
Soluble IL-2R Levels Predict in-Hospital Mortality in COVID-19 Patients with Respiratory Failure

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
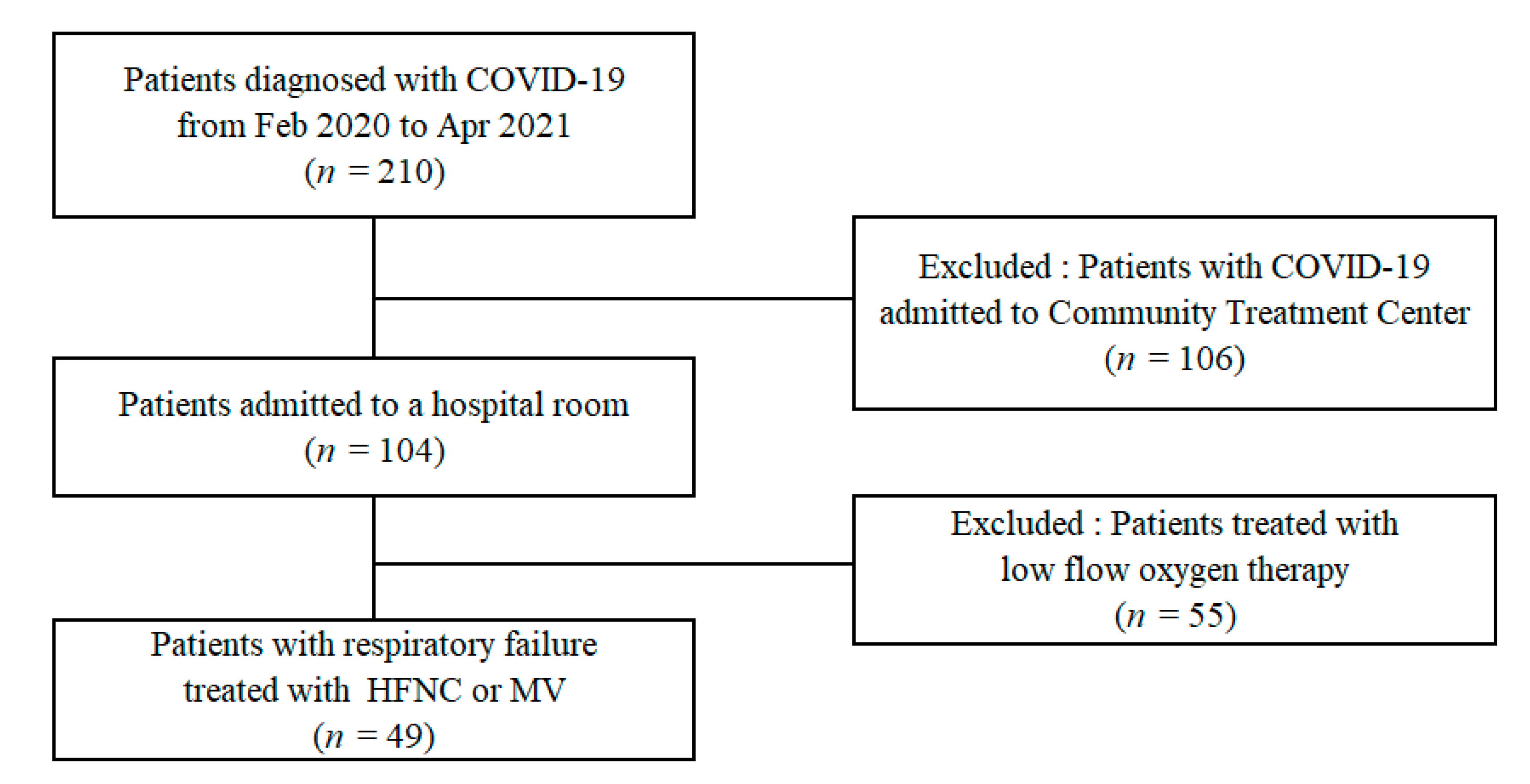
2.1. Patient Recruitment
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Elezkurtaj, S.; Greuel, S.; Ihlow, J.; Michaelis, E.G.; Bischoff, P.; Kunze, C.A.; Sinn, B.V.; Gerhold, M.; Hauptmann, K.; Ingold-Heppner, B.; et al. Causes of death and comorbidities in hospitalized patients with COVID-19. Sci. Rep. 2021, 11, 4263. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Henry, B.M.; Oliveira, M.H.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velavan, T.P.; Meyer, C.G. Mild versus severe COVID-19: Laboratory markers. Int. J. Infect. Dis. 2020, 95, 304–307. [Google Scholar] [CrossRef]
- Riva, G.; Castellano, S.; Nasillo, V.; Ottomano, A.M.; Bergonzini, G.; Paolini, A.; Lusenti, B.; Milić, J.; De Biasi, S.; Gibellini, L.; et al. Monocyte Distribution Width (MDW) as novel inflammatory marker with prognostic significance in COVID-19 patients. Sci. Rep. 2021, 11, 12716. [Google Scholar] [CrossRef]
- Li, X.; Liu, C.; Mao, Z.; Xiao, M.; Wang, L.; Qi, S.; Zhou, F. Predictive values of neutrophil-to-lymphocyte ratio on disease severity and mortality in COVID-19 patients: A systematic review and meta-analysis. Crit. Care 2020, 24, 647. [Google Scholar] [CrossRef]
- Gooding, R.; Riches, P.; Dadian, G.; Moore, J.; Gore, M. Increased soluble interleukin-2 receptor concentration in plasma predicts a decreased cellular response to IL-2. Br. J. Cancer 1995, 72, 452–455. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Goshua, G.; Pine, A.B.; Meizlish, M.; Chang, C.-H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensiv. Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grifoni, E.; Valoriani, A.; Cei, F.; Lamanna, R.; Gelli, A.M.G.; Ciambotti, B.; Vannucchi, V.; Moroni, F.; Pelagatti, L.; Tarquini, R.; et al. Interleukin-6 as prognosticator in patients with COVID-19. J. Infect. 2020, 81, 452–482. [Google Scholar] [CrossRef] [PubMed]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg. Microbes Infect. 2020, 9, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Yang, X.; Yang, Q.; Wang, Y.; Wu, Y.; Xu, J.; Yu, Y.; Shang, Y. Thrombocytopenia and its association with mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1469–1472. [Google Scholar] [CrossRef]
