
Lung Ultrasound Findings in Healthy Children and in Those Who Had Recent, Not Severe COVID-19 Infection

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
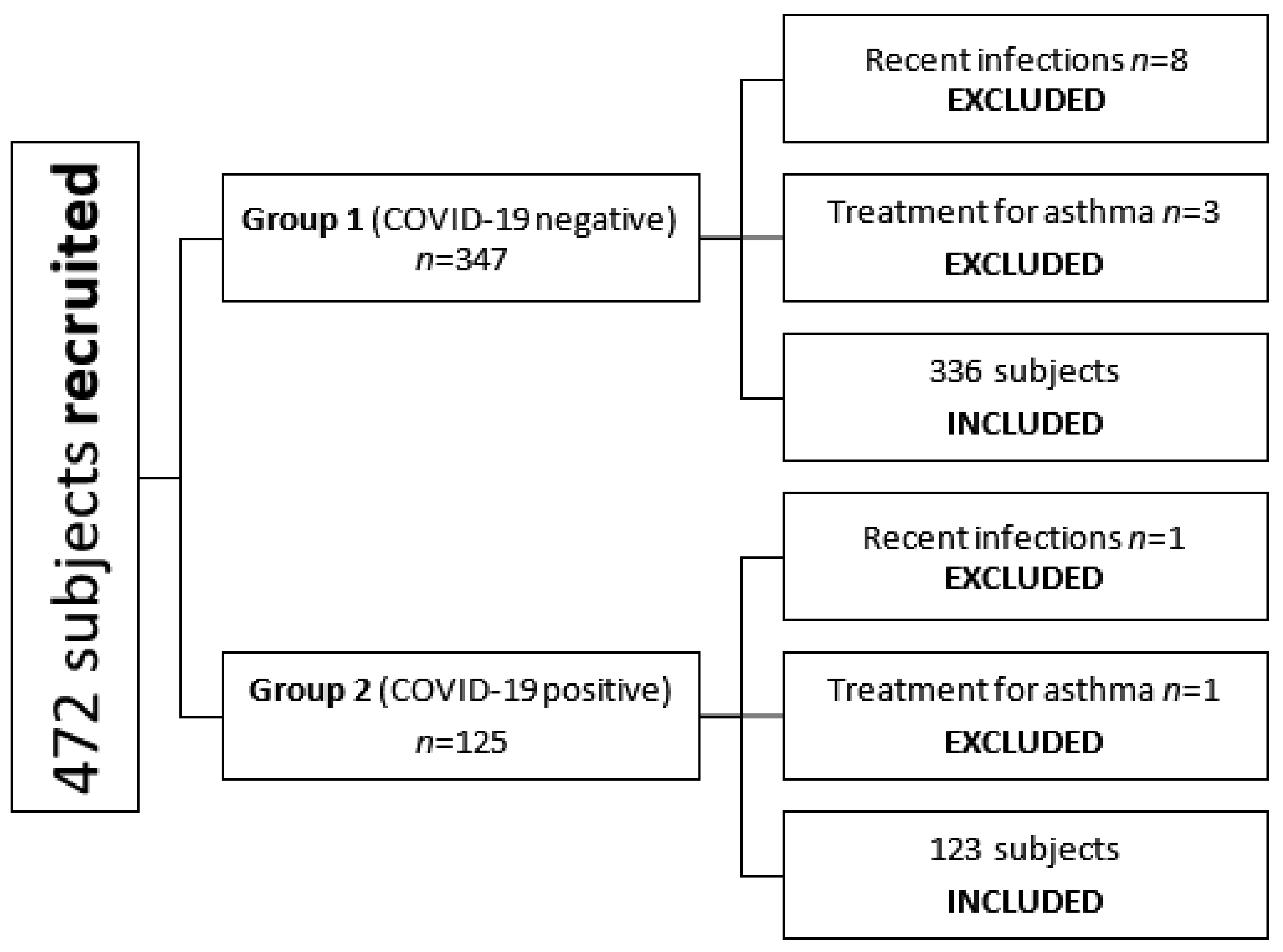
2. Methods
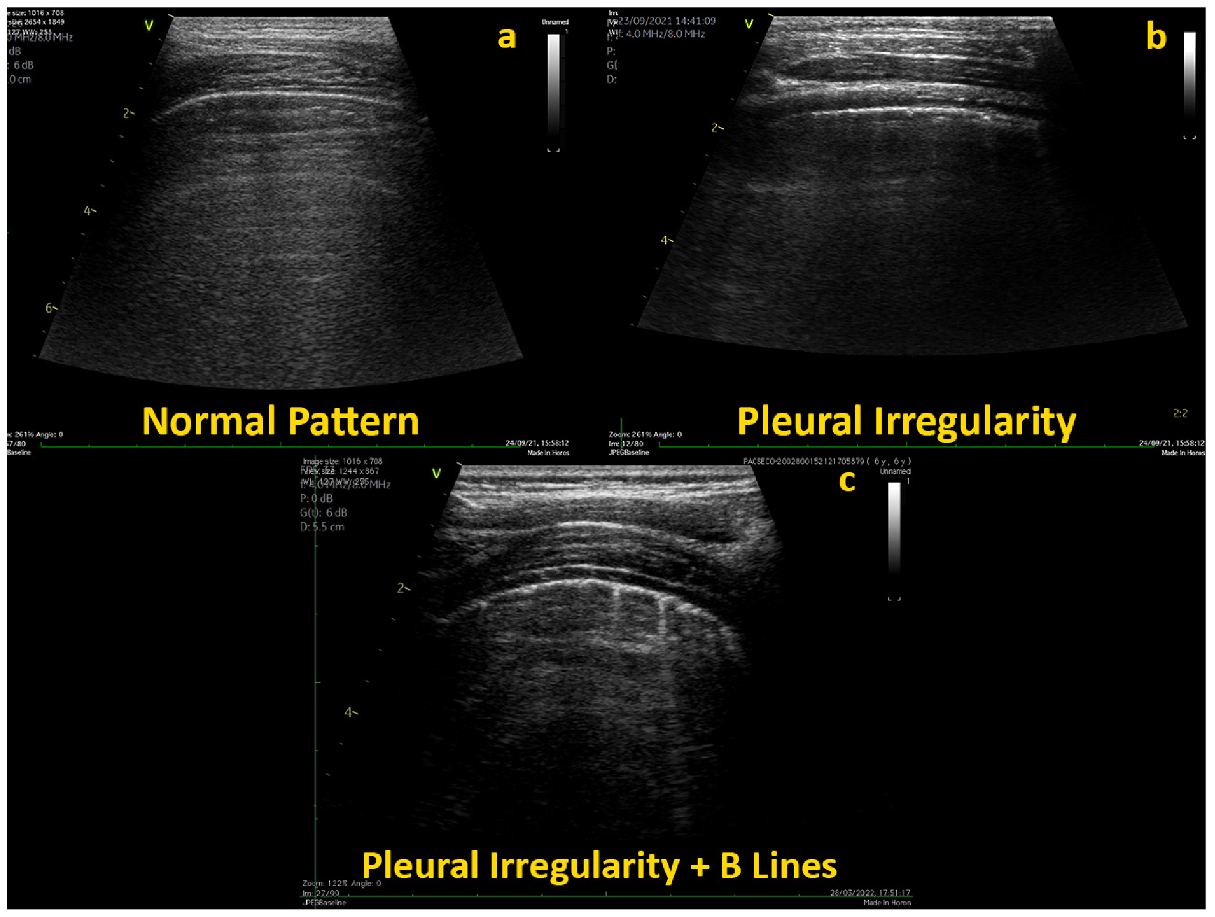
Lung Ultrasound Examination
- Pattern 1: Absence of sub-pleural artifacts and no B-lines, point 0;
- Pattern 2: Only mild basal posterior sub-pleural artifacts and no B-lines, point 0–0.1’;
- Pattern 3: Mild posterior basal, para-spine, and apical short subpleural vertical artifacts and no B-lines, point 0.1–0.2;
- Pattern 4: Mild posterior basal, para-spine, and apical short subpleural vertical artifacts and rare B-lines (e.g., ≤2 in each segment), point 0.2–0.4;
- Pattern 5: Mild, diffuse short subpleural vertical artifacts and rare B-lines (e.g., ≤2 in each segment), point 0.4–0.6;
- Pattern 6: Mild, diffuse short subpleural vertical artifacts and limited B-lines (e.g., ≤4 in each segment), point 0.6–0.8;
- Pattern 7: Mild, diffuse short subpleural vertical artifacts with mild subpleural areas of atelectasis and limited B-lines (e.g., ≤4 in each segment), point 0.8–1.
