measurement by M and XL probes in non-alcoholic fatty liver disease. Gut 2019, 68, 2057–2064. [Google Scholar] [CrossRef]
- Chan, W.; Nik Mustapha, N.; Mahadeva, S.; Wong, V.W.; Cheng, J.Y.; Wong, G.L. Can the same controlled attenuation parameter cut-offs be used for M and XL probes for diagnosing hepatic steatosis? J. Gastroenterol. Hepatol. 2018, 33, 1787–1794. [Google Scholar] [CrossRef]
- Caussy, C.; Alquiraish, M.; Nguyen, P.; Hernandez, C.; Cepin, S.; Fortney, L.E.; Ajmera, V.; Bettencourt, R.; Collier, S.; Hooker, J.; et al. Optimal threshold of controlled attenuation parameter with MRI-PDFF as the gold standard for the detection of hepatic steatosis. Hepatology 2018, 67, 1348–1359. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Nguyen, P.; Hernandez, C.; Bettencourt, R.; Ramirez, K.; Fortney, L.; Hooker, J.; Sy, E.; Savides, M.T.; Alquiraish, M.H.; et al. Magnetic resonance elastography vs. transient elastography in detection of fibrosis and noninvasive measurement of steatosis in patients with biopsy-proven nonalcoholic fatty liver disease. Gastroenterology 2017, 152, 598–607.e2. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, Y.; Kuroda, H.; Abe, T.; Ishida, K.; Oguri, T.; Noguchi, S.; Sugai, T.; Kamiyama, N.; Takikawa, Y. The B-Mode Image-Guided Ultrasound Attenuation Parameter Accurately Detects Hepatic Steatosis in Chronic Liver Disease. Ultrasound Med. Biol. 2018, 44, 2223–2232. [Google Scholar] [CrossRef]
- Tamaki, N.; Koizumi, Y.; Hirooka, M.; Yada, N.; Takada, H.; Nakashima, O.; Kudo, M.; Hiasa, Y.; Izumi, N. Novel quantitative assessment system of liver steatosis using a newly developed attenuation measurement method. Hepatol. Res. 2018, 48, 821–828. [Google Scholar] [CrossRef]
- Ferraioli, G.; Maiocchi, L.; Raciti, M.; Tinalli, C.; De Silvestri, A.; Nichetti, M.; De Cata, P.; Rondanelli, M.; Chiovato, L.; Calliada, F.; et al. Detection of liver steatosis with a novel ultrasound-based technique. Clin. Transl. Gastroenterol. 2019, 10, e00081. [Google Scholar] [CrossRef]
- Bae, J.; Lee, D.; Lee, J.; Kim, H.; Yu, S.j.; Lee, J.H.; Cjo, E.J.; Lee, Y.B.; Han, J.K.; Choi, B. Assessment of hepatic steatosis by using attenuation imaging: A quantitative, easy-to-perform ultrasound technique. Eur. Radiol. 2019, 29, 6499–6507. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G.; Filice, C.; Castera, L.; Choi, B.; Sporea, I.; Wilson, S.; Cosgrove, D.; Dietrich, C.; Amy, D.; Bamber, J.; et al. WFUMB Guidelines and Recommendations for Clinical Use of Ultrasound Elastography: Part3: Liver. Ultrasound Med. Biol. 2015, 41, 1161–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilar-Gomez, E.; Calzadilla-Bertot, L.; Wai-Sun Wong, V.; Castellanos, M.; Aller-de la Fuente, R.; Metwally, M.; Eslam, M.; Gonzalez-Fabian, L.; Alvarez-Quiñones Sanz, M.; Conde-Martin, A.F.; et al. Fibrosis severity as a determinant of cause-specific mortality in patients with advanced nonalcoholic fatty liver disease: A multi-national cohort study. Gastroenterology 2018, 155, 443–457.e17. