
Effect of Different Corticosteroid Regimens on the Outcome of Severe COVID-19-Related Acute Respiratory Failure. A Retrospective Analysis

 , ,
, ,
Abstract
:Highlights
- The exact type and dose of corticosteroid to be used in critically ill patients with COVID-19-related acute hypoxemic respiratory failure has not yet been established.
- In a retrospective trial, we were unable to find any difference between dexamethasone and methylprednisolone at standard doses in patient-centered outcomes. High-dose boluses of methylprednisolone were associated with a worse prognosis.
- The beneficial effects seen in critically ill COVID-19 patients treated with corticosteroids might be a class effect. High-dose, rescue boluses seemed harmful.
1. Quick Look
1.1. Current Knowledge
1.2. What This Paper Contributes to Our Knowledge
2. Introduction
3. Methods
3.1. Ethics
3.2. Study Design
3.3. Enrolment Criteria
3.4. Management of Critically Ill Subjects
3.5. Data Collection
3.6. Corticosteroid Regimens
3.7. Outcomes
3.8. Statistical Analysis
4. Results
5. Discussion
5.1. Inflammation and COVID-19
5.2. Corticosteroids and COVID-19
5.3. Case Mix
5.4. Dexamethasone vs. Methylprednisolone
5.5. Usual Care vs. Rescue Boluses
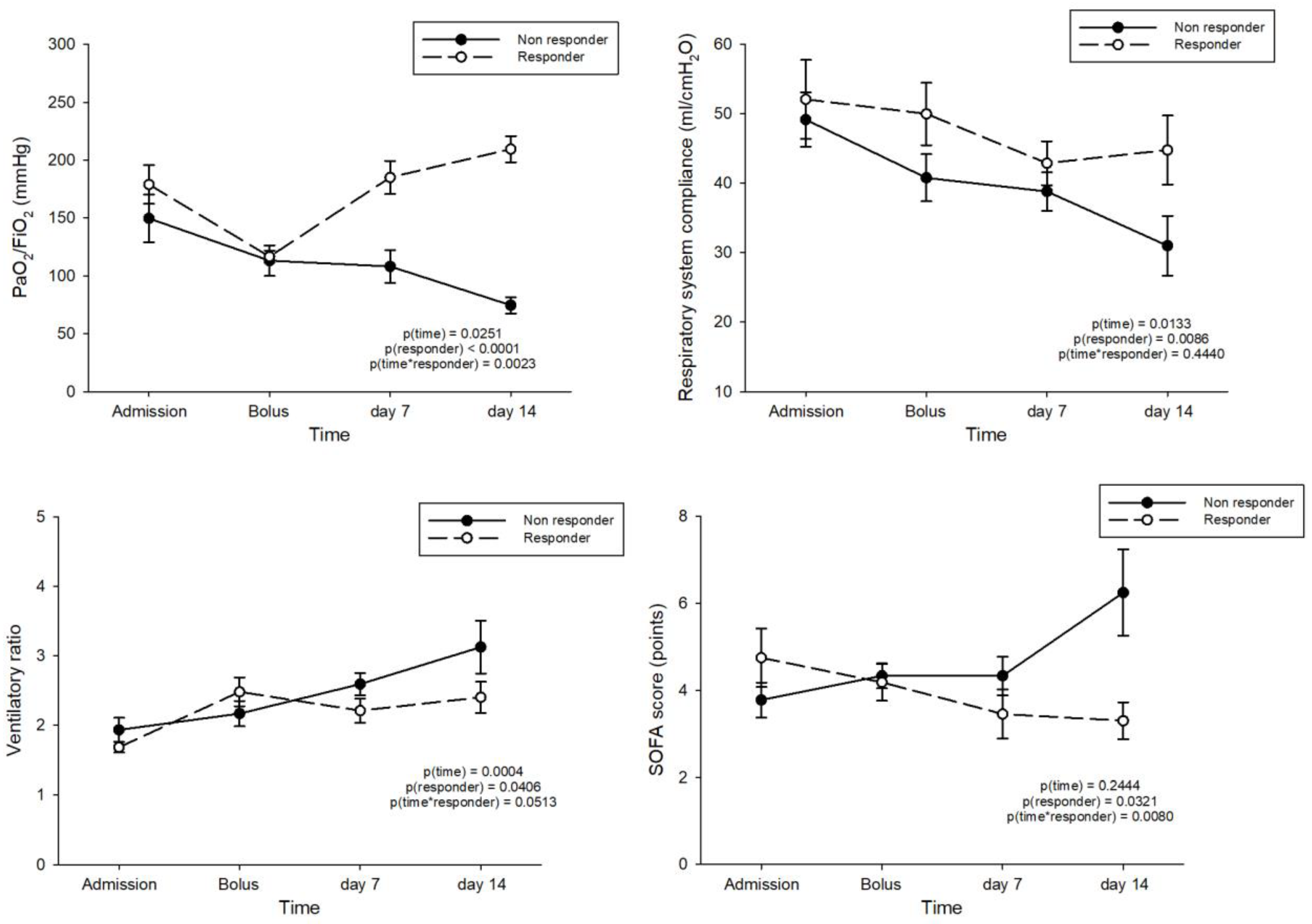
5.6. Responders and Non-Responders to the High-Dose, Rescue Bolus of Corticosteroids
5.7. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America guidelines on the treatment and management of patients with COVID-19. Clinical Infectious Diseases. 2020 Apr 27. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Prescott, H.C.; Rice, T.W. Corticosteroids in COVID-19 ARDS: Evidence and Hope During the Pandemic. JAMA 2020, 324, 1292–1295. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Chrousos, G.P.; Meduri, G.U. The ten reasons why corticosteroid therapy reduces mortality in severe COVID-19. Intensive Care Med. 2020, 46, 2067–2070. [Google Scholar] [CrossRef]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Bruggen, M.C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Angus, D.C.; Derde, L.; Al-Beidh, F.; Annane, D.; Arabi, Y.; Beane, A.; van Bentum-Puijk, W.; Berry, L.; Bhimani, Z.; Bonten, M.; et al. Effect of Hydrocortisone on Mortality and Organ Support in Patients With Severe COVID-19: The REMAP-CAP COVID-19 Corticosteroid Domain Randomized Clinical Trial. JAMA 2020, 324, 1317–1329. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef]
