
Soluble Urokinase Receptor as a Promising Marker for Early Prediction of Outcome in COVID-19 Hospitalized Patients


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
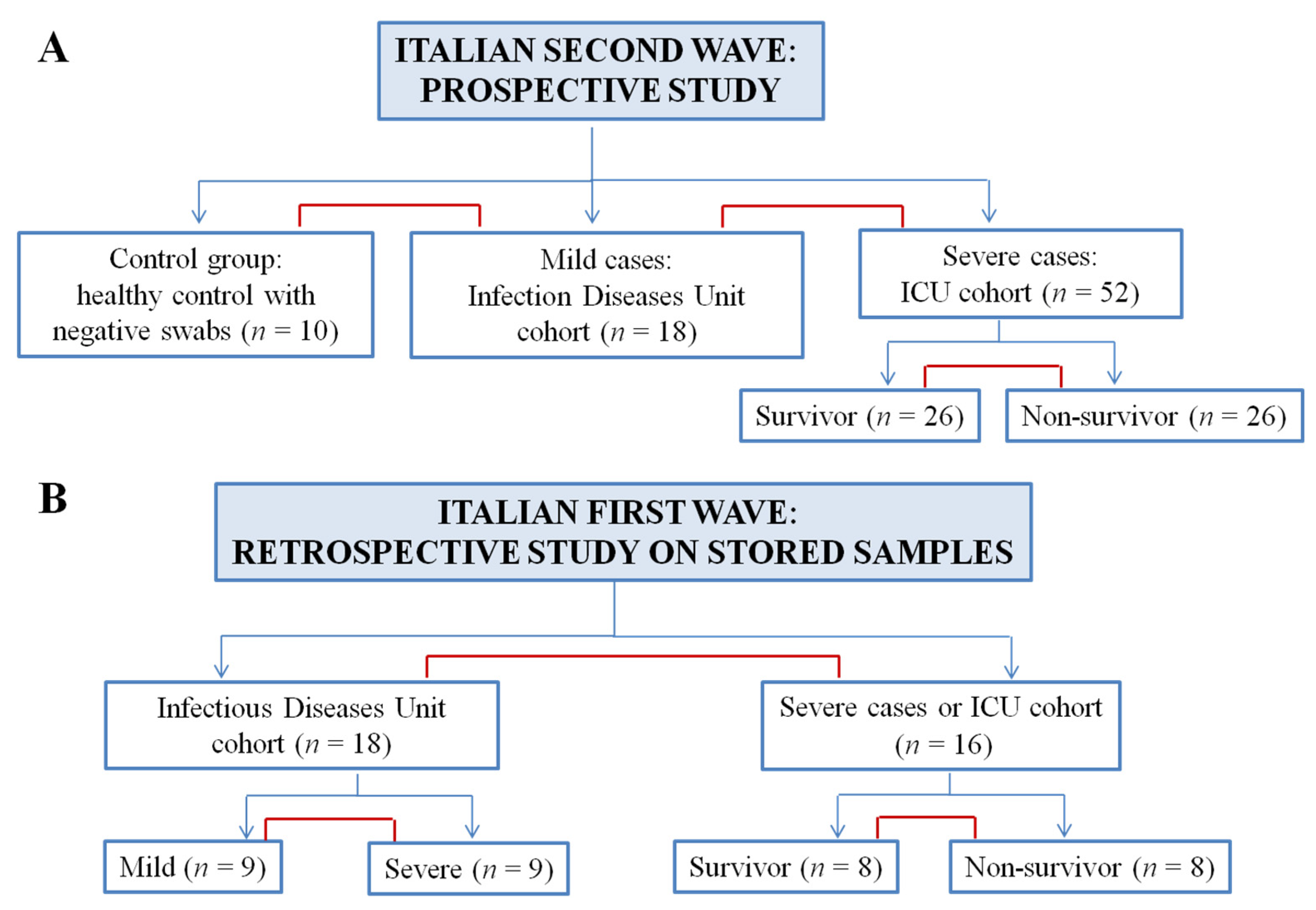
2.1. Study Participants and Study Design
2.2. SARS-CoV-2 Testing
2.3. Measurements Methods
2.4. Statistical Analysis
3. Results
3.1. Experimental Design and Patients’ Enrollment
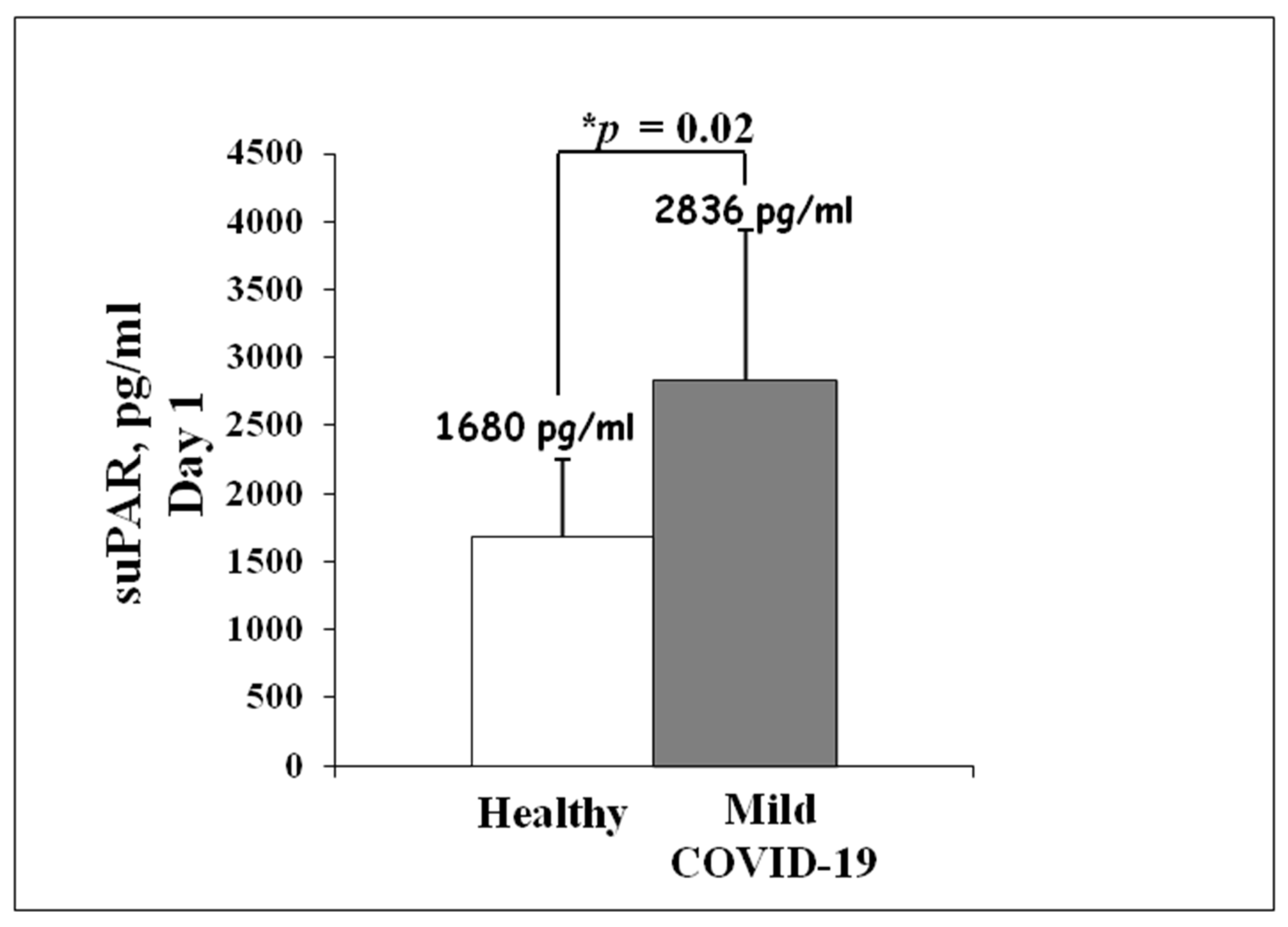
3.2. suPAR Serum Levels in Mild Cases of COVID-19 during Italian Second Wave
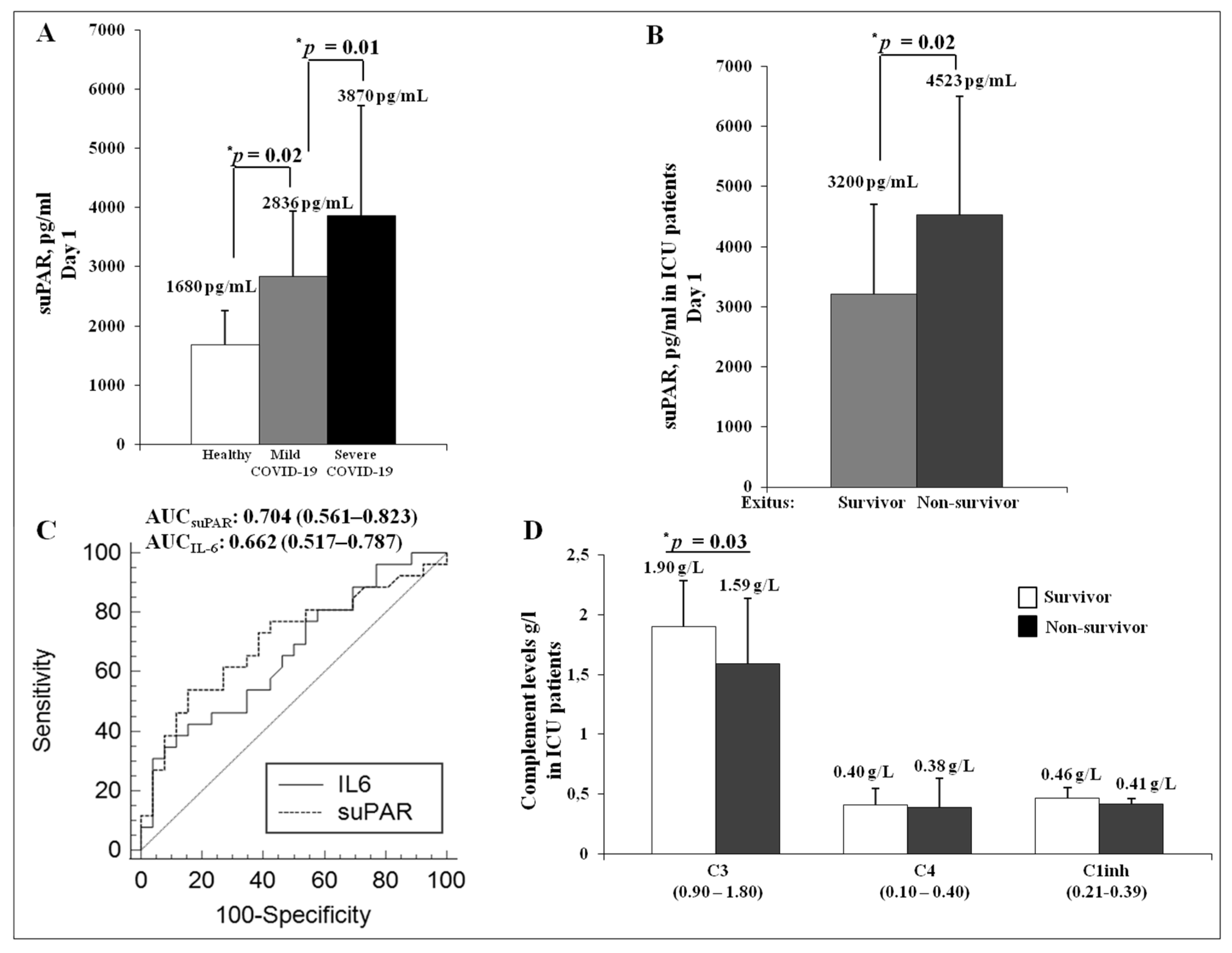
3.3. Presenting Characteristics and Analysis of suPAR Serum Levels in Severe Cases of COVID-19 during Italian Second Wave
3.4. Analysis of the Complement System in the ICU Cohort
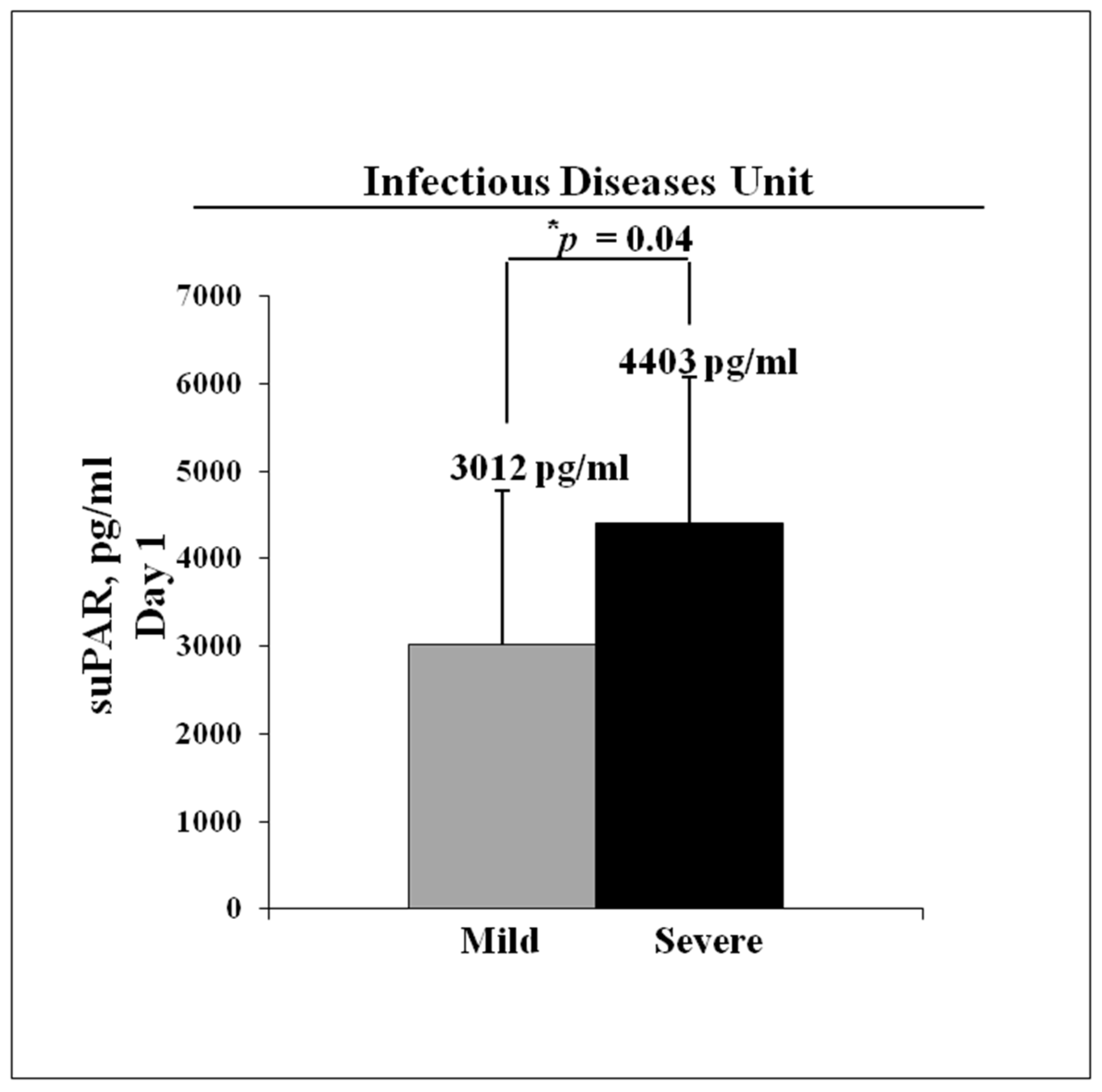
3.5. Retrospective Analysis of suPAR Serum Levels in Hospitalized COVID-19 Patients during Italian First Wave
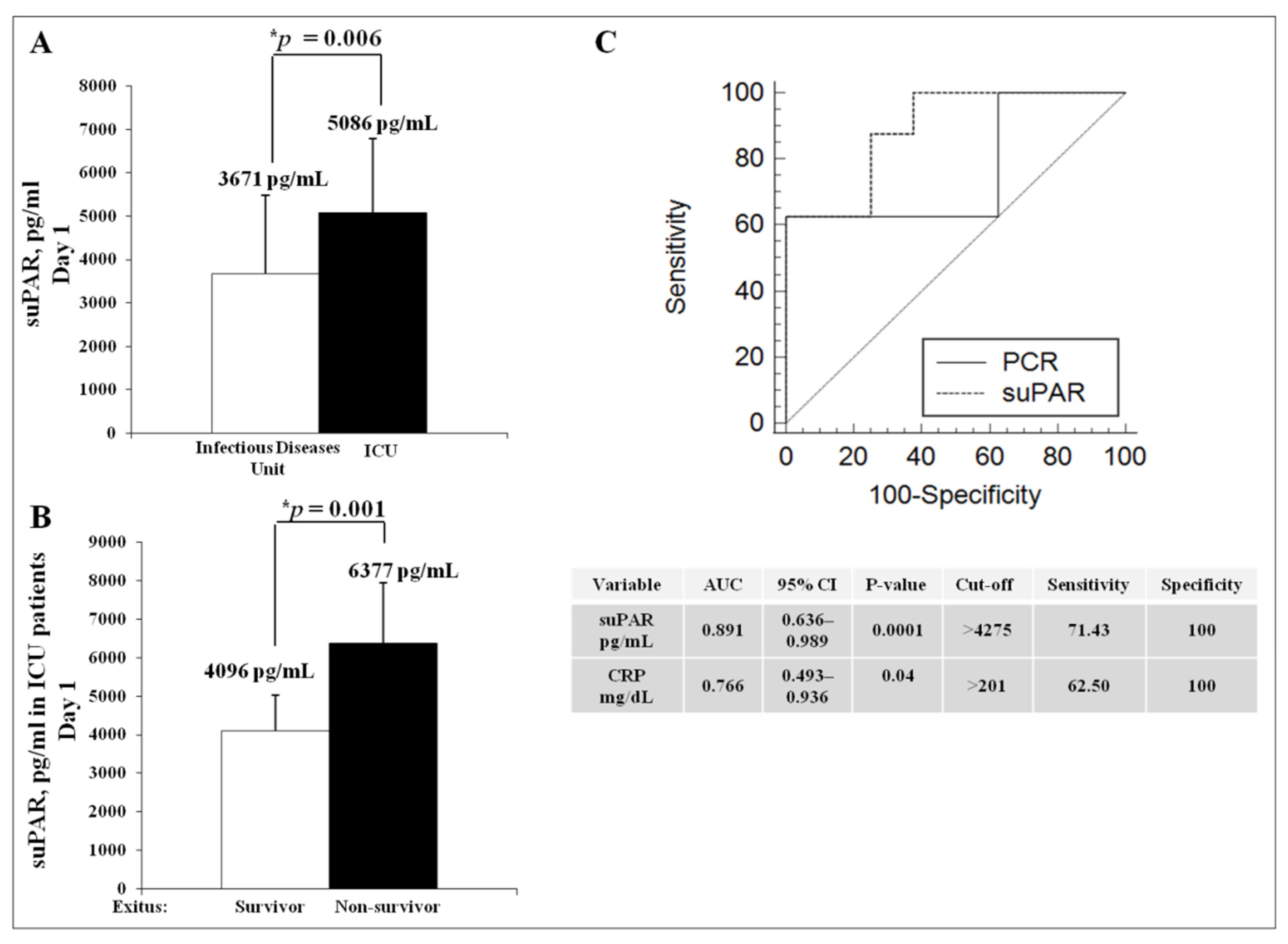
3.6. Retrospective Analysis of suPAR Serum Levels in Severe Cases of COVID-19 during Italian First Wave
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 pandemic: A global health crisis. Physiol. Genom. 2020, 52, 549–557. [Google Scholar]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dahal, S.; Kumar, D.; Kv, H. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [PubMed]
- Stephen, A.L.; Kyra, H.G.; Qifang, B.; Forrest, K.J.; Zheng, Q.; Hannah, R.M.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) from Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Guet, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: A systematic review and meta-analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 11, e201429. [Google Scholar]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients with COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef] [PubMed]