- Hou, H.; Zhang, B.; Huang, H.; Luo, Y.; Wu, S.; Tang, G.; Liu, W.; Mao, L.; Wang, F.; Sun, Z. Using IL-2R/lymphocytes for predicting the clinical progression of patients with COVID-19. Clin. Exp. Immunol. 2020, 201, 76–84. [Google Scholar] [CrossRef]
- Henderson, L.A.; Canna, S.W.; Schulert, G.S.; Volpi, S.; Lee, P.Y.; Kernan, K.F.; Caricchio, R.; Mahmud, S.; Hazen, M.M.; Halyabar, O.; et al. On the Alert for Cytokine Storm: Immunopathology in COVID-19. Arthritis Rheumatol. 2020, 72, 1059–1063. [Google Scholar] [CrossRef] [Green Version]
- Webb, B.J.; Peltan, I.D.; Jensen, P.; Hoda, D.; Hunter, B.; Silver, A.; Starr, N.; Buckel, W.; Grisel, N.; Hummel, E.; et al. Clinical criteria for COVID-19-associated hyperinflammatory syndrome: A cohort study. Lancet Rheumatol. 2020, 2, e754–e763. [Google Scholar] [CrossRef]
- Caricchio, R.; Gallucci, M.; Dass, C.; Zhang, X.; Gallucci, S.; Fleece, D.; Bromberg, M.; Criner, G.J. Preliminary predictive criteria for COVID-19 cytokine storm. Ann. Rheum. Dis. 2021, 80, 88–95. [Google Scholar] [CrossRef]
- Quartuccio, L.; Fabris, M.; Sonaglia, A.; Peghin, M.; Domenis, R.; Cifù, A.; Curcio, F.; Tascini, C. Interleukin 6, soluble interleukin 2 receptor alpha (CD25), monocyte colony-stimulating factor, and hepatocyte growth factor linked with systemic hyperinflammation, innate immunity hyperactivation, and organ damage in COVID-19 pneumonia. Cytokine 2021, 140, 155438. [Google Scholar] [CrossRef] [PubMed]
- Cron, R.Q. COVID-19 cytokine storm: Targeting the appropriate cytokine. Lancet Rheumatol. 2021, 3, e236–e237. [Google Scholar] [CrossRef]
- Group, R.C. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar]
- Riva, G.; Nasillo, V.; Tagliafico, E.; Trenti, T.; Comoli, P.; Luppi, M. COVID-19: More than a cytokine storm. Crit. Care 2020, 24, 549. [Google Scholar] [CrossRef]