- Dequin, P.F.; Heming, N.; Meziani, F.; Plantefeve, G.; Voiriot, G.; Badie, J.; Francois, B.; Aubron, C.; Ricard, J.D.; Ehrmann, S.; et al. Effect of Hydrocortisone on 21-Day Mortality or Respiratory Support Among Critically Ill Patients With COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Recovery Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- W. H. O. Rapid Evidence Appraisal for COVID-19 Therapies Working Group; Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Kolilekas, L.; Loverdos, K.; Giannakaki, S.; Vlassi, L.; Levounets, A.; Zervas, E.; Gaga, M. Can steroids reverse the severe COVID-19 induced “cytokine storm”? J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- So, C.; Ro, S.; Murakami, M.; Imai, R.; Jinta, T. High-dose, short-term corticosteroids for ARDS caused by COVID-19: A case series. Respirol. Case Rep. 2020, 8, e00596. [Google Scholar] [CrossRef]
- Callejas Rubio, J.L.; Luna Del Castillo, J.D.; de la Hera Fernandez, J.; Guirao Arrabal, E.; Colmenero Ruiz, M.; Ortego Centeno, N. Effectiveness of corticoid pulses in patients with cytokine storm syndrome induced by SARS-CoV-2 infection. Med. Clin. 2020, 155, 159–161. [Google Scholar] [CrossRef]
- Villar, J.; Ferrando, C.; Martinez, D.; Ambros, A.; Munoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; Gonzalez-Higueras, E.; Conesa, L.A.; et al. Dexamethasone treatment for the acute respiratory distress syndrome: A multicentre, randomised controlled trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- Annane, D.; Pastores, S.M.; Rochwerg, B.; Arlt, W.; Balk, R.A.; Beishuizen, A.; Briegel, J.; Carcillo, J.; Christ-Crain, M.; Cooper, M.S.; et al. Guidelines for the diagnosis and management of critical illness-related corticosteroid insufficiency (CIRCI) in critically ill patients (Part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Intensive Care Med. 2017, 43, 1751–1763. [Google Scholar] [CrossRef]
- Ho, J.C.; Ooi, G.C.; Mok, T.Y.; Chan, J.W.; Hung, I.; Lam, B.; Wong, P.C.; Li, P.C.; Ho, P.L.; Lam, W.K.; et al. High-dose pulse versus nonpulse corticosteroid regimens in severe acute respiratory syndrome. Am. J. Respir. Crit. Care Med. 2003, 168, 1449–1456. [Google Scholar] [CrossRef]
