
Larval Wound Therapy: Possibilities and Potential Limitations—A Literature Review
 , ,
, ,
Abstract
:1. Introduction
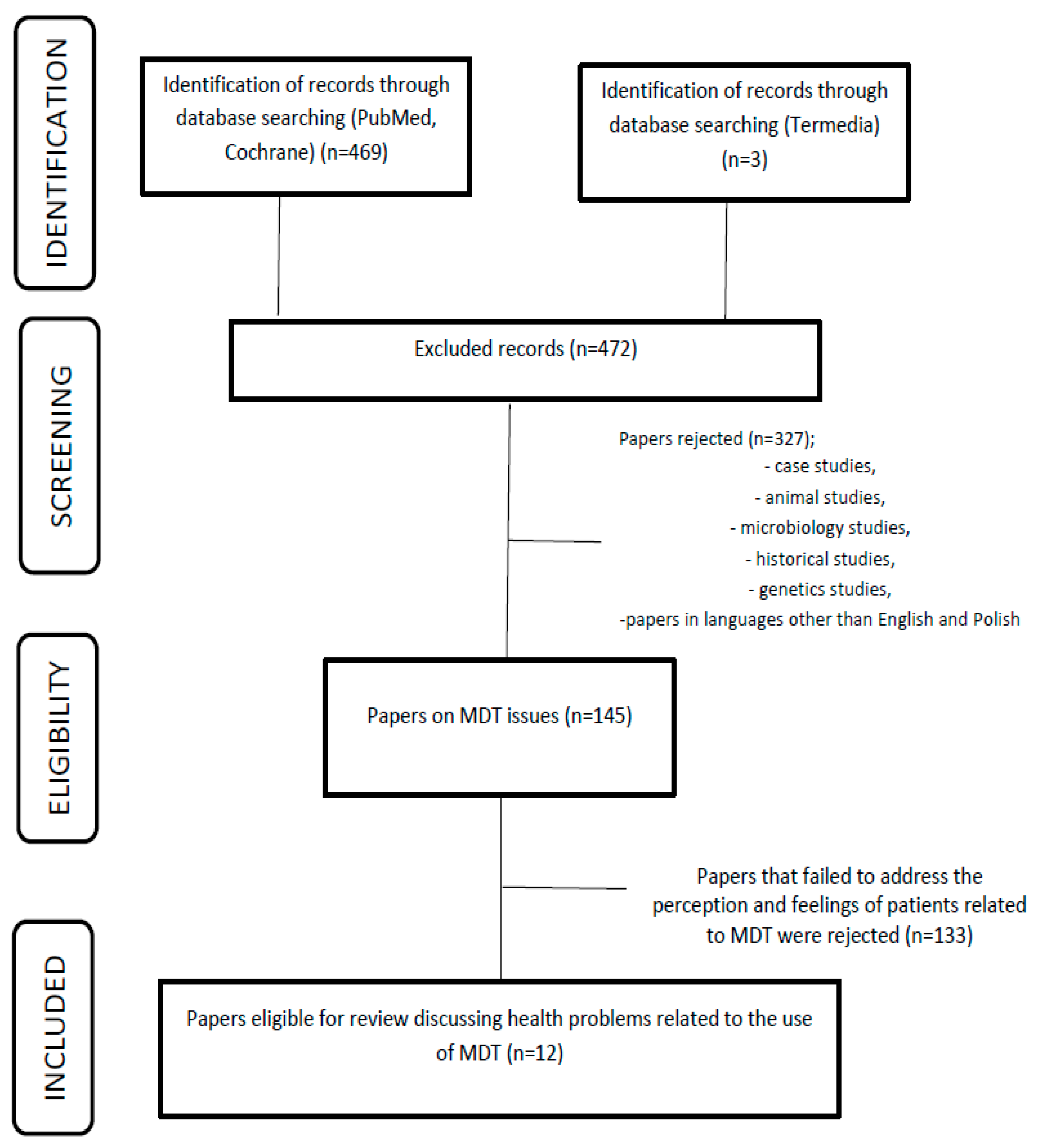
2. Materials and Methods
2.1. Patient-Centered Care (PCC) Model
2.2. Lucilia sericata Larvae and Topical Protocols for the Treatment of Difficult-to-Heal and Chronic Wounds
2.3. Health Problems in the Care of a Patient Qualified for MDT
2.4. Cost of Larval Therapy Application
2.5. Potential Problems Related to Larval Therapy Based on the Analyzed Literature

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Problem | Nursing Interventions | Justification Based on EBM |
|---|---|---|
| Increased wound exudate | Explanation of MDT’s action based on the secretion and excretion of digestive enzymes by the larvae, which liquefy the necrosis, resulting in characteristic brown exudate. Inspect the dressing at least every 24 h or more frequently if the exudate is high. Dress the wound with superabsorbent dressings. Dressing inspection should be performed by medical personnel or under their remote supervision, using systems to stay in contact with the person conducting the therapy. | Wound exudate is a physiological phenomenon that occurs at various stages of wound healing. Excess exudate is not desirable and can pose challenges when caring for a patient with a difficult-to-heal wound. Increased exudate and its composition may indicate an infection or contamination/bacterial infection [25,26]. The excessive exudate during MDT therapy is a result of the mechanism of action of maggots in the wound. Lucilia sericata larvae produce numerous secretions and excretions that exhibit antibacterial, antibiofilm, anti-inflammatory, and synergistic effects with selected antibiotics [21,26]. |
| Risk of wound bleeding | Selection of the larval application method should be based on the wound’s location, size, and etiology. For wounds located in the abdominal or head areas, it is advisable to use a closed dressing, commonly referred to as a ‘‘biobag’’ or ‘‘biosachet.’’ This precaution is necessary to minimize the potential risk of damaging major blood vessels. In cases where patients have known coagulation disorders or are taking anticoagulants, MDT therapy should be administered with careful consideration, taking into account the patient’s individual advantages and disadvantages. Depending on the patient’s clinical condition, inpatient therapy should be considered, and maintaining open communication with the treating physician is crucial. For outpatient care, it is recommended to change the dressing at least every 24 h, or more frequently if the dressing shows signs of bleeding. The dressing should be regularly inspected by medical staff, with an evaluation of the skin’s condition, the vitality of the larvae, and the patient’s psychophysical state. In cases of active bleeding, apply pressure without restricting the mobility of the larvae. It is important to adhere to the protocols outlined by the Polish Society for the Treatment of Wounds (PTLR) [6,12]. | For many years, it was believed that MDT could only be administered to distal body parts. However, the current literature indicates that MDT can also be used in large blood vessels. Patients should be well-prepared for therapy and closely monitored during the process [31]. Patients with deep, penetrating wounds who are on anticoagulants (NOACs or VKAs) are at the greatest risk of bleeding. Antithrombotic treatment does not absolutely contraindicate MDT, but it requires extreme caution [34]. |
| Itching and pain sensations within the wound | Qualification of the patient for therapy after a subjective and objective examination should involve assessing the patient’s suitability for treatment. Patients with a wound-related pain rating exceeding 4 points on the NRS scale and a history suggesting peripheral ischemia require special attention in pain management, particularly concerning hyperalgesia and allodynia. Pharmacotherapy decisions should be tailored to individual patient needs. In cases of hyperalgesia, consideration should be given to either reducing the duration of larvae presence in the wound to 24–48 h or decreasing the number of larvae applied, thus spreading wound debridement over multiple MDT sessions. It is crucial to establish