- Fara, A.; Mitrev, Z.; Rosalia, R.A.; Assas, B.M. Cytokine storm and COVID-19: A chronicle of pro-inflammatory cytokines. Open Biol. 2020, 10, 200160. [Google Scholar] [CrossRef]
- Di Spigna, G.; Spalletti Cernia, D.; Vargas, M.; Buonavolontà, L.; Servillo, G.; Postiglione, L. Drastically elevated levels of Interleukin-6 and its soluble receptor complex in COVID-19 patients with acute respiratory distress. Clin. Med. Investig. 2020. [Google Scholar] [CrossRef]
- Izcovich, A.; Ragusa, M.A.; Tortosa, F.; Marzio, M.A.L.; Agnoletti, C.; Bengolea, A.; Ceirano, A.; Espinosa, F.; Saavedra, E.; Sanguine, V.; et al. Prognostic factors for severity and mortality in patients infected with COVID-19: A systematic review. PLoS ONE 2020, 15, e0241955. [Google Scholar]
- Mahmood, N.; Mihalcioiu, C.; Rabbani, S.A. Multifaceted Role of the Urokinase-Type Plasminogen Activator (uPA) and Its Receptor (uPAR): Diagnostic, Prognostic, and Therapeutic Applications. Front. Oncol. 2018, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blasi, F.; Carmeliet, P. uPAR: A versatile signalling orchestrator. Nat. Rev. Mol. Cell Biol. 2002, 3, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.W.; Marshall, C.J. Regulation of cell signalling by uPAR. Nat. Rev. Mol. Cell Biol. 2010, 11, 23–36. [Google Scholar] [PubMed]
- Montuori, N.; Carriero, M.V.; Salzano, S.; Rossi, G.; Ragno, P. The cleavage of the urokinase receptor regulates its multiple functions. J. Biol. Chem. 2002, 277, 46932–46939. [Google Scholar] [CrossRef] [Green Version]
- Madsen, C.D.; Sidenius, N. The interaction between urokinase receptor and vitronectin in cell adhesion and signalling. Eur. J. Cell Biol. 2008, 87, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Degryse, B.; Resnati, M.; Czekay, R.P.; Loskutoff, D.J.; Blasi, F. Domain 2 of the urokinase receptor contains an integrin-interacting epitope with intrinsic signaling activity: Generation of a new integrin