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Shili, S.; Zuberbuhler, F.; Hiriart, J.B.; Lannes, A.; Chermak, F.; Hunault, G.; Foucher, J.; Oberti, F.; Fouchard-Hubert, I.; et al. Liver stiffness measurement with fibroscan. Clin. Transl. Gastroenterol. 2019, 10, e00023. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Cheong, J.Y.; Um, S.H.; Seo, Y.S.; Kim, D.J.; Hwang, S.G.; Yang, J.M.; Han, K.H.; Cho, S.W. Comparison of surrogate serum markers and transient elastography (fibroscan) for assessing cirrhosis in patients with chronic viral hepatitis. Dig. Dis. Sci. 2010, 55, 3552–3560. [Google Scholar] [CrossRef] [PubMed]
- Castera, L.; Le Bail, B.; Roudot-Thoraval, F.; Bernard, P.H.; Foucher, J.; Merrouche, W.; Couzigou, P.; de Ledinghen, V. Early detection in routine clinical practice of cirrhosis and oeshophageal carices in chronic hepatitis C: Comparison of transient elastography (Fibroscan) with standard laboratory tests and non-invasive scores. J. Hepatol. 2009, 50, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.; Alex, F.; Robert, P. Fibrotest and fibroscan for the prediction of hepatitis C-related fibrosis: A systemic review of diagnostic test accuracy. Am. J. Gastroenterol. 2007, 102, 2589–2600. [Google Scholar]



{kind=link}
{kind=link}
| Parameter | Study Group (n = 534) | Excluded Group (n = 242) | p-Value |
|---|---|---|---|
| Age, years (means) | 60.8 ± 8.7 | 61.5 ± 7 | 0.27 |
| Gender (n,%) | |||
| Male | 251 (47.1%) | 87 (35.9%) | 0.004 |
| Female | 283 (52.9%) | 155 (64.1%) | 0.004 |
| BMI (kg/m2) (mean ± SD) | 32 ± 6 | 35.01 ± 6 | <0.0001 |
| Hypertension (n,%) | 295 (55.2%) | 131 (54.1%) | 0.83 |
| Waist circumference (median, range) | 108 (68–148) | 110 (92–155) | <0.01 |
| AST, IU/L (median, range) | 23 (7–150) | 36 (20–152) | <0.0001 |
| ALT, IU/L (median, range) | 36 (9–160) | 50.4 (14.8–176) | <0.0001 |
| Platelets × 103/mm3 (median, range) | 242 (71–450) | 234 (67–602) | 0.83 |
| Total cholesterol, mg/dL (median, range) | 179 (70–418) | 182 (87–879) | 0.65 |
| Triglycerides, mg/dL (median, range) | 149 (30–887) | 220 (29–8000) | <0.001 |
| LDL, mg/dL (median, range) | 105 (7–262) | 107(34–277) | 0.37 |
| HDL, mg/dL (median, range) | 35 (10–120) | 40 (13–120) | 0.58 |
| LSM, kPa (mean ± SD) | 7.73 ± 5.7 | 13.2 ± 7.1 | <0.0001 |
| CAP, dB/m (mean ± SD) | 317 ± 59.5 | 336 ± 61.1 | <0.0001 |
| Fibrosis stage | n = 534 | n = 69 | |
| F0-1 | 388 (72.6%) | 26 (37.6%) | <0.0001 |
| F2 | 42 (7.8%) | 6 (10.1%) | 0.35 |
| F3 | 61 (11.4%) | 6 (10.1%) | 0.68 |
| F4 | 43 (8.2%) | 31 (42.2%) | <0.0001 |
| Steatosis stage | n = 534 | n = 69 | |
