Pallidal Deep Brain Stimulation in DYT6 Dystonia: Clinical Outcome and Predictive Factors for Motor Improvement

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Material and Method
3. Results
3.1. Baseline Characteristics
3.2. Timing of Surgery and Follow-Up
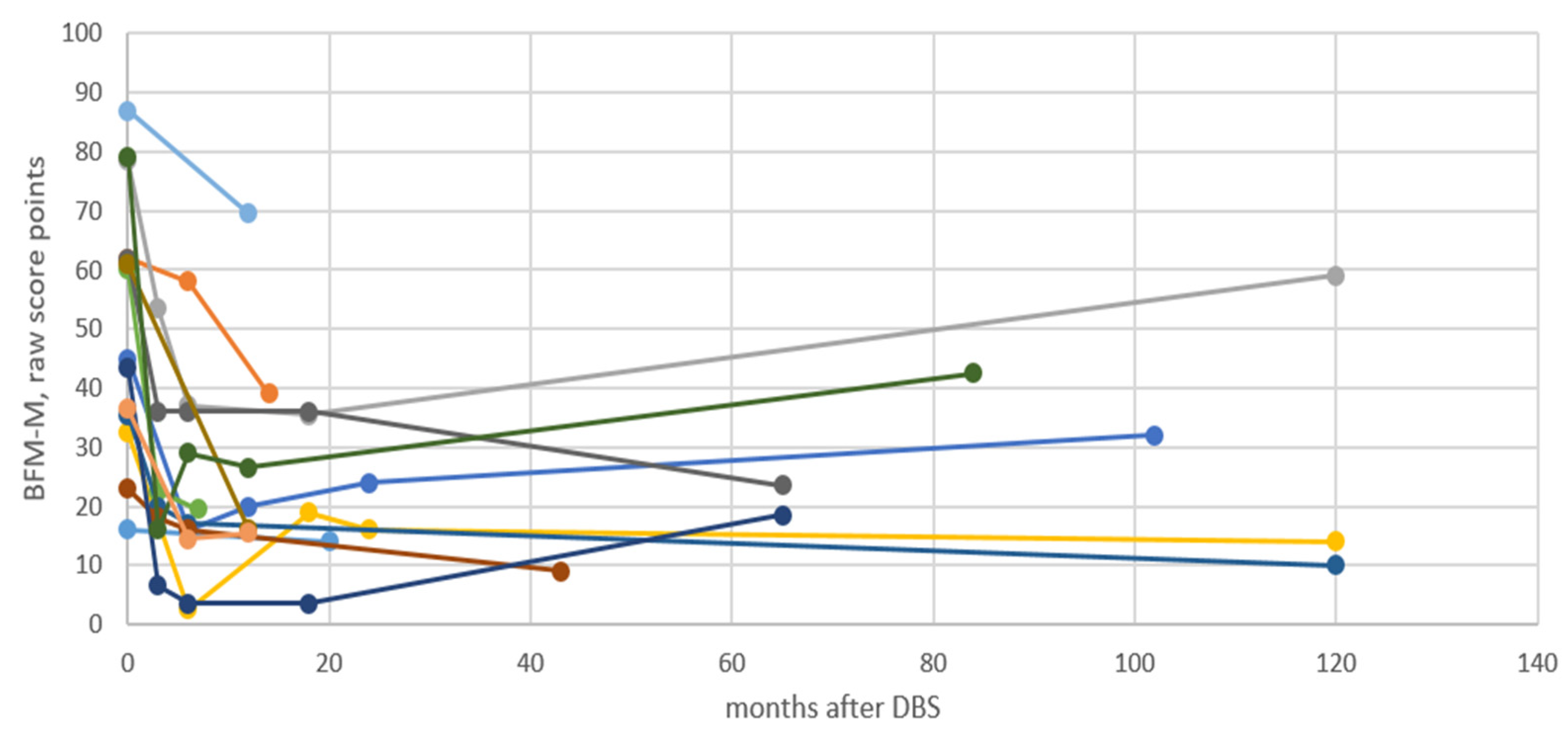
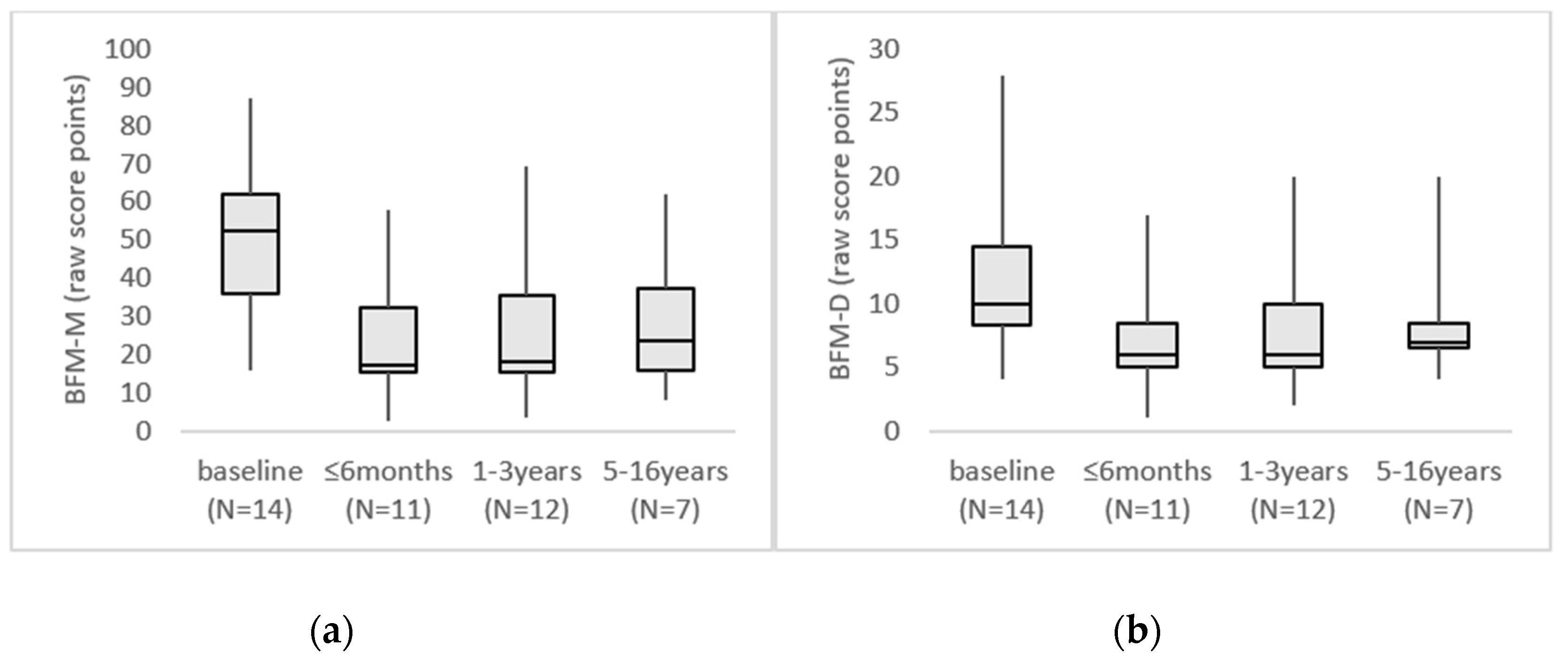
3.3. Clinical Outcome
3.4. Correlation Timing of Surgery and Clinical Outcome
3.5. Complications and Side Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Albanese, A.; Bhatia, K.; Bressman, S.B.; Delong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: a consensus update. Mov. Disord. Off. J. Mov. Disord. Soc. 2013, 28, 863–873. [Google Scholar] [CrossRef] [Green Version]
- Ozelius, L.J.; Hewett, J.W.; Page, C.E.; Bressman, S.B.; Kramer, P.L.; Shalish, C.; de Leon, D.; Brin, M.F.; Raymond, D.; Corey, D.P.; et al. The early-onset torsion dystonia gene (DYT1) encodes an ATP-binding protein. Nat. Genet. 1997, 17, 40–48. [Google Scholar] [CrossRef]
- Lohmann, K.; Klein, C. Update on the Genetics of Dystonia. Curr. Neurol. Neurosci. Rep. 2017, 17, 26. [Google Scholar] [CrossRef]
- Page, D.; Butler, A.; Jahanshahi, M. Quality of life in focal, segmental, and generalized dystonia. Mov. Disord. Off. J. Mov. Disord. Soc. 2007, 22, 341–347. [Google Scholar] [CrossRef]
- Lin, J.P.; Lumsden, D.E.; Gimeno, H.; Kaminska, M. The impact and prognosis for dystonia in childhood including dystonic cerebral palsy: A clinical and demographic tertiary cohort study. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1239–1244. [Google Scholar] [CrossRef]
- Roubertie, A.; Mariani, L.L.; Fernandez-Alvarez, E.; Doummar, D.; Roze, E. Treatment for dystonia in childhood. Eur. J. Neurol. 2012, 19, 1292–1299. [Google Scholar] [CrossRef]
- Termsarasab, P.; Thammongkolchai, T.; Frucht, S.J. Medical treatment of dystonia. J. Clin. Mov. Disord. 2016, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A.; Lozano, A.M. Deep brain stimulation for movement disorders: 2015 and beyond. Curr. Opin. Neurol. 2015, 28, 423–436. [Google Scholar] [CrossRef]
- Holloway, K.L.; Baron, M.S.; Brown, R.; Cifu, D.X.; Carne, W.; Ramakrishnan, V. Deep brain stimulation for dystonia: a meta-analysis. Neuromodulation J. Int. Neuromodulation Soc. 2006, 9, 253–261. [Google Scholar] [CrossRef]
