
Implant Site Changes in Three Different Clinical Approaches: Orthodontic Extrusion, Regenerative Surgery and Spontaneous Healing after Extraction: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
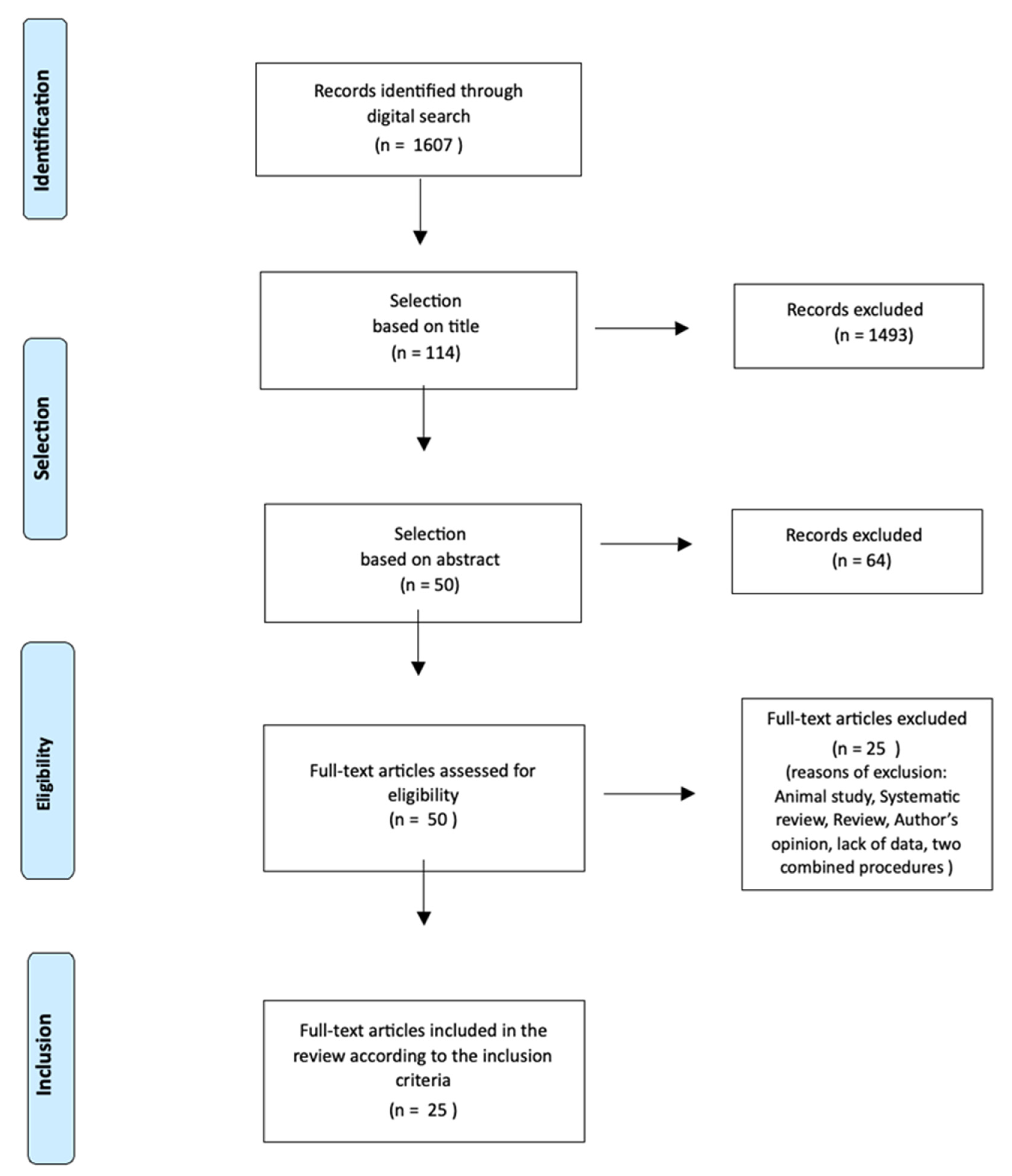
2.1. Search Strategy and Study Selection
2.2. Inclusion Criteria
- Human studies;
- English language;
- Type of studies: case reports, case series, randomized controlled trials, prospective studies;
- Population (P): subjects needing ridge regenerative procedures prior to implant rehabilitation;
- Intervention (I): implant site development through orthodontic extrusion or regenerative surgery (ridge splitting, guided bone regeneration, distraction osteogenesis, bone and soft tissue grafting);
- Control (C): spontaneous bone healing after tooth loss and delayed implant placement;
- Outcome (O): primary outcome was changes in the amount of bone and soft tissue in the implant site.
2.3. Secondary Outcome
- Esthetic outcome;
- Implant survival rate;
- Complications.
2.4. Data Extraction
- Type of study;
- Year;
- Author;
- Patient age;
- Patient gender;
- Health conditions and smoking habit;
- Treated teeth;
- Reason for treatment need;
- Type of treatment (orthodontic, surgical, absent);
- Orthodontic technique: type of appliance, extrusion method, the intensity of the force, anchorage, extrusion ratio (mm/month), duration of the orthodontic treatment (months), frequency of follow-up (weeks), post-orthodontic retention (months), amount of tooth extrusion (mm), amount of bone augmentation (mm), amount of soft tissue augmentation (mm), efficacy of orthodontic extrusion in hard and soft tissue regeneration (%);
- Regenerative surgery: type of treatment (GTR, GBR, bone graft, distraction osteogenesis, ridge-splitting), materials and membranes used, and type of defects;
- Hard tissue changes;
- Soft tissue changes;
- Timing of implant placement;
- Type of implant;
- Treatment outcomes;
- Complications;
- Follow-up data;
- Implant survival rate.
2.5. Methodological Quality and Risk of Bias Evaluation
- ROBINS-I tools for non-randomized studies (Prospective studies, Case series);
- Rob 2.0 for Randomized Controlled Trials (RCT).