| S0 | 127 (23.9%) | 19 (27.5%) | 0.32 |
| S1 | 48 (8.9%) | 5 (7.2%) | 0.51 |
| S2 | 37 (6.9%) | 4 (5.7%) | 0.63 |
| S3 | 322 (60.3%) | 41 (59.6%) | 0.91 |
| Insulin | 106 (19.7%) | 79 (32.9%) | 0.0001 |
| Oral antidiabetics | 328 (61.4%) | 107 (44.2%) | <0.0001 |
| T2DM duration | 10 ± 2.0 | 15 ± 4.1 | <0.0001 |
| Parameter | Normal Weight (n = 57) | Overweight (n = 150) | Obesity (n = 327) | p-Value |
|---|---|---|---|---|
| Age, years (means) | 62 ± 8.6 | 61.1 ± 10.3 | 59.7 ± 9.71 | 0.09 |
| Gender (n,%) | ||||
| Male | 25 (43.8%) | 72 (48%) | 154 (47.1%) | 0.75 |
| Female | 32 (56.2%) | 78 (52%) | 173 (52.9%) | 0.75 |
| BMI (kg/m2) (mean ± SD) | 22.8±1.9 | 27.7±1.4 | 35.5±4.6 | <0.0001 |
| Hypertension (n,%) | 30 (52.63%) | 77 (50.9%) | 188 (57.3%) | 0.63 |
| Waist circumference (median, range) | 90 (68–110) | 100 (70–118) | 115 (90–148) | 0.75 |
| AST, IU/L (median, range) | 23 (12–132) | 21 (9–136) | 24 (7–150) | 0.42 |
| ALT, IU/L (median, range) | 34 (14–120) | 36 (13–143) | 37 (9–160) | 0.98 |
| Platelets × 103/mm3 (median, range) | 242 (78–418) | 236 (71–441) | 245 (82–602) | 0.50 |
| Total cholesterol, mg/dL (median, range) | 184 (96–288) | 186 (70–400) | 194 (77–418) | 0.08 |
| Triglycerides, mg/dL (median, range) | 141 (30–582) | 146 (50–598) | 160 (43–887) | 0.10 |
| LDL, mg/dL (median, range) | 114 (7–205) | 107 (12–215) | 110 (17–262) | 0.35 |
| HDL, mg/dL (median, range) | 47 (25–120) | 41 (7–121) | 40 (10–131) | 0.51 |
| LSM, kPa (mean ± SD) | 6.92 ± 5.85 | 7.21 ± 2.1 | 8.32 ± 6.34 | 0.03 |
| CAP, dB/m (mean ± SD) | 255.56 ± 60.8 | 300.9 ± 55.8 | 335.2 ± 51.2 | <0.0001 |
| Fibrosis stage | ||||
| F0-1 | 45 (78.9%) | 121 (80.6%) | 222 (67.9%) | 0.93 |
| F2 | 4 (7%) | 11 (7.3%) | 29 (8.8%) | 0.82 |
| F3 | 5 (8.7%) | 12 (8%) | 42 (13%) | 0.90 |
| F4 | 3 (5.4%) | 6 (4%) | 34 (10.3%) | 0.95 |
| Steatosis stage | ||||
| S0 | 36 (63.1%) | 45 (29.9%) | 46 (14.1%) | <0.0001 |
| S1 | 6 (10.5%) | 19 (12.5%) | 23 (7%) | <0.0001 |
| S2 | 1 (1.9%) | 12 (8%) | 24 (7.4%) | 0.2 |
| S3 | 14 (24.5%) | 75 (49.6%) | 234 (71.5%) | <0.0001 |
| Insulin | 10 (18%) | 46 (30%) | 50 (52%) | <0.0001 |
| Oral antidiabetics | 22 (6.6%) | 126 (38.1%) | 182 (55.1%) | <0.0001 |
| T2DM duration | 8 ± 1.2 | 9 ± 2.3 | 13 ± 1.4 | 0.34 |
| Variable | Overall | Normal Weight | Overweight | Obesity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ß | SE | p-Value | ß | SE | p-Value | ß | SE | p-Value | ß | SE | p-Value | |
| Age | 0.84 | 0.002 | 0.06 | 0.28 | 0.4 | 0.93 | 0.61 | 0.24 | 0.61 | 0.89 | 0.15 | 0.25 |
| Female gender | –0.60 | 0.02 | <0.0001 | 0.45 | 0.05 | 0.01 | 0.10 | 0.02 | 0.47 | 0.54 | 0.01 | 0.54 |
| BMI | 0.02 | 0.003 | <0.0001 | 0.02 | 0.02 | 0.35 | 0.03 | 0.02 | 0.30 | 0.08 | 0.18 | 0.0008 |
| Waist circumference | –0.69 | 0.17 | <0.0001 | 0.01 | 0.006 | 0.006 | 0.36 | 0.41 | 0.02 | 0.14 | 0.2 | 0.001 |