3. Statistical Analysis
4. Results
4.1. LUS Score in Healthy Children Who Did Not Experience COVID-19 Infection
4.2. LUS Score in Healthy Children Who Had Previous COVID-19 Infection
4.3. Comparison of Patients with Positive and Negative Anamnesis for COVID-19
4.4. LUS Correlation with Symptoms of Previous COVID-19 Infection
4.5. Confounders: Differences among Age Groups
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Group 1 (Negative) n = 336 | Group 2 (Positive) n = 123 | |||||||
|---|---|---|---|---|---|---|---|---|
| Right Lung | Left Lung | Right Lung | Left Lung | |||||
| n | % | n | % | n | % | n | % | |
| Pattern 1 | 32 | 9.52 | 36 | 10.71 | 8 | 6.50 | 2 | 1.63 |
| Pattern 2 | 13 | 3.87 | 13 | 3.87 | 12 | 9.76 | 19 | 15.45 |
| Pattern 3 | 171 | 50.89 | 150 | 44.64 | 37 | 30.08 | 48 | 39.02 |
| Pattern 4 | 76 | 22.62 | 92 | 27.38 | 44 | 35.77 | 31 | 25.20 |
| Pattern 5 | 28 | 8.33 | 28 | 8.33 | 12 | 9.76 | 14 | 11.38 |
| Pattern 6 | 10 | 2.988 | 11 | 3.27 | 6 | 4.88 | 6 | 4.88 |
| Pattern 7 | 6 | 1.79 | 6 | 1.79 | 4 | 3.25 | 3 | 2.44 |
| Asymptomatic COVID-19 n = 47 | Mild Symptomatology n = 56 | Moderate Symptomatology n = 20 | Asympt vs. Mild | Asympt vs. Mod | Mild vs. Mod | Neg vs. Asympt | Neg vs. Mild | Neg vs. Mod | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min– Max | Mean | SD | Min– Max | Mean | SD | Min– Max | p | p | p | p | p | p | |
| Right LUS | 0.282 | 0.188 | 0.0– 0.8 | 0.296 | 0.194 | 0.0– 1.0 | 0.418 | 0.27 | 0.1– 1.0 | 0.691 | 0.026 | 0.043 | 0.247 | 0.048 | <0.0001 |
| Left LUS | 0.26 | 0.16 | 0.1– 0.8 | 0.328 | 0.212 | 0.0– 1.0 | 0.364 | 0.24 | 0.1– 1.0 | 0.06 | 0.044 | 0.546 | 0.919 | 0.009 | 0.012 |
| Group 1 (Negative) | Group 2 (Positive) | |||||||
|---|---|---|---|---|---|---|---|---|
| Age Groups | n | Mean | SD | n | Mean | SD | p | |
| Global LUS | <24 months | 5 | 0.22 | 0.07 | 3 | 0.4 | 0.24 | / |
| 2–5 years | 24 | 0.27 | 0.16 | 2 | 0.18 | 0.18 | / | |
| 5–11 years | 153 | 0.26 | 0.16 | 55 | 0.28 | 0.18 | 0.5 | |
| 11–18 years | 154 | 0.258 | 0.148 | 63 | 0.33 | 0.2 | 0.004 | |
| Right LUS | <24 months | 5 | 0.22 | 0.044 | 3 | 0.4 | 0.2 | / |
| 2–5 years | 24 | 0.27 | 0.174 | 2 | 0.15 | 0.212 | / | |
| 5–11 years | 153 | 0.254 | 0.168 | 55 | 0.28 | 0.204 | 0.4 | |
| 11–18 years | 154 | 0.25 | 0.154 | 63 | 0.332 | 0.21 | 0.0018 | |
| Left LUS | <24 months | 5 | 0.26 | 0.09 | 3 | 0.434 | 0.288 | / |
| 2–5 years | 24 | 0.25 | 0.162 | 2 | 0.2 | 0.142 | / | |
| 5–11 years | 153 | 0.264 | 0.18 | 55 | 0.28 | 0.184 | 0.6 | |