inhibitor. J. Biol. Chem. 2005, 280, 24792–24803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaurasia, P.; Aguirre-Ghiso, J.A.; Liang, O.D.; Gardsvoll, H.; Ploug, M.; Ossowski, L. A region in urokinase plasminogen receptor domain III controlling a functional association with α5β1 integrin and tumor growth. J. Biol. Chem. 2006, 281, 14852–14863. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Aguirre Ghiso, J.; Estrada, Y.; Ossowski, L. EGFR is a transducer of the urokinase receptor initiated signal that is required for in vivo growth of a human carcinoma. Cancer Cell 2002, 1, 445–457. [Google Scholar] [CrossRef] [Green Version]
- Kiyan, J.; Kiyan, R.; Haller, H.; Dumler, I. Urokinase-induced signaling in human vascular smooth muscle cells is mediated by PDGFR-beta. EMBO J. 2005, 24, 1787–1797. [Google Scholar] [CrossRef] [Green Version]
- Rossi, F.W.; Napolitano, F.; Pesapane, A.; Mascolo, M.; Staibano, S.; Matucci-Cerinic, M.; Guiducci, S.; Ragno, P.; di Spigna, G.; Postiglione, L.; et al. Upregulation of the N-Formyl Peptide Receptors in Scleroderma Fibroblasts Fosters the Switch to Myofibroblasts. J. Immunol. 2015, 194, 5161–5173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, F.; Rossi, F.W.; Pesapane, A.; Varricchio, S.; Ilardi, G.; Mascolo, M.; Staibano, S.; Lavecchia, A.; Ragno, P.; Selleri, C.; et al. N-Formyl Peptide Receptors Induce Radical Oxygen Production in Fibroblasts Derived from Systemic Sclerosis by Interacting with a Cleaved Form of Urokinase Receptor. Front. Immunol. 2018, 9, 574. [Google Scholar] [CrossRef] [Green Version]
- Thuno, M.; Macho, B.; Eugen-Olsen, J. suPAR: The molecular crystal ball. Dis. Markers 2009, 27, 157–172. [Google Scholar] [CrossRef]