contact with the healthcare provider responsible for the therapy to determine the evacuation of larvae from the wound. Furthermore, future research should focus on the treatment of peripheral arterial disease in patients with an ABPI of < 0.5, a condition often associated with pain, poor vascularization, and concurrent infection. | Contradictory opinions have been presented regarding areas of pain and the perceived effectiveness of therapy. Pain associated with larval activity in the wound can be safely and effectively controlled with the use of pharmacotherapy. In cases of severe symptoms, larvae should be removed from the wound [27,29,30]. In a retrospective study conducted by Mumcuoglu et al. involving 435 patients treated for a total of 723 wounds, it was observed that 38% of patients reported the onset or exacerbation of wound pain during the application of biosurgical dressings. In most cases, pain was managed with analgesics, and only in five cases the issues necessitated a discontinuation of therapy and removal of the dressing [35]. Individuals who are particularly sensitive, have low acceptance of MDT, or have ischemic wounds are more prone to increased pain and require customized preparation for MDT therapy [21,34]. Mudge et al. suggest that factors such as pain management, patient education, and treatment compliance are crucial for enhancing the effectiveness of maggot therapy [34]. |
| Risk of skin irritation around the wound | Increasing the patient’s knowledge about MDT therapy. Clarification of the maggot pattern in the wound, thus possibly increasing wound exudate. Before applying the larvae, the edges of the wound should be protected with a protective paste. Each time the dressing is inspected, the skin around the wound should be assessed, applying additional protective paste as needed. Skin assessment after evacuation of the larvae; in the event of damage, follow the TIMERS scheme when supplying. Proceeding in accordance with the algorithms proposed by PTLR [6]. | Excessive exudate related to the mechanism of action of Lucilia sericata larvae may determine the maceration of the skin around the wound. The presence of bacteria and proteolytic enzymes may cause micro-damage, which, in the course of contamination, may enlarge the wound area [21,30]. Protection of the wound edges is a key element of activities resulting from the concept of wound hygiene [30,35]. |
3. Discussion
4. Conclusions
Limitation
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jones, R.E.; Foster, D.S.; Longaker, M.T. Management of Chronic Wounds-2018. JAMA 2018, 320, 1481–1482. [Google Scholar] [CrossRef] [PubMed]
- Potempa, M.; Jonczyk, P.; Janerka, M.; Kucharzewski, M.; Krawczyk-Krupka, A. Determinants and epidemiology of chronic wounds. Leczenie Ran 2014, 11, 43–50. [Google Scholar] [CrossRef]
- Cwajda-Białasik, J.; Mościcka, P.; Szewczyk, M. Selected methods of treatment of chronic wounds. Pielęgniarstwo Chir. I Angiol. (Surg. Vasc. Nurs.) 2019, 13, 1–11. [Google Scholar]
- Atkin, L.; Bućko, Z.; Conde Montero, E.; Cutting, K.; Moffatt, C.; Probst, A.; Romanelli, M.; Schultz, G.S.; Tettelbach, W. Implementing TIMERS: The race against hard-to-heal wounds. J. Wound Care 2019, 23 (Suppl. S3a), S1–S50. [Google Scholar] [CrossRef]
- Murphy, C.; Atkin, L.; Dissemond, J.; Hurlow, J.; Tan, Y.K.; Apelqvist, J.; James, G.; Salles, N.; Wu, J.; Tachi, M.; et al. Defying hard-to-heal wounds with an early antibiofilm intervention strategy: ‘wound hygiene’. J. Wound Care 2019, 28, 818–822. [Google Scholar] [CrossRef]
- Szewczyk, M.; Cwajda-Białasik, J.; Mościcka, P.; Cierzniakowska, K.; Bazaliński, D.; Jawień, A.; Spannbauer, A.; Polak, A.; Sopata, M.; Kozłowska, E.; et al. Treatment of pressure ulcers–recommendations of the Polish Wound Management Association. Part II. Leczenie Ran 2020, 17, 151–184. [Google Scholar] [CrossRef]
- Moya-López, J.; Costela-Ruiz, V.; García-Recio, E.; Sherman, R.A.; De Luna-Bertos, E. Advantages of Maggot Debridement Therapy for Chronic Wounds: A Bibliographic Review. Adv. Ski. Wound Care 2020, 33, 515–525. [Google Scholar] [CrossRef]
- Bazaliński, D.; Kózka, M.; Karnas, M.; Więch, P. Effectiveness of Chronic Wound Debridement with the Use of Larvae of Lucilia Sericata. J. Clin. Med. 2019, 8, 1845. [Google Scholar] [CrossRef]