| 11–18 years | 154 | 0.262 | 0.16 | 63 | 0.326 | 0.208 | 0.02 | |
| Measurements | ICC Inter-Observer | ICC Intra-Observer | CV Inter-Observer | CV Intra-Observer |
|---|---|---|---|---|
| Right LUS | 0.779 (0.728–0.899) | 0.790 (0.722–0.849) | 5.3 | 3.1 |
| Left LUS | 0.799 (0.731–0.850) | 0.863 (0.755–0.945) | 5.4 | 3.3 |
References
- Liu, J.; Guo, G.; Kurepa, D.; Volpicelli, G.; Sorantin, E.; Lovrenski, J.; Alonso-Ojembarrena, A.; Hsieh, K.-S.; Lodha, A.; Yeh, T.F.; et al. Specification and guideline for technical aspects and scanning parameter settings of neonatal lung ultrasound examination. J. Matern. Fetal Neonatal Med. 2022, 35, 1003–1016. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Pereda, M.A.; Chavez, M.A.; Hooper-Miele, C.C.; Gilman, R.H.; Steinhoff, M.C.; Ellington, L.E.; Gross, M.; Price, C.; Tielsch, J.M.; Checkley, W. Lung ultrasound for the diagnosis of pneumonia in children: A meta-analysis. Pediatrics 2015, 35, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Cattarossi, L. Lung ultrasound: Its role in neonatology and pediatrics. Early Hum. Dev. 2013, 89, S17–S19. [Google Scholar] [CrossRef]
- Cantinotti, M.; Ali, L.A.; Scalese, M.; Giordano, R.; Melo, M.; Remoli, E.; Franchi, E.; Clemente, A.; Moschetti, R.; Festa, P.; et al. Lung ultrasound reclassification of chest X-ray data after pediatric cardiac surgery. Paediatr. Anaesth. 2018, 28, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, A.O.; Costa, R.M.; Uzun, R.; Fraga, A.M.A.; Ribeiro, J.D.; Marson, F.A.L. Applicability of lung ultrasound in COVID-19 diagnosis and evaluation of the disease progression: A systematic review. Pulmonology 2021, 27, 529–562. [Google Scholar] [CrossRef]
- Cheung, J.C.; Lam, K.N. POCUS in COVID-19, pearls and pitfalls. Lancet Respir. Med. 2020, 8, e34. [Google Scholar] [CrossRef]
- Di Cicco, M.; Tozzi, M.G.; Ragazzo, V.; Peroni, D.; Kantar, A. Chronic respiratory diseases other than asthma in children: The COVID-19 tsunami. Ital. J. Pediatr 2021, 47, 220. [Google Scholar] [CrossRef] [PubMed]
- Gregori, G.; Sacchetti, R. Lung ultrasound in outpatient approach to children with suspected COVID-19. Ital. J. Pediatr. 2020, 46, 171. [Google Scholar] [CrossRef] [PubMed]
- Sainz, T.; Udaondo, C.; Méndez-Echevarría, A.; Calvo, C. Lung Ultrasound for Evaluation of COVID-19 in Children. Arch. Bronconeumol. 2021, 57, 94–96. [Google Scholar] [CrossRef]