- Rasmussen, L.J.H.; Ladelund, S.; Haupt, T.H.; Ellekilde, G.; Poulsen, J.H.; Iversen, K.; Eugen-Olsen, J.; Andersen, O. Soluble urokinase plasminogen activator receptor (suPAR) in acute care: A strong marker of disease presence and severity, readmission and mortality. A retrospective cohort study. Emerg. Med. J. 2016, 33, 769–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostrowski, S.R.; Ullum, H.; Goka, B.Q.; Hoyer-Hansen, G.; Obeng-Adjei, G.; Pedersen, B.K.; Akanmori, B.D.; Kurtzhals, J.A.L. Plasma concentrations of soluble urokinase-type plasminogen activator receptor are increased in patients with malaria and are associated with a poor clinical or a fatal outcome. J. Infect. Dis. 2005, 191, 1331–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eugen-Olsen, J.; Gustafson, P.; Sidenius, N.; Fischer, T.K.; Parner, J.; Aaby, P.; Gomes, V.F.; Lisse, I. The serum level of soluble urokinase receptor is elevated in tuberculosis patients and predicts mortality during treatment: A community study from Guinea-Bissau. Int. J. Tuberc. Lung Dis. 2002, 6, 686–692. [Google Scholar] [PubMed]
- Ostrowski, S.R.; Piironen, T.; Hoyer-Hansen, G.; Gerstoft, J.; Pedersen, B.K.; Ullum, H. Reduced release of intact and cleaved urokinase receptor in stimulated whole-blood cultures from human immunodeficiency virus-1-infected patients. Scand. J. Immunol. 2005, 61, 347–356. [Google Scholar] [CrossRef]
- Freeley, S.; Kemper, C.; Le Friec, G. The ‘Ins and Outs’ of complement-driven immune responses. Immunol. Rev. 2016, 274, 16–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajic, G.; Degn, S.E.; Thiel, S.; Andersen, G.R. Complement activation, regulation, and molecular basis for complement-related diseases. EMBO J. 2015, 34, 2735–2757. [Google Scholar] [CrossRef] [Green Version]
- Peng, Q.; Li, K.; Sacks, S.H.; Zhou, W. The Role of Anaphylatoxins C3a and C5a in Regulating Innate and Adaptive Immune Responses. Inflamm. Allergy-Drug Targets 2009, 8, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Risitano, A.M.; Mastellos, D.C.; Huber-Lang, M.; Yancopoulou, D.; Garlanda, C.; Ciceri, F.; Lambris, J.D. Complement as a target in COVID-19? Nat. Rev. Immunol. 2020, 20, 448. [Google Scholar] [CrossRef]