- Remy, K.E.; Brakenridge, S.C.; Francois, B.; Daix, T.; Deutschman, C.S.; Monneret, G.; Jeannet, R.; Laterre, P.-F.; Hotchkiss, R.S.; Moldawer, L.L. Immunotherapies for COVID-19: Lessons learned from sepsis. Lancet Respir. Med. 2020, 8, 946–949. [Google Scholar] [CrossRef]
- Damoiseaux, J. The IL-2—IL-2 receptor pathway in health and disease: The role of the soluble IL-2 receptor. Clin. Immunol. 2020, 218, 108515. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Hwang, B.; Chiang, B.N. Cytokines predict coronary aneurysm formation in Kawasaki disease patients. Eur. J. Nucl. Med. Mol. Imaging 1993, 152, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Sundel, R.P. Kawasaki disease. Rheum. Dis. Clin. N. Am. 2015, 41, 63–73. [Google Scholar] [CrossRef]
- Symons, J.A.; Wood, N.C.; Di Giovine, F.S.; Duff, G.W. Soluble IL-2 receptor in rheumatoid arthritis. Correlation with disease activity, IL-1 and IL-2 inhibition. J. Immunol. 1988, 141, 2612–2618. [Google Scholar]
- Zhang, Y.; Wang, X.; Li, X.; Xi, D.; Mao, R.; Wu, X.; Cheng, S.; Sun, X.; Yi, C.; Ling, Z.; et al. Potential contribution of increased soluble IL-2R to lymphopenia in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 878–880. [Google Scholar] [CrossRef]
- Kaya, H.; Kaji, M.; Usuda, D. Soluble interleukin-2 receptor levels on admission associated with mortality in coronavirus disease 2019. Int. J. Infect. Dis. 2021, 105, 522–524. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Survivors (n = 39) | Non-Survivors (n = 10) | Total (n = 49) | p-Value |
|---|---|---|---|---|
| Age (years) | 70.0 (64.0, 74.0) | 78.0 (65.0, 84.8) | 71.0 (64.5, 77.0) | 0.063 |
| Sex, male (%) | 22 (56.4) | 7 (70.0) | 29 (59.2) | 0.517 |
| BMI, kg/m2 | 24.0 (21.4, 25.7) | 20.4 (18.8, 25.1) | 24.0 (20.5, 25.5) | 0.132 |
| Hypertension | 22 (56.4) | 8 (80.0) | 30 (61.2) | 0.176 |
| Diabetes | 10 (25.6) | 6 (60.0) | 16 (32.7) | 0.041 |
| PaO2/FiO2, kPa | 149.8 (100.9, 184.3) | 125.1 (86.3, 229.2) | 148.7 (96.9, 197.9) | 0.951 |
| ARDS | ||||
| Mild | 9 (23.1) | 3 (30.0) | 12 (24.5) | |
| Moderate | 21 (53.8) | 4 (40.0) | 25 (51.0) | |
| Severe | 9 (23.1) | 3 (30.0) | 12 (24.5) | |
| WBC (103/uL) | 8.6 (6.7, 12.6) | 6.2 (4.5, 8.5) | 8.1 (6.0, 11.0) | 0.080 |
