Intravesical Chemotherapy after Radical Nephroureterectomy for Primary Upper Tract Urothelial Carcinoma: A Systematic Review and Network Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
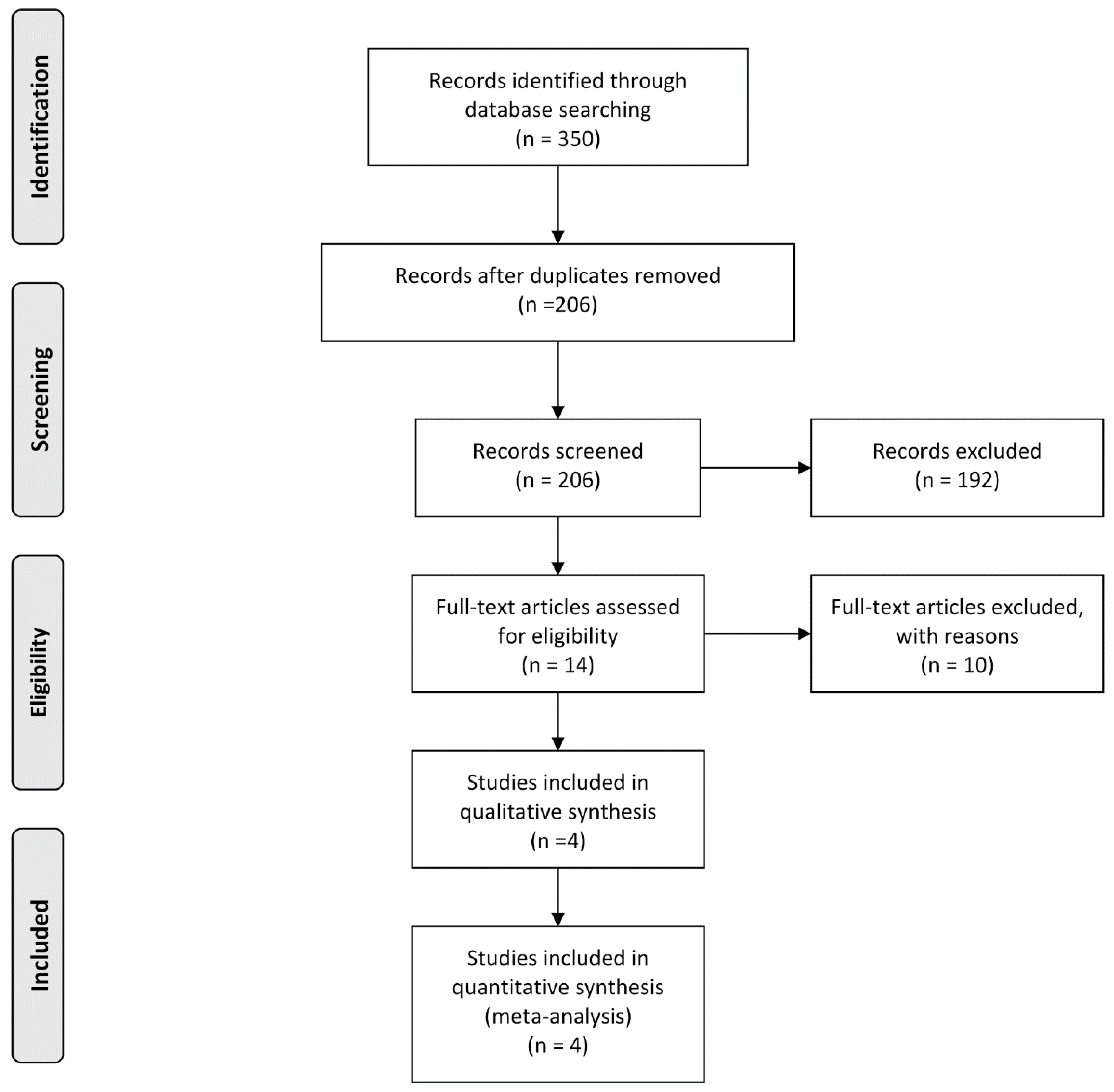
2.1. Search Strategy
2.2. Eligible Criteria
- (1)
- Articles included patients with primary upper tract urothelial carcinoma.