- Gralinski, L.E.; Sheahan, T.P.; Morrison, T.E.; Menachery, V.D.; Jensen, K.; Leist, S.R. Complement Activation Contributes to Severe Acute Respiratory Syndrome Coronavirus Pathogenesis. mBio 2018, 9, e01753-18. [Google Scholar] [CrossRef] [Green Version]
- Polycarpou, A.; Howard, M.; Farrar, C.A.; Greenlaw, R.; Fanelli, G.; Wallis, R.; Klavinskis, L.S.; Sacks, S. Rationale for targeting complement in COVID-19. EMBO Mol. Med. 2020, 12, e12642. [Google Scholar] [PubMed]
- Java, A.; Apicelli, A.J.; Liszewski, M.K.; Coler-Reilly, A.; Atkinson, J.P.; Kim, A.H.; Kulkarni, H.S. The complement system in COVID-19: Friend and foe? JCI Insight 2020, 5, e140711. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, F.; Montuori, N. The Role of the Plasminogen Activation System in Angioedema: Novel Insights on the Pathogenesis. J. Clin. Med. 2021, 10, 518. [Google Scholar] [CrossRef]
- .Wang, J.; Cai, K.; Zhang, R.; He, X.; Shen, X.; Liu, J.; Xu, J.; Qiu, F.; Lei, W.; Wang, J.; et al. Novel one-step single-tube nested quantitative real-time PCR assay for highly sensitive detection of SARS-CoV-2. Anal. Chem. 2020, 92, 9399–9404. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S. Remdesivir for the Treatment of COVID-19-Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Favaloro, E.J. Elevated soluble urokinase plasminogen activator receptor (suPAR) in COVID-19 patients. Clin. Chem. Lab. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Giudice, V.; Pagliano, P.; Vatrella, A.; Masullo, A.; Poto, S.; Polverino, B.M.; Gammaldi, R.; Maglio, A.; Sellitto, C.; Vitale, C.; et al. Combination of Ruxolitinib and Eculizumab for Treatment of Severe SARS-CoV-2-Related Acute Respiratory Distress Syndrome: A Controlled Study. Front. Pharmacol. 2020, 11, 857. [Google Scholar] [CrossRef]
