Targeting Metabolic Consequences of Insulin Resistance in Polycystic Ovary Syndrome by D-chiro-inositol and Emerging Nutraceuticals: A Focused Review

 , ,
, ,
Abstract
:1. Introduction
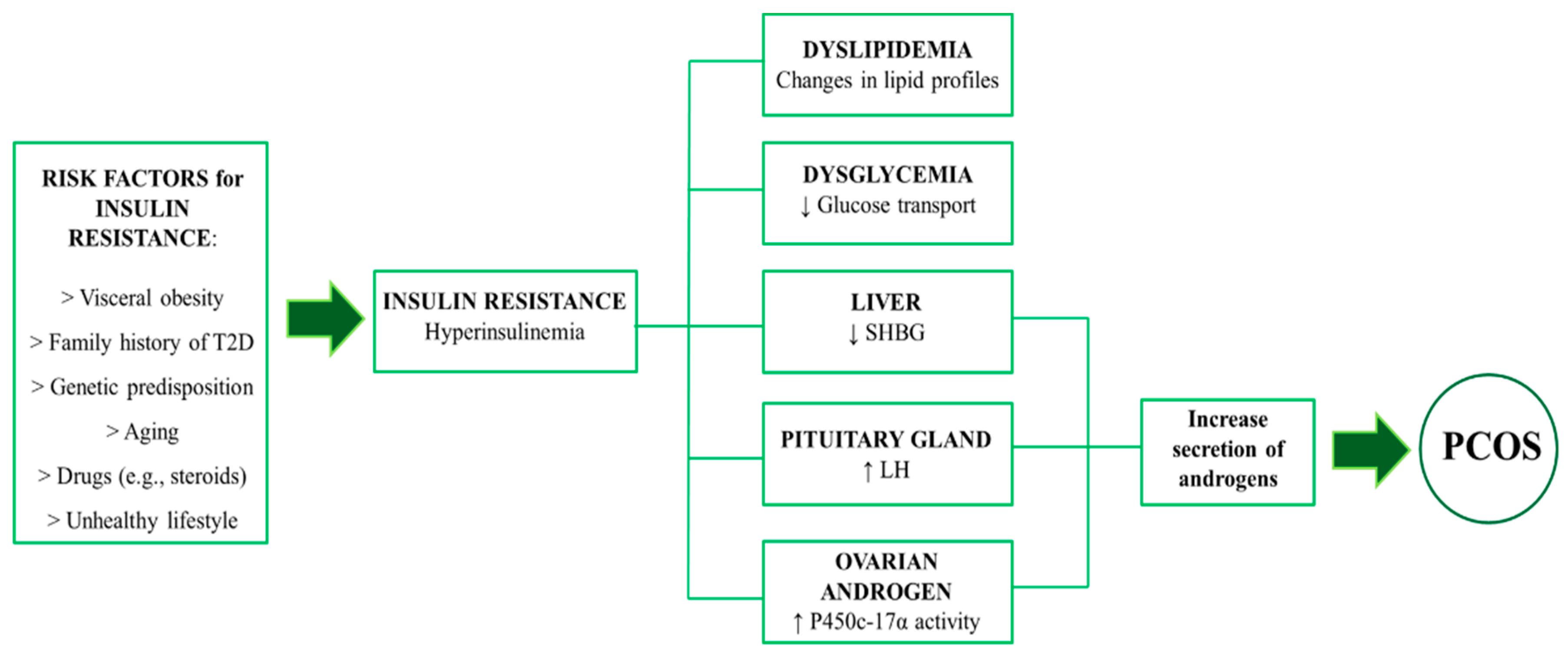
2. Metabolic Consequences of InsR in PCOS
3. The Relevance of D-chiro-inositol and other Nutraceuticals in Insulin Signaling and InsR: Preclinical Evidence
3.1. D-Chiro-Inositol
3.2. Flaxseed Lignans
3.3. Ipomea Batatas
3.4. Lagerstroemia Speciosa (banaba)
4. Clinical Potential for improving InsR in PCOS
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ding, T.; Hardiman, P.J.; Petersen, I.; Wang, F.-F.; Qu, F.; Baio, G. The prevalence of polycystic ovary syndrome in reproductive-aged women of different ethnicity: A systematic review and meta-analysis. Oncotarget 2017, 8, 96351–96358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Dumesic, D.A.; Oberfield, S.E.; Stener-Victorin, E.; Marshall, J.C.; Laven, J.S.; Legro, R.S. Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr. Rev. 2015, 36, 487–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azziz, R.; Carmina, E.; Chen, Z.; Dunaif, A.; Laven, J.S.E.; Legro, R.S.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J.; Yildiz, B.O. Polycystic ovary syndrome. Nat. Rev. Dis. Primer 2016, 2, 16057. [Google Scholar] [CrossRef] [PubMed]
- Macut, D.; Bjekić-Macut, J.; Rahelić, D.; Doknić, M. Insulin and the polycystic ovary syndrome. Diabetes Res. Clin. Pract. 2017, 130, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.; Feng, H.L. Extra- and intra-ovarian factors in polycystic ovary syndrome: Impact on oocyte maturation and embryo developmental competence. Hum. Reprod. Update 2011, 17, 17–33. [Google Scholar] [CrossRef]
- Farshchi, H.; Rane, A.; Love, A.; Kennedy, R.L. Diet and nutrition in polycystic ovary syndrome (PCOS): Pointers for nutritional management. J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol. 2007, 27, 762–773. [Google Scholar] [CrossRef]
- Chiofalo, B.; Laganà, A.S.; Palmara, V.; Granese, R.; Corrado, G.; Mancini, E.; Vitale, S.G.; Ban Frangež, H.; Vrtačnik-Bokal, E.; Triolo, O. Fasting as possible complementary approach for polycystic ovary syndrome: Hope or hype? Med. Hypotheses 2017, 105, 1–3. [Google Scholar] [CrossRef]
- Marsh, K.A.; Steinbeck, K.S.; Atkinson, F.S.; Petocz, P.; Brand-Miller, J.C. Effect of a low glycemic index compared with a conventional healthy diet on polycystic ovary syndrome. Am. J. Clin. Nutr. 2010, 92, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Jamilian, M.; Asemi, Z. The Effects of Soy Isoflavones on Metabolic Status of Patients With Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2016, 101, 3386–3394. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; Shen, H.; Wu, Q.F.; Tian, L.; Hu, M.H. Treatment of polycystic ovarian syndrome with insulin resistance by insulin-sensitizer. Clin. Exp. Obstet. Gynecol. 2014, 41, 288–292. [Google Scholar] [PubMed]
- Pasquali, R.; Gambineri, A. Insulin sensitizers in polycystic ovary syndrome. Front. Horm. Res. 2013, 40, 83–102. [Google Scholar] [PubMed]