- Kupsch, A.; Benecke, R.; Muller, J.; Trottenberg, T.; Schneider, G.H.; Poewe, W.; Eisner, W.; Wolters, A.; Muller, J.U.; Deuschl, G.; et al. Pallidal deep-brain stimulation in primary generalized or segmental dystonia. N. Engl. J. Med. 2006, 355, 1978–1990. [Google Scholar] [CrossRef] [Green Version]
- Vidailhet, M.; Vercueil, L.; Houeto, J.L.; Krystkowiak, P.; Lagrange, C.; Yelnik, J.; Bardinet, E.; Benabid, A.L.; Navarro, S.; Dormont, D.; et al. Bilateral, pallidal, deep-brain stimulation in primary generalised dystonia: A prospective 3 year follow-up study. Lancet Neurol. 2007, 6, 223–229. [Google Scholar] [CrossRef]
- Moro, E.; LeReun, C.; Krauss, J.K.; Albanese, A.; Lin, J.P.; Walleser Autiero, S.; Brionne, T.C.; Vidailhet, M. Efficacy of pallidal stimulation in isolated dystonia: a systematic review and meta-analysis. Eur. J. Neurol. 2017, 24, 552–560. [Google Scholar] [CrossRef]
- Cif, L.; Coubes, P. Historical developments in children’s deep brain stimulation. Eur. J. Paediatr. Neurol. 2017, 21, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Reese, R.; Volkmann, J. Deep Brain Stimulation for the Dystonias: Evidence, Knowledge Gaps, and Practical Considerations. Mov. Disord. Clin. Pract. 2017, 4, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Fox, M.D.; Alterman, R.L. Brain Stimulation for Torsion Dystonia. JAMA Neurol. 2015, 72, 713–719. [Google Scholar] [CrossRef] [Green Version]
- Andrews, C.; Aviles-Olmos, I.; Hariz, M.; Foltynie, T. Which patients with dystonia benefit from deep brain stimulation? A metaregression of individual patient outcomes. J. Neurol. Neurosurg. Psychiatry 2010, 81, 1383–1389. [Google Scholar] [CrossRef] [Green Version]
- Elkaim, L.M.; Alotaibi, N.M.; Sigal, A.; Alotaibi, H.M.; Lipsman, N.; Kalia, S.K.; Fehlings, D.L.; Lozano, A.M.; Ibrahim, G.M. Deep brain stimulation for pediatric dystonia: a meta-analysis with individual participant data. Dev. Med. Child Neurol. 2019, 61, 49–56. [Google Scholar] [CrossRef]
- Bruggemann, N.; Kuhn, A.; Schneider, S.A.; Kamm, C.; Wolters, A.; Krause, P.; Moro, E.; Steigerwald, F.; Wittstock, M.; Tronnier, V.; et al. Short- and long-term outcome of chronic pallidal neurostimulation in monogenic isolated dystonia. Neurology 2015, 84, 895–903. [Google Scholar] [CrossRef]