- Sherman, R.A.; Pechter, E.A. Maggot therapy: A review of the therapeutic applications of fly larvae in human medicine, especially for treating osteomyelitis. Med. Vet. Entomol. 1988, 2, 225–230. [Google Scholar] [CrossRef]
- Sherman, R.A. Mechanisms of maggot-induced wound healing: What do we know, and where do we go from here? Evid. Based Complement. Altern. Med. 2014, 2014, 592419. [Google Scholar] [CrossRef]
- von Beckerath, O.; Kanya, S.; Gäbel, G.; Kröger, K.; Juntermanns, B. Use of maggot debridement therapy in hospitalised patients in Germany. Int. Wound J. 2020, 17, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Mrozikiewicz-Rakowska, B.; Tusiński, M.; Lipiński, P.; Bazaliński, D.; Dynarska, J.; Czwakiel, L.; Zymon, A.; Mospan, B.; Malinowska, K.; Sopata, M.; et al. Statement of the Polish Wound Management Association on larval therapy in wound management. Leczenie Ran 2023, 20, 89–95. [Google Scholar] [CrossRef]
- Mohd Zubir, M.Z.; Holloway, S.; Mohd Noor, N. Maggot Therapy in Wound Healing: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6103. [Google Scholar] [CrossRef]
- King, C. Changing attitudes toward maggot debridement therapy in wound treatment: A review and discussion. J. Wound Care 2020, 29 (Suppl. S2c), S28–S34. [Google Scholar] [CrossRef] [PubMed]
- Nigam, Y.; Morgan, C. Does maggot therapy promote wound healing? The clinical and cellular evidence. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Malone, M.; Bjarnsholt, T.; McBain, A.J.; James, G.A.; Stoodley, P.; Leaper, D.; Tachi, M.; Schultz, G.; Swanson, T.; Wolcott, R.D. The prevalence of biofilms in chronic wounds: A systematic review and meta-analysis of published data. J. Wound Care 2017, 26, 20–25. [Google Scholar] [CrossRef]
- Becerikli, M.; Wallner, C.; Dadras, M.; Wagner, J.M.; Dittfeld, S.; Jettkant, B.; Gestmann, F.; Mehlhorn, H.; Mehlhorn-Diehl, T.; Lehnhardt, M.; et al. Maggot Extract Interrupts Bacterial Biofilm Formation and Maturation in Combination with Antibiotics by Reducing the Expression of Virulence Genes. Life 2022, 12, 237. [Google Scholar] [CrossRef]
- Malekian, A.; Esmaeeli Djavid, G.; Akbarzadeh, K.; Soltandallal, M.; Rassi, Y.; Rafinejad, J.; Rahimi Foroushani, A.; Farhoud, A.; Bakhtiary, R.; Totonchi, M. Efficacy of Maggot Therapy on Staphylococcus aureus and Pseudomonas aeruginosa in Diabetic Foot Ulcers: A Randomized Controlled Trial. J. Wound Ostomy Cont. Nurs. 2019, 46, 25–29. [Google Scholar] [CrossRef]
- Blueman, D.; Bousfield, C. The use of larval therapy to reduce the bacterial load in chronic wounds. J. Wound Care 2012, 21, 244–253. [Google Scholar] [CrossRef]
- Cazander, G.; Pritchard, D.I.; Nigam, Y.; Jung, W.; Nibbering, P.H. Multiple actions of Lucilia sericata larvae in hard-to-heal wounds: Larval secretions contain molecules that accelerate wound healing, reduce chronic inflammation and inhibit bacterial infection. Bioessays 2013, 35, 1083–1092. [Google Scholar] [CrossRef]
- Opletalová, K.; Blaizot, X.; Mourgeon, B.; Chêne, Y.; Creveuil, C.; Combemale, P.; Laplaud, A.L.; Sohyer-Lebreuilly, I.; Dompmartin, A. Maggot therapy for wound debridement: A randomized multicenter trial. Arch. Dermatol. 2012, 148, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Gazi, U.; Taylan-Ozkan, A.; Mumcuoglu, K.Y. The effect of Lucilia sericata larval excretion/secretion (ES) products on cellular responses in wound healing. Med. Vet. Entomol. 2021, 35, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Giap, T.T.; Lee, M.; Jeong, H.; Jeong, M.; Go, Y. Patient- and family-centered care interventions for improving the quality of health care: A review of systematic reviews. Int. J. Nurs. Stud. 2018, 87, 69–83. [Google Scholar] [CrossRef] [PubMed]
- den Boer, J.; Nieboer, A.P.; Cramm, J.M. A cross-sectional study investigating patient-centred care, co-creation of care, well-being and job satisfaction among nurses. J. Nurs. Manag. 2017, 25, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Pajarillo, C.; Sherman, R.A.; Sheridan, R.; Kazis, L.E. Health professionals’ perceptions of maggot debridement therapy. J. Wound Care. 2021, 30 (Suppl. S9a), VIIi–VIIxi. [Google Scholar] [CrossRef]