- Denina, M.; Scolfaro, C.; Silvestro, E.; Pruccoli, G.; Mignone, F.; Zoppo, M.; Ramenghi, U.; Garazzino, S. Lung Ultrasound in Children with COVID-19. Pediatrics 2020, 146, e20201157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchese, P.; Scalese, M.; Giordano, R.; Assanta, N.; Franchi, E.; Koestenberger, M.; Ravaglioli, A.; Kutty, S.; Cantinotti, M. Pediatric ranges of normality for 2D speckle-tracking echocardiography atrial strain: Differences between p- and r-gating and among new (Atrial Designed) and conventional (Ventricular Specific) software’s. Echocardiography 2021, 38, 2025–2031. [Google Scholar] [CrossRef]
- 34820892. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 24 October 2020).
- Cantinotti, M.; Giordano, R.; Scalese, M.; Marchese, P.; Franchi, E.; Viacava, C.; Molinaro, S.; Assanta, N.; Koestenberger, M.; Kutty, S.; et al. Prognostic Value of a New Lung Ultrasound Score to Predict Intensive Care Unit Stay in Pediatric Cardiac Surgery. Ann. Thorac. Surg. 2020, 109, 178–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prnjavorac, B.; Mujaković, A.; Prnjavorac, L.; Bego, T.; Jusufović, E.; Begić, E.; Torlak-Arnaut, V.; Mutapčić, M.; Škiljo, H.; Hodžić, E.; et al. Chest X-ray resolution after SARS-CoV-2 infection. Med. Glas. 2021, 18, 370–377. [Google Scholar] [CrossRef]
- Vitale, V.; Ricci, Z.; Cogo, P. Lung ultrasonography and pediatric cardiac surgery: First experience with a new tool for postoperative lung complications. Ann. Thorac. Surg. 2014, 97, e121–e124. [Google Scholar] [CrossRef]
- Rodríguez-Fanjul, J.; Llop, A.S.; Balaguer, M.; Bautista-Rodriguez, C.; Hernando, J.M.; Jordan, I. Usefulness of Lung Ultrasound in Neonatal Congenital Heart Disease (LUSNEHDI): Lung Ultrasound to Assess Pulmonary Overflow in Neonatal Congenital Heart Disease. Pediatr. Cardiol. 2016, 37, 1482–1487. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Volpicelli, G. How I do it: Lung ultrasound. Cardiovasc. Ultrasound 2014, 12, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buda, N.; Kosiak, W.; Wełnicki, M.; Skoczylas, A.; Olszewski, R.; Piotrkowski, J.; Skoczyński, S.; Radzikowska, E.; Jassem, E.; Grabczak, E.M.; et al. Recommendations for Lung Ultrasound in Internal Medicine. Diagnostics 2020, 10, 597. [Google Scholar] [CrossRef]
- Raimondi, F.; Migliaro, F.; Sodano, A.; Umbaldo, A.; Romano, A.; Vallone, G.; Capasso, L. Can neonatal ultrasound monitor fluid clearence and preditc the need of respiratory support? Crit. Care 2012, 16, R220. [Google Scholar] [CrossRef] [Green Version]
- Cantinotti, M.; Marchese, P.; Giordano, R.; Franchi, E.; Assanta, N.; Jani, V.; Kutty, S.; Gargani, L. Overview of Lung Ultrasound in Pediatric Cardiology. Diagnostics 2022, 12, 763. [Google Scholar] [CrossRef] [PubMed]