- Laganà, A.S.; Barbaro, L.; Pizzo, A. Evaluation of ovarian function and metabolic factors in women affected by polycystic ovary syndrome after treatment with D-Chiro-Inositol. Arch. Gynecol. Obstet. 2015, 291, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Samuel, V.T.; Shulman, G.I. Mechanisms for insulin resistance: Common threads and missing links. Cell 2012, 148, 852–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawson, M.A.; Jain, S.; Sun, S.; Patel, K.; Malcolm, P.J.; Chang, R.J. Evidence for insulin suppression of baseline luteinizing hormone in women with polycystic ovarian syndrome and normal women. J. Clin. Endocrinol. Metab. 2008, 93, 2089–2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti-Kandarakis, E.; Papavassiliou, A.G. Molecular mechanisms of insulin resistance in polycystic ovary syndrome. Trends Mol. Med. 2006, 12, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Xie, X.; Jia, Y.; Li, S. Associations of insulin receptor and insulin receptor substrates genetic polymorphisms with polycystic ovary syndrome: A systematic review and meta-analysis. J. Obstet. Gynaecol. Res. 2016, 42, 844–854. [Google Scholar] [CrossRef]
- Mioni, R.; Chiarelli, S.; Xamin, N.; Zuliani, L.; Granzotto, M.; Mozzanega, B.; Maffei, P.; Martini, C.; Blandamura, S.; Sicolo, N.; et al. Evidence for the presence of glucose transporter 4 in the endometrium and its regulation in polycystic ovary syndrome patients. J. Clin. Endocrinol. Metab. 2004, 89, 4089–4096. [Google Scholar] [CrossRef] [Green Version]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- Trent, M.; Austin, S.B.; Rich, M.; Gordon, C.M. Overweight status of adolescent girls with polycystic ovary syndrome: Body mass index as mediator of quality of life. Ambul. Pediatr. Off. J. Ambul. Pediatr. Assoc. 2005, 5, 107–111. [Google Scholar] [CrossRef]
- Tafeit, E.; Möller, R.; Rackl, S.; Giuliani, A.; Urdl, W.; Freytag, U.; Crailsheim, K.; Sudi, K.; Horejsi, R. Subcutaneous adipose tissue pattern in lean and obese women with polycystic ovary syndrome. Exp. Biol. Med. 2003, 228, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Horejsi, R.; Möller, R.; Rackl, S.; Giuliani, A.; Freytag, U.; Crailsheim, K.; Sudi, K.; Tafeit, E. Android subcutaneous adipose tissue topography in lean and obese women suffering from PCOS: Comparison with type 2 diabetic women. Am. J. Phys. Anthropol. 2004, 124, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Goverde, A.J.; van Koert, A.J.B.; Eijkemans, M.J.; Knauff, E.a.H.; Westerveld, H.E.; Fauser, B.C.J.M.; Broekmans, F.J. Indicators for metabolic disturbances in anovulatory women with polycystic ovary syndrome diagnosed according to the Rotterdam consensus criteria. Hum. Reprod. Oxf. Engl. 2009, 24, 710–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legro, R.S.; Kunselman, A.R.; Dodson, W.C.; Dunaif, A. Prevalence and predictors of risk for type 2 diabetes mellitus and impaired glucose tolerance in polycystic ovary syndrome: A prospective, controlled study in 254 affected women. J. Clin. Endocrinol. Metab. 1999, 84, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Misso, M.L.; Wild, R.A.; Norman, R.J. Impaired glucose tolerance, type 2 diabetes and metabolic syndrome in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2010, 16, 347–363. [Google Scholar] [CrossRef]