3. Results
3.1. Characteristics of the Included Studies
3.2. Characteristics of the Participants
3.3. Types of Treatment
3.3.1. Orthodontic Implant Site Development

{kind=link}
| Author | Patient Age | Sex | Treated Teeth | Reason of Extraction | Type of Appliance | Extrusion Method | Intensity of the Force | Anchorage | Extrusion Ratio | Follow-Up Weeks | Retention (month) | Amount of Tooth Extrusion (mm) | Amount of Bone Augmentation (mm) | Amount of Soft Tissue Augmentation (mm) | Efficacy % Bone | Efficacy % Soft Tissue |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Joo, Son, Lee [10] | 46 | F | 1.3 | Periodontitis | Multi-bkt appliance. | SS archwire with extrusion steps | 10–15 g | Steel archwire | 1 mm/month | 4 | 2 | NR | NR | 2 mm of overcorrection of the gingival margin | NR | NR |
| Watanabe et al. [7] | 41 | M | 1.1 | Periodontitis | Partial multi-bkt from 15 to 25. Micro-arch appliances Formula-R, Roth Type; Tomy Intl Inc. | Co-Cr Archwire with extrusion step, L-loop and inset component for palatal movement. Then TMA archwire | 15–80 g | NR | 1.4 mm/month | 4 | 2.5 | 7 | NR | 6–7 mm | NR | NR |
| Amato, Mirabella et al. [11] | NR | 3 M 10 F | n° 32 teeth, mainly anterior teeth | Periodontitis or non restorable teeth | Multi-bkt appliance. | SS archwire with extrusion steps and finally TMA | 15–50 g | Steel archwire | 1 mm/month | 4 | 2 | 3–10 mm | 0.6–8.0 mm | 1.7–7.7 mm | 70% | 65% |
| S. Hyun Kim et al. [9] | 30 | F | 1.1–1.2 | Periodontitis | Removable appliance and orthodontic hooks bonded to the cervical region of 1.1 and 1.2 | Elastic bands from the bonded hooks and the removable appliance | 70–100 g | Removable appliance | 1 mm/week followed by 3 weeks of stabilization | 4 | 1.5 | NR | NR | NR | NR | NR |
| Paolone et al. [8] | 57 | M | 2.1 | Trauma | Partial lingual multi-bkt from 14 to 24 (Ormco 7th gen). | Cu-NiTi archwire then TMA. More apical bonding. | NR | composite resin 12-11-X-22 veneer pontic | 0.5 mm/month | 2 | 6 | NR | NR | NR | NR | NR |
| Holst et al. [13] | 23 | F | 2.1 | Non-restorable | Partial ceramic multi-bkt from 14 to 24 | NiTi archwire. More apical bonding. | 30–50 g | NR | NR | 4 | 3 | NR | NR | NR | NR | NR |
| Erkut et al. [14] | 62 | F | 1.4–1.5 1.6 | Periodontitis | Full bimaxillary multi-bkt appliance | NiTi archwire. More apical bonding. Then SS archwire with extrusion steps and inter-maxillary elastics | <100 g | Steel archwire | NR | 2 | None | NR | NR | NR | NR | NR |
| Mantzikos, Shamus [12] | 34 | M | 1.1–2.1 | Periodontitis | Partial multi-bkt appliance from 13 to 23 | SS archwire with extrusion steps, then NiTi archwire | NR | NR | NR | 4 | 4–6 | NR | 7–8 mm | 5 mm | NR | NR |
| de Barros et al. [29] | 56 | F | 1.1–2.1 | Periodontitis | Full bimaxillary multi-bkt appliance | NiTi archwire. More apical bonding | NR | Steel archwire | NR | 2 weeks | 1 | NR | NR | NR | NR | NR |
| Chou et al. [30] | 40 | F | 4.6 | Periodontitis | Full bimaxillary multi-bkt appliance | SS archwire with L-shape loop | NR | Steel archwire | 0.5 mm/month | 1 month | 6 months | NR | 8 mm increase in the level bone on the mesial side; 6 mm increase on the distal side | NR | NR | NR |
| Mantzikos and Shamus [6] | NR | NR | 1.1–2.1 | Periodontitis | Partial multi-bkt appliance from 13 to 23 | SS archwire. More apical bonding | NR | Steel archwire | NR | 2 weeks | 3 months | NR | Mean 8 mm | NR | NR | NR |
3.3.2. Regenerative Procedures for Implant Site Development
| Author | Patient Age | Sex | Treated Teeth | Type of Defect | Type of Treatment | Materials | Type of Membranes | Follow-Up | Hard Tissue Changes | Soft Tissue Changes | Complications | Implant Survival Rate |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Xi Jiang et al. [15] | From 20 to 52 years | 15 M 13 F | Maxillary incisors | NR | Implant placement using submerged or transmucosal surgical technique and simultaneous GBR | Deproteinized bovine bone mineral (Bio-Oss) | resorbable collagen membrane (Bio-Gide) | 1 week 1 month 6 months Radiographic evaluations | GBR with resorbable collagen membrane and particulate bovine bone undergoes some horizontal volume reduction during the healing stage. Greater reduction happens in the coronal region. The use of different implant healing strategies (transmucosal or submerged) doesn’t make significant differences. | NR | None | 100% |
| J.P. Sullivan [16] | 32 | F | 1.1 | Cawood and Howell class V defect. | Autogenous bone graft from an intraoral site | Bone block from the right retromolar area and bovine derived bone particulate (Bio Oss) to fill the gaps | Resorbable porcine derived membrane (Bio-Gide) | 3 years | After 3 months the bone block was well integrated | NR | None | NR |
| Fagan et al. [17] | From 27 to 51 years | 18 M 19 F | Anterior maxilla | Absence or loss >50% of the buccal plate and gingival recession or thin gingival biotypes | Bone graft, use of platelet-derived growth factors and pediculated connective tissue graft to simultaneously augment hard and soft tissue. Immediate or delayed implant placement. | Freeze-dried mineralized bone allograft, recombinant human platelet derived growth factor mixture | titanium-reinforced membrane | 1 year | Enhancement of hard tissue | Enhancement of soft tissue | None | 97.3% |
| Petrungaro et al. [18] | 55 years and 26 years | 2 F | Mandibular right posterior region (Case report 2) and maxillary anterior region (Case report 3) | Advanced bone loss in the mandibular right posterior region (Case report 2) and in the maxillary anterior region (Case report 3) | Allogenic block graft and delayed implants | Puros block allograft rehydrated with platelet-rich plasma and additional particulate mineralized bone graft material (Puros) | Tutoplast Processed Pericardium; Tutogen Medical | 1 year | Enhancement of hard tissue | NR | None | NR |