- Quarato, C.M.I.; Mirijello, A.; Maggi, M.M.; Borelli, C.; Russo, R.; Lacedonia, D.; Barbaro, M.P.F.; Scioscia, G.; Tondo, P.; Rea, G.; et al. Lung Ultrasound in the Diagnosis of COVID-19 Pneumonia: Not Always and Not Only What Is COVID-19 “Glitters”. Front. Med. 2021, 8, 707602. [Google Scholar] [CrossRef] [PubMed]
- Schmickl, C.N.; Menon, A.A.; Dhokarh, R.; Seth, B.; Schembri, F. Opti-mizing B-lines on lung ultrasound: An in-vitro to in-vivo pilot study with clinical implications. J. Clin. Monit. Comput. 2020, 34, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Matthias, I.; Panebianco, N.L.; Maltenfort, M.G.; Dean, A.J.; Baston, C. Effect of Machine Settings on Ultrasound Assessment of B-lines. J. Ultrasound Med. 2020, 40, 2039–2046. [Google Scholar] [CrossRef]
- Musolino, A.M.; Boccuzzi, E.; Buonsenso, D.; Supino, M.C.; Mesturino, M.A.; Pitaro, E.; Ferro, V.; Nacca, R.; Sinibaldi, S.; Palma, P.; et al. The Role of Lung Ultrasound in Diagnosing COVID-19-Related Multisystemic Inflammatory Disease: A Preliminary Experience. J. Clin. Med. 2022, 11, 234. [Google Scholar] [CrossRef] [PubMed]


| Whole Population n = 459 | Group 1 (Negative) n = 336 | Group 2 (Positive) n = 123 | Group 1 vs. Group 2 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min | Max | Median | Mean | SD | Min | Max | Median | Mean | SD | Min | Max | Median | p | |
| Age (years) | 10.564 | 3.839 | 0.293 | 17.868 | 10.701 | 10.498 | 3.941 | 0.293 | 17.868 | 10.618 | 10.745 | 3.555 | 0.934 | 17.847 | 11.118 | 0.543 |
| Weight (kg) | 39.556 | 17.11 | 8.000 | 133.00 | 37.000 | 39.275 | 17.30 | 8.000 | 133.00 | 36.500 | 40.321 | 16.65 | 13.00 | 83.000 | 39.000 | 0.563 |
| Height (cm) | 141.56 | 23.80 | 11.00 | 189.00 | 144.00 | 140.77 | 24.47 | 11.00 | 187.00 | 144.00 | 143.71 | 21.82 | 80.00 | 189.00 | 145.00 | 0.242 |
| BSA (m2) | 1.231 | 0.355 | 0.339 | 2.051 | 1.216 | 1.222 | 0.355 | 0.339 | 2.051 | 1.202 | 1.255 | 0.353 | 0.548 | 2.038 | 1.255 | 0.379 |
| Right LUS | 0.268 | 0.176 | 0.0 | 1.0 | 0.2 | 0.254 | 0.16 | 0.0 | 0.8 | 0.2 | 0.308 | 0.206 | 0.0 | 1.0 | 0.3 | 0.0034 |
| Left LUS | 0.274 | 0.178 | 0.0 | 1.0 | 0.2 | 0.262 | 0.168 | 0.0 | 0.8 | 0.2 | 0.306 | 0.200 | 0.0 | 1.0 | 0.2 | 0.02 |
| Global LUS | 0.271 | 0.163 | 0.0 | 1.0 | 0.2 | 0.259 | 0.154 | 0.0 | 0.8 | 0.2 | 0.306 | 0.185 | 0.0 | 1.0 | 0.25 | 0.006 |
| Total n = 459 | Group 1 (Negative) n = 336 | Group 2 (Positive) n = 123 | ||||
|---|---|---|---|---|---|---|
| Total LUS Score | Total LUS Score | Total LUS Score | ||||