- Lim, S.S.; Davies, M.J.; Norman, R.J.; Moran, L.J. Overweight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Alvero, R. Racial and ethnic differences in physiology and clinical symptoms of polycystic ovary syndrome. Semin. Reprod. Med. 2013, 31, 365–369. [Google Scholar] [CrossRef] [Green Version]
- Legro, R.S.; Kunselman, A.R.; Dunaif, A. Prevalence and predictors of dyslipidemia in women with polycystic ovary syndrome. Am. J. Med. 2001, 111, 607–613. [Google Scholar] [CrossRef]
- Wild, R.A.; Rizzo, M.; Clifton, S.; Carmina, E. Lipid levels in polycystic ovary syndrome: Systematic review and meta-analysis. Fertil. Steril. 2011, 95, 1073–1079.e11. [Google Scholar] [CrossRef]
- Shi, Y.; Cui, Y.; Sun, X.; Ma, G.; Ma, Z.; Gao, Q.; Chen, Z.-J. Hypertension in women with polycystic ovary syndrome: Prevalence and associated cardiovascular risk factors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 173, 66–70. [Google Scholar] [CrossRef]
- Elting, M.W.; Korsen, T.J.; Bezemer, P.D.; Schoemaker, J. Prevalence of diabetes mellitus, hypertension and cardiac complaints in a follow-up study of a Dutch PCOS population. Hum. Reprod. Oxf. Engl. 2001, 16, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, A.; Dragotto, J.; Giuliani, A.; Bizzarri, M. Myo-inositol and D-chiro-inositol (40:1) reverse histological and functional features of polycystic ovary syndrome in a mouse model. J. Cell. Physiol. 2019, 234, 9387–9398. [Google Scholar] [CrossRef]
- Li, X.; Cui, P.; Jiang, H.-Y.; Guo, Y.-R.; Pishdari, B.; Hu, M.; Feng, Y.; Billig, H.; Shao, R. Reversing the reduced level of endometrial GLUT4 expression in polycystic ovary syndrome: A mechanistic study of metformin action. Am. J. Transl. Res. 2015, 7, 574–586. [Google Scholar] [PubMed]
- La Marca, A.; Grisendi, V.; Dondi, G.; Sighinolfi, G.; Cianci, A. The menstrual cycle regularization following D-chiro-inositol treatment in PCOS women: A retrospective study. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2015, 31, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Pundir, J.; Psaroudakis, D.; Savnur, P.; Bhide, P.; Sabatini, L.; Teede, H.; Coomarasamy, A.; Thangaratinam, S. Inositol treatment of anovulation in women with polycystic ovary syndrome: A meta-analysis of randomised trials. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 299–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bevilacqua, A.; Bizzarri, M. Inositols in Insulin Signaling and Glucose Metabolism. Int. J. Endocrinol. 2018, 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asplin, I.; Galasko, G.; Larner, J. chiro-inositol deficiency and insulin resistance: a comparison of the chiro-inositol- and the myo-inositol-containing insulin mediators isolated from urine, hemodialysate, and muscle of control and type II diabetic subjects. Proc. Natl. Acad. Sci. USA 1993, 90, 5924–5928. [Google Scholar] [CrossRef] [Green Version]
- Fonteles, M.C.; Almeida, M.Q.; Larner, J. Antihyperglycemic effects of 3-O-methyl-D-chiro-inositol and D-chiro-inositol associated with manganese in streptozotocin diabetic rats. Horm. Metab. Res. Horm. Stoffwechselforschung Horm. Metab. 2000, 32, 129–132. [Google Scholar] [CrossRef]