- Foti, G.; Giannini, A.; Bottino, N.; Castelli, G.P.; Cecconi, M.; Grasselli, G.; Guatteri, L.; Latronico, N.; Langer, T.; Monti, G.; et al. Management of critically ill patients with COVID-19: Suggestions and instructions from the coordination of intensive care units of Lombardy. Minerva Anestesiol. 2020, 86, 1234–1245. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Calfee, C.S.; Beitler, J.R.; Soni, N.; Ho, K.; Matthay, M.A.; Kallet, R.H. Physiologic Analysis and Clinical Performance of the Ventilatory Ratio in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2019, 199, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical Characteristics of Covid-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Joly, B.S.; Siguret, V.; Veyradier, A. Understanding pathophysiology of hemostasis disorders in critically ill patients with COVID-19. Intensive Care Med. 2020, 46, 1603–1606. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Wartha, F.; Beiter, K.; Normark, S.; Henriques-Normark, B. Neutrophil extracellular traps: Casting the NET over pathogenesis. Curr. Opin. Microbiol. 2007, 10, 52–56. [Google Scholar] [CrossRef]
- Radic, M.; Marion, T.N. Neutrophil extracellular chromatin traps connect innate immune response to autoimmunity. Semin. Immunopathol. 2013, 35, 465–480. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, B.; Massberg, S. Thrombosis as an intravascular effector of innate immunity. Nat. Rev. Immunol. 2013, 13, 34–45. [Google Scholar] [CrossRef]
- Vargas, A.; Boivin, R.; Cano, P.; Murcia, Y.; Bazin, I.; Lavoie, J.P. Neutrophil extracellular traps are downregulated by glucocorticosteroids in lungs in an equine model of asthma. Respir. Res. 2017, 18, 207. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Lee, H.K. Re-analysis of Single Cell Transcriptome Reveals That the NR3C1-CXCL8-Neutrophil Axis Determines the Severity of COVID-19. Front. Immunol. 2020, 11, 2145. [Google Scholar] [CrossRef]
- Meduri, G.U.; Annane, D.; Chrousos, G.P.; Marik, P.E.; Sinclair, S.E. Activation and regulation of systemic inflammation in ARDS: Rationale for prolonged glucocorticoid therapy. Chest 2009, 136, 1631–1643. [Google Scholar] [CrossRef]
- Russell, C.D.; Millar, J.E.; Baillie, J.K. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet 2020, 395, 473–475. [Google Scholar] [CrossRef] [Green Version]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit. Care Med. 2020, 48, e440–e469. [Google Scholar] [CrossRef]