- Vitiello, A.; La Porta, R.; D’Aiuto, V.; Ferrara, F. Pharmacological approach for the reduction of inflammatory and prothrombotic hyperactive state in COVID-19 positive patients by acting on complement cascade. Hum. Immunol. 2021, 82, 264–269. [Google Scholar] [CrossRef] [PubMed]
- D’Alonzo, D.; De Fenza, M.; Pavone, V. COVID-19 and pneumonia: A role for the uPA/uPAR system. Drug Discov. Today 2020, 25, 1528–1534. [Google Scholar]
- Rovina, N.; Akinosoglou, K.; Eugen-Olsen, J.; Hayek, S.; Reiser, J.; Giamarellos-Bourboulis, E.J. Soluble urokinase plasminogen activator receptor (suPAR) as an early predictor of severe respiratory failure in patients with COVID-19 pneumonia. Crit. Care 2020, 24, 187. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, A.; Mouzarou, A.; Samara, E.; Xanthos, T.; Ischaki, E.; Pantazopoulos, I. Soluble Urokinase Plasminogen Activator Receptor: A Biomarker for Predicting Complications and Critical Care Admission of COVID-19 Patients. Mol. Diagn. Ther. 2020, 24, 517–521. [Google Scholar] [CrossRef]
- Azam, T.U.; Shadid, H.R.; Blakely, P.; O’Hayer, P.; Berlin, H.; Pan, M.; Zhao, P.; Zhao, L.; Pennathur, S.; Pop-Busui, R.; et al. Soluble Urokinase Receptor (SuPAR) in COVID-19-Related AKI. J. Am. Soc. Nephrol. 2020, 31, 2725–2735. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort (n = 18) | Healthy (n = 10) | p-Value * | |
|---|---|---|---|
| Clinical characteristics: | |||
| Age, average (SD) | 59 (16) | 55 (12) | 0.228 |
| Male, n (%) | 14 (77) | 2 (10) | 0.005 * |
| Clinical Status Ordinal Scale | 3.8 (1.15) | ||
| Diabetes, n (%) | 2 (11) | ||
| Chronic heart failure, n (%) | 1 (5.5) | ||
| Chronic kidney disease, n (%) | - | ||
| Died | 0 | ||
| Laboratory findings, average (SD): | |||