- Gao, Y.-F.; Zhang, M.-N.; Wang, T.-X.; Wu, T.-C.; Ai, R.-D.; Zhang, Z.-S. Hypoglycemic effect of D-chiro-inositol in type 2 diabetes mellitus rats through the PI3K/Akt signaling pathway. Mol. Cell. Endocrinol. 2016, 433, 26–34. [Google Scholar] [CrossRef]
- Larner, J.; Huang, L.C.; Schwartz, C.F.; Oswald, A.S.; Shen, T.Y.; Kinter, M.; Tang, G.Z.; Zeller, K. Rat liver insulin mediator which stimulates pyruvate dehydrogenase phosphate contains galactosamine and D-chiroinositol. Biochem. Biophys. Res. Commun. 1988, 151, 1416–1426. [Google Scholar] [CrossRef]
- Ortmeyer, H.K.; Bodkin, N.L.; Hansen, B.C.; Larner, J. In vivo D-chiroinositol activates skeletal muscle glycogen synthase and inactivates glycogen phosphorylase in rhesus monkeys. J. Nutr. Biochem. 1995, 6, 499–503. [Google Scholar] [CrossRef]
- Genazzani, A.D. Inositol as putative integrative treatment for PCOS. Reprod. Biomed. Online 2016, 33, 770–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, M.; Maddaford, T.G.; Austria, J.A.; Aliani, M.; Netticadan, T.; Pierce, G.N. Dietary Flaxseed as a Strategy for Improving Human Health. Nutrients 2019, 11, 1171. [Google Scholar] [CrossRef] [Green Version]
- Prasad, K. Secoisolariciresinol diglucoside from flaxseed delays the development of type 2 diabetes in Zucker rat. J. Lab. Clin. Med. 2001, 138, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Kinniry, P.; Amrani, Y.; Vachani, A.; Solomides, C.C.; Arguiri, E.; Workman, A.; Carter, J.; Christofidou-Solomidou, M. Dietary flaxseed supplementation ameliorates inflammation and oxidative tissue damage in experimental models of acute lung injury in mice. J. Nutr. 2006, 136, 1545–1551. [Google Scholar] [CrossRef] [PubMed]
- MacDonald-Wicks, L.K.; Garg, M.L. Modulation of carbon tetrachloride-induced oxidative stress by dietary fat in rats(open star). J. Nutr. Biochem. 2002, 13, 87–95. [Google Scholar] [CrossRef]
- Fukumitsu, S.; Aida, K.; Ueno, N.; Ozawa, S.; Takahashi, Y.; Kobori, M. Flaxseed lignan attenuates high-fat diet-induced fat accumulation and induces adiponectin expression in mice. Br. J. Nutr. 2008, 100, 669–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Fofana, B.; Roy, M.; Ghose, K.; Yao, X.-H.; Nixon, M.-S.; Nair, S.; Nyomba, G.B.L. Flaxseed lignan secoisolariciresinol diglucoside improves insulin sensitivity through upregulation of GLUT4 expression in diet-induced obese mice. J. Funct. Foods 2015, 18, 1–9. [Google Scholar] [CrossRef]
- Sun, J.; Tang, Y.; Yu, X.; Xu, Y.; Liu, P.; Xiao, L.; Liu, L.; Deng, Q.; Yao, P. Flaxseed lignans alleviate high fat diet-induced hepatic steatosis and insulin resistance in mice: Potential involvement of AMP-activated protein kinase. J. Funct. Foods 2016, 24, 482–491. [Google Scholar] [CrossRef]
- Abel, C.; Busia, K. An exploratory ethnobotanical study of the practice of herbal medicine by the Akan peoples of Ghana. Altern. Med. Rev. J. Clin. Ther. 2005, 10, 112–122. [Google Scholar]
- Pochapski, M.T.; Fosquiera, E.C.; Esmerino, L.A.; Dos Santos, E.B.; Farago, P.V.; Santos, F.A.; Groppo, F.C. Phytochemical screening, antioxidant, and antimicrobial activities of the crude leaves’ extract from Ipomoea batatas (L.) Lam. Pharmacogn. Mag. 2011, 7, 165–170. [Google Scholar] [PubMed]