- Dumville, J.C.; Worthy, G.; Soares, M.O.; Bland, J.M.; Cullum, N.; Dowson, C.; Iglesias, C.; McCaughan, D.; Mitchell, J.L.; Nelson, E.A.; et al. VenUS II: A randomised controlled trial of larval therapy in the management of leg ulcers. Health Technol. Assess. 2009, 13, 1–182, iii–iv. [Google Scholar] [CrossRef]
- McCaughan, D.; Cullum, N.; Dumville, J. VenUS II Team. Patients’ perceptions and experiences of venous leg ulceration and their attitudes to larval therapy: An in-depth qualitative study. Health Expect. 2015, 18, 527–541. [Google Scholar] [CrossRef]
- Morozov, A.M.; Sherman, R.A. Survey of patients of the Tver region of Russia regarding maggots and maggot therapy. Int. Wound J. 2019, 16, 401–405. [Google Scholar] [CrossRef]
- Spilsbury, K.; Cullum, N.; Dumville, J.; O’Meara, S.; Petherick, E.; Thompson, C. Exploring patient perceptions of larval therapy as a potential treatment for venous leg ulceration. Health Expect. 2008, 11, 148–159. [Google Scholar] [CrossRef]
- Turkmen, A.; Graham, K.; McGrouther, D.A. Therapeutic applications of the larvae for wound debridement. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 184–188. [Google Scholar] [CrossRef]
- Mita, J.P.; Bazaliński, D.; Sztembis, R.; Kuberka, I.; Więch, P. Perceived stress and readiness to undertake biodebridement in the group of nurses undertaking prevention and treatment of chronic wounds. Front. Public Health 2022, 10, 1090677. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, R.C.; Williams, S.; Brown, A.; Humphreys, I.; Clifford, R.; Nigam, Y. Evaluating nursing opinion and perception of maggot therapy for hard-to-heal wound management. J. Wound Care 2022, 31, 846–863. [Google Scholar] [CrossRef] [PubMed]
- Nigam, Y.; Williams, S.; Humphreys, I.; Clifford, R.; Brown, A. An exploration of public perceptions and attitudes towards maggot therapy. J. Wound Care 2022, 31, 756–770. [Google Scholar] [CrossRef] [PubMed]
- Mudge, E.; Price, P.; Walkley, N.; Harding, K.G. A randomized controlled trial of larval therapy for the debridement of leg ulcers: Results of a multicenter, randomized, controlled, open, observer blind, parallel group study. Wound Repair Regen. 2014, 22, 43–51. [Google Scholar] [CrossRef]
- Mumcuoglu, K.Y.; Davidson, E.; Avidan, A.; Gilead, L. Pain related to maggot debridement therapy. J. Wound Care 2012, 21, 400, 402, 404–405. [Google Scholar] [CrossRef]
- van der Meer, L.; Nieboer, A.P.; Finkenflügel, H.; Cramm, J.M. The importance of person-centred care and co-creation of care for the well-being and job satisfaction of professionals working with people with intellectual disabilities. Scand. J. Caring Sci. 2018, 32, 76–81. [Google Scholar] [CrossRef]
- Sherman, R.A. Maggot therapy takes us back to the future of wound care: New and improved maggot therapy for the 21st century. J. Diabetes Sci. Technol. 2009, 3, 336–344. [Google Scholar] [CrossRef]
- Siavash, M.; Najjarnezhad, A.; Mohseni, N.; Abtahi, S.M.; Karimy, A.; Sabzevari, M.H. Efficacy of Maggot Debridement Therapy on Refractory Atypical Diabetic Foot Ulcers: An Open-Label Study. Int. J. Low. Extrem. Wounds 2021, 20, 315–320. [Google Scholar] [CrossRef]
- Wilson, M.R.; Nigam, Y.; Knight, J.; Pritchard, D.I. What is the optimal treatment time for larval therapy? A study on incubation time and tissue debridement by bagged maggots of the greenbottle fly, Lucilia sericata. Int. Wound J. 2019, 16, 219–225. [Google Scholar] [CrossRef]
- Sun, X.; Jiang, K.; Chen, J.; Wu, L.; Lu, H.; Wang, A.; Wang, J. A systematic review of maggot debridement therapy for chronically infected wounds and ulcers. Int. J. Infect. Dis. 2014, 25, 32–37. [Google Scholar] [CrossRef]
- Nord, C.L.; Dalmaijer, E.S.; Armstrong, T.; Baker, K.; Dalgleish, T. A Causal Role for Gastric Rhythm in Human Disgust Avoidance. Curr. Biol. 2021, 31, 629–634.e3. [Google Scholar] [CrossRef] [PubMed]
- Entwistle, V.; Williams, B. Health literacy: The need to consider images as well as words. Health Expect 2008, 11, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Bazaliński, D.; Karnas, M.; Wołkowicz, M.; Kózka, M.; Więch, P. Zastosowanie larw Lucilia sericata w oczyszczaniu ran przewlekłych-studium trzech przypadków [Application of Lucilia sericata larvae in the debridement of chronic wounds-a study of three cases]. Leczenie Ran 2018, 15, 105–111. [Google Scholar] [CrossRef]