- Lee, N.; Allen Chan, K.C.; Hui, D.S.; Ng, E.K.; Wu, A.; Chiu, R.W.; Wong, V.W.; Chan, P.K.; Wong, K.T.; Wong, E.; et al. Effects of early corticosteroid treatment on plasma SARS-associated Coronavirus RNA concentrations in adult patients. J. Clin. Virol. 2004, 31, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Mandourah, Y.; Al-Hameed, F.; Sindi, A.A.; Almekhlafi, G.A.; Hussein, M.A.; Jose, J.; Pinto, R.; Al-Omari, A.; Kharaba, A.; et al. Corticosteroid Therapy for Critically Ill Patients with Middle East Respiratory Syndrome. Am. J. Respir. Crit. Care Med. 2018, 197, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.K.; Wong, D.A.; Tong, L.K.; Ip, S.M.; Lo, A.C.; Lau, C.S.; Yeung, E.Y.; Lim, W.W. Viral shedding patterns of coronavirus in patients with probable severe acute respiratory syndrome. Lancet 2004, 363, 1699–1700. [Google Scholar] [CrossRef] [Green Version]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Vergano, M.; Bertolini, G.; Giannini, A.; Gristina, G.R.; Livigni, S.; Mistraletti, G.; Riccioni, L.; Petrini, F. SIAARTI recommendations for the allocation of intensive care treatments in exceptional, resource-limited circumstances. Minerva Anestesiol. 2020, 86, 469–472. [Google Scholar] [CrossRef]


{kind=link}
| Dexamethasone (N = 51) | Methylprednisolone (N = 29) | p | |
|---|---|---|---|
| Male sex—n (%) | 44 (86.3) | 24 (82.8) | 0.6720 |
| Age—years | 58 ± 9 | 64 ± 9 | 0.0154 |
| Height (cm) | 172 ± 7 | 173 ± 8 | 0.7017 |
| Actual body weight (kg) | 82 ± 16 | 80 ± 18 | 0.6178 |
| Body mass index (kg/m2) | 27.7 ± 5.3 | 26.8 ± 5.2 | 0.4522 |
| Predicted body weight (kg) | 67 ± 6 | 67 ± 6 | 0.7249 |
| SAPS II score | 26 ± 6 | 28 ± 8 | 0.2515 |
| SOFA score | 5 [3; 7] | 3 [2; 4] | 0.0057 |
| Frailty score | 2 [2; 2] | 2 [2; 3] | 0.0921 |
| Comorbidities—n (%) | |||
| Hypertension | 17 (33.3) | 13 (44.8) | 0.3101 |
| Diabetes | 6 (11.8) | 4 (13.8) | 0.7982 |
| Obesity | 14 (27.5) | 4 (13.8) | 0.1545 |
| COPD | 3 (5.9) | 1 (3.4) | 0.0990 |
| Duration of symptoms before hospitalization (days) | 7 [5; 10] | 7 [5; 10] | 0.6324 |
| CPAP before ICU admission—n (%) | 47 (92.2) | 25 (86.2) | 0.3945 |
| Prone position during CPAP—n (%) | 24 (47.1) | 13 (44.8) | 0.8471 |
| Duration of CPAP before intubation (days) | 2 [1; 4] | 3 [1; 6] | 0.1232 |
| Prone positioning during ICU stay—n (%) | 24 (47.0) | 10 (34.5) | 0.274 |
| Tracheostomy—n (%) | 17 (33.3) | 9 (31.0) | 0.8330 |
| Administration of tocilizumab—n (%) | 12 (23.5) | 10 (34.5) | 0.2927 |
| Biochemistry at ICU admission | |||
| Procalcitonin (μg/L) | 0.53 [0.21; 1.12] | 0.26 [0.13; 0.53] | 0.0445 |
| C-reactive protein (mg/L) | 17.4 [10.9; 24.9] | 12.1 [6.3; 17.1] | 0.0084 |