- Kusano, S.; Abe, H.; Okada, A. Study of Antidiabetic Activity of White Skinned Sweet Potato (Ipomoea batatas L.). Nippon Nōgeikagaku Kaishi 1998, 72, 1045–1052. [Google Scholar] [CrossRef] [Green Version]
- Kusano, S.; Abe, H. Antidiabetic activity of white skinned sweet potato (Ipomoea batatas L.) in obese Zucker fatty rats. Biol. Pharm. Bull. 2000, 23, 23–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, R.; Li, Q.; Long, L.; Li, J.; Yang, R.; Gao, D. Antidiabetic activity of flavone from Ipomoea Batatas leaf in non-insulin dependent diabetic rats. Int. J. Food Sci. Technol. 2006, 42, 80–85. [Google Scholar] [CrossRef]
- Nagamine, R.; Ueno, S.; Tsubata, M.; Yamaguchi, K.; Takagaki, K.; Hira, T.; Hara, H.; Tsuda, T. Dietary sweet potato (Ipomoea batatas L.) leaf extract attenuates hyperglycaemia by enhancing the secretion of glucagon-like peptide-1 (GLP-1). Food Funct. 2014, 5, 2309–2316. [Google Scholar] [CrossRef]
- Garcia, F. On the hypoglycemic effect of decoction of Lagerstroemia speciosa leaves (banaba) administered orally. J. Philipp. Isl. Med. Assoc. 1940, 20, 395–402. [Google Scholar]
- Stohs, S.J.; Miller, H.; Kaats, G.R. A review of the efficacy and safety of banaba (Lagerstroemia speciosa L.) and corosolic acid. Phytother Res. 2012, 26, 317–324. [Google Scholar] [CrossRef]
- Park, M.-Y.; Lee, K.-S.; Sung, M.-K. Effects of dietary mulberry, Korean red ginseng, and banaba on glucose homeostasis in relation to PPAR-alpha, PPAR-gamma, and LPL mRNA expressions. Life Sci. 2005, 77, 3344–3354. [Google Scholar] [CrossRef]
- Hayashi, T.; Maruyama, H.; Kasai, R.; Hattori, K.; Takasuga, S.; Hazeki, O.; Yamasaki, K.; Tanaka, T. Ellagitannins from Lagerstroemia speciosa as activators of glucose transport in fat cells. Planta Med. 2002, 68, 173–175. [Google Scholar] [CrossRef]
- Miura, T.; Itoh, Y.; Kaneko, T.; Ueda, N.; Ishida, T.; Fukushima, M.; Matsuyama, F.; Seino, Y. Corosolic acid induces GLUT4 translocation in genetically type 2 diabetic mice. Biol. Pharm. Bull. 2004, 27, 1103–1105. [Google Scholar] [CrossRef] [Green Version]
- Miura, T.; Ueda, N.; Yamada, K.; Fukushima, M.; Ishida, T.; Kaneko, T.; Matsuyama, F.; Seino, Y. Antidiabetic effects of corosolic acid in KK-Ay diabetic mice. Biol. Pharm. Bull. 2006, 29, 585–587. [Google Scholar] [CrossRef] [Green Version]
- Shim, K.S.; Lee, S.-U.; Ryu, S.Y.; Min, Y.K.; Kim, S.H. Corosolic acid stimulates osteoblast differentiation by activating transcription factors and MAP kinases. Phytother. Res. 2009, 23, 1754–1758. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-Q.; Tian, W.; Liu, X.-X.; Zhang, K.; Huo, J.-C.; Liu, W.-J.; Li, P.; Xiao, X.; Zhao, M.-G.; Cao, W. Corosolic acid inhibits the proliferation of glomerular mesangial cells and protects against diabetic renal damage. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheang, K.I.; Baillargeon, J.