- Soares, M.O.; Iglesias, C.P.; Bland, J.M.; Cullum, N.; Dumville, J.C.; Nelson, E.A.; Torgerson, D.J.; Worthy, G.; VenUS II on behalf of the VenUS II team. Cost effectiveness analysis of larval therapy for leg ulcers. BMJ 2009, 338, b825. [Google Scholar] [CrossRef] [PubMed]
- Wayman, J.; Nirojogi, V.; Walker, A.; Sowinski, A.; A Walker, M. The cost effectiveness of larval therapy in venous ulcers. J. Tissue Viability 2000, 10, 91–94. [Google Scholar] [CrossRef]
- Mirabzadeh, A.; Ladani, M.J.; Imani, B.; Rosen, S.A.; Sherman, R.A. Maggot therapy for wound care in Iran: A case series of the first 28 patients. J. Wound Care 2017, 26, 137–143. [Google Scholar] [CrossRef]
- Malisiewicz, A.; Zymon, A.; Bazaliński, D. Problems associated with local treatment of the sternum wound–a literature review. Pielęgniarstwo Chir. I Angiol. (Surg. Vasc. Nurs.) 2023, 17, 6–17. [Google Scholar]
- Nasoori, A.; Hoomand, R. Maggot debridement therapy for an electrical burn injury with instructions for the use of Lucilia sericata larvae. J. Wound Care 2017, 26, 734–741. [Google Scholar] [CrossRef]
- Lin, Y.; Amin, M.; Donnelly, A.; Amar, S. Maggot Debridement Therapy of a Leg Wound from Kaposi’s Sarcoma: A Case Report. J. Glob. Oncol. 2015, 1, 92–98. [Google Scholar] [CrossRef]
- Steenvoorde, P.; van Doorn, L.P. Maggot Debridement Therapy: Serious bleeding can occur: Report of a case. J. Wound Ostomy Cont. Nurs. 2008, 35, 412–414. [Google Scholar] [CrossRef]
- Bazaliński, D.; Przybek-Mita, J.; Lisowicz, K.; Skórka, M.; Więch, P. Defensins of Lucilia sericata Larvae and Their Influence on Wound Repair Processes in Practical Assessment-A Study of Three Cases. Int. J. Environ. Res. Public Health 2023, 20, 5357. [Google Scholar] [CrossRef] [PubMed]
- Jafari, A.; Hosseini, S.V.; Hemmat, H.J.; Khazraei, H. Lucillia Sericata larval therapy in the treatment of diabetic chronic wounds. J. Diabetes Metab. Disord. 2022, 21, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Szczepanowski, Z.; Grabarek, B.O.; Boroń, D.; Tukiendorf, A.; Kulik-Parobczy, I.; Miszczyk, L. Microbiological effects in patients with leg ulcers and diabetic foot treated with Lucilia sericata larvae. Int. Wound J. 2022, 19, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Kilańska, D.; Grabowska, H. ICNP®—Podstawowe rozwiązania, strategia, praktyka pielegniarska (zarządzanie wiedzą), edukacja i miejsce w systemie informatycznym ochrony zdrowia [ICNP®-basic solutions, strategy, nursing practice (knowledge management), education, and place in the healthcare informatics system]. In International Classification of Nursing Practice ICNP® in Nursing Practice; Wydawnictwo Lekarskie PZWL: Warszawa, Poland, 2014; pp. 49–97. (In Polish) [Google Scholar]
- Ślusarska, B. Implementacje praktyczne wybranych klasyfikacji diagnoz i interwencji pielęgniarskich dla pielęgniarstwa polskiego. Practical implementations of selected classifications of diagnoses and nursing interventions for Polish nursing. Public Health Manag. 2016, 14, 11–22. (In Polish) [Google Scholar]
- Gieroń, M.; Słowik-Rylska, M.; Kręcisz, B. Effectiveness of maggot debridement therapy in treating chronic wounds–review of current literature. Med. Stud. Stud. Med. 2018, 34, 325–331. [Google Scholar] [CrossRef]
- Bazaliński, D. Efficacy of Biological Therapy Using Lucilia sericata Larvae in the Treatment of Chronic Wounds in Patients in Long-Term and Palliative Care; University of Rzeszów: Rzeszów, Poland, 2019; Available online: https://wydawnictwo.ur.edu.pl/produkt/skutecznosc-terapii-biologicznej-z-wykorzystaniem-larw-lucilia-sericata-w-leczeniu-ran-przewleklych-u-chorych-w-opiece-dlugoterminowej-i-paliatywnej/ (accessed on 7 October 2023). (In Polish)
- Rafter, L. A patient’s perceptions of using larval therapy. Wounds UK 2010, 6, 130–132. [Google Scholar]
- Armstrong, D.G.; Rowe, V.L.; D’Huyvetter, K.; Sherman, R.A. Telehealth-guided home-based maggot debridement therapy for chronic complex wounds: Peri- and post-pandemic potential. Int. Wound J. 2020, 17, 1490–1495. [Google Scholar] [CrossRef]
- Abela, G. Benefits of maggot debridement therapy on leg ulcers: A literature review. Br. J. Community Nurs. 2017, 22 (Suppl. S6), S14–S19. [Google Scholar] [CrossRef]