| Fibrinogen (mg/100 mL) | 680 [610; 770] | 660 [514; 747] | 0.5111 |
| D-dimer (ng/mL) | 2270 [813; 4085] | 1225 [712; 5051] | 0.6794 |
| Haemoglobin (g/dL) | 11.4 ± 1.9 | 11.2 ± 1.7 | 0.6765 |
| Platelet count (1/mm3) | 278,156 ± 11,3686 | 263,714 ± 88,567 | 0.5625 |
| White blood cell (1/mm3) | 9709 ± 4212 | 8429 ± 3605 | 0.1786 |
| Creatinine (mg/dL) | 0.83 ± 0.37 | 0.86 ± 0.32 | 0.8162 |
| Bilirubin (mg/dL) | 0.72 [0.49; 1.14] | 0.55 [0.39; 0.72] | 0.0334 |
| Interleukin-6 (ng/L) | 88 [8; 198] | 78 [26; 159] | 0.9176 |
| Mechanical ventilation and gas exchange at ICU admission | |||
| Respiratory system compliance (ml/cmH2O) | 50.8 ± 15.6 | 47.6 ± 14.4 | 0.3884 |
| Airway driving pressure (cmH2O) | 10 [8; 12] | 11 [9; 13] | 0.1734 |
| Airway plateau pressure (cmH2O) | 24 [22; 26] | 24 [23; 28] | 0.7076 |
| PEEP (cmH2O) | 14 [14; 15] | 14 [13; 15] | 0.1281 |
| Tidal volume (mL) | 492 ± 53 | 491 ± 52 | 0.9457 |
| Tidal volume (mL/kg abw) | 7.4 ± 0.9 | 7.4 ± 0.7 | 0.9191 |
| Respiratory rate (1/min) | 20 ± 3 | 19 ± 3 | 0.5045 |
| FiO2 (%) | 70.9 ± 13.5 | 69.6 ± 17.7 | 0.7247 |
| pH | 7.36 ± 0.09 | 7.37 ± 0.07 | 0.5994 |
| PaO2 (mmHg) | 129.6 ± 46.9 | 135.6 ± 59.8 | 0.6314 |
| PaCO2 (mmHg) | 51.2 ± 12.8 | 46.2 ± 8.5 | 0.0777 |
| PaO2/FiO2 (mmHg) | 188.6 ± 75.1 | 201.3 ± 74.5 | 0.4863 |
| Ventilatory ratio | 1.9 [1.5; 2.3] | 1.6 [1.3; 2.0] | 0.0451 |
| Dexamethasone (N = 51) | Methylprednisolone (N = 29) | p | p * | |
|---|---|---|---|---|
| Primary outcome: | ||||
| Length of ICU stay (days) | 13 [7; 21] | 11 [6; 22] | 0.869 | 0.272 |
| Secondary outcomes: | ||||
| Duration of mechanical ventilation (days) | 13 [8; 18] | 10 [6; 22] | 0.572 | 0.418 |
| Length of hospital stay (days) | 23 [16; 31] | 27 [19; 40] | 0.101 | 0.009 |
| Ventilator-free days (days) | 0 [0; 19] | 15 [0; 20] | 0.148 | 0.931 |
| ICU mortality—n (%) | 22 (43.1) | 11 (37.9) | 0.649 | 0.789 |
| Hospital mortality—n (%) | 26 (60.0) | 11 (37.9) | 0.260 | 0.954 |
| Patients who developed VAP—n (%) | 25 (49.0) | 15 (51.7) | 0.816 | 0.153 |
| Number of VAP per patient | 1 [1; 2] | 2 [2; 3] | 0.006 | 0.046 |
| Patients who developed bacteremia—n (%) | 20 (39.2) | 10 (34.5) | 0.674 | 0.899 |
| Number of bacteremias per patient | 2 [1; 2] | 1 [1; 2] | 0.770 | 0.287 |
| High-dose rescue boluses of methylprednisolone—n (%) | 14 (27.5) | 8 (27.6) | 0.990 | 0.908 |
| No Boluses (N = 59) | Rescue Boluses (N = 22) | p | |
|---|---|---|---|
