Physical Health and Psychological Outcomes in Adult Patients with Long-Bone Fracture Non-Unions: Evidence Today

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Data Extraction
2.1.1. Inclusion Criteria
- Participants—adult (human) patients over the age of 18 years with diaphyseal long bone fracture non-union(s). Other anatomical sites and non-diaphyseal fracture types were excluded. Eligible studies were those written in English and published after 1995.
- Intervention—no particular intervention needed.
- Comparison—to the situation after union was achieved or to matched population norms.
- Outcome—physical health measures and psychological wellbeing measures (e.g., Post-Traumatic Stress Disorder (PTSD), psychological trauma, depression, anxiety, etc.).
2.1.2. Exclusion Criteria
2.2. Methodological Quality Assessment
2.3. Statistical Analysis
2.3.1. Subgroup Analysis
2.3.2. Sensitivity Analysis
3. Results
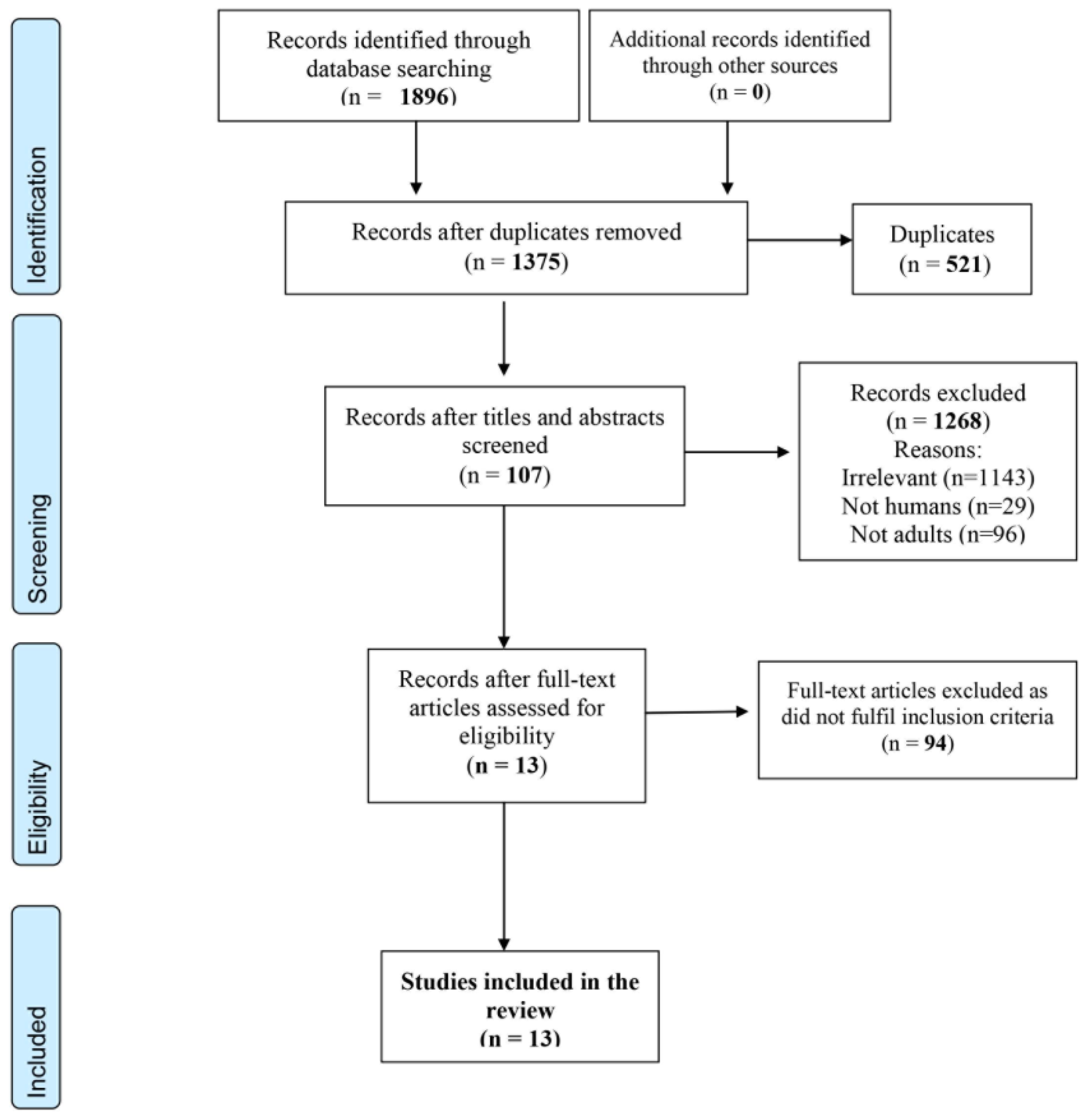
3.1. Study Selection Procedure
3.2. Characteristics of Included Studies
3.3. Methodological Quality of Included Studies
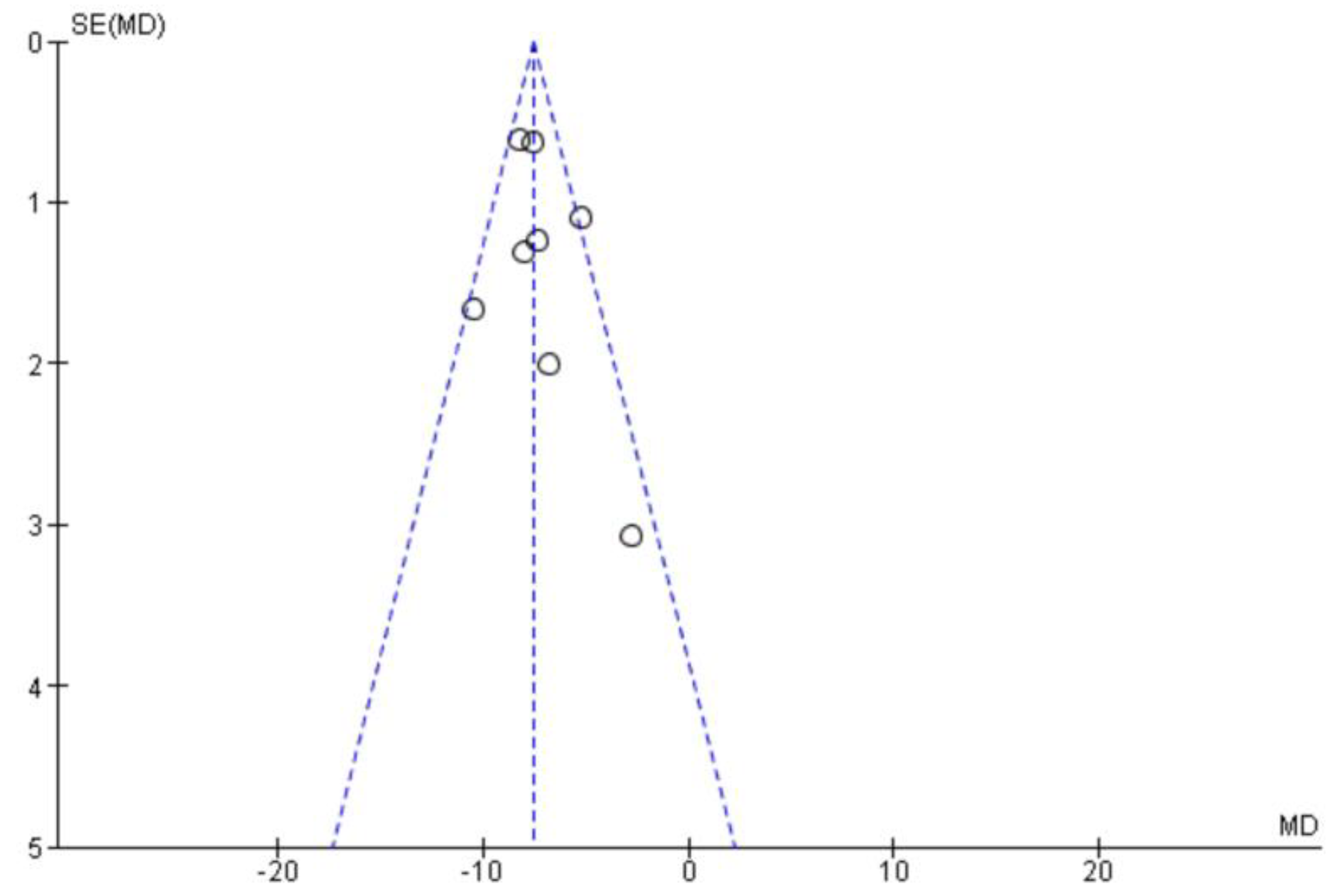
3.4. Publication Bias
3.5. Physical Health State Assessment
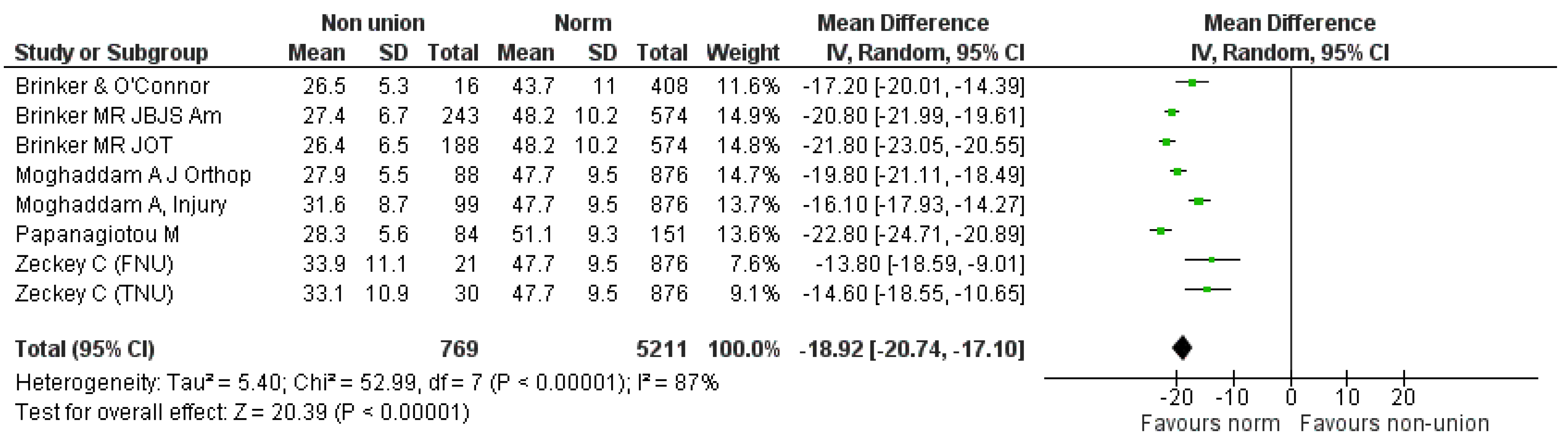
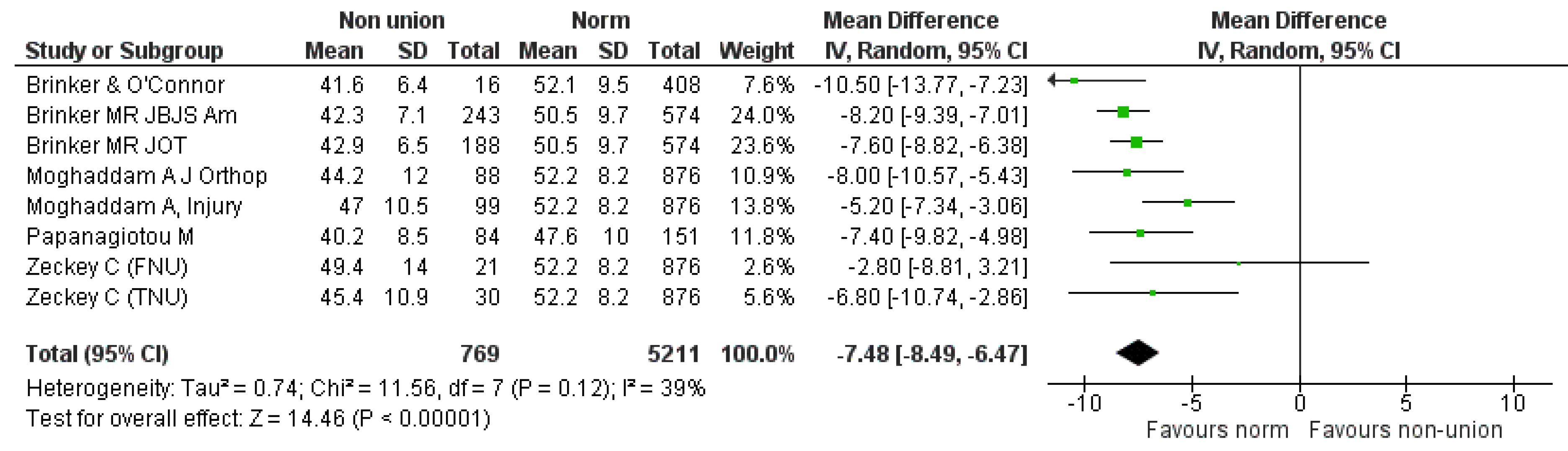
3.6. Quantitative Analysis
3.7. Subgroup Analysis
3.8. Sensitivity Analysis
3.9. Non-Quantitative Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Schmidmaier, G.; Moghaddam, A. Long bone nonunion. Z. Orthop. Unf. 2015, 153, 659–674. [Google Scholar] [CrossRef]
- Available online: https://www.nice.org.uk/guidance/mtg12/chapter/1-Recommendations (accessed on 27 September 2019).
- Bishop, J.A.; Palanca, A.A.; Bellino, M.J.; Lowenberg, D.W. Assessment of compromised fracture healing. J. Am. Acad. Orthop. Surg. 2012, 20, 273–282. [Google Scholar] [CrossRef]
- Mills, L.A.; Simpson, A.H.R.W. The relative incidence of fracture non-union in the Scottish population (5.17 million): A 5-year epidemiological study. BMJ Open 2013, 3, e002276. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.nice.org.uk/guidance/mtg12/chapter/2-The-technology (accessed on 27 September 2019).