| AST | 0.52 | 0.03 | 0.03 | 0.18 | 0.1 | 0.39 | 0.48 | 0.07 | 0.79 | 0.61 | 0.04 | 0.001 |
| ALT | 0.60 | 0.02 | 0.41 | 0.18 | 0.09 | 0.40 | 0.36 | 0.08 | 0.07 | 0.71 | 0.02 | 0.52 |
| Total cholesterol | 0.41 | 0.08 | 0.01 | 0.01 | 0.001 | 0.24 | 0.16 | 0.01 | 0.03 | 0.54 | 0.09 | 0.07 |
| Triglycerides | 0.43 | 0.04 | <0.0001 | 0.002 | 0.002 | <0.0001 | 0.37 | 0.06 | 0.09 | 0.63 | 0.04 | 0.007 |
| Blood glucose | 0.41 | 0.06 | 0.0009 | 0.25 | 0.16 | 0.91 | 0.32 | 0.1 | 0.09 | 0.47 | 0.07 | 0.001 |
| HbA1c | 0.37 | 0.1 | 0.06 | 0.03 | 0.01 | 0.83 | 0.35 | 0.2 | 0.55 | 0.36 | 0.1 | 0.008 |
| LSM | 0.50 | 0.03 | 0.0006 | 0.02 | 0.08 | 0.02 | 0.35 | 0.08 | 0.05 | 0.67 | 0.04 | 0.12 |
| Insulin | 0.60 | 0.03 | 0.10 | 0.31 | 0.06 | 0.06 | 0.53 | 0.05 | 0.20 | 0.67 | 0.04 | 0.12 |
| Oral Antidiabetics | 0.52 | 0.04 | 0.14 | 0.11 | 0.01 | 0.19 | 0.41 | 0.09 | 0.26 | 0.67 | 0.05 | 0.73 |
| T2DM duration | 0.67 | 0.03 | 0.10 | 0.22 | 0.09 | 0.94 | 0.56 | 0.08 | 0.65 | 0.1 | 0.02 | 0.54 |
| Variable | Overall | Normal Weight | Overweight | Obesity | ||||
|---|---|---|---|---|---|---|---|---|
| OR 95% CI | p-Value | OR 95% CI | p-Value | OR 95% CI | p-Value | OR 95% CI | p-Value | |
| Female gender | 0.89(0.75–0.95) | 0.85 | 0.59 (0.45–0.78) | 0.78 | – | – | – | – |
| BMI | 0.99 (0.92–1.07) | 0.97 | 0.89 (0.46–1.79) | 0.76 | – | – | 1.02 (0.94–1.11) | 0.14 |
| Waist circumference | 1.07 (1.03–1.11) | 0.05 | 1.13 (0.97–1.32) | 0.10 | 1.07 (1.005–1.14) | 0.08 | 1.05 (0.98–1.08) | 0.002 |
| AST | 1.01 (0.99–1.02) | 0.11 | – | – | – | – | 0.99 (0.98–1) | 0.10 |
| Total cholesterol | 1 (0.99–1.009) | 0.70 | – | – | 1 (0.99–1.01) | 0.17 | – | – |
| Triglycerides | 1 (1.002–1.009) | 0.07 | 1.02 (1–1.14) | 0.94 | – | – | 1.01 (0.97–1.04) | 0.31 |
| Blood glucose | 1 (0.99–1.006) | 0.22 | – | – | – | – | 1 (0.99–1) | 0.32 |
| HbA1c | – | – | – | – | – | – | 1 (0.99–1.02) | 0.27 |
| LSM | 1.08 (1.03–1.13) | 0.58 | 1 (0.98–1.25) | 0.68 | – | – | – | – |
| Variable | Overall | Normal Weight | Overweight | Obese | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ß | SE | p | ß | SE | p | ß | SE | p | ß | SE | p | |
| Age | 0.16 | 0.1 | 0.75 | 0.20 | 0.3 | 0.85 | 0.004 | 0.002 | 0.10 | 0.26 | 0.14 | 0.83 |
| Female gender | 0.20 | 0.01 | 0.45 | -0.24 | 0.08 | 0.006 | 0.18 | 0.01 | 0.32 | 0.05 | 0.04 | 0.21 |
| BMI | 0.01 | 0.002 | <0.0001 | 0.03 | 0.02 | 0.09 | 0.02 | 0.01 | 0.2 | 0.25 | 0.02 | <0.0001 |
| Waist circumference | 0.0006 | 0.001 | 0.0002 | 0.08 | 0.04 | 0.08 | 0.2 | 0.2 | 0.64 | 0.54 | 0.02 | 0.002 |
| AST | 0.004 | 0.009 | <0.0001 | 0.05 | 0.02 | 0.01 | 0.05 | 0.01 | 0.0002 | 0.16 | 0.03 | 0.01 |
| ALT | 0.24 | 0.02 | 0.43 | 0.002 | 0.01 | 0.09 | 0.01 | 0.01 | 0.23 | 0.23 | 0.02 | 0.57 |