- Jinnah, H.A.; Alterman, R.; Klein, C.; Krauss, J.K.; Moro, E.; Vidailhet, M.; Raike, R. Deep brain stimulation for dystonia: A novel perspective on the value of genetic testing. J. Neural Transm. (Vienna) 2017, 124, 417–430. [Google Scholar] [CrossRef]
- Fuchs, T.; Gavarini, S.; Saunders-Pullman, R.; Raymond, D.; Ehrlich, M.E.; Bressman, S.B.; Ozelius, L.J. Mutations in the THAP1 gene are responsible for DYT6 primary torsion dystonia. Nat. Genet. 2009, 41, 286–288. [Google Scholar] [CrossRef]
- Bressman, S.B.; Raymond, D.; Fuchs, T.; Heiman, G.A.; Ozelius, L.J.; Saunders-Pullman, R. THAP1 (DYT6) mutations in early-onset primary dystonia. Lancet Neurol. 2009, 8, 441–446. [Google Scholar] [CrossRef] [Green Version]
- LeDoux, M.S.; Xiao, J.; Rudzinska, M.; Bastian, R.W.; Wszolek, Z.K.; Van Gerpen, J.A.; Puschmann, A.; Momcilovic, D.; Vemula, S.R.; Zhao, Y. Genotype-phenotype correlations in THAP1 dystonia: molecular foundations and description of new cases. Parkinsonism Relat. Disord. 2012, 18, 414–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groen, J.L.; Ritz, K.; Contarino, M.F.; van de Warrenburg, B.P.; Aramideh, M.; Foncke, E.M.; van Hilten, J.J.; Schuurman, P.R.; Speelman, J.D.; Koelman, J.H.; et al. DYT6 dystonia: mutation screening, phenotype, and response to deep brain stimulation. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 2420–2427. [Google Scholar] [CrossRef] [PubMed]
- Zittel, S.; Moll, C.K.; Bruggemann, N.; Tadic, V.; Hamel, W.; Kasten, M.; Lohmann, K.; Lohnau, T.; Winkler, S.; Gerloff, C.; et al. Clinical neuroimaging and electrophysiological assessment of three DYT6 dystonia families. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 2405–2412. [Google Scholar] [CrossRef] [PubMed]
- Panov, F.; Tagliati, M.; Ozelius, L.J.; Fuchs, T.; Gologorsky, Y.; Cheung, T.; Avshalumov, M.; Bressman, S.B.; Saunders-Pullman, R.; Weisz, D.; et al. Pallidal deep brain stimulation for DYT6 dystonia. J. Neurol. Neurosurg. Psychiatry 2012, 83, 182–187. [Google Scholar] [CrossRef]