- Kanakaris, N.K.; Giannoudis, P.V. The health economics of the treatment of long-bone non-unions. Injury 2007, 38, S77–S84. [Google Scholar] [CrossRef]
- Tay, W.H.; de Steiger, R.; Richardson, M.; Gruen, R.; Balogh, Z.J. Health outcomes of delayed union and nonunion of femoral and tibial shaft fractures. Injury 2014, 45, 1653–1658. [Google Scholar] [CrossRef]
- Brinker, M.R.; Hanus, B.D.; Sen, M.; O’Connor, D.P. The Devastating Effects of Tibial Nonunion on Health-Related Quality of Life. J. Bone Jt. Surg. Am. 2013, 95, 2170–2176. [Google Scholar] [CrossRef]
- Zeckey, C.; Mommsen, P.; Andruszkow, H.; Macke, C.; Frink, M.; Stübig, T.; Hüfner, T.; Krettek, C.; Hildebrand, F. The aseptic femoral and tibial shaft non-union in healthy patients -an analysis of the health-related quality of life and the socioeconomic outcome. Open Orthop. J. 2011, 5, 193–197. [Google Scholar] [CrossRef]
- Wichlas, F.; Tsitsilonis, S.; Disch, A.C.; Haas, N.P.; Hartmann, C.; Graef, F.; Schwabe, P. Long-term functional outcome and quality of life after successful surgical treatment of tibial nonunions. Int. Orthop. 2015, 39, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Bowen, C.V.; Botsford, D.J.; Hudak, P.L.; Evans, P.J. Microsurgical treatment of septic nonunion of the tibia. Quality of life results. Clin. Orthop. Relat. Res. 1996, 332, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Zlowodzki, M.; Obremskey, W.T.; Thomison, J.B.; Kregor, P.J. Functional outcome after treatment of lower-extremity nonunions. J. Trauma 2005, 58, 312–317. [Google Scholar] [CrossRef]
- Brinker, M.R.; O’Connor, D.P. Outcomes of tibial nonunion in older adults following treatment using the Ilizarov method. J. Orthop. Trauma 2007, 21, 634–642. [Google Scholar] [CrossRef]
- Braly, H.L.; O’Connor, D.P.; Brinker, M.R. Percutaneous autologous bone marrow injection in the treatment of distal meta-diaphyseal tibialnonunions and delayed unions. J. Orthop. Trauma 2013, 27, 527–533. [Google Scholar] [CrossRef]
- Moghaddam, A.; Zietzschmann, S.; Bruckner, T.; Schmidmaier, G. Treatment of atrophic tibia non-unions according to ‘diamond concept’: Results of one- and two-step treatment. Injury 2015, 46, S39–S50. [Google Scholar] [CrossRef]
- Papanagiotou, M.; Dailiana, Z.H.; Karachalios, T.; Varitimidis, S.; Vlychou, M.; Hantes, M.; Malizos, K.N. RhBMP-7 for the treatment of nonunion of fractures of long bones. Bone Jt. J. 2015, 97, 997–1003. [Google Scholar] [CrossRef]
- Schottel, P.C.; O’Connor, D.P.; Brinker, M.R. Time trade-off as a measure of health-related quality of life: Long bone nonunions have a devastating impact. J. Bone Jt. Surg. Am. 2015, 97, 1406–1410. [Google Scholar] [CrossRef]