| CRP, mg/dL | 6.75 (6.4) | ||
| Procalcitonin, ng/mL | 0.15 (0.15) | ||
| IL-6, pg/mL | 63.7 (84) | 3.0 (0.80) | 0.003 * |
| suPAR, pg/mL | 2836 (1102) | 1680 (567) | 0.02 * |
| ICU Cohort (n = 52) | Survivors (n = 26) | Non-Survivors (n = 26) | p-Value * | |
|---|---|---|---|---|
| Clinical characteristics: | ||||
| Age, average (SD) | 70 (11) | 64 (12) | 72 (9.8) | 0.008 * |
| Male, n (%) | 43 (82) | 20 (76) | 23 (88) | 0.465 |
| Charlson’s comorbidity index (DS) | 4.3 (3.1) | 3.3 (3) | 5.3 (2.9) | 0.01 * |
| Diabetes, n (%) | 11 (21) | 5 (19) | 6 (23) | 1.000 |
| Hypertension, n (%) | 33 (63) | 17 (65) | 16 (61) | 1.000 |
| Chronic heart failure, n (%) | 1 (1.9) | - | 1 (3.8) | 1.000 |
| Chronic kidney disease, n (%) | 11 (21) | 2 (7.6) | 9 (34) | 0.008 * |
| Laboratory findings, average (SD): | ||||
| CRP, mg/dL | 119 (92) | 99.9 (88) | 139 (93) | 0.06 |
| Procalcitonin, ng/mL | 10.2 (41) | 6.7 (27.3) | 13.7 (51.6) | 0.271 |
| IL-6, pg/mL | 65.9 (92) | 41.6 (44) | 73.2 (120) | 0.02 * |
| suPAR pg/mL | 3870 (567) | 3200 (1488) | 4523 (1976) | 0.004 * |
| Cohort (n = 18) | Mild (n = 9) | Severe (n = 9) | p-Value * | |
|---|---|---|---|---|
| Clinical characteristics: | ||||
| Age, average (SD) | 69 (16) | 65 (17) | 73 (15) | 0.149 |
| Male, n (%) | 16 (88) | 8 (89) | 8 (89) | 1.000 |
| Clinical Status Ordinal Scale | 5 (1.10) | 4.6 (0.7) | 5.5 (1.1) | 0.03 * |
| Diabetes, n (%) | 7 (39) | 4 (44) | 3 (33) | 1.000 |
| Chronic heart failure, n (%) | 3 (17) | 2 (22) | 1 (11) | 1.000 |
| Died, n (%) | 3 (11) | - | 3 (33) | 0.165 |
| Laboratory findings, average (SD): | ||||
| CRP, mg/dL | 8.5 (7.5) | 12.42 (8.8) | 3.4 (1.7) | 0.004 * |
| Procalcitonin, ng/mL | 0.25 (0.52) | 0.29 (0.65) | 0.10 (0.13) | 0.196 |
| IL-6, pg/mL | 254 (690) | 138 (341) | 371 (931) | 0.245 |
| suPAR, pg/mL | 3671 (1817) | 3012 (1766) | 4403 (1665) | 0.04 * |