| n | % | n | % | n | % | |
| Pattern 1 | 41 | 8.93 | 35 | 10.42 | 7 | 5.69 |
| Pattern 2 | 26 | 5.66 | 16 | 4.76 | 10 | 8.13 |
| Pattern 3 | 206 | 44.88 | 171 | 50.89 | 37 | 30.08 |
| Pattern 4 | 117 | 25.49 | 76 | 22.62 | 46 | 37.4 |
| Pattern 5 | 41 | 8.93 | 22 | 6.55 | 12 | 9.76 |
| Pattern 6 | 17 | 3.7 | 10 | 2.98 | 6 | 4.88 |
| Pattern 7 | 11 | 2.4 | 6 | 1.79 | 5 | 4.07 |
| Asymptomatic COVID-19 n = 47 | Mild Symptomatology n = 56 | Moderate Symptomatology n = 20 | Asympt vs. Mild | Asympt vs. Mod | Mild vs. Mod | Neg vs. Asympt | Neg vs. Mild | Neg vs. Mod | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min– Max | Mean | SD | Min– Max | Mean | SD | Min– Max | p | p | p | p | p | p | |
| Age (y) | 10.797 | 3.943 | 0.934– 17.847 | 10.311 | 3.214 | 1.477– 15.529 | 12.048 | 3.336 | 6.762– 17.479 | 0.487 | 0.247 | 0.06 | 0.4 | 0.213 | 0.09 |
| Weight (kg) | 41.93 | 18.25 | 16.7– 83.0 | 36.74 | 14.15 | 13.0– 75.0 | 47.68 | 17.43 | 24.0– 78.0 | 0.103 | 0.262 | 0.01 | 0.12 | 0.11 | 0.08 |
| Height (cm) | 145.63 | 22.355 | 107.0– 189.0 | 140.04 | 21.78 | 80.0– 175.0 | 150.53 | 19.07 | 120.0– 180.0 | 0.195 | 0.423 | 0.078 | 0.049 | 0.07 | 0.32 |
| BSA | 1.286 | 0.383 | 0.712– 2.038 | 1.184 | 0.315 | 0.548– 1.863 | 1.402 | 0.349 | 0.912– 1.949 | 0.133 | 0.278 | 0.02 | 0.74 | 0.62 | 0.13 |
| Global LUS | 0.26 | 0.15 | 0.1– 0.8 | 0.312 | 0.19 | 0.0– 1.0 | 0.392 | 0.23 | 0.1– 1.0 | 0.19 | 0.01 | 0.14 | 0.7 | 0.018 | 0.0004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantinotti, M.; Marchese, P.; Assanta, N.; Pizzuto, A.; Corana, G.; Santoro, G.; Franchi, E.; Viacava, C.; Van den Eynde, J.; Kutty, S.; et al. Lung Ultrasound Findings in Healthy Children and in Those Who Had Recent, Not Severe COVID-19 Infection. J. Clin. Med. 2022, 11, 5999. https://doi.org/10.3390/jcm11205999
Cantinotti M, Marchese P, Assanta N, Pizzuto A, Corana G, Santoro G, Franchi E, Viacava C, Van den Eynde J, Kutty S, et al. Lung Ultrasound Findings in Healthy Children and in Those Who Had Recent, Not Severe COVID-19 Infection. Journal of Clinical Medicine. 2022; 11(20):5999. https://doi.org/10.3390/jcm11205999
Chicago/Turabian StyleCantinotti, Massimiliano, Pietro Marchese, Nadia Assanta, Alessandra Pizzuto, Giulia Corana, Giuseppe Santoro, Eliana Franchi, Cecilia Viacava, Jef Van den Eynde, Shelby Kutty, and et al. 2022. "Lung Ultrasound Findings in Healthy Children and in Those Who Had Recent, Not Severe COVID-19 Infection" Journal of Clinical Medicine 11, no. 20: 5999. https://doi.org/10.3390/jcm11205999