| Male sex–n (%) | 50 (84.8) | 19 (86.4) | 0.8552 |
| Age (years) | 60 ± 10 | 61 ± 8 | 0.9370 |
| Height (cm) | 173 ± 8 | 172 ± 5 | 0.5460 |
| Actual body weight (kg) | 81 ± 18 | 83 ± 15 | 0.6079 |
| Body mass index (kg/m2) | 27.1 ± 5.3 | 28.3 ± 5.1 | 0.3589 |
| Predicted body weight (kg) | 67 ± 6 | 66 ± 4 | 0.5597 |
| SAPS II score | 27.1 ± 6.8 | 26.3 ± 6.7 | 0.6316 |
| SOFA score | 4 [3; 6] | 4 [3; 7] | 0.8614 |
| Frailty score | 2 [2; 3] | 2 [2; 2] | 0.6307 |
| Comorbidities–n (%) | |||
| Hypertension | 22 (39.3) | 8 (36.4) | 0.8110 |
| Diabetes | 9 (16.1) | 2 (9.1) | 0.4250 |
| Obesity | 12 (21.4) | 6 (27.3) | 0.5811 |
| COPD | 2 (3.6) | 2 (9.1) | 0.3203 |
| Duration of symptoms before hospitalization (days) | 7 [5; 10] | 7 [5; 10] | 0.7977 |
| CPAP before ICU admission–n (%) | 51 (86.4) | 22 (100) | 0.0696 |
| Prone position during CPAP–n (%) | 26 (44.1) | 11 (50) | 0.6347 |
| Duration of CPAP before intubation (days) | 3 [1; 4] | 3 [1; 5] | 0.3951 |
| Prone positioning during ICU stay–n (%) | 26 (44.0) | 8 (36.4) | 0.532 |
| Tracheostomy–n (%) | 19 (32.2) | 7 (31.8) | 0.9743 |
| Type of corticosteroid drug–n (%) | |||
| Dexamethasone | 37 (62.7) | 14 (63.6) | 0.8284 |
| Methylprednisolone | 21 (35.6) | 8 (36.4) | |
| No corticosteroids | 1 (1.7) | 0 | |
| Aministration of tocilizumab–n (%) | 14 (23.7) | 8 (36.4) | 0.2555 |
| Biochemistry at ICU admission | |||
| Procalcitonin (μg/L) | 0.42 [0.18; 0.87] | 0.36 [0.15; 0.90] | 0.6940 |
| C-reactive protein (mg/L) | 13.9 [8.5; 20.5] | 17.7 [13.2; 23.6] | 0.2380 |
| Fibrinogen (mg/100 mL) | 664 [587; 747] | 685 [619; 786] | 0.3774 |
| D-dimer (ng/mL) | 1568 [775; 4314] | 2419 [712; 4546] | 0.4282 |
| Haemoglobin (g/dL) | 11.2 ± 1.9 | 11.7 ± 1.6 | 0.2940 |
| Platelet count (1/mm3) | 279,913 ± 112,359 | 254,818 ± 79,324 | 0.3405 |
| White blood cell (1/mm3) | 9442 ± 4228 | 8746 ± 3389 | 0.4913 |
| Creatinine (mg/dL) | 0.84 ± 0.34 | 0.88 ± 0.41 | 0.6075 |
| Bilirubin (mg/dL) | 0.7 [0.4; 1.1] | 0.6 [0.4; 0.7] | 0.1644 |
| Interleukin-6 (ng/L) | 58 [20; 142] | 198 [91; 264] | 0.0258 |
| Respiratory mechanics and gas exchange at ICU admission | |||
| Respiratory system compliance (ml/cmH2O) | 49.8 ± 15.1 | 50.4 ± 16.1 | 0.8713 |
| Airway driving pressure (cmH2O) | 10 [8; 12] | 11 [9; 12] | 0.4195 |
| Airway plateau pressure (cmH2O) | 24 [22; 27] | 25 [24; 26] | 0.2378 |
| PEEP (cmH2O) | 14 [12; 15] | 14 [14; 14] | 0.9575 |
| Tidal volume (mL) | 487 ± 55 | 508 ± 41 | 0.1143 |