- Krause, P.; Bruggemann, N.; Volzmann, S.; Horn, A.; Kupsch, A.; Schneider, G.H.; Lohmann, K.; Kuhn, A. Long-term effect on dystonia after pallidal deep brain stimulation (DBS) in three members of a family with a THAP1 mutation. J. Neurol. 2015, 262, 2739–2744. [Google Scholar] [CrossRef]
- Burke, R.E.; Fahn, S.; Marsden, C.D.; Bressman, S.B.; Moskowitz, C.; Friedman, J. Validity and reliability of a rating scale for the primary torsion dystonias. Neurology 1985, 35, 73. [Google Scholar] [CrossRef] [Green Version]
- Albanese, A.; Sorbo, F.D.; Comella, C.; Jinnah, H.A.; Mink, J.W.; Post, B.; Vidailhet, M.; Volkmann, J.; Warner, T.T.; Leentjens, A.F.; et al. Dystonia rating scales: critique and recommendations. Mov. Disord. Off. J. Mov. Disord. Soc. 2013, 28, 874–883. [Google Scholar] [CrossRef] [Green Version]
- Volkmann, J.; Wolters, A.; Kupsch, A.; Muller, J.; Kuhn, A.A.; Schneider, G.H.; Poewe, W.; Hering, S.; Eisner, W.; Muller, J.U.; et al. Pallidal deep brain stimulation in patients with primary generalised or segmental dystonia: 5-year follow-up of a randomised trial. Lancet Neurol. 2012, 11, 1029–1038. [Google Scholar] [CrossRef]
- Panov, F.; Gologorsky, Y.; Connors, G.; Tagliati, M.; Miravite, J.; Alterman, R.L. Deep brain stimulation in DYT1 dystonia: A 10-year experience. Neurosurgery 2013, 73, 86–93; discussion 93. [Google Scholar] [CrossRef] [Green Version]
- Cif, L.; Vasques, X.; Gonzalez, V.; Ravel, P.; Biolsi, B.; Collod-Beroud, G.; Tuffery-Giraud, S.; Elfertit, H.; Claustres, M.; Coubes, P. Long-term follow-up of DYT1 dystonia patients treated by deep brain stimulation: an open-label study. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.; Carss, K.J.; Rankin, J.; Nichols, J.M.; Grozeva, D.; Joseph, A.P.; Mencacci, N.E.; Papandreou, A.; Ng, J.; Barral, S.; et al. Mutations in the histone methyltransferase gene KMT2B cause complex early-onset dystonia. Nat. Genet. 2017, 49, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Deutschlander, A.; Asmus, F.; Gasser, T.; Steude, U.; Botzel, K. Sporadic rapid-onset dystonia-parkinsonism syndrome: Failure of bilateral pallidal stimulation. Mov. Disord. Off. J. Mov. Disord. Soc. 2005, 20, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Di Giovanni, M.; Amami, P.; Lalli, S. Failure of pallidal deep brain stimulation in DYT12-ATP1A3 dystonia. Parkinsonism Relat. Disord. 2017, 45, 99–100. [Google Scholar] [CrossRef]