-P.; Essah, P.A.; Ostlund, R.E.; Apridonize, T.; Islam, L.; Nestler, J.E. Insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator correlates with insulin sensitivity in women with polycystic ovary syndrome. Metabolism 2008, 57, 1390–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nestler, J.E.; Jakubowicz, D.J.; Reamer, P.; Gunn, R.D.; Allan, G. Ovulatory and metabolic effects of D-chiro-inositol in the polycystic ovary syndrome. N. Engl. J. Med. 1999, 340, 1314–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genazzani, A.D.; Santagni, S.; Rattighieri, E.; Chierchia, E.; Despini, G.; Marini, G.; Prati, A.; Simoncini, T. Modulatory role of D-chiro-inositol (DCI) on LH and insulin secretion in obese PCOS patients. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2014, 30, 438–443. [Google Scholar] [CrossRef] [PubMed]
- González, F.; Rote, N.S.; Minium, J.; Kirwan, J.P. Reactive oxygen species-induced oxidative stress in the development of insulin resistance and hyperandrogenism in polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 336–340. [Google Scholar] [CrossRef] [Green Version]
- De Leo, V.; La Marca, A.; Cappelli, V.; Stendardi, A.; Focarelli, R.; Musacchio, M.C.; Piomboni, P. Evaluation of the treatment with D-chiro-inositol on levels of oxidative stress in PCOS patients. Minerva Ginecol. 2012, 64, 531–538. [Google Scholar]
- Haidari, F.; Banaei-Jahromi, N.; Zakerkish, M.; Ahmadi, K. The effects of flaxseed supplementation on metabolic status in women with polycystic ovary syndrome: A randomized open-labeled controlled clinical trial. Nutr. J. 2020, 19, 8. [Google Scholar] [CrossRef]
- Pan, A.; Yu, D.; Demark-Wahnefried, W.; Franco, O.H.; Lin, X. Meta-analysis of the effects of flaxseed interventions on blood lipids. Am. J. Clin. Nutr. 2009, 90, 288–297. [Google Scholar] [CrossRef] [Green Version]
- Mohammadi-Sartang, M.; Sohrabi, Z.; Barati-Boldaji, R.; Raeisi-Dehkordi, H.; Mazloom, Z. Flaxseed supplementation on glucose control and insulin sensitivity: A systematic review and meta-analysis of 25 randomized, placebo-controlled trials. Nutr. Rev. 2018, 76, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Ludvik, B.; Hanefeld, M.; Pacini, G. Improved metabolic control by Ipomoea batatas (Caiapo) is associated with increased adiponectin and decreased fibrinogen levels in type 2 diabetic subjects. Diabetes Obes. Metab. 2008, 10, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.-K.; Chen, C.-M.; Hsiao, T.-J.; Liu, C.-W.; Li, S.-C. White Sweet Potato as Meal Replacement for Overweight White-Collar Workers: A Randomized Controlled Trial. Nutrients 2019, 11, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judy, W.V.; Hari, S.P.; Stogsdill, W.W.; Judy, J.S.; Naguib, Y.M.A.; Passwater, R. Antidiabetic activity of a standardized extract (Glucosol) from Lagerstroemia speciosa leaves in Type II diabetics. A dose-dependence study. J. Ethnopharmacol. 2003, 87, 115–117. [Google Scholar] [CrossRef]
- Tsuchibe, S.; Kataumi, S.; Mori, M.; Mori, H. An inhibitory effect on the increase in the postprandial blood glucose by Banaba extract capsule enriched corosolic acid. J. Integr. Study Diet. Habits 2006, 17, 255–259. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, M.; Matsuyama, F.; Ueda, N.; Egawa, K.; Takemoto, J.; Kajimoto, Y.; Yonaha, N.; Miura, T.; Kaneko, T.; Nishi, Y.; et al. Effect of corosolic acid on postchallenge plasma glucose levels. Diabetes Res. Clin. Pract. 2006, 73, 174–177. [Google Scholar] [CrossRef]