| Artzi et al. [19] | From 42 to 54 years | 1 M 3 F | 1.3–1.1 4.4 and all the upper left quadrant | Different amount of bone loss | Immediate post-extractive implant placement and simultaneous GBR | Demineralized freeze-dried bone particles (Dembone) | e-PTFE membrane | 2 years | Enhancement of hard tissue with histological evaluations. | NR | None | NR |
| Artzi et al. [20] | From 32 to 40 years | 3 F | 1.6 1.5–1.4 1.2–1.1 2.1–2.2 | Different amount of bone loss | GBR and delayed implant placement | Demineralized freeze-dried bone particles (Dembone) | e-PTFE membrane | 2 years | Enhancement of hard tissue | NR | Early exposure of the e-PTFE membrane in one case, but with no consequences | NR |
| Sezer et al. [24] | NR | NR | Distraction was performed in different mandibular areas, according to each patient need. | Severe alveolar bone atrophy in mandible | Alveolar Distraction Osteogenesis | Distraction device (Modus ARS 1.5 V2 Distractor; Medartis) | None | 3 years | Increase in alveolar bone height with new bone formation beneath the distracted bone. Mean bone gain after distraction: 7mm | Simultaneous lengthening of the surrounding soft tissues. | In 1 patient a progressive lingual inclination of the distracted segment occurred during distraction. In 1 patient, a transient paresthesia of the area innervated by the inferior alveolar nerve was observed. Infection was observed in 1 case in the postoperative period. | 100% |
| McCarthy et al. [25] | From 18 to 68 years | 12 M 5 F | Anterior maxilla | Different amount of bone loss in the anterior maxilla. | Onlay Bone Grafts from the mandibular symphysis to anterior maxilla. | Corticocancellous block grafts and particulate cancellous grafts from the mandibular symphysis. | Nonresorbable Gore-Tex membrane | 3 years | Enhancement of hard tissue and improvement of the esthetic outcome. | NR | 4 patients reported paresthesia at the donor site immediately following the graft surgery. | 97.1% |
| Gozneli et al. [27] | 40 | M | 1.2–1.1 2.1–2.2 | Severe alveolar bone loss and gingival recessions in anterior maxilla. | Alveolar Distraction Osteogenesis | Distractor device (Modus Distractor; Medartis) | None | 1.5 years | An adequate vertical bone volume was obtained. | An adequate soft tissue volume around implants was obtained. | None | NR |
3.3.3. Spontaneous Healing of the Extraction Socket and Delayed Implant Placement
| Author | Patient Age | Sex | Type of Treatment | Treated Teeth | Timing of Implant Placement | Follow-Up | Hard Tissue Changes | Soft Tissue Changes | Complications | Implant Survival Rate |
|---|---|---|---|---|---|---|---|---|---|---|
| Crespi et al. [21] | From 43 to 70 years | 14 M 26 F | Atraumatic tooth extraction. Spontaneous healing of the extraction socket. Granulation tissue left in situ. No graft procedure. | Maxillary molars | Delayed implant placement 3 months after extraction | 3 months, 3 years | Bucco-lingual width showed a statistically significant decrease at implant placement. Moreover, a statistically significant increase was measured 3 years after implant insertion. Not statistically significant differences were found between baseline values (before extraction) and at 3 years from implant placement (11.44 ± 1.80 mm and 11.59 ± 1.61 mm, respectively). Vertical dimension showed statistically significant increase between baseline values (before extraction) and at 3 years from implant placement (8.05 ± 2.12 mm and 12.48 ± 2.04 mm, respectively) | NR | NR | 100% |
| Iasella et al. [22] | From 28 to 76 years | 10 M 14 F | Ridge Preservation procedure for implant site development with freeze-dried bone allograft and a collagen membrane compared to extraction alone | Teeth extracted consisted of: 11 maxillary premolar, 6 maxillary incisors, 1 maxillary canine and 6 mandibular premolars. | Delayed implant placement 4–6 months after extraction | 6 months | Ridge preservation procedures improved ridge height and width dimensions when compared to extraction alone. The width of the RP group decreased from 9.2 ± 1.2 mm to 8.0 ± 1.4 mm, while in the EXT group decreased from 9.1 ± 1.0 mm to 6.4 ± 2.2 mm, a difference of 1.6 mm. Most of resorption occurred from the buccal. The vertical change for the RP group was a gain of 1.3 ± 2.0 mm versus a loss 0.9 ± 1.6 mm for the EXT group. Histologic analysis revealed more bone in the RP group. | On the buccal aspect the RP group lost soft tissue thickness (−0.1 ± 0.5 mm), while the EXT group gained thickness (0.4 ± 0.6 mm) | Some sites showed little dehiscences at the time of implant placement | NR |
| Barone et al. [23] | From 26 to 69 years | 16 M 24 F | Xenograft versus Extraction Alone for Ridge Preservation after tooth extraction. | Tooth extractions were performed both in maxillary than in mandibular arch, according to each patient need. | Delayed implant placement, 7 months after extraction. | 7 months | A significantly greater horizontal resorption was observed at EXT sites (4.3 ± 0.8 mm) compared to RP sites (2.5 ± 1.2 mm). The ridge height reduction at the buccal side was 3.6 ± 1.5 mm for the extraction-alone group, whereas it was 0.7 ± 1.4 mm for the ridge-preservation group. Moreover, the vertical change at the lingual sites was 0.4 mm in the ridge-preservation group and 3 mm in the extraction-alone group. The histologic analysis showed a significantly higher percentage of trabecular bone and total mineralized tissue in ridge-preservation sites compared to extraction-alone sites | NR | None | NR |