- Vuletic, V.; Chudy, D.; Almahariq, F.; Dobricic, V.; Kostic, V.; Bogdanovic, N. Excellent outcome of pallidal deep brain stimulation in DYT6 dystonia: A case report. J. Neurol. Sci. 2016, 366, 18–19. [Google Scholar] [CrossRef]
- Jech, R.; Bares, M.; Krepelova, A.; Urgosik, D.; Havrankova, P.; Ruzicka, E. DYT 6-a novel THAP1 mutation with excellent effect on pallidal DBS. Mov. Disord. Off. J. Mov. Disord. Soc. 2011, 26, 924–925. [Google Scholar] [CrossRef]
- Tsering, D.; Tochen, L.; Lavenstein, B.; Reddy, S.K.; Granader, Y.; Keating, R.F.; Oluigbo, C.O. Considerations in deep brain stimulation (DBS) for pediatric secondary dystonia. Child’s Nerv. Syst. CHNS Off. J. Int. Soc. Pediatric Neurosurg. 2017, 33, 631–637. [Google Scholar] [CrossRef]
- Coubes, P.; Cif, L.; El Fertit, H.; Hemm, S.; Vayssiere, N.; Serrat, S.; Picot, M.C.; Tuffery, S.; Claustres, M.; Echenne, B.; et al. Electrical stimulation of the globus pallidus internus in patients with primary generalized dystonia: long-term results. J. Neurosurg. 2004, 101, 189–194. [Google Scholar] [CrossRef]
- Alterman, R.L.; Tagliati, M. Deep brain stimulation for torsion dystonia in children. Child’s Nerv. Syst. CHNS Off. J. Int. Soc. Pediatric Neurosurg. 2007, 23, 1033–1040. [Google Scholar] [CrossRef]
- Vasques, X.; Cif, L.; Gonzalez, V.; Nicholson, C.; Coubes, P. Factors predicting improvement in primary generalized dystonia treated by pallidal deep brain stimulation. Mov. Disord. Off. J. Mov. Disord. Soc. 2009, 24, 846–853. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Number | Gender | THAP1 (NM_018105.3) Sequence Variant | Patient Previously Reported | Variant Previously Reported | Age at Disease Onset (Years) | Initial Anatomical Distribution | Preop BFM-M | Preop BFM-D | Preoperative Medication |
|---|---|---|---|---|---|---|---|---|---|
| 1 | F | c.-34G > A variant in the 5’ untranslated region | no | no | 42 | cervical | 16 | 4 | botulinum toxin, benzodiazepines, gabapentin, NSAID |
| 2 | F | c.377_378delCT p.Pro126Argfs*2 exon 3 | no | Blanchard 2011 PMID: 21520283 | 9 | cervical | 62 | 10 | L-dopa, botulinum toxin |
| 3 | M | c.173T > C p.Phe58Ser exon 2 | no | Miyamoto 2014 PMID: 24227593 | 6 | left foot | 78.5 | 28 | baclofen, L-dopa, trihexyphenidyl |