| ICU Cohort (n = 16) | Survivors (n = 8) | Non-Survivors (n = 8) | p-Value * | |
|---|---|---|---|---|
| Clinical characteristics: | ||||
| Age, average (SD) | 65 (13) | 61 (12) | 69 (14) | 0.121 |
| Male, n (%) | 13 (82) | 6 (75) | 7 (87.5) | 1.000 |
| Diabetes, n (%) | 3 (18.7) | 1 (12.5) | 2 (25) | 1.000 |
| Hypertension, n (%) | 8 (50) | 6 (75) | 2 (25) | 0.066 |
| Chronic heart failure, n (%) | 6 (37.5) | 3 (37.5) | 3 (37.5) | 1.000 |
| Chronic kidney disease, n (%) | 2 (12.5) | - | 2 (25) | 0.233 |
| Laboratory findings, average (SD): | ||||
| CRP, mg/dL | 192 (102) | 138 (48) | 246 (116) | 0.01 * |
| IL-6, pg/mL | 85.25 (53) | 96.37 (66) | 74.13 (37) | 0.184 |
| suPAR, pg/mL | 5086 (1709) | 4096 (935) | 6377 (1555) | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Napolitano, F.; Di Spigna, G.; Vargas, M.; Iacovazzo, C.; Pinchera, B.; Spalletti Cernia, D.; Ricciardone, M.; Covelli, B.; Servillo, G.; Gentile, I.; et al. Soluble Urokinase Receptor as a Promising Marker for Early Prediction of Outcome in COVID-19 Hospitalized Patients. J. Clin. Med. 2021, 10, 4914. https://doi.org/10.3390/jcm10214914
Napolitano F, Di Spigna G, Vargas M, Iacovazzo C, Pinchera B, Spalletti Cernia D, Ricciardone M, Covelli B, Servillo G, Gentile I, et al. Soluble Urokinase Receptor as a Promising Marker for Early Prediction of Outcome in COVID-19 Hospitalized Patients. Journal of Clinical Medicine. 2021; 10(21):4914. https://doi.org/10.3390/jcm10214914
Chicago/Turabian StyleNapolitano, Filomena, Gaetano Di Spigna, Maria Vargas, Carmine Iacovazzo, Biagio Pinchera, Daniela Spalletti Cernia, Margherita Ricciardone, Bianca Covelli, Giuseppe Servillo, Ivan Gentile, and et al. 2021. "Soluble Urokinase Receptor as a Promising Marker for Early Prediction of Outcome in COVID-19 Hospitalized Patients" Journal of Clinical Medicine 10, no. 21: 4914. https://doi.org/10.3390/jcm10214914