| Barone et al. [28] | From 20 to 63 years | 20 M 38 F | Spontaneous healing vs. ridge preservation with secondary soft tissue healing | Tooth extractions were performed both in maxillary than in mandibular arch, according to each patient need. | Delayed implant placement, 4 months after tooth extraction | 8 months | In the grafted group changes in horizontal dimension showed an average resorption of 1.6 ± 0.55 mm. Vertical bone resorption was 0.3 ± 0.76 mm, 1.1 ± 0.96 mm, 0.3 ± 0.85 mm, 0.9 ± 0.98 mm at the mesial, buccal, distal and lingual sites respectively. In the non-grafted group, horizontal bone resorption was significantly higher (3.6 ± 0.72 mm). Vertical measurements indicated an average resorption of 1 ± 0.7 mm, 2.1 ± 0.6 mm, 1 ± 0.8 mm and 2 ± 0.73 mm respectively, at the mesial, buccal, distal and lingual sites. | The width of keratinized gingiva was better preserved in the grafted group. A greater shift of the gingival tissue towards the occlusal direction (mean 1.1 ± 0.9 mm) was observed in the grafted sites when compared to non-grafted sites (mean 0.7 ± 0.8 mm). | None | NR |
| Marconcini, Covani et al. [26] | mean of 53 years | 17 M 25 F | Ridge preservation with cortical (CORT) or collagenated (COLL) corticocancellous porcine bone compared to extraction alone (EXT). | According to each patient need: 1 tooth among first molars, first and second premolars or canines of both arches. | Delayed implant placement, 3 months after extraction. | 4 years | There were no differences regarding marginal bone change between the collagenated (COLL) and the cortical (CORT) corticocancellous porcine bone groups. Both grafts seemed to preserve the peri-implant marginal bone better than the natural healing. The total amount of marginal bone loss from T0 to T4-year was 1.14 ± 0.23 mm in the CORT group, 1.13 ± 0.29 mm in the COLL group and 1.92 ± 0.07 mm in the EXT group. | The Pink Esthetic Score (PES) resulted significantly better (9.42 ± 0.75) for the CORT group than for the COLL group (8.53 ± 1.18) and EXT group (6.07 ± 1.89) at 4-year evaluation. | None | 100% |
3.4. Methodological Quality and Risk of Bias Evaluation
4. Discussion
Study Limitations
5. Conclusions
- Low and controlled (<100 g) extrusive forces;
- Extrusion ratio < 1 mm/month;
- Extrusion according to the tooth long axis;
- A post-extrusion retention period is suggested to wait for the maturation of the regenerated bone;
- Immediate post-extractive implants are suggested to keep the hard and soft tissues volume obtained through the orthodontic technique; a guided insertion could be beneficial for aesthetic and patient comfort.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chappuis, V.; Araujo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Moya-Villaescusa, M.J.; Sanchez-Perez, A. Measurement of ridge alterations following tooth removal: A radiographic study in humans. Clin. Oral Implant. Res. 2010, 21, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Seibert, J.S.; Salama, H. Alveolar ridge preservation and reconstruction. Periodontology 2000 1996, 11, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Salama, H.; Salama, M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: A systematic approach to the management of extraction site defects. Int. J. Periodontics Restor. Dent. 1993, 13, 312–333. [Google Scholar]
- Mantzikos, T.; Shamus, I. Forced eruption and implant site development: An osteophysiologic response. Am. J. Orthod. Dentofac. Orthophedics 1999, 115, 583–591. [Google Scholar] [CrossRef]
- Mantzikos, T.; Shamus, I. Forced eruption and implant site development: Soft tissue response. Am. J. Orthod. Dentofac. Orthophedics 1997, 112, 596–606. [Google Scholar] [CrossRef]
- Watanabe, T.; Marchack, B.W.; Takei, H. Creating labial bone for immediate implant placement: A minimally invasive approach by using orthodontic therapy in the esthetic zone. J. Prosthet. Dent. 2013, 110, 435–441. [Google Scholar] [CrossRef]
- Paolone, M.; Kaitsas, R.; Paolone, G.; Kaitsas, V. Lingual orthodontics and forced eruption: A means for osseous and tissue regeneration. Case Report. Prog. Orthod. 2008, 9, 90–110. [Google Scholar]
- Hyun Kim, S.; Tramontina, V.A.; Papalexiou, V.; Luczyszyn, S.M. Orthodontic extrusion and implant site development using an interocclusal appliance for a severe mucogingival deformity: A clinical report. J. Prosthet. Dent. 2011, 105, 72–77. [Google Scholar] [CrossRef]
- Joo, J.Y.; Son, S.; Lee, J.Y. Implant site development for enhancing esthetics of soft and hard tissue and simplification of implant surgery using a forced eruption. Int. J. Periodontics Restor. Dent. 2016, 36, 583–589. [Google Scholar] [CrossRef]
- Amato, F.; Mirabella, D.; Macca, U.; Tarnow, D.P. Implant site development by orthodontic forced extraction: A preliminary study. Int. J. Oral Maxillofac. Implant. 2012, 27, 411–420. [Google Scholar]
- Mantzikos, T.; Shamus, I. Case report: Forced eruption and implant site development. Angle Orthod. 1998, 68, 179–186. [Google Scholar] [PubMed]
- Holst, S.; Hegenbarth, E.; Schlegel, K.A.; Holst, A.I. Restoration of a nonrestorable central incisor using forced orthodontic eruption, immediate implant placement and an all-ceramic restoration: A clinical report. J. Prosthet. Dent. 2007, 98, 251–255. [Google Scholar] [CrossRef]