| Tidal volume (mL/kg abw) | 7.3 ± 0.8 | 7.7 ± 0.7 | 0.0890 |
| Respiratory rate (1/min) | 19 ± 3 | 18 ± 2 | 0.0582 |
| FiO2 (%) | 68.9 ± 13.2 | 73.9 ± 18.3 | 0.1848 |
| pH | 7.36 ± 0.09 | 7.38 ± 0.08 | 0.3923 |
| PaO2 (mmHg) | 137.1 ± 51.2 | 118.7 ± 49.6 | 0.1563 |
| PaCO2 (mmHg) | 50.3 ± 12.7 | 47.5 ± 8.2 | 0.3401 |
| PaO2/FiO2 (mmHg) | 204.2 ± 77.4 | 166.1 ± 58.8 | 0.0410 |
| Ventilatory ratio | 1.9 [1.4; 2.3] | 1.8 [1.5; 2.0] | 0.6625 |
| Worst respiratory mechanics and gas exchange during the first week | |||
| Respiratory system compliance (ml/cmH2O) | 47.3 ± 13.0 | 45.9 ± 13.7 | 0.6688 |
| Airway driving pressure (cmH2O) | 11 [8; 12] | 13 [11; 16] | 0.0065 |
| Airway plateau pressure (cmH2O) | 24 [22; 27] | 27 [22; 29] | 0.1921 |
| PEEP (cmH2O) | 14 [12; 15] | 14 [12; 14] | 0.8115 |
| Tidal volume (mL) | 485 ± 54 | 546 ± 81 | 0.0003 |
| Respiratory rate (1/min) | 20 ± 3 | 20 ± 2 | 0.5984 |
| FiO2 (%) | 69.1 ± 12.9 | 70.7 ± 14.6 | 0.6516 |
| pH | 7.35 ± 0.08 | 7.40 ± 0.07 | 0.0239 |
| PaO2 (mmHg) | 126.3 ± 40.2 | 80.7 ± 20.9 | <0.0001 |
| PaCO2 (mmHg) | 50.8 ± 12.2 | 52.0 ± 10.0 | 0.6684 |
| PaO2/FiO2 (mmHg) | 187.5 ± 60.2 | 116.3 ± 28.2 | <0.0001 |
| Ventilatory ratio | 1.9 [1.5; 2.3] | 2.1 [1.8; 3.0] | 0.0445 |
| Worst SOFA score | 4 [3; 6] | 4 [4; 6] | 0.1162 |
| No Boluses | Rescue Boluses | Regression Output | p | |
|---|---|---|---|---|
| (a) Unadjusted comparison | N = 59 | N = 22 | ||
| Primary outcome | ||||
| Length of ICU stay (days) | 10.5 [6; 17] | 18 [13; 23] | b = 6.69 ± 3.35 | 0.050 |
| Secondary outcomes | ||||
| Duration of mechanical ventilation (days) | 9.5 [6; 16] | 18 [13; 23] | b = 7.66 ± 2.86 | 0.090 |
| Length of hospital stay (days) | 25 [18; 35] | 21 [16; 37] | b = 0.88 ± 3.92 | 0.822 |
| Ventilator-free days (days) | 15 [0; 22] | 0 [0; 0] | b = −9.93 ± 2.34 | <0.001 |
| Hospital mortality–n (%) | 20 (33.9) | 17 (77.3) | OR = 6.63 ± 3.83 | <0.001 |
| Patients who developed VAP–n (%) | 24 (40.7) | 16 (72.7) | OR = 3.88 ± 2.13 | 0.013 |
| Number of VAP per patient | 2 [1; 2] | 2 [1; 2] | b = 0.25 ± 0.37 | 0.505 |
| Patients who developed bacteremia–n (%) | 16 (27.1) | 15 (68.2) | OR = 5.75 ± 3.12 | <0.001 |
| Number of bacteremias per patient | 2 [1; 2] | 1 [1; 2] | b = −0.21 ± 0.27 | 0.434 |
| (b) Propensity-matched sample | n = 22 | N = 22 | ||
| Primary outcome | ||||
| Length of ICU stay (days) | 11 [6; 24] | 18 [13; 23] | b = 14.61 ± 7.60 | 0.059 |
| Secondary outcomes | ||||