| Lymphocyte (103/uL) | 0.8 (0.5, 1.0) | 0.6 (0.4, 1.0) | 0.7 (0.5, 1.0) | 0.517 |
| Platelet (103/uL) | 185.0 (136.0, 246.0) | 127.5 (109.5, 170.8) | 181.0 (126.0, 232.0) | 0.022 |
| Albumin (g/dL) | 3.7 (3.3, 3.9) | 3.6 (3.1, 3.8) | 3.6 (3.3, 3.9) | 0.358 |
| Total bilirubin (mg/dL) | 0.7 (0.5, 0.9) | 0.7 (0.5, 1.3) | 0.7 (0.5, 1.0) | 0.566 |
| Bicarbonate (mmol/L) | 23.0 (21.0, 25.0) | 22.0 (19.0, 23.5) | 23.0 (21.0, 24.8) | 0.164 |
| Creatinine (mg/dL) | 0.7 (0.6, 1.1) | 1.0 (0.9, 2.3) | 0.9 (0.6, 1.1) | 0.012 |
| Troponin (pg/mL) | 12.0 (7.0, 17.3) | 33.0 (17.5, 75.8) | 12.0 (8.0, 25.3) | 0.001 |
| LDH (IU/L) | 527.0 (427.0, 639.0) | 494.0 (379.8, 652.3) | 514.0 (420.0, 641.5) | 0.779 |
| Procalcitonin (ng/mL) | 0.3 (0.1, 0.5) | 0.5 (0.4, 1.2) | 0.3 (0.1, 0.5) | 0.009 |
| Fibrinogen (mg/dL) | 471.0 (390.8, 613.5) | 433.0 (305.5, 521.5) | 458.0 (381.0, 599.0) | 0.213 |
| D-dimer (ng/mL) | 480.0 (273.0, 1386.0) | 599.5 (328.5, 3858.5) | 494.0 (294.0, 1288.5) | 0.333 |
| Ferritin (ng/mL) | 787.8 (443.6, 1485.7) | 1056.0 (422.1, 1688.0) | 801.3 (446.1, 1485.6) | 0.505 |
| CRP (mg/L) | 107.6 (59.7, 155.9) | 140.3 (55.7, 218.4) | 112.2 (59.7, 180.3) | 0.371 |
| IL-6 (pg/mL) | 65.1 (17.8, 147.1) | 160.1 (81.4, 320.7) | 89.3 (19.4, 158.4) | 0.072 |
| Soluble IL2 receptor (U/mL) | 853.0 (727.5, 1150.5) | 1159.0 (1099.5, 1376.5) | 905.5 (740.3, 1230.8) | 0.010 |
| Invasive ventilation | 11 (28.2) | 4 (40.0) | 14 (32.6) | 0.582 |
| SOFA score | 3.0 (0.3, 8.3) | 3.0 (2.8, 4.0) | 3.0 (3.0, 3.0) | 0.385 |
| APACHE II score | 24.0 (20.0, 26.0) | 24.5 (19.0, 28.5) | 24.0 (20.0, 26.5) | 0.391 |
| Hospital day | 18.5 (15.0, 24.3) | 21.5 (13.5, 33.0) | 19.0 (15.0, 25.3) | 0.695 |
| Variable | Survivors (n = 39) | Non-Survivors (n = 10) | Total (n = 49) | p-Value |
|---|---|---|---|---|
| PaO2/FiO2, kPa | 216.0 (165.4, 290.1) | 140.6 (71.3, 160.5) | 206.7 (141.7, 264.5) | 0.001 |
| ARDS | ||||
| Mild | 22 (56.4) | 2 (20.0) | 24 (49.0) | |
| Moderate | 15 (38.5) | 5 (50.0) | 20 (40.8) | |
| Severe | 0 (0.0) | 3 (30.0) | 3 (6.1) | |
| WBC (103/uL) | 11.7 (7.0, 13.2) | 16.2 (7.7, 21.1) | 11.8 (7.4, 16.0) | 0.189 |