- Erkut, S.; Arman, A.; Gulsahi, A.; Uckan, S.; Gulsahi, K. Forced eruption and implant treatment in posterior maxilla: A clinical report. J. Prosthet. Dent. 2007, 97, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zhang, Y.; Mi, P.; Lin, Y. Hard tissue volume stability of guided bone regeneration during the healing stage in the anterior maxilla: A clinical and radiographic study. Clin. Implant. Dent. Relat. Res. 2018, 20, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.P. Implant placement in the esthetic zone following an autogenous bone graft from an intraoral site: A Case Study. Prim. Dent. J. 2013, 2, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Fagan, M.C.; Owens, H.; Smaha, J.; Kao, R.T. Simultaneous hard and soft tissue augmentation for implants in the esthetic zone: Report of 37 consecutive cases. J. Periodontol. 2008, 79, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Petrungaro, P.; Salomon, A. Localized ridge augmentation with allogenic block grafts prior to implant placement: Case reports and histologic evaluations. Implant. Dent. 2005, 14, 139–148. [Google Scholar] [CrossRef]
- Artzi, Z.; Nemcovsky, C. Bone regeneration in extraction sites. Part I: The simultaneous approach. Implant. Dent. 1997, 6, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Artzi, Z.; Nemcovsky, C.; Rosenblat, O.; Zohar, R.; Kozak, D. Bone regeneration in extraction sites. Part II: The staged approach. Implant. Dent. 1997, 6, 183–187. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Crespi, G.; Gastaldi, G.; Gherlone, E.F. Delayed implants outcome in maxillary molar region. Clin. Implant. Dent. Relat. Res. 2017, 19, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Iasella, J.M.; Greenwell, H.; Miller, R.L.; Hill, M.; Drisko, C.; Bohra, A.A.; Scheetz, J.P. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: A clinical and histologic study in human. J. Periodontol. 2003, 74, 990–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, A.; Aldini, N.N.; Fini, M.; Giardino, R.; Calvo Guirado, J.L.; Covani, U. Xenograft versus extraction alone for ridge preservation after tooth removal: A clinical and histomorphometric study. J. Periodontol. 2008, 79, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B.; Koyuncu, B.O.; Gunbay, T.; Sezak, M. Alveolar distraction osteogenesis in the human mandible: A clinical and histomorphometric study. Implant. Dent. 2012, 21, 317–322. [Google Scholar] [CrossRef]
- McCarthy, C.; Patel, R.R.; Wragg, P.F.; Brook, I.M. Dental implants and onlay bone grafts in the anterior maxilla: Analysis of clinical outcome. Int. J. Oral Maxillofac. Implant. 2003, 18, 238–241. [Google Scholar]
- Marconcini, S.; Giammarinaro, E.; Derchi, G.; Alfonsi, F.; Covani, U.; Barone, A. Clinical outcomes of implants placed in ridge-preserved versus nonpreserved sites: A 4-year randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2018, 20, 906–914. [Google Scholar] [CrossRef]
- Gozneli, R.; Ozkan, Y.; Akalin, Z.F. Rehabilitation of maxillary anterior esthetics by alveolar distraction osteogenesis with immediate implant placement: A case report. Implant. Dent. 2010, 19, 468–476. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implant. Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef]
- de Barros, L.A.; de Almeida Cardoso, M.; de Avila, E.D.; de Molon, R.S.; Sigueira, D.F.; Mollo-Junior Fde, A. Six-year follow-up of maxillary anterior rehabilitation with forced orthodontic extrusion: Achieving esthetic excellence with a multidisciplinary approach. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 607–615. [Google Scholar] [CrossRef]
- Chou, Y.H.; Du, J.K.; Chou, S.T.; Hu, K.F.; Tsai, C.C.; Ho, K.Y.; Wu, Y.M.; Ho, Y.P. An interdisciplinary treatment approach combining orthodontic forced eruption with immediate implant placement to achieve a satisfactory treatment outcome: A case report. Clin. Implant. Dent. Relat. Res. 2013, 15, 113–120. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Komarek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of oral implant failure, up to abutment connection. J. Clin. Periodontol. 2007, 34, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, G.; Quirynen, M.; Komarek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin. Oral Implant. Res. 2008, 19, 670–676. [Google Scholar] [CrossRef]
- Bornestein, M.M.; Cionca, N.; Mombelli, A. Systemic conditions and treatments as risk for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 12–27. [Google Scholar]
- Diz, P.; Scully, C.; Sanz, M. Dental implants in the medically compromised patient. J. Dent. 2013, 41, 195–206. [Google Scholar] [CrossRef]
- Vervaeke, S.; Collaert, B.; Cosyn, J.; Deschepper, E.; De Bruyn, H. A multifactorial analysis to identify predictors of implant failure and peri-implant bone loss. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 1), 298–307. [Google Scholar] [CrossRef]
- Rondriguez-Arqueta, O.F.; Figueiredo, R.; Valmaseda-Castellon, E.; Gay-Escoda, C. Postoperative complications in smoking patients treated with implants. A retrospective study. J. Oral Maxillofac. Surg. 2011, 69, 2152–2157. [Google Scholar] [CrossRef]
- Kois, J.C.; Kan, J.Y. Predictable peri-implant gingival esthetics: Surgical and prosthodontics rationales. Pract. Proced. Aesthetic Dent. 2001, 13, 691–698. [Google Scholar]
- Koke, U.; Sander, C.; Heinecke, A.; Muller, H.P. A possible influence of gingival dimensions on attachment loss and gingival recession following placement of artificial crowns. Int. J. Periodontics Restor. Dent. 2003, 23, 439–445. [Google Scholar]
- Kan, J.Y.; Morimoto, T.; Rungcharassaeng, K.; Roe, P.; Smith, D.H. Gingival biotype assessment in the esthetic zone: Visual versus direct measurement. Int. J. Periodontics Restor. Dent. 2010, 30, 237–243. [Google Scholar]