- (2)
- Articles compared intravesical recurrence with or without intravesical chemotherapy.
- (3)
- Articles reported intravesical-recurrence free survival rates after radical nephroureterectomy.
- (1)
- Non-human study.
- (2)
- Review articles, letters, editorial comments, and case reports.
- (3)
- Articles without sufficient data to acquire hazard ratio (HR) or standard error (SE).
- (4)
- Articles including conservative surgery instead of radical surgery, other neoadjuvant or adjuvant treatment, metastatic disease, or non-urothelial carcinoma.
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Overview of Studies Included
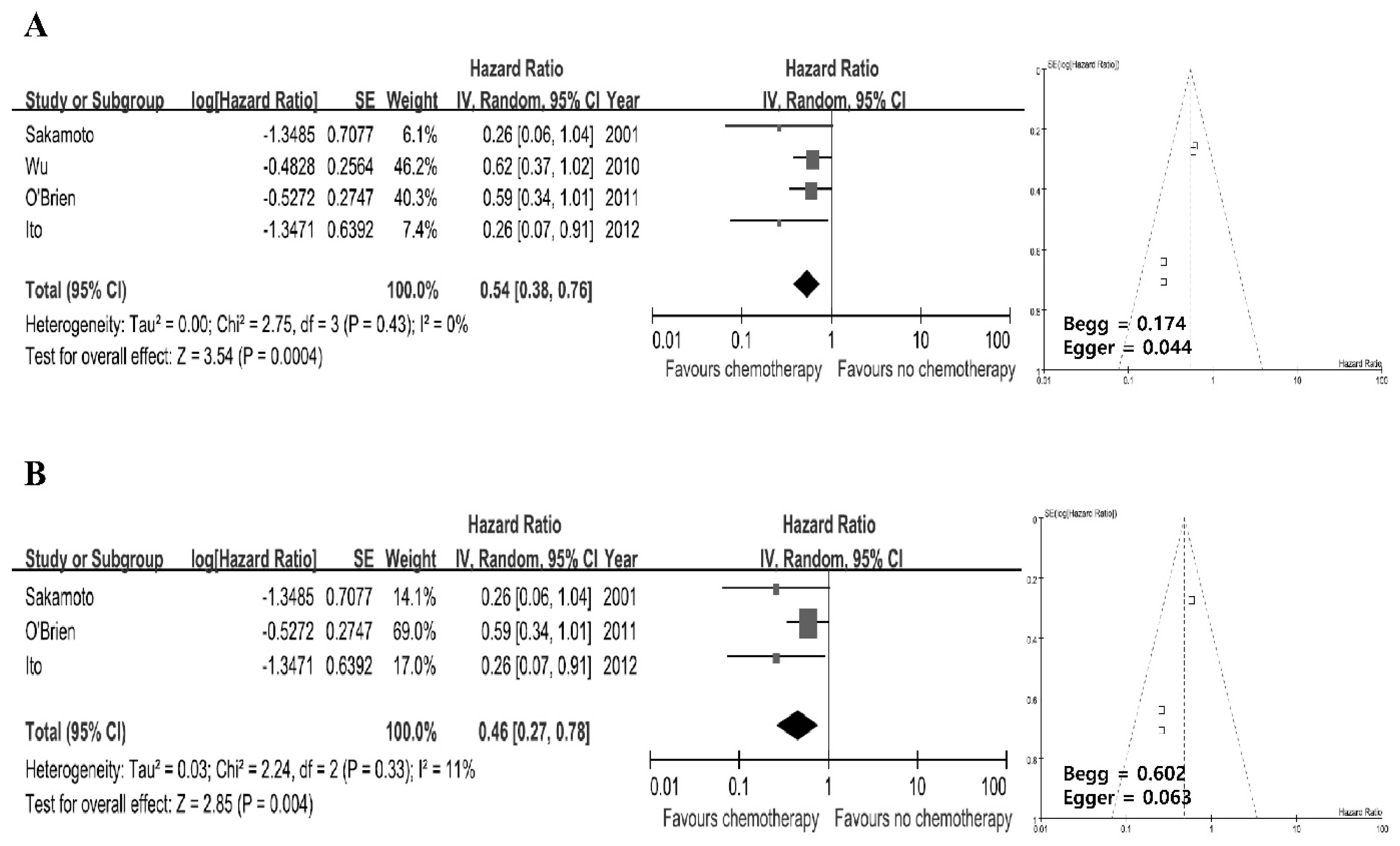
3.2. Pair-Wise Meta-Analysis
3.3. Bayesian Framework Network Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, H.; Mao, X.; Bai, Y.; Li, H.; Liu, L.; Pu, C.; Li, J.; Tang, Y.; Wei, Q.; Han, P. The effect of intravesical chemotherapy in the prevention of intravesical recurrence after nephroureterectomy for upper tract urothelial carcinoma: A meta-analysis. J. Chemother. 2015, 27, 195–200. [Google Scholar] [CrossRef]
- Wu, P.; Zhu, G.; Wei, D.; Liu, S.; Walsh, K.; Li, D.; Harron, U.; Wang, X.; Ma, H.; Wan, B.; et al. Prophylactic intravesical chemotherapy decreases bladder tumor recurrence after nephroureterectomy for primary upper tract urothelial carcinoma: A systematic review and meta-analysis. J. BUON 2015, 20, 1229–1238. [Google Scholar] [PubMed]
- Zigeuner, R.; Pummer, K. Urothelial Carcinoma of the Upper Urinary Tract: Surgical Approach and Prognostic Factors. Eur. Urol. 2008, 53, 720–731. [Google Scholar] [CrossRef] [PubMed]
- Seisen, T.; Granger, B.; Colin, P.; Léon, P.; Utard, G.; Renard-Penna, R.; Compérat, E.; Mozer, P.; Cussenot, O.; Shariat, S.F.; et al. A Systematic Review and Meta-analysis of Clinicopathologic Factors Linked to Intravesical Recurrence after Radical Nephroureterectomy to Treat Upper Tract Urothelial Carcinoma. Eur. Urol. 2015, 67, 1122–1133. [Google Scholar] [CrossRef] [PubMed]
- Li, W.-M.; Shen, J.-T.; Li, C.-C.; Ke, H.-L.; Wei, Y.-C.; Wu, W.-J.; Chou, Y.-H.; Huang, C.-H. Oncologic Outcomes Following Three Different Approaches to the Distal Ureter and Bladder Cuff in Nephroureterectomy for Primary Upper Urinary Tract Urothelial Carcinoma. Eur. Urol. 2010, 57, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.-J.; Ke, H.-L.; Yang, Y.-H.; Li, C.-C.; Chou, Y.-H.; Huang, C.