| Duration of mechanical ventilation (days) | 9 [6; 18] | 18 [13; 23] | b = 15.85 ± 7.57 | 0.040 |
| Length of hospital stay (days) | 27 [21; 35] | 21 [16; 37] | b = 9.29 ± 7.26 | 0.205 |
| Ventilator-free days (days) | 8 [0; 21] | 0 [0; 0] | b = −9.30 ± 2.08 | <0.001 |
| Hospital mortality–n (%) | 9 (40.9) | 17 (77.3) | OR = 9.84 ± 7.67 | 0.003 |
| Patients who developed VAP–n (%) | 11 (50.0) | 16 (72.7) | OR = 9.68 ± 6.90 | 0.001 |
| Number of VAP per patient | 1 [1; 2] | 2 [1; 2] | b = 1.80 ± 1.08 | 0.105 |
| Patients who developed bacteremia–n (%) | 5 (22.7) | 15 (68.2) | OR = 16.62 ± 11.7 | <0.001 |
| Number of bacteremias per patient | 2 [2; 3] | 1 [1; 2] | b = 0.19 ± 0.52 | 0.710 |
| Bolus Non-Responders (n = 10–45.5%) | Bolus Responders (n = 12–54.5%) | p | |
|---|---|---|---|
| Pimary outcome | |||
| Length of ICU stay (days) | 21 [11; 23] | 18 [16; 26] | 0.8868 |
| Secondary outcomes | |||
| Duration of mechanical ventilation (days) | 21 [12; 23] | 18 [14; 23] | 0.9150 |
| Length of hospital stay (days) | 21 [15; 23] | 33 [17; 46] | 0.2703 |
| Ventilator-free days (days) | 0 [0; 0] | 0 [0; 9] | 0.0324 |
| Hospital mortality–n (%) | 10 (100) | 7 (58.3) | 0.0274 |
| Patients who developed VAP–n (%) | 7 (70.0) | 9 (75.0) | 0.8825 |
| Number of VAP per patient | 2 [1; 2] | 2 [1; 2] | 0.7665 |
| Patients who developed bacteremia–n (%) | 7 (70.0) | 8 (66.7) | 0.5773 |
| Number of bacteremias per patient | 1 [1; 2] | 2 [1; 2] | 0.5085 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umbrello, M.; Formenti, P.; Nespoli, S.; Pisano, E.; Bonino, C.; Muttini, S. Effect of Different Corticosteroid Regimens on the Outcome of Severe COVID-19-Related Acute Respiratory Failure. A Retrospective Analysis. J. Clin. Med. 2021, 10, 4847. https://doi.org/10.3390/jcm10214847
Umbrello M, Formenti P, Nespoli S, Pisano E, Bonino C, Muttini S. Effect of Different Corticosteroid Regimens on the Outcome of Severe COVID-19-Related Acute Respiratory Failure. A Retrospective Analysis. Journal of Clinical Medicine. 2021; 10(21):4847. https://doi.org/10.3390/jcm10214847
Chicago/Turabian StyleUmbrello, Michele, Paolo Formenti, Stefano Nespoli, Eleonora Pisano, Cecilia Bonino, and Stefano Muttini. 2021. "Effect of Different Corticosteroid Regimens on the Outcome of Severe COVID-19-Related Acute Respiratory Failure. A Retrospective Analysis" Journal of Clinical Medicine 10, no. 21: 4847. https://doi.org/10.3390/jcm10214847