- Brinker, M.R.; Trivedi, A.; O’Connor, D.P. Debilitating effects of femoral nonunion on health-related quality of life. J. Orthop. Trauma 2017, 31, e37–e42. [Google Scholar] [CrossRef]
- Moghaddam, A.; Thaler, B.; Bruckner, T.; Tanner, M.; Schmidmaier, G. Treatment of atrophic femoral non-unions according to the diamond concept: Results of one- and two-step surgical procedure. J. Orthop. 2016, 14, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- Kontodimopoulos, N.; Pappa, E.; Niakas, D.; Tountas, Y. Validity of SF-12 summary scores in a Greek general population. Health Qual. Life Outcomes 2007, 5, 55. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the hospital anxiety and depression scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of event scale: A measure of subjective stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef]
- Richter, J.C.; Waydhas, C.; Pajonk, F.G. Incidence of posttraumatic stress disorder after prolonged surgical intensive care unit treatment. Psychosomatics 2006, 47, 223–230. [Google Scholar] [CrossRef]
- Starr, A.J.; Smith, W.R.; Frawley, W.H.; Borer, D.S.; Morgan, S.J.; Reinert, C.M.; Mendoza-Welch, M. Symptoms of posttraumatic stress disorder after orthopaedic trauma. J. Bone Jt. Surg. Am. 2004, 86, 1115–1121. [Google Scholar] [CrossRef]
- Quale, A.J.; Schanke, A.K.; Froslie, K.F.; Roise, O. Severity of injury does not have any impact on posttraumatic stress symptoms in severely injured patients. Injury 2009, 40, 498–505. [Google Scholar] [CrossRef]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Burdine, J.N.; Felix, M.R.; Abel, A.L.; Wiltraut, C.J.; Musselman, Y.J. The SF-12 as a population health measure: An exploratory examination of potential for application. Health Serv. Res. 2000, 35, 885–904. [Google Scholar] [PubMed]
- Johnson, J.A.; Pickard, A.S. Comparison of the EQ-5D and SF-12 health surveys in a general population survey in Alberta, Canada. Med. Care 2000, 38, 115–121. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study No. | Name (year) [Country] | Reference | Sample | Sex distribution | Age Range (Median) | Anatomic Location | Mechanism of Injury (Open/Closed Fracture) (Type NU) |
|---|---|---|---|---|---|---|---|
| Study 1 | Bowen et al. (1996) (Canada) | [15] | 9 patients Septic only | Males: 8 Females: 1 | 17–69 (32) | Tibial | Yes |
| Study 2 | Zlowodzki et al. (2005) (USA) | [16] | 23 patients 5 septic (not defined femur/tib) | Unknown | 7 Tibial 16 femoral | No | |
| Study 3 | Brinker (2007) (USA) | [17] | 23 patients 8 septic | Males: 8 Females: 15 | 61–92 (72) | Tibial | No (open/closed) |