-H. Should Patients With Primary Upper Urinary Tract Cancer Receive Prophylactic Intravesical Chemotherapy After Nephroureterectomy? J. Urol. 2010, 183, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Novara, G.; De Marco, V.; Dalpiaz, O.; Galfano, A.; Bouygues, V.; Gardiman, M.; Martignoni, G.; Patard, J.J.; Artibani, W.; Ficarra, V. Independent predictors of contralateral metachronous upper urinary tract transitional cell carcinoma after nephroureterectomy: Multi-institutional dataset from three European centers. Int. J. Urol. 2009, 16, 187–191. [Google Scholar] [CrossRef]
- O’Brien, T.; Ray, E.; Singh, R.; Coker, B.; Beard, R. British Association of Urological Surgeons Section of Oncology. Prevention of bladder tumours after nephroureterectomy for primary upper urinary tract urothelial carcinoma: A prospective, multicentre, randomised clinical trial of a single postoperative intravesical dose of mitomycin C (the ODMIT-C Trial). Eur. Urol. 2011, 60, 703–710. [Google Scholar] [CrossRef]
- Sakamoto, N.; Naito, S.; Kumazawa, J.; Ariyoshi, A.; Osada, Y.; Omoto, T.; Fujisawa, Y.; Morita, I.; Yamashita, H. Prophylactic intravesical instillation of mitomycin C and cytosine arabinoside for prevention of recurrent bladder tumors following surgery for upper urinary tract tumors: A prospective randomized study. Int. J. Urol. 2001, 8, 212–216. [Google Scholar] [CrossRef]
- Ito, A.; Shintaku, I.; Satoh, M.; Ioritani, N.; Aizawa, M.; Tochigi, T.; Kawamura, S.; Aoki, H.; Numata, I.; Takeda, A.; et al. Prospective Randomized Phase II Trial of a Single Early Intravesical Instillation of Pirarubicin (THP) in the Prevention of Bladder Recurrence After Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma: The THP Monotherapy Study Group Trial. J. Clin. Oncol. 2013, 31, 1422–1427. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Babjuk, M.; Compérat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Böhle, A.; Van Rhijn, B.W.; Kaasinen, E.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Cell Carcinoma: 2015 Update. Eur. Urol. 2015, 68, 868–879. [Google Scholar] [CrossRef] [PubMed]
- Tonin, F.S.; Rotta, I.; Mendes, A.M.; Pontarolo, R.; Mendes, A.E.M. Network meta-analysis: A technique to gather evidence from direct and indirect comparisons. Pharm. Pract. 2017, 15, 943. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, D.M.; Dias, S.; Welton, N.J. Extending Treatment Networks in Health Technology Assessment: How Far Should We Go? Value Health 2015, 18, 673–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debray, T.P.; Schuit, E.; Efthimiou, O.; Reitsma, J.B.; Ioannidis, J.P.; Salanti, G.; Moons, K.G. An overview of methods for network meta-analysis using individual participant data: When do benefits arise? Stat. Methods Med. Res. 2016. [Google Scholar] [CrossRef]