- Kitching, M. Patients’ perceptions and experiences of larval therapy. J Wound Care. 2004, 13, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.; Campbell, D. A retrospective, quality improvement review of maggot debridement therapy outcomes in a foot and leg ulcer clinic. Ostomy Wound Manag. 2014, 60, 16–25. [Google Scholar]
- Sun, X.; Chen, J.; Zhang, J.; Wang, W.; Sun, J.; Wang, A. Maggot debridement therapy promotes diabetic foot wound healing by up-regulating endothelial cell activity. J. Diabetes Complicat. 2016, 30, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, P.; McCardle, J.; Ricci, E.; Stang, D.; Vig, S. Appropriate use of larval debridement therapy in diabetic foot management: Consensus recommendations. Diabet. Foot J. 2015, 18, 37–42. [Google Scholar]
- Sherman, R.A. Maggot versus conservative debridement therapy for the treatment of pressure ulcers. Wound Repair. Regen. 2002, 10, 208–214. [Google Scholar] [CrossRef]
- Shi, E.; Shofler, D. Maggot debridement therapy: A systematic review. Br. J. Community Nurs. 2014, 19 (Suppl. S12), S6–S13. [Google Scholar] [CrossRef] [PubMed]
- Zarchi, K.; Jemec, G.B. The efficacy of maggot debridement therapy--a review of comparative clinical trials. Int. Wound J. 2012, 9, 469–477. [Google Scholar] [CrossRef]
- Mumcuoglu, K.Y. Clinical applications for maggots in wound care. Am. J. Clin. Dermatol. 2001, 2, 219–227. [Google Scholar] [CrossRef]
- Lipiński, P.; Trzciński, R.; Dziki, Ł.; Mik, M. Phantom pain as an adverse effect after maggot (Lucilia sericata) debridement therapy: A case study. J. Wound Care 2020, 29, 303–305. [Google Scholar] [CrossRef]
- Fleischman, W.; Grassberger, M.; Sherman, R. Maggot Therapy—A Handbook of Maggot-Assisted Wound Healing; Georg Thieme Verlag: Stuttgart, Germany, 2004; ISBN 9781588902320. [Google Scholar]
- McNichol, L.; Bliss, D.Z.; Gray, M. Moisture-Associated Skin Damage: Expanding Practice Based on the Newest ICD-10-CM Codes for Irritant Contact Dermatitis Associated with Digestive Secretions and Fecal or Urinary Effluent from an Abdominal Stoma or Enterocutaneous Fistula. J. Wound Ostomy Cont. Nurs. 2022, 49, 235–239. [Google Scholar] [CrossRef]
- White, R.J.; Cutting, K.F. Interventions to avoid maceration of the skin and wound bed. Br. J. Nurs. 2003, 12, 1186–1201. [Google Scholar] [CrossRef]
- Brown, A.; Horobin, A.; Blount, D.G.; Hill, P.J.; English, J.; Rich, A.; Williams, P.M.; Pritchard, D.I. Blow fly Lucilia sericata nuclease digests DNA associated with wound slough/eschar and with Pseudomonas aeruginosa biofilm. Med. Vet. Entomol. 2012, 26, 432–439. [Google Scholar] [CrossRef]




| Author | Type of Work | Participants | Conclusion |
|---|---|---|---|
| Opletova et al. (2012) [21] | Randomized controlled trial | 105 patients with lower leg ulcers ABPI ≥ 0.8, divided into two groups. | MDT showed no significant benefit on day 15 compared to conventional treatment. Debridement with MDT was much faster and took place in the first week of treatment. Another type of dressing should be used after 2 or 3 applications of MDT. Pain scores were similar and low in both groups. |
| Parajilio et al. (2021) [25] | Original article | Qualitative study via information provided by the Biotherapeutics, Education, and Research Foundation (BTER) website. Structured telephone interviews were conducted with nine healthcare professionals who use MDT. | Specifically, the ‘yuck’ factor and the perception of MDT as an ‘ancient’ modality contributed to MDT stigma; in addition, a lack of outpatient insurance coverage deterred MDT use. |
| Dumville et al. (2009) [26] | Randomized controlled trial | 267 patients with mixed lower leg ulcers ABPI ≥ 0.6, divided into two groups. | Larval therapy did not improve the healing time of the lower leg ulcers or reduce the number of bacteria compared to the hydrogel, but it significantly shortened the time required for wound cleansing. An increase in pain sensations during MDT was noted. |
| McCaughan et al. (2015) [27] | Randomized controlled trial | 18 people (12 men, 6 women) aged from 29 to 93 years (median age 64) with at least one venous leg ulcer. Most were willing to try the “worms” (larvae) and were able to overcome the feeling of disgust because they wanted to heal their wounds. | Patients may hold unrealistic expectations that larval therapy will effect a longed-for cure for their leg ulcer(s), but an absence of healing may lead to feelings of disappointment or despair. |