| Study 4 | Zeckey et al. (2011) (Germany) | [9] | 51 patients Aseptic only | M: (TNU 21/FNU 14) F: (TNU 9/FNU 7) | Femur: (41.5) Tibia: (37.6) | 21 Femoral 30 Tibial | No |
| Study 5 | Braly et al. (2013) (USA) | [18] | 11 patients Aseptic only | Males: 4 Females: 7 | 24–51 (40.1) | Tibial | No |
| Study 6 | Brinker et al. (2013) (USA) | [8] | 237 patients 44 septic | Males: 158 Females: 79 | Males: (46.3) Females: (49.4) | 243 Tibial | No (open/closed) |
| Study 7 | Tay et al. (2014) (Australia) | [7] | 138 patients delayed/nonunion | Males: 107 Females: 31 | 127 younger than 65 years | Femoral and Tibial | Yes (open/closed) |
| Study 8 | Moghaddam et al. (2015) (Germany) | [19] | 99 patients 35 septic | Males: 74 Females: 25 | (47.4) | Tibial NU 49 (1 step) 50 (2 steps) | No (open/closed) |
| Study 9 | Papanagiotou et al. (2015) (Greece) | [20] | 84 patients 30 septic | Males: 60 Females: 24 | 18–81 (46) | 41 Tibial 30 Femoral 10 Humeral 3 Forearm | No (Hypertrophic/atrophic) |
| Study 10 | Schottel et al. (2015) (USA) | [21] | 832 patients 106 septic | Males: 488 Females: 346 | 18–93 (49.6) | 435 Tibias 201 Femoral 125 Humeral 33 Forearm 38 Clavicle | No |
| Study 11 | Wichlas et al. (2015) (Germany) | [10] | 64 patients 30 septic | Males: 49 Females: 15 | 19–78 (42.8) | Tibial | Yes (open/closed) (Hypertrophic/atrophic) |
| Study 12 | Brinker et al. (2017) (USA) | [22] | 187 patients 10 septic | Males: 102 Females: 85 | Males: (42.8) Females: (55.9) | 188 Femoral | No (open/closed) |
| Study 13 | Moghaddam et al. (2017) (Germany) | [23] | 88 patients 72 BMP-7 16 septic | Males: 43 Females: 45 | (49.9) | Femoral One stage:41 Two stages:47 | Yes (open/closed) Atrophic only |
| Author (year) | Design | QoL | Psych | Pre-Intervention | Post-Intervention | Comparison/Groups | MINORS Score |
|---|---|---|---|---|---|---|---|
| Bowen et al. (1996) | Retrospective cohort | SF-36 WOMAC | N/A | ✓ (1–6 years, median 3) | Septic NU vs. USA age-adjusted norms (35–44). Absence of control group | 13 | |
| Zlowodzki et al. (2005) | Prospective cohort | SF-36 | N/A | ✓ (2 weeks before surgery) | ✓ (236–740 days, Median: 449) | vs. normal US population. Also septic vs. aseptic NU | 13 |
| Brinker (2007) | Prospective cohort | SF-12 QALY’s | N/A | ✓ | ✓ (18–61 months, Median 38 months) | Pre-op vs. post-op outcome scores | 9 |
| Zeckey et al. (2011) | Retrospective cohort | SF-12 | HADS IES | ✓ | aseptic NU vs. uneventful healing | 10 | |
| Braly et al. (2013) | Prospective cohort | SF-12 Time trade-off | N/A | ✓ | ✓ (1.3–8.2 years, median 4.4 years) | Pre-op vs. post-op outcome scores | 12 |
| Brinker et al. (2013) | Prospective cohort | SF-12 Time trade-off | N/A | ✓ | NU vs. other orthopaedic conditions/chronic medical problems/general US population | 9 | |