- Tetzlaff, J.; Moher, D.; Liberati, A.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazumdar, M.; Begg, C.B. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Ades, A.E. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 2004, 23, 3105–3124. [Google Scholar] [CrossRef]
- Caldwell, D.M.; Ades, A.E.; Higgins, J.P.T.; Higgins, J. Simultaneous comparison of multiple treatments: Combining direct and indirect evidence. BMJ 2005, 331, 897–900. [Google Scholar] [CrossRef]
- Woods, B.S.; Hawkins, N.; A Scott, D. Network meta-analysis on the log-hazard scale, combining count and hazard ratio statistics accounting for multi-arm trials: A tutorial. BMC Med. Res. Methodol. 2010, 10, 54. [Google Scholar] [CrossRef]
- Dias, S.; Welton, N.J.; Caldwell, D.M.; Ades, A.E. Checking consistency in mixed treatment comparison meta-analysis. Stat. Med. 2010, 29, 932–944. [Google Scholar] [CrossRef]
- Takahashi, T.; Habuchi, T.; Kakehi, Y.; Mitsumori, K.; Akao, T.; Terachi, T.; Yoshida, O. Clonal and chronological genetic analysis of multifocal cancers of the bladder and upper urinary tract. Cancer Res. 1998, 58, 5835–5841. [Google Scholar]
- Habuchi, T. Metachronous multifocal development of urothelial cancers by intraluminal seeding. Lancet 1993, 342, 1087–1088. [Google Scholar] [CrossRef]
- Häfner, C.; Knuechel, R.; Stoehr, R.; Hartmann, A. Clonality of multifocal urothelial carcinomas: 10 years of molecular genetic studies. Int. J. Cancer 2002, 101, 1–6. [Google Scholar] [CrossRef]
- Takahashi, T.; Kakehi, Y.; Mitsumori, K.; Akao, T.; Terachi, T.; Kato, T.; Ogawa, O.; Habuchi, T. Distinct microsatellite alterations in upper urinary tract tumors and subsequent bladder tumors. J. Urol. 2001, 165, 672–677. [Google Scholar] [CrossRef]
- Jones, T.D.; Wang, M.; Eble, J.N.; MacLennan, G.T.; Lopez-Beltran, A.; Zhang, S.; Cocco, A.; Cheng, L. Molecular Evidence Supporting Field Effect in Urothelial Carcinogenesis. Clin. Cancer Res. 2005, 11, 6512–6519. [Google Scholar] [CrossRef]