- Hammerle, C.H.; Lang, N.P. Single stage surgery combining transmucosal implant placement with guided bone regeneration and bioresorbable materials. Clin. Oral Implant. Res. 2001, 12, 9–18. [Google Scholar] [CrossRef]
- Jung, R.E.; Fenner, N.; Hammerle, C.H.; Zitzmann, N.U. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12–14 years. Clin. Oral Implant. Res. 2013, 24, 1065–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiapasco, M.; Zaniboni, M. Clinical of GBR procedures to correct peri-implant dehiscences and fenestrations: A systematic review. Clin. Oral Implant. Res. 2009, 20, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Holst, A.I.; Nkenke, E.; Blatz, M.B.; Geiselhoringer, H.; Holst, S. Prosthetic considerations for orthodontic implant site development in the adult patient. J. Oral Maxillofac. Surg. 2009, 67, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Kaitsas, R.; Paolone, M.G.; Paolone, G. Guided orthodontic regeneration: A tool to enhance conventional regenerative techniques in implant surgery. Int. Orthod. 2015, 13, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Paolone, M.G.; Kaitsas, R. Orthodontic-periodontal interactions: Orthodontic extrusion in interdisciplinary regenerative treatments. Int. Orthod. 2018, 16, 217–245. [Google Scholar] [CrossRef]
- Taskonak, B.; Ozkan, Y. An alveolar bone augmentation technique to improve esthetics in anterior ceramic FPDs: A clinical report. J. Prosthodont. 2006, 15, 32–36. [Google Scholar] [CrossRef]
- Uribe, F.; Taylor, T.; Shafer, D.; Nanda, R. A novel approach for implant site development through root tipping. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 649–655. [Google Scholar] [CrossRef]
- Hof, M.; Pommer, B.; Strbac, G.D.; Suto, D.; Watzek, G.; Zechner, W. Esthetic evaluation of single-tooth implants in the anterior maxilla following autologous bone augmentation. Clin. Oral Implant. Res. 2013, 24 (Suppl. A), 88–93. [Google Scholar] [CrossRef]
- Bauer, C.; Boileau, M.J.; Bazert, C. Implementation of orthodontic extraction for pre-implant soft tissue management: A systematic review. Int. Orthod. 2019, 17, 20–37. [Google Scholar] [CrossRef]
- Almurtadha, R.H.; Alhammadi, M.S.; Fayed, M.M.S.; Abou-El-Ezz, A.; Halboub, E. Changes in soft tissue profile after orthodontic treatment with and without extraction: A systematic review and meta-analysis. J. Evid.-Based Dent. Pract. 2018, 18, 193–202. [Google Scholar] [CrossRef]
- Alsahhaf, A.; Att, W. Orthodontic extrusion for pre-implant site enhancement: Principles and clinical guidelines. J. Prosthodont. Res. 2016, 60, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, C.; Linde, A.; Gottlow, J.; Nyman, S. Healing of bone defects by guided tissue regeneration. Plast. Recostructive Surg. 1998, 81, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Devlin, H.; Sloan, P. Early bone healing events in the human extraction socket. Int. J. Oral Maxillofac. Surg. 2002, 31, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Magkavali-Trikka, P.; Kirmanidou, Y.; Michalakis, K.; Gracis, S.; Kalpidis, C.; Pissiotis, A.; Hirayama, H. Efficacy of two site-development procedures for implants in the Maxillary esthetic region: A systematic review. Int. J. Oral Maxillofac. Implant. 2015, 30, 73–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morjaria, K.R.; Wilson, R.; Palmer, R.M. Bone healing after tooth extraction with or without an intervention: A systematic review of randomized controlled trials. Clin. Implant. Dent. Relat. Res. 2014, 16, 1–20. [Google Scholar] [CrossRef]
- Lekholm, U.; Wannfors, K.; Isaksson, S.; Adielsson, B. Oral implants in combination with bone grafts. A 3 year retrospective multicenter study using Branemark implant system. Int. J. Oral Maxillofac. Surg. 1999, 28, 181–187. [Google Scholar] [CrossRef]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin. Oral Implant. Res. 2011, 23, 22–38. [Google Scholar] [CrossRef]
- Pietrokovski, J.; Massler, M. Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Wang, R.E.; Lang, N.P. Ridge preservation after tooth extraction. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 147–156. [Google Scholar] [CrossRef]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Ingber, J.S. Forced eruption part II: A method of treating non-restorable teeth—Periodontal and restorative considerations. J. Periodontol. 1976, 47, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Ingber, J.S. Forced eruption part I: A method of treating isolated one and two wall infrabony osseous defects—Rationale and case report. J. Periodontol. 1974, 45, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Somar, M.; Mohadeb, J.V.; Huang, C. Predictability of orthodontic forced eruption in developing an implant site: A systematic review. J. Clin. Orthod. 2016, 50, 485–492. [Google Scholar] [PubMed]
- Korayem, M.; Flores-Mir, C.; Nassar, U.; Olfert, K. Implant site development by orthodontic extrusion: A systematic review. Angle Orthod. 2008, 78, 752–760. [Google Scholar] [CrossRef]
- Misch, C.M. Implant site development using ridge splitting techniques. Oral Maxillofac. Surg. Clin. N. Am. 2004, 16, 65–74. [Google Scholar] [CrossRef] [PubMed]

| Author | Year | Type of Study | Type of Treatment | Treatment Outcomes | Timing of Implant Placement | Type of Implant | Follow-Up | Complications | Implant Survival Rate |
|---|---|---|---|---|---|---|---|---|---|
| Joo, Son, Lee [10] | 2016 | Case report | Orthodontic extrusion | Enhancement of hard and soft tissue and successful implant placement | Immediate post-extractive implant | 4.0 × 11.5 mm Nobel Biocare | 6 months | None | NR |