- Davinelli, S.; Calabrese, V.; Zella, D.; Scapagnini, G. Epigenetic nutraceutical diets in Alzheimer’s disease. J. Nutr. Health Aging. 2014, 18, 800–805. [Google Scholar] [CrossRef]
- Davinelli, S.; Scapagnini, G. Polyphenols: A Promising Nutritional Approach to Prevent or Reduce the Progression of Prehypertension. High Blood Press. Cardiovasc. Prev. 2016, 23, 197–202. [Google Scholar] [CrossRef]
- Scapagnini, G.; Davinelli, S.; Kaneko, T.; Koverech, G.; Koverech, A.; Calabrese, E.J.; Calabrese, V. Dose response biology of resveratrol in obesity. J. Cell. Commun. Signal. 2014, 8, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Banaszewska, B.; Pawelczyk, L.; Spaczynski, R. Current and future aspects of several adjunctive treatment strategies in polycystic ovary syndrome. Reprod. Biol. 2019, 19, 309–315. [Google Scholar] [CrossRef]
- Trummer, C.; Schwetz, V.; Kollmann, M.; Wölfler, M.; Münzker, J.; Pieber, T.R.; Pilz, S.; Heijboer, A.C.; Obermayer-Pietsch, B. Lerchbaum E2. Effects of vitamin D supplementation on metabolic and endocrine parameters in PCOS: A randomized-controlled trial. Eur. J. Nutr. 2019, 58, 2019–2028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davinelli, S.; Corbi, G.; Zarrelli, A.; Arisi, M.; Calzavara-Pinton, P.; Grassi, D.; De Vivo, I.; Scapagnini, G. Short-term supplementation with flavanol-rich cocoa improves lipid profile, antioxidant status and positively influences the AA/EPA ratio in healthy subjects. J. Nutr. Biochem. 2018, 61, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Genovese, C.; Davinelli, S.; Mangano, K.; Tempera, G.; Nicolosi, D.; Corsello, S.; Vergalito, F.; Tartaglia, E.; Scapagnini, G.; Di Marco, R. Effects of a new combination of plant extracts plus d-mannose for the management of uncomplicated recurrent urinary tract infections. J. Chemother. 2018, 30, 107–114. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Intervention | Study Design | Population | Dosage/Duration | Outcomes | Results |
|---|---|---|---|---|---|---|
| Cheang et al. [64] | DCI supplementation | RCT with placebo | 11 women (18–40 y) with PCOS | 1200 mg twice daily for 6 weeks | Hormones, plasma DCI, DCI-IPG release, insulin sensitivity | Significant relationship between DCI-IPG release and insulin sensitivity |
| Nestler et al. [65] | DCI supplementation | RCT with placebo | 44 obese women (18–40 y) with PCOS | 1200 mg/day for 6 to 8 weeks | Hormones, lipid profiles, BP, plasma insulin | Increase of the action of insulin, improvement of ovulatory function and decrease androgens, BP, and TG |
| Genazzani et al. [66] | DCI supplementation | Intervention trial | 22 obese women (age not reported) with PCOS | 500 mg/day for 12 weeks | Hormones and plasma insulin | Improvement of hormonal pattern, especially LH and FSH, and restores insulin sensitivity |
| De Leo et al. [68]. | DCI supplementation | Intervention trial | 20 women (age not reported) with PCOS | 500 mg twice daily for12 weeks | Oxidative stress on follicular fluids | Reduction of the oxidation of thiol groups |