| Total cholesterol | 0.17 | 0.06 | 0.76 | 0.26 | 0.18 | 0.5 | 0.13 | 0.08 | 0.95 | 0.19 | 0.09 | 0.68 |
| Triglycerides | 0.0004 | 0.04 | 0.53 | 0.01 | 0.08 | 0.07 | 0.14 | 0.03 | 0.85 | 0.25 | 0.03 | 0.49 |
| Blood glucose | 0.31 | 0.06 | 0.13 | 0.24 | 0.12 | 0.30 | 0.14 | 0.07 | 0.91 | 0.19 | 0.07 | 0.49 |
| HbA1c | 0.02 | 0.01 | 0.04 | 0.39 | 0.2 | 0.21 | 0.01 | 0.01 | 0.3 | 0.03 | 0.01 | 0.02 |
| CAP | 0.001 | 0.002 | 0.0002 | 0.001 | 0.07 | 0.01 | 0.1 | 0.1 | 0.1 | 0.03 | 0.1 | 0.17 |
| Severe steatosis | 0.11 | 0.03 | 0.0007 | 0.52 | 0.34 | 0.13 | 0.35 | 0.5 | 0.47 | 0.58 | 0.1 | 0.03 |
| Insulin | 0.01 | 0.02 | 0.55 | 0.2 | 0.01 | 0.15 | 0.1 | 0.02 | 0.57 | 0.2 | 0.05 | 0.45 |
| Oral Antidiabetics | 0.15 | 0.02 | 0.28 | 0.2 | 0.02 | 0.8 | 0.05 | 0.01 | 0.47 | 0.84 | 0.01 | 0.89 |
| T2DM duration | 0.22 | 0.02 | 0.34 | 0.4 | 0.04 | 0.58 | 0.06 | 0.01 | 0.51 | 0.75 | 0.01 | 0.74 |
| Variable | Overall | Normal Weight | Overweight | Obese | ||||
|---|---|---|---|---|---|---|---|---|
| OR 95% CI | p-Value | OR 95% CI | p-Value | OR 95% CI | p-Value | OR 95% CI | p-Value | |
| Female gender | – | – | 0.19(0.07-5.21) | 0.32 | – | – | – | – |
| BMI | 1.05 (0.97–1.14) | 0.20 | – | – | – | – | 1.1 (0.94–1.3) | 0.09 |
| Waist circ. | 1.01 (0.97–1.04) | 0.59 | – | – | – | – | 1 (0.98–1.03) | 0.8 |
| AST | 1.02 (1–1.04) | 0.001 | 1.03 (1–1.6) | 0.02 | 1.03 (1.01–1.05) | 0.003 | 1.04 (0.99–1.2) | 0.01 |
| HbA1c | 1.1 (0.94–1.3) | 0.21 | – | – | – | – | 1.01 (0.97–1.08) | 0.17 |
| CAP | 1 (0.99–1.01) | 0.41 | 1.01 (0.98–1.03) | 0.40 | – | – | – | – |
| Severe steatosis | 2.5 (1.5–3.1) | 0.09 | – | – | – | – | 5 (1.5–31.4) | <0.0001 |
| F ≤ 2 (n = 430) | ≥F3 (n = 104) | p-Value | |
|---|---|---|---|
| LSM (kPa) | 5.82 ± 1.60 | 12.48 ± 7.9 | <0.0001 |
| APRI | 0.29 ± 0.17 | 0.44 ± 0.3 | <0.0001 |
| FIB-4 | 1 ± 0.15 | 1.39 ± 1 | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sporea, I.; Mare, R.; Popescu, A.; Nistorescu, S.; Baldea, V.; Sirli, R.; Braha, A.; Sima, A.; Timar, R.; Lupusoru, R. Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience. J. Clin. Med. 2020, 9, 1032. https://doi.org/10.3390/jcm9041032
Sporea I, Mare R, Popescu A, Nistorescu S, Baldea V, Sirli R, Braha A, Sima A, Timar R, Lupusoru R. Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience. Journal of Clinical Medicine. 2020; 9(4):1032. https://doi.org/10.3390/jcm9041032
Chicago/Turabian StyleSporea, Ioan, Ruxandra Mare, Alina Popescu, Silviu Nistorescu, Victor Baldea, Roxana Sirli, Adina Braha, Alexandra Sima, Romulus Timar, and Raluca Lupusoru. 2020. "Screening for Liver Fibrosis and Steatosis in a Large Cohort of Patients with Type 2 Diabetes Using Vibration Controlled Transient Elastography and Controlled Attenuation Parameter in a Single-Center Real-Life Experience" Journal of Clinical Medicine 9, no. 4: 1032. https://doi.org/10.3390/jcm9041032