| Lymphocyte (103/uL) | 0.8 (0.5, 1.2) | 0.4 (0.2, 0.5) | 0.7 (0.4, 1.2) | 0.005 |
| Platelet (103/uL) | 272.0 (187.0, 362.0) | 117.0 (72.0, 173.8) | 242.0 (152.0, 353.0) | 0.001 |
| Albumin (g/dL) | 2.9 (2.7, 3.2) | 2.8 (2.7, 3.0) | 2.9 (2.7, 3.2) | 0.235 |
| Total bilirubin (mg/dL) | 0.6 (0.4, 0.9) | 0.7 (0.4, 1.0) | 0.6 (0.4, 0.9) | 0.795 |
| Bicarbonate (mmol/L) | 25.0 (24.0, 29.0) | 24.0 (23.0, 28.8) | 25.0 (23.0, 29.0) | 0.416 |
| Creatinine (mg/dL) | 0.6 (0.5, 0.7) | 0.9 (0.7, 2.0) | 0.6 (0.5, 0.8) | 0.001 |
| LDH (IU/L) | 402.0 (320.5, 475.3) | 532.0 (432.5, 637.5) | 420.0 (334.0, 532.0) | 0.013 |
| Procalcitonin (ng/mL) | 0.1 (0.0, 0.1) | 0.2 (0.1, 0.7) | 0.1 (0.1, 0.2) | 0.008 |
| Fibrinogen (mg/dL) | 384.5 (348.5, 434.3) | 440.5 (256.8, 543.0) | 399.0 (349.0, 458.0) | 0.634 |
| D-dimer (ng/mL) | 982.0 (360.0, 3591.0) | 1877.5 (454.8, 6152.0) | 987.5 (373.8, 3787.0) | 0.338 |
| Ferritin (ng/mL) | 548.1 (334.0, 846.5) | 592.9 (410.0, 770.5) | 571.1 (346.1, 840.1) | 0.746 |
| CRP (mg/L) | 25.6 (8.7, 52.3) | 65.5 (35.5, 112.0) | 35.3 (10.1, 54.4) | 0.016 |
| IL-6 (pg/mL) | 17.9 (6.1, 51.9) | 100.7 (41.1, 244.6) | 21.6 (8.0, 87.5) | 0.001 |
| Soluble IL2 receptor (U/mL) | 845.0 (563.8, 1061.3) | 1313.0 (1001.3, 1963.5) | 949.5 (640.0, 1126.3) | 0.001 |
| Invasive ventilation | 22 (56.4) | 7 (70.0) | 27 (59.2) | 0.617 |
| Variable | Non-MV Group (n = 20) | MV Group (n = 29) | p-Value |
|---|---|---|---|
| Age (years) | 71.0 (65.3, 78.6) | 70.0 (63.0, 75.5) | 0.653 |
| Sex, male (%) | 10 (50.0) | 19 (65.5) | 0.377 |
| BMI, kg/m2 | 24.2 (20.3, 25.9) | 23.8 (20.5, 25.4) | 0.717 |
| PaO2/FiO2, kPa | 153.2 (127.6, 207.2) | 123.1 (87.7, 172.9) | 0.186 |
| WBC (103/uL) | 8.2 (7.1, 10.7) | 7.7 (5.5, 11.8) | 0.307 |
| Lymphocyte (103/uL) | 0.6 (0.5, 1.0) | 0.8 (0.5, 0.9) | 0.805 |
| Platelet (103/uL) | 182.0 (134.3, 252.0) | 164.0 (118.0, 208.0) | 0.251 |
| Albumin (g/dL) | 3.8 (3.5, 4.1) | 3.5 (3.2, 3.8) | 0.016 |
| Total bilirubin (mg/dL) | 0.6 (0.4, 0.7) | 0.8 (0.6, 1.2) | 0.001 |
| Bicarbonate (mmol/L) | 22.0 (20.3, 24.0) | 23.0 (21.0, 25.0) | 0.382 |
| Creatinine (mg/dL) | 0.9 (0.7, 1.1) | 0.8 (0.6, 1.0) | 0.428 |
| Troponin (pg/mL) | 12.0 (9.3, 