| Morozow et al. 2019 [28] | Original article | A total of 576 people were enrolled: 414 (72%) women and 162 (28%) men. Patients’ perception of the sight of maggots and larval therapy were assessed. | Maggots are repulsive to many people, and this may influence the acceptance of larval therapy. |
| Spilsbury et al. (2008) [29] | Original article | The preferences of 35 patients regarding the acceptance of two forms of larval therapy (“in biobags” and “loose”) were assessed. | Eliciting patient preferences and increasing their involvement in treatment decisions are important elements for improving quality and achieving better health outcomes. These findings have implications for practitioners offering larval therapy as a treatment option and for the feasibility of clinical trials. |
| Turkmen et al. (2010) [30] | Original article | Larval therapy was implemented in 34 patients with chronic wounds; in 29 (85%), satisfactory wound cleansing was observed. In the remaining five patients, failures occurred due to insufficient dressing sealing in two patients (6%), death of larvae in two patients (6%), and method intolerance in one patient (3%). | Larval therapy should be considered as a therapeutic option for the management of certain challenging wounds. |
| Przybek-Mita et al. (2022) [31] | Original article | The study group consisted of 290 nurses specialized in chronic wounds undergoing training out of an entire group of 1136 individuals participating in training courses organized in Poland in 2020–2021. | The level of perceived stress may influence decisions related to the use of biological therapy. The higher the level of stress, the lower the readiness to undertake MDT. |
| Hopkins et al. (2022) [32] | Original article | The first stage of this mixed-methods study was a focus group organized to discuss MDT and the opinions of specialist nurses. An anonymous online survey was then launched via Nursing Times and distributed on social media to all nurses. Finally, in-depth interviews were conducted with specialist and general nurses. | Nurses specializing in wound care choose MDT more often than nurses without experience in this field. Attention was paid to the need for nurse training to solve problems with acceptance and willingness to use this method in practice. |
| Nigam et al. (2022) [33] | Original article | In a group of 412 respondents regarding the acceptance of larval therapy, only 36% of the respondents agreed to accept larval therapy as a first-line treatment in the case of a hypothetical painful wound. | Study participants expressed concerns and fears related to the use of larval therapy. Positive associations were reported between knowledge scores and potential acceptance of larvae therapy, suggesting that information dissemination and education may be an important factor influencing public perception and acceptance of the method. |
| Mudge et al. (2014) [34] | Randomized controlled trial | 88 patients with venous and mixed ulcers ABPI ≥ 0.5 divided into two groups. | Larval therapy cleansed ulcerative wounds faster than hydrogel. Patients in the larvae group experienced more discomfort and pain during wound cleansing compared to the hydrogel group. |
| Mumcuoglu et al. (2012) [35] | Original article | Of the 435 patients who underwent MTD, 165 (38%) reported increased pain. In five patients, treatment had to be discontinued due to uncontrolled pain. | A large percentage of patients treated with MDT reported increasing pain with each day of therapy. It is necessary to introduce painkillers when cleaning with larvae. |
| Health Problem | Nursing Interventions | Justification Based on EBM |
|---|---|---|
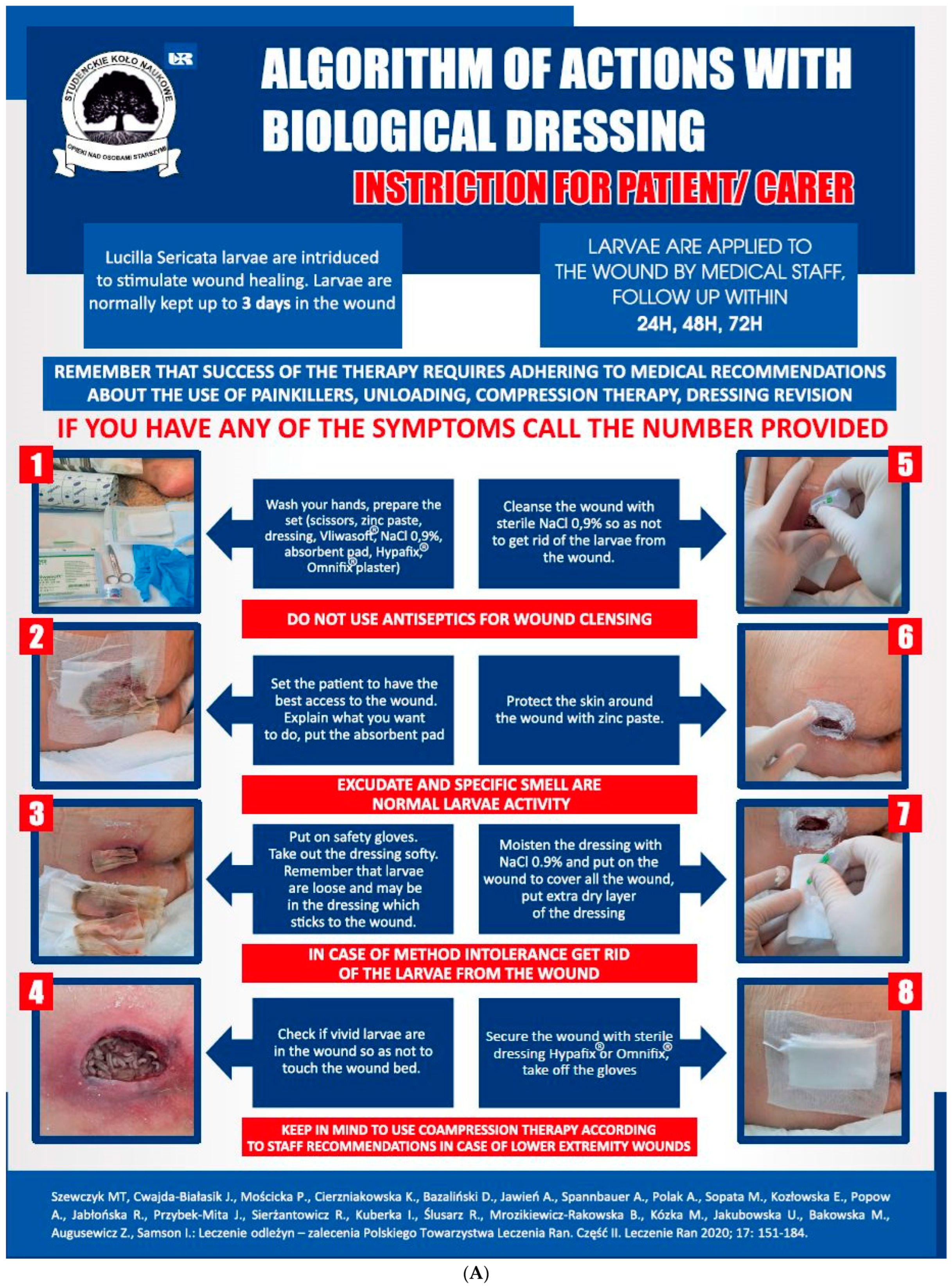
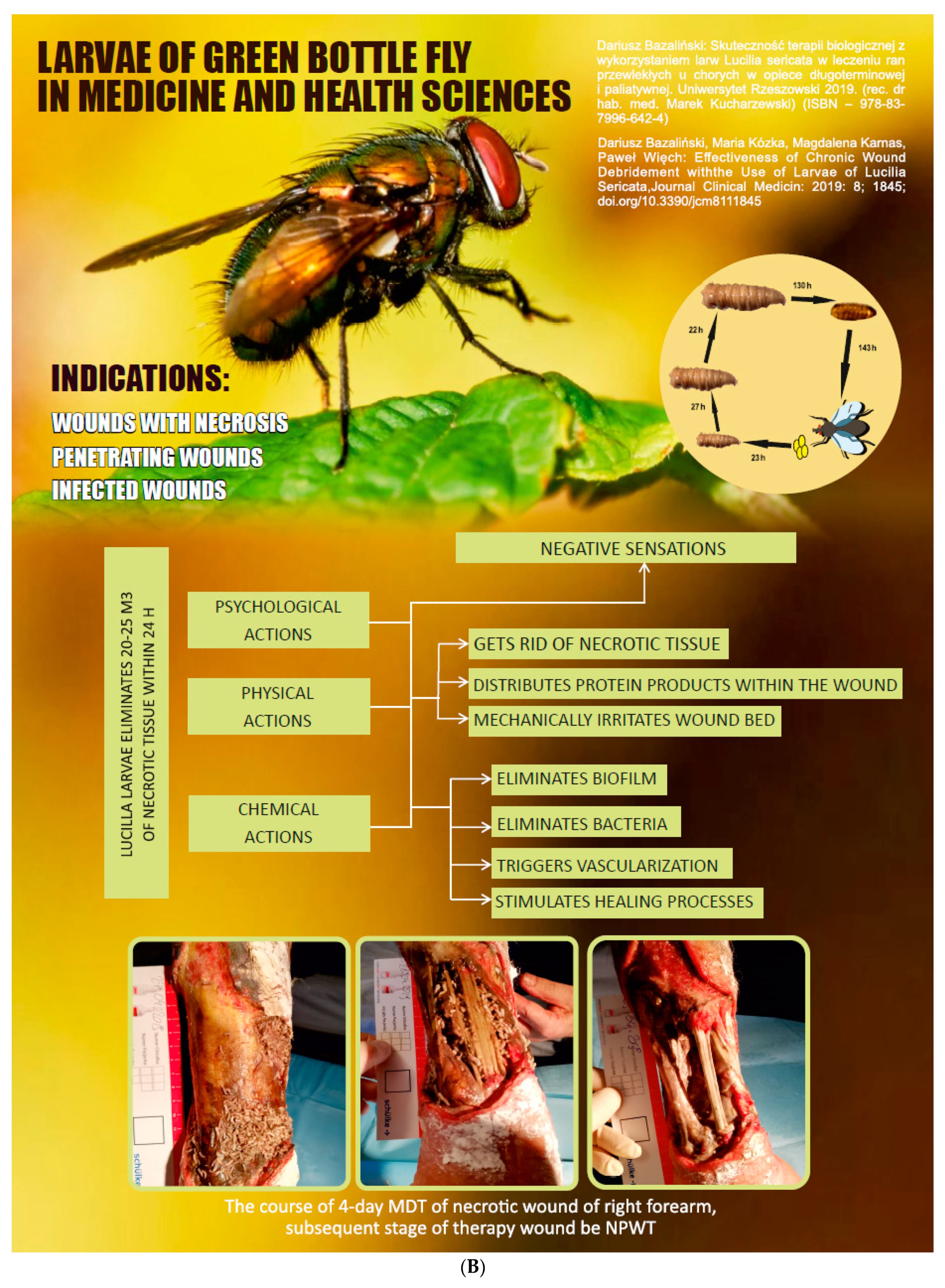