- Wang, Y.; Lang, M.R.; Pin, C.L.; I Izawa, J. Comparison of the clonality of urothelial carcinoma developing in the upper urinary tract and those developing in the bladder. SpringerPlus 2013, 2, 412. [Google Scholar] [CrossRef] [Green Version]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Compérat, E.; Cowan, N.C.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Shariat, S.F.; et al. EAU Guidelines on Upper Urinary Tract Urothelial Carcinoma 2018. In European Association of Urology Guidleines, 2018th ed.; European Association of Urology Guidelines Office: Arnhem, The Netherlands, 2018. [Google Scholar]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef]
- Miyake, H.; Hara, I.; Kamidono, S.; Eto, H. Multifocal transitional cell carcinoma of the bladder and upper urinary tract: Molecular screening of clonal origin by characterizing cd44 alternative splicing patterns. J. Urol. 2004, 172, 1127–1129. [Google Scholar] [CrossRef]
- Power, N.E.; Izawa, J. Comparison of Guidelines on Non-Muscle Invasive Bladder Cancer (EAU, CUA, AUA, NCCN, NICE). Bladder Cancer 2016, 2, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Shen, Z.; Shen, T.; Wientjes, M.G.; O’Donnell, M.A.; Au, J.L.-S. Intravesical Treatments of Bladder Cancer: Review. Pharm. Res. 2008, 25, 1500–1510. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, T.; Sadzuka, Y.; Nagasawa, K.; Ohnishi, N.; Yokoyama, T.; Sonobe, T. Membrane Transport and Antitumor Activity of Pirarubicin, and Comparison with Those of Doxorubicin. Jpn. J. Cancer Res. 1999, 90, 775–780. [Google Scholar] [CrossRef]
- Mouridsen, H.T.; Alfthan, C.; Bastholt, L.; Bergh, J.; Dalmark, M.; Eksborg, S.; Hellsten, S.; Kjaer, M.; Peterson, C.; Skovsgard, T.; et al. Current status of epirubicin (Farmorubicin) in the treatment of solid tumours. Acta Oncol. 1990, 29, 257–285. [Google Scholar] [CrossRef]
- Azémar, M.-D.; Compérat, E.; Richard, F.; Cussenot, O.; Rouprêt, M. Bladder recurrence after surgery for upper urinary tract urothelial cell carcinoma: Frequency, risk factors, and surveillance. Urol. Oncol. Semin. Orig. Investig. 2011, 29, 130–136. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Country | Study Type | No. of Center | Recruitment Period | No. of Patients (Chemotherapy/Control) | Chemotherapy | Duration | |
|---|---|---|---|---|---|---|---|---|
| Sakamoto [10] | 2001 | Japan | Prospective | Multicenter | 1993–1996 | 25 (13/12) | MMC 20 mg and Ara-C 200 mg/30 mg | 2 weekly, 5 fortnightly, 21 monthly |
| Wu [7] | 2010 | Taiwan | Retrospective | Single | 1985–2007 | 196 (27/31/138) | Epirubicin 20 mg/20 mL, MMC 10 mg/20 mL | 6–8 weekly |
| O’Brien [9] | 2011 | UK | Prospective | Multicenter | 2000–2006 | 239 (120/119) | MMC 40 mg/40 mL | Single |