| 4 | F | c.70_71+8del10 p.Gly24fs*71 exon 1 | no | no | 15 | right upper limb | 32.5 | 9 | trihexyphenidyl, baclofen |
| 5 | M | c.464A > C p.Gln155Pro exon 3 | no | no | 6 | right upper limb | 45 | 5 | trihexyphenidyl, baclofen |
| 6 | M | c.238A > G p.Ile80Val exon 2 | no | Ledoux 2012 PMID: 22377579 Lohmann 2012 PMID: 21847143 Golanska 2015 PMID: 26087139 | 14 | cervical | 60 | 15 | trihexyphenidyl, valproic acid, gabapentin |
| 7 | F | c.94C > T p.Leu32Phe exon 2 | no | no | 7 | right upper limb | 35.5 | 12 | trihexyphenidyl |
| 8 | F | c.70_71 + 8del10 p.Gly24fs*71 exon 1 | no | no | 40 | cervical | 23 | 6 | botulinum toxin, benzodiazepine |
| 9 | F | c.207_209delCAA p.Asn69-Asn69del exon 2 | no | Groen 2010 PMID: 20687191 Clot 2011 PMID: 21110056 | 6 | right upper limb | 62 | 10 | L-dopa, trihexyphenidyl |
| 10 | F | c.85C > T premature stop codon at amino acid position 29 exon 2 | no | Djamarti 2009 PMID: 19345148 Bressman 2009 PMID: 19345147 Xiromerisiou 2012 PMID: 22903657 Dobričić 2013 PMID: 23180184 | 9 | right lower limb | 61 | 10 | L-dopa, trihexyphenidyl, botulinum toxin |
| 11 | F | c.16T > C p.Ser6Pro exon 1 | Cif 2012 PMID: 22339165 (prior to the DYT-THAP1 diagnosis) | Clot 2011 PMID: 21110056 | 9 | speech | 43.5 | 13 | benzodiazepines, trihexyphenidyl, carbamazepine |
| 12 | M | c.77C > G p.Pro26Arg exon 2 | Lumsden 2012 PMID: 23452222 (prior to the DYT-THAP1 diagnosis) | Houlden 2010 PMID: 20211909 Campagne 2012 PMID: 22844099 | 4 | Hands | 79 | 26 | L-dopa, trihexiphenidyl, bensodiazepine |
| 13 | M | c.19G > A p.Ala7Thr exon 1 | no | no | 6 | left foot | 87 | 23 | L-dopa |
| 14 | F | c.98G > A p.Cys33Tyr exon2 variant of uncertain significance | no | no | 9 | left foot | 36.5 | 8 | trihexyphenidyl, L-dopa |
| Patient Number | Age at GPi-DBS (Years) | Disease Duration Before GPi-DBS (Years) | Length of Follow-Up after GPi-DBS (Years, Months) | Change in BFM-M, Last Follow-Up Compared to Baseline (%) | Responder (>25% Improvement BFM-M) | Effect on Speech and/or Swallowing | Intra-Cerebral Revision (number) | DBS Device at Last Follow-Up (Number of Changes) | Stimulation Frequency at Last Follow-Up (Hz) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 57 | 15 | 1 year 8 months | −13 | no | no | 0 | Medtronic Activa RC (1) | 130 |