| Tay et al. (2014) | Retrospective cohort | SF-12 | N/A | ✓ (up to 1 year) | NU/DU vs. uneventful healing | 14 | |
| Moghaddam et al. (2015) | Prospective cohort | SF-12 | N/A | ✓ | ✓ (up to 1 year) | 1-step vs. 2-step Masquelet Each group pre-op vs. post-op | 17 |
| Papanagiotoy et al. (2015) | Prospective cohort | SF-12 | N/A | ✓ | ✓ (up to 1 year) | Pre-op vs. post-op outcome scores | 10 |
| Schottel et al. (2015) | Retrospective cohort | Time trade-off | N/A | ✓ | NU in different anatomical sites vs. general population/medical problems | 14 | |
| Wichlas et al. (2015) | Retrospective cohort | SF-36 | N/A | ✓ (median 5 years) | vs. normal population | 16 | |
| Brinker et al. (2017) | Retrospective cohort | SF-12 Time trade-off | N/A | ✓ | NU vs. other orthopaedic conditions/chronic medical problems/general US population | 12 | |
| Moghaddam et al. (2017) | Prospective case series | SF-12 | N/A | X | X (up to 1 year) | 1-step vs. 2-step Masquelet Each group pre-op vs. post-op | 20 |
| Comparison | Original Analysis | Number of Studies | Refs | Mean Difference [95% CI] | Statistical Method | Statistical Model | Hetero-Geneity |
|---|---|---|---|---|---|---|---|
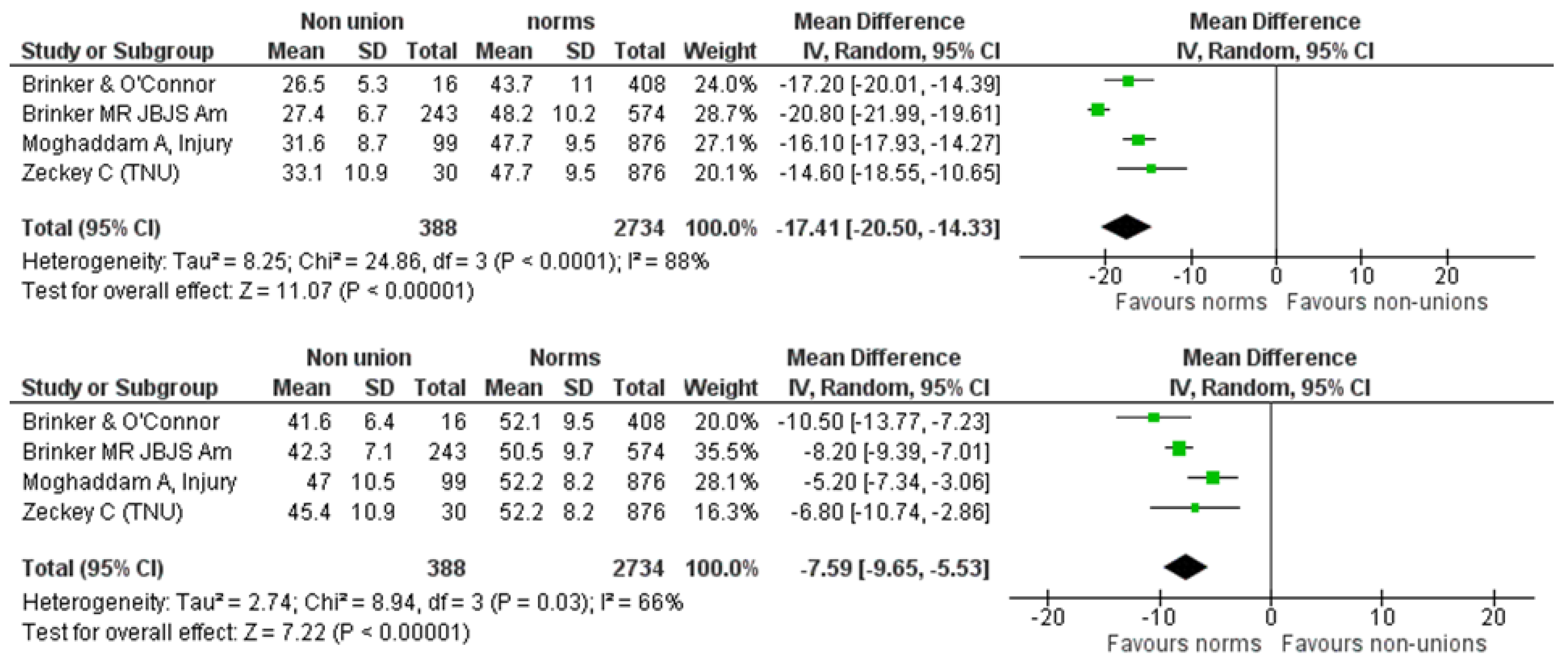
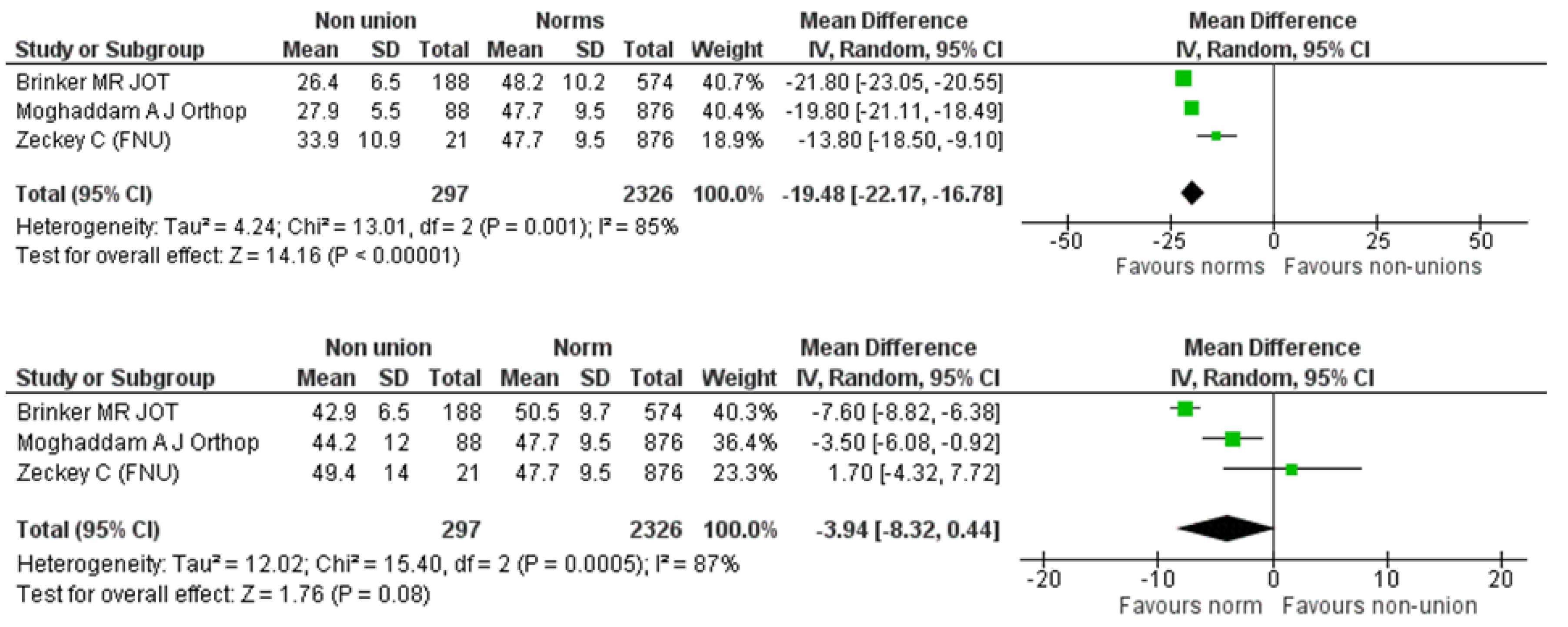
| SF-12 PCS pooled analysis of non-union versus normal population. | Figure 3 | 3 | [19,22,23] | −19.30 [−22.27, −16.33] | Inverse Variance (IV) | Random effects | I2 = 92% |
| SF-12 MCS pooled analysis between non-union and respective normal population. | Figure 4 | 3 | [19,22,23] | −6.98 [−8.57, −5.40] | IV | Random effects | I2 = 52% |
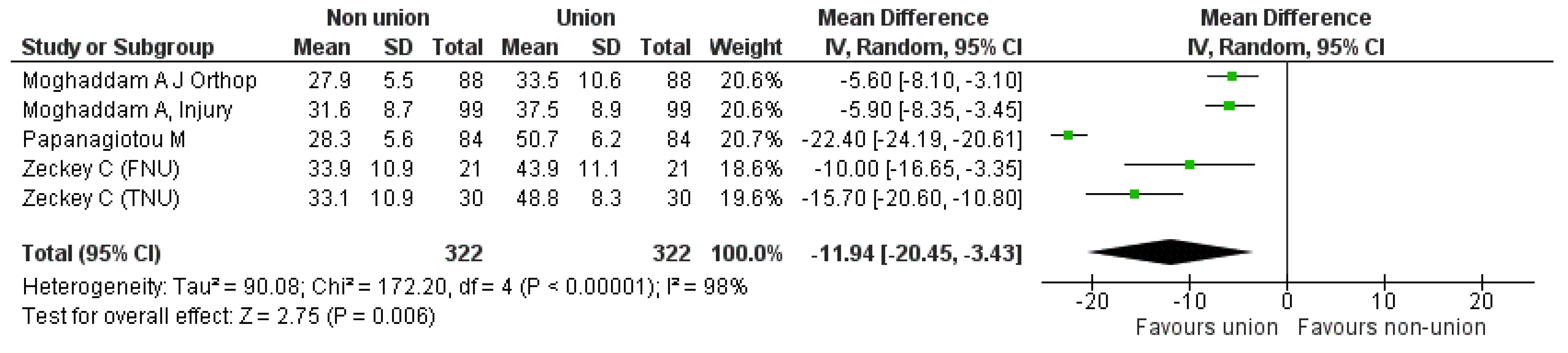
| SF-12 PCS pooled analysis between nonunion and union. | Figure 5 | 2 | [19,23] | −5.75 [−7.50, −4.0] | IV | Fixed effects | I2 = 0 |
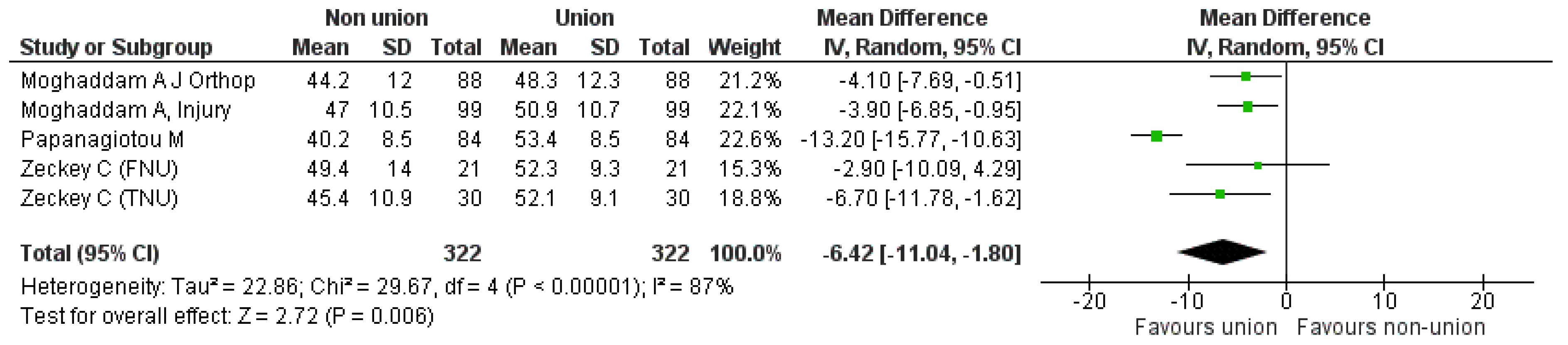
| SF-12 MCS pooled analysis between nonunion and union. | Figure 6 | 2 | [19,23] | −3.98 [−6.26, −1.70] | IV | Fixed effects | I2 = 0 |
| Author [ref] | Wei-Han Tay [7] | Braly HL [18] | Schottel PC [21] | ||
|---|---|---|---|---|---|
| Anatomical Site | Fem/Tibia | Long bones | |||
| DU/NU | P-treat | DU/NU | P-treat | Non unions | |
| Population Size | 285 | 138 | 6 | 6 | 832 |
| SF-12 | |||||
| PCS | 32 (median) | 44 (median) | 29.5 (mean) | 46.6 (mean) | |
| 18 (IQR) | 22 (IQR) | 3.3 (sd) | 4.8 (sd) | ||
| MCS | 51 (median) | 56 (median) | nr | nr | |
| 19 (IQR) | 13 (IQR) | ||||
| Return to Work | 59% (62/105) | 72% (145/202) | nr | nr | |
| Ongoing Pain | 72% (76/106) | 54% (114/212) | nr | nr | |
| AAOS Lower Limb Core Scale | 55.9 (40.8–83.6) | 87.7 (65.7–100) | |||