| Repulsion and disgust caused by the sight of larvae wriggling in the wound | Increase patient knowledge about Medical Maggot Therapy (MDT) to reduce negative feelings. Reinforce positive health behaviors and focus education on the positive effects of rapid wound debridement with minimal discomfort. In order to gauge patient acceptance, it is recommended to use a questionnaire assessment, such as the Perceived Stress Scale (PSS10) to assess stress levels and an MDT acceptance assessment. Explain the mechanism of action of the larvae in the wound and the potential use of a “biobag” to reduce visual sensations. Implement procedures to limit the view of maggots in the wound, such as using posters (see Figure 2), brochures, and instructional videos. Facilitate direct communication with the healthcare provider who administers the therapy to reduce patient anxiety. After completing the therapy, encourage patients to assess the effects of wound debridement. | Patients who consented to the MDT application re-evaluated their initial expectations compared to the post-treatment period. Positive opinions about the therapy persisted; small larvae in the first growth phase did not frighten the patients [25,26,27]. MDT experiences and interpersonal relationships influenced the perception and interactions between the patients and other individuals, including medical staff, friends, family, and fellow patients. The longer the problems with wound healing lasted, the higher the acceptance of larval therapy [28]. |
| Anxiety about the larvae leaving the wound | Explanation of application methods, including both closed and open techniques, and highlighting the potential benefits of each method, can help to address anxiety about the larvae leaving the wound. Ensuring continuous contact with a dedicated healthcare professional responsible for the treatment is essential. To further mitigate concerns, sealing the wound with an appropriate dressing and having medical staff regularly inspect the dressing for patients who may not be self-reliant, or implementing remote supervision using audio-visual techniques, are all recommended strategies. | Anxiety related to the fear of larvae leaving the dressing was discussed by Turkmen [30] and Sherman and Morozov [28]. Nursing staff’s uncertainty contributes to patients’ apprehension regarding the adoption of an unfamiliar therapy. Building confidence in their actions instills a sense of security in patients, reducing their anxieties both before and during MDT therapy [28]. Encouraging patient preferences and enhancing their involvement in treatment decisions are crucial components of quality improvement and better health outcomes. These findings hold significance for practitioners offering larval therapy [25,27,28]. Medical staff may also experience anxiety, especially concerning the appearance and movement of larvae, potentially leading to their hesitancy in using this method [31]. |
| Lack of motivation to engage in health-related actions and resistance to treatment | If possible, assess the need for support, motivation, and self-care capabilities. In cases of the absence or limited functional resources, consider long-term care options and enhance collaboration with primary healthcare providers and caregivers. | Older age, loneliness, and limited self-care can lead to a decrease in or lack of motivation for health-related activities [32]. People subjected to larval therapy whose wounds did not heal for a long time showed a positive attitude and trust in wound healing [29]. In Nigam et al.’s study, 36% of the participants agreed that they would accept larval therapy as a first-line treatment for a hypothetical painful wound, although this number increased with wound severity. The most dominant concerns regarding larval therapy were the sensations and feelings of disgust associated with the therapy [33]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazaliński, D.; Przybek-Mita, J.; Pytlak, K.; Kardyś, D.; Bazaliński, A.; Kucharzewski, M.; Więch, P. Larval Wound Therapy: Possibilities and Potential Limitations—A Literature Review. J. Clin. Med. 2023, 12, 6862. https://doi.org/10.3390/jcm12216862
Bazaliński D, Przybek-Mita J, Pytlak K, Kardyś D, Bazaliński A, Kucharzewski M, Więch P. Larval Wound Therapy: Possibilities and Potential Limitations—A Literature Review. Journal of Clinical Medicine. 2023; 12(21):6862. https://doi.org/10.3390/jcm12216862
Chicago/Turabian StyleBazaliński, Dariusz, Joanna Przybek-Mita, Kamila Pytlak, Daria Kardyś, Adrian Bazaliński, Marek Kucharzewski, and Paweł Więch. 2023. "Larval Wound Therapy: Possibilities and Potential Limitations—A Literature Review" Journal of Clinical Medicine 12, no. 21: 6862. https://doi.org/10.3390/jcm12216862