| Watanabe et al. [7] | 2013 | Case report | Orthodontic extrusion | Successful implant therapy. Satisfying esthetic and biologic results | Immediate post-extractive implant | 3.75 × 15 mm implant Nobel Mk III Nobel Biocare | 4 years | None | 100% |
| McCarthy et al. [25] | 2003 | Case series (17 patients) | Onlay Bone Grafts from the mandibular symphysis to anterior maxilla. | Satisfying results | Immediate or delayed implants | Brånemark System Mark II implants (Nobel Biocare) | 3 years | 4 patients reported paresthesia at the donor site immediately following the graft surgery. | 97.1% |
| Amato, Mirabella et al. [11] | 2012 | Case series (13 patients) | Orthodontic extrusion | Successful implant therapy. Satisfying esthetic and biologic results | Immediate post-extractive implant | 3.25, 4.0, 5.0 × 10, 11, 13, 15 mm. Biomet | 1.5–5 years | 1 implant failed ,Recessions 0.2–5.7 mm | 96% |
| S. Hyun Kim et al. [9] | 2011 | Case report | Orthodontic extrusion | Successful implant placement and improvement of esthetics | 6 weeks post extraction | 3.75 × 11 screw-type machined- submerged implants Titamax Ti Cortical; Neodent, | 5 years | Interdental papillae deficiency around 1.1 and 1.2 Some external root resorption in the apical third of 1.2 | NR |
| Marconcini, Covani et al. [26] | 2018 | RCT (42 patients) | Ridge preservation procedure with cortical (CORT) or collagenated (COLL) corticocancellous porcine bone compared to extraction alone (EXT) | Ridge preservation was more effective than natural healing in preserving marginal bone and in achieving esthetic outcomes around implants. The CORT showed better clinical outcomes than COLL. | 3 months after extraction | Delayed implants (BT Evo; Biotec) | 4 years | None | 100% |
| Paolone et al. [8] | 2008 | Case report | Orthodontic extrusion | Successful implant therapy. Satisfying esthetic and biologic results | Immediate post-extractive implant | 4.5 × 15 mm root-form implant FRIALIT-2 Dentsply FRIADENT | NR | None | NR |
| Holst et al. [13] | 2007 | Case report | Orthodontic extrusion | Successful implant rehabilitation and good esthetic outcomes | Immediate post-extractive implant | 4 × 13 mm implant Nobel Biocare | 2 years | None | NR |
| Erkut et al. [14] | 2007 | Case report | Orthodontic extrusion | Successful implant therapy. Satisfying esthetic and biologic results | Immediate post-extractive implant | 4.1 × 12 mm implants | 7 months | None | NR |
| Mantzikos and Shamus [5] | 1999 | Case series (5 patients) | Orthodontic extrusion | Enhancement of soft and hard tissue and successful implant placement | Immediate post-extractive implant | NR | NR | None | NR |
| Mantzikos, Shamus [12] | 1998 | Case report | Orthodontic extrusion | Enhancement of soft and hard tissue and successful implant placement | 4 weeks after extraction | 3.75 × 15 mm implants | NR | None | NR |
| Xi Jiang et al. [15] | 2017 | RCT (28 patients) | GBR | Good results | Simultaneous implant placement using submerged or transmucosal surgical technique | Dentsply implants | 6 months | None | NR |
| J.P. Sullivan [16] | 2013 | Case report | Autogenous bone graft from an intraoral site | Good results | 3 months after bone grafting | NR | 3 years | None | NR |
| Sezer et al. [24] | 2012 | Case series (10 patients) | Alveolar Distraction Osteogenesis | Good results | 4 months after consolidation of distracted segments | Strauman implants | 3 years | In 1 patient a progressive lingual inclination of the distracted segment occurred during distraction. In 1 patient, a transient paresthesia of the area innervated by the inferior alveolar nerve was observed. Infection was observed in 1 case in the postoperative period. | 100% |
| Fagan et al. [17] | 2008 | Case series (37 patients) | Freeze-dried mineralized bone allograft (FDBA), recombinant human platelet-derived growth factor mixture with a titanium-reinforced membrane and a pediculated connective tissue graft (PCTG) to simultaneously augment hard and soft tissue. | Good esthetic and functional results | Immediate implants (25 patients) Or delayed implants (12 patients) | BioMet. or Nobel Biocare implants | 1 year | None | 97.3% |
| Petrungaro et al. [18] | 2005 | 2 Case reports | Allogenic block graft | Good results | Delayed implants | Screw-Vent implants (Zimmer Dental) | 1 year | None | NR |
| Artzi et al. [19] | 1997 | 4 Case reports | Immediate post-extractive implant placement and simultaneous GBR | Good results | Immediate post-extractive implants | Cylindrical implants, Integral Omniloc | 2 years | None | NR |
| Artzi et al. [20] | 1997 | 3 Case reports | GBR and delayed implant placement | Good results | Delayed implant placement, 9 months after GBR | NR | 2 years | Early exposure of the e-PTFE membrane in one case, but with no consequences | NR |
| Crespi et al. [21] | 2016 | Prospective study (40 patients) | No graft procedure. Spontaneous healing of the extraction socket. Granulation tissue left in situ. Delayed implant placement after 3 months | Good results | Delayed implant placement, 3 months after tooth extraction | Titanium implants with rough surface, Titanium Plasma Spray. | 3 months, 3 years | None | 100% |
| Iasella et al. [22] | 2003 | RCT (24 patients) | Ridge Preservation with freeze-dried bone allograft and a collagen membrane for implant site development compared to extraction alone | Ridge preservation procedures improved ridge height and width dimensions compared to extraction alone. | Delayed implants | Root-form implants | 6 months | Some sites showed little dehiscences at the time of implant placement | NR |