| BPI (intensity) | 2.9 | 2.7 | |||
| BPI (intereference) | 4.6 | 2.3 | |||
| Time Trade-off | 19% | 5% | Mean utility score: 0.68 | ||
| Time Trade-off (years) | 5.6 | ||||
| Author [ref] | Wichlas F [10] | Zlowodzki M [16] | Bowen CVA [15] | |||||
|---|---|---|---|---|---|---|---|---|
| Anatomical Site | Tibia | Femur:16, Tib.: 7 | Septic tibial nonunions (n = 8) | |||||
| Population Size | 64 | 23 | 8 | |||||
| SF-36 | Study population (n = 64) | Normal population (45–65 years) | p-value | Study Population | After Tx | p-value | Study population (n = 8) | Normal population (35–44 years). (Only p-values are reported) |
| General Health | 61 ± 25 | 62.7 ± 18.8 | 0.59 | 56 ± 26 | 57 ± 24 | 0.751 | p < 0.001 | |
| Physical Functioning | 64 ± 31 | 79.1 ± 22.4 | <0.001 | 232 ± 6 | 43 ± 29 | 0.002 | p < 0.01 | |
| Role Physical | 64 ± 45 | 74 ± 37.6 | 0.08 | 3 ± 8 | 36 ± 37 | 0.001 | ns | |
| Role Emotional | 74 ± 43 | 84.8 ± 28.5 | 0.049 | 28 ± 44 | 49 ± 45 | 0.072 | ns | |
| Social Functioning | 76 ± 27 | 83 ± 22 | 0.04 | 27 ± 27 | 46 ± 32 | 0.042 | ns | |
| Bodily Pain | 65 ± 30 | 58.5 ± 25.8 | <0.001 | 23 ± 19 | 28 ± 17 | 0.308 | p < 0.001 | |
| Vitality | 51 ± 22 | 57.7 ± 18.7 | 0.018 | 42 ± 23 | 45 ± 22 | 0.681 | ns | |
| Mental Health | 64 ± 25 | 68.8 ± 18.5 | 0.13 | 57 ± 23 | 63 ± 22 | 0.302 | p < 0.001 | |
| Author [ref] | Zeckey C et al. [9] | ||
|---|---|---|---|
| Parameter | TNU (n = 30) | TH (n = 30) | p-Value |
| IES | 19.1 ± 2.5 | 12.7 ± 2.9 | 0.01 |
| HADS-D | 4.1 ± 4.1 | 2.8 ± 4.1 | 0.3 |
| HADS-A | 6.2 ± 3.7 | 4.8 ± 4.4 | 0.8 |
| FNU (n = 21) | FH (n = 21) | ||
| IES | 16.5 ± 11.1 | 18.3 ± 8.4 | 0.7 |
| HADS-D | 5.9 ± 4.7 | 3.6 ± 3.9 | 0.4 |
| HADS-A | 5.7 ± 4.8 | 3.9 ± 2.2 | 0.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, L.; Igoe, E.; Kleftouris, G.; Papachristos, I.V.; Papakostidis, C.; Giannoudis, P.V. Physical Health and Psychological Outcomes in Adult Patients with Long-Bone Fracture Non-Unions: Evidence Today. J. Clin. Med. 2019, 8, 1998. https://doi.org/10.3390/jcm8111998
Johnson L, Igoe E, Kleftouris G, Papachristos IV, Papakostidis C, Giannoudis PV. Physical Health and Psychological Outcomes in Adult Patients with Long-Bone Fracture Non-Unions: Evidence Today. Journal of Clinical Medicine. 2019; 8(11):1998. https://doi.org/10.3390/jcm8111998
Chicago/Turabian StyleJohnson, Louise, Emily Igoe, George Kleftouris, Ioannis V. Papachristos, Costas Papakostidis, and Peter V. Giannoudis. 2019. "Physical Health and Psychological Outcomes in Adult Patients with Long-Bone Fracture Non-Unions: Evidence Today" Journal of Clinical Medicine 8, no. 11: 1998. https://doi.org/10.3390/jcm8111998