| Ito [11] | 2013 | Japan | Prospective | Multicenter | 2005–2008 | 72 (36/36) | Pirarubicin 30 mg/30 mL | Single |
| Median Age, Range (Years) | No. of Gender (M/F) | Tumor Stage (≤T1/T2/T3/T4/NA) | Tumor Grade (High/Low/NA) | Tumor Site (Pelvis/Ureter/Both/NA) | Median FU, Range (Months) | |
|---|---|---|---|---|---|---|
| Sakamoto [10] | NA, 55–85 | 16/9 | 9/16/0/0/0/ | 4/21/0 | NA | 45, 6–65 |
| Wu [7] | 65, 23–86 | 92/104 | 86/63/47/0/0 | 81/115/0 | 54/95/0/37 | 55.6, 12–182 |
| O’Brien [9] | NA, 36–90 | NA | 139/32/57/4/7 | 18/214/7 | NA | 12 |
| Ito [11] | NA | 43/29 | 39/8/25/0/0 | 39/33/0 | 40/28/3/0 | 24.9, 2.6–39.3 |
| All Studies | ||||||||||
| * Rank | A | B | C | D | E | F | ||||
| 1 | 46.0 | 4.9 | 2.3 | 1.2 | 45.6 | 0.0 | ||||
| 2 | 29.4 | 19.4 | 11.3 | 7.7 | 32.3 | 0.0 | ||||
| 3 | 9.7 | 32.9 | 25.7 | 22.0 | 9.7 | 0.2 | ||||
| 4 | 6.5 | 23.8 | 30.1 | 32.9 | 6.0 | 0.5 | ||||
| 5 | 5.6 | 16.9 | 27.3 | 33.7 | 4.7 | 11.7 | ||||
| 6 | 2.8 | 2.1 | 3.3 | 2.5 | 1.7 | 87.6 | ||||
| A. MMC 20 mg + Ara-C 200 mg (maintenance). B. MMC 10 mg (induction). C. Epirubicin 20 mg (induction). D. MMC 40 mg (single instillation). E. Pirarubicin 30 mg (single instillation). F. Control. | ||||||||||
| Prospective Controlled Trials | ||||||||||
| * Rank | A | B | C | D | ||||||
| 1 | 49.2 | 2.3 | 48.5 | 0.0 | ||||||
| 2 | 37.9 | 21.2 | 40.8 | 0.2 | ||||||
| 3 | 10.0 | 74.0 | 9.0 | 7.0 | ||||||
| 4 | 2.8 | 2.6 | 1.8 | 92.8 | ||||||
| A. MMC 20 mg + Ara-C 200mg (maintenance). B. MMC 40 mg (single instillation). C. Pirarubicin 30 mg (single instillation). D. Control. | ||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, S.H.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Choo, M.S.; Ku, J.H. Intravesical Chemotherapy after Radical Nephroureterectomy for Primary Upper Tract Urothelial Carcinoma: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2019, 8, 1059. https://doi.org/10.3390/jcm8071059
Yoo SH, Jeong CW, Kwak C, Kim HH, Choo MS, Ku JH. Intravesical Chemotherapy after Radical Nephroureterectomy for Primary Upper Tract Urothelial Carcinoma: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2019; 8(7):1059. https://doi.org/10.3390/jcm8071059
Chicago/Turabian StyleYoo, Sang Hyun, Chang Wook Jeong, Cheol Kwak, Hyeon Hoe Kim, Min Soo Choo, and Ja Hyeon Ku. 2019. "Intravesical Chemotherapy after Radical Nephroureterectomy for Primary Upper Tract Urothelial Carcinoma: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 8, no. 7: 1059. https://doi.org/10.3390/jcm8071059