| Barone et al. [23] | 2008 | RCT (40 patients) | Xenograft for Ridge Preservation after tooth extraction versus Extraction Alone | The ridge preservation procedure significantly limited the resorption of hard tissue after tooth extraction compared to extraction alone. | Delayed implants | NR | 7 months | None | NR |
| Gozneli et al. [27] | 2010 | Case report | Alveolar Distraction Osteogenesis | Good results | 4 months after consolidation of distracted segments, immediate post-extractive implants | Strauman implants | 1.5 years | None | NR |
| Barone et al. [28] | 2012 | RCT (58 patients) | Spontaneous healing vs. ridge preservation with secondary soft tissue healing | Alveolar ridge preservation technique limits the contour changes after tooth extraction and allows a better preservation of facial keratinized tissue. | Delayed implant placement, 4 months after tooth extraction | NR | 8 months | None | NR |
| Borelli de Barros et al. [29] | 2013 | Case report | Orthodontic extrusion | Successful implant therapy. Satisfying results | Immediate post-extractive implant | Cone Morse 3.5 × 13 mm. Neodent | 6 years | None | NR |
| Chou et al. [30] | 2011 | Case report | Orthodontic extrusion | Good esthetic and functional outcomes | Immediate post-extractive implant | 5 × 11.5 mm Implant Osseotite, Biomet | 2 years | None | NR |
| Reference | Type of Study | Random Sequence Generation | Allocation Concealment | Selective Reporting | Other Bias | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Conclusion |
|---|---|---|---|---|---|---|---|---|---|
| Xi Jiang et al. [15] | RCT | yes | yes | no | unclear | no | unclear | no | good quality |
| Iasella et al. [22] | RCT | yes | unclear | no | unclear | no | yes | no | good quality |
| Barone et al. [23] | RCT | yes | unclear | no | unclear | no | yes | no | good quality |
| Barone et al. [28] | RCT | yes | unclear | no | unclear | no | yes | no | good quality |
| Marconcini, Covani et al. [26] | RCT | yes | yes | no | unclear | no | yes | no | good quality |
| Reference | Type of Study | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias due to Missing Data | Bias in Measurement of Outcomes | Bias in the Selection of the Reported Results | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| Amato, Mirabella et al. [11] | Case series | low risk | low risk | low risk | low risk | low risk | moderate risk | low risk | Low risk |
| Sezer et al. [24] | Case series | low risk | low risk | low risk | low risk | low risk | low risk | low risk | Low risk |
| Fagan et al. [17] | Case series | low risk | low risk | low risk | low risk | high risk | moderate risk | high risk | Moderate risk |
| McCarthy et al. [25] | Case series | low risk | low risk | low risk | low risk | high risk | moderate risk | high risk | Moderate risk |
| Crespi et al. [21] | Prospective study | low risk | low risk | low risk | low risk | high risk | low risk | moderate risk | Moderate risk |
| Reference | Title (Max 1) | Key Words (Max 1) | Abstract (Max 4) | Introduction (Max 1) | Patient Information (Max 4) | Clinical Findings (Max 1) | Timeline (Max 1) | Diagnostic Assessment (Max 4) | Therapeutic Intervention (Max 3) | Follow-Up and Outcomes (Max 4) | Discussion (Max 4) | Patient Perspective (Max 1) | Informed Consent (Max 1) | Total (Max 30) | Quality of the Study |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Joo, Son, Lee [10] | 1 | 0 | 2 | 1 | 3 | 1 | 1 | 4 | 3 | 4 | 4 | 0 | 1 | 25 | G |
| Watanabe et al. [7] | 1 | 0 | 2 | 1 | 2 | 1 | 1 | 2 | 3 | 1 | 3 | 0 | 0 | 18 | P |
| de Barros et al. [29] | 1 | 0 | 2 | 1 | 2 | 1 | 1 | 3 | 3 | 2 | 4 | 0 | 0 | 20 | S |
| Hyun Kim et al. [9] | 1 | 0 | 3 | 1 | 3 | 1 | 1 | 2 | 3 | 2 | 3 | 0 | 1 | 21 | S |
| Chou et al. [30] | 1 | 1 | 4 | 1 | 3 | 1 | 1 | 4 | 3 | 1 | 3 | 0 | 0 | 23 | S |
| Paolone et al. [8] | 1 | 1 | 2 | 1 | 4 | 1 | 1 | 3 | 3 | 0 | 2 | 0 | 0 | 19 | P |
| Holst et al. [13] | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 3 | 1 | 3 | 0 | 0 | 12 | P |
| Erkut et al. [14] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 3 | 3 | 1 | 1 | 0 | 1 | 16 | P |
| Mantzikos, Shamus [12] | 1 | 1 | 2 | 1 | 4 | 1 | 1 | 4 | 3 | 0 | 0 | 0 | 0 | 17 | P |
| J.P. Sullivan [16] | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 4 | 3 | 0 | 1 | 0 | 0 | 17 | P |
| Gozneli et al. [27] | 1 | 1 | 4 | 1 | 3 | 1 | 1 | 2 | 3 | 3 | 4 | 0 | 1 | 25 | G |
| Petrungaro et al. [18] | 1 | 1 | 3 | 1 | 1 | 1 | 1 | 0 | 3 | 1 | 1 | 0 | 0 | 14 | P |
| Artzi et al. [19] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 3 | 0 | 0 | 11 | P |
| Artzi et al. [20] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 3 | 0 | 0 | 11 | P |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isola, G.; Nucera, R.; Damonte, S.; Ugolini, A.; De Mari, A.; Migliorati, M. Implant Site Changes in Three Different Clinical Approaches: Orthodontic Extrusion, Regenerative Surgery and Spontaneous Healing after Extraction: A Systematic Review. J. Clin. Med. 2022, 11, 6347. https://doi.org/10.3390/jcm11216347
Isola G, Nucera R, Damonte S, Ugolini A, De Mari A, Migliorati M. Implant Site Changes in Three Different Clinical Approaches: Orthodontic Extrusion, Regenerative Surgery and Spontaneous Healing after Extraction: A Systematic Review. Journal of Clinical Medicine. 2022; 11(21):6347. https://doi.org/10.3390/jcm11216347
Chicago/Turabian StyleIsola, Gaetano, Riccardo Nucera, Silvia Damonte, Alessandro Ugolini, Anna De Mari, and Marco Migliorati. 2022. "Implant Site Changes in Three Different Clinical Approaches: Orthodontic Extrusion, Regenerative Surgery and Spontaneous Healing after Extraction: A Systematic Review" Journal of Clinical Medicine 11, no. 21: 6347. https://doi.org/10.3390/jcm11216347