| Haidari et al. [69] | Flaxseed powder supplementation | Open label RCT | 41 patients (18–45 y) with PCOS | 30 g/day for 12 weeks | Anthropometric and biochemical parameters | Reduction in body weight, HOMA-IR, TG, hs-CRP and leptin, and increase in QUIKI, and HDL |
| Pan et al. [70] | Supplementation with flaxseed and its derivatives | Meta-analysis of 28 RCTs | 1539 subjects (age not reported) with HC, T2D, or healthy | Median dose 38 g; median duration 8.5 weeks | Blood lipid concentrations | Reduction in total and LDL-cholesterol |
| Mohammadi-Sartang et al. [71] | Supplementation with whole flaxseed, flaxseed oil, and lignan extract | Meta-analysis of 25 RCTs | 2080 subjects (mean age from 29.4 to 67.6 y) with PCOS, HC, T2D, CVD, MetS, obesity, or healthy | Whole flaxseed from 10–60 g ALA from 1 to 15 g; Lignans from 21 to 600 mg Duration from 2 to 48 weeks | Glucose control and insulin sensitivity | Reduction in blood glucose, insulin levels, and increase in QUIKI |
| Ludvik et al. [72] | Supplementation with sweet potato | RCT with Placebo | 61 patients (mean age 57.2 y) with T2D | 4 g/day for 20 weeks | Insulin sensitivity, T2D parameters, lipids, adiponectin, hs-CRP, and fibrinogen | Improvement in HbA1c, TG, adiponectin, fibrinogen, and insulin sensitivity |
| Shih et al. [73] | Supplementation with sweet potato | RCT with no placebo | 56 overweight (mean age 38.7 y) participants | 132 g/day for 8 weeks | Anthropometric and biochemical parameters | Improvement in HbA1c, and reduction in BMI |
| Judy et al. [74] | Supplementation with an extract from banaba | RCT with no placebo | 10 subjects (55–70 y) With T2D | 16, 32 and 48 mg/day for 2 weeks | Blood glucose levels | Reduction in blood glucose levels |
| Tsuchibe et al. [75] | Supplementation with corosolic acid extracted from banaba | RCT with no placebo | 12 healthy subjects (mean age 57.7 y) | 10 mg/day for 2 weeks | Postprandial blood glucose and anthropometric parameters | Inhibitory effect on postprandial blood glucose. Reduction in BMI. |
| Fukushima et al. [76] | Supplementation with corosolic acid extracted from banaba | double-blind and cross-over RCT | 31 subjects (mean age 51.6 y) with T2D and impaired glucose tolerance | 10 mg; different time points | Fasting plasma glucose | Lowering effect on post-challenge plasma glucose levels |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davinelli, S.; Nicolosi, D.; Di Cesare, C.; Scapagnini, G.; Di Marco, R. Targeting Metabolic Consequences of Insulin Resistance in Polycystic Ovary Syndrome by D-chiro-inositol and Emerging Nutraceuticals: A Focused Review. J. Clin. Med. 2020, 9, 987. https://doi.org/10.3390/jcm9040987
Davinelli S, Nicolosi D, Di Cesare C, Scapagnini G, Di Marco R. Targeting Metabolic Consequences of Insulin Resistance in Polycystic Ovary Syndrome by D-chiro-inositol and Emerging Nutraceuticals: A Focused Review. Journal of Clinical Medicine. 2020; 9(4):987. https://doi.org/10.3390/jcm9040987
Chicago/Turabian StyleDavinelli, Sergio, Daria Nicolosi, Cinzia Di Cesare, Giovanni Scapagnini, and Roberto Di Marco. 2020. "Targeting Metabolic Consequences of Insulin Resistance in Polycystic Ovary Syndrome by D-chiro-inositol and Emerging Nutraceuticals: A Focused Review" Journal of Clinical Medicine 9, no. 4: 987. https://doi.org/10.3390/jcm9040987