| 2 | 14 | 5 | 1 year 2 months | −37 | yes | some | 0 | Medtronic Activa PC | 130 |
| 3 | 13 | 7 | 11 years 1 month | −21 | initially | some | 0 | Medtronic Activa RC (2) | 130 |
| 4 | 17 | 2 | 10 years 0 month | −57 | yes | no | 0 | Activa RC (2) | 180 |
| 5 | 14 | 8 | 8 years 7 months | −29 | yes | no | 0 | Medtronic Activa RC (1) | 180 |
| 6 | 32 | 18 | 7 months | −68 | yes | no | 0 | Medtronic Activa SC | 100 |
| 7 | 26 | 19 | 13 years 9 months | −78 | yes | no | 0 | Medtronic Activa SC (1) | RGPi 110; LGPi 90 |
| 8 | 54 | 14 | 3 years 7 months | −61 | yes | no | 0 | Medtronic Activa SC | RGPi 125; LGPi 90 |
| 9 | 11 | 5 | 6 years 0 month | −62 | yes | no | 0 | Medtronic Activa RC | 130 |
| 10 | 22 | 13 | 1 year 0 month | −74 | yes | no | 0 | Soletra, medtronic leads | 130 |
| 11 | 20 | 11 | 16 years 4 months | −60 | yes | no | 1 | Medtronic Activa RC | 130 |
| 12 | 12 | 8 | 6 years 11 months | −46 | yes | some | 0 | Activa RC (1) | 130 |
| 13 | 8 | 2 | 1 year 1 month | −20 | no | some | 2 | Medtronic Activa RC (1) | NR |
| 14 | 19 | 10 | 1 year 0 month | −58 | yes | no | 0 | Vercise-DBS-system/Boston Scientific | 130 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danielsson, A.; Carecchio, M.; Cif, L.; Koy, A.; Lin, J.-P.; Solders, G.; Romito, L.; Lohmann, K.; Garavaglia, B.; Reale, C.; et al. Pallidal Deep Brain Stimulation in DYT6 Dystonia: Clinical Outcome and Predictive Factors for Motor Improvement. J. Clin. Med. 2019, 8, 2163. https://doi.org/10.3390/jcm8122163
Danielsson A, Carecchio M, Cif L, Koy A, Lin J-P, Solders G, Romito L, Lohmann K, Garavaglia B, Reale C, et al. Pallidal Deep Brain Stimulation in DYT6 Dystonia: Clinical Outcome and Predictive Factors for Motor Improvement. Journal of Clinical Medicine. 2019; 8(12):2163. https://doi.org/10.3390/jcm8122163
Chicago/Turabian StyleDanielsson, Annika, Miryam Carecchio, Laura Cif, Anne Koy, Jean-Pierre Lin, Göran Solders, Luigi Romito, Katja Lohmann, Barbara Garavaglia, Chiara Reale, and et al. 2019. "Pallidal Deep Brain Stimulation in DYT6 Dystonia: Clinical Outcome and Predictive Factors for Motor Improvement" Journal of Clinical Medicine 8, no. 12: 2163. https://doi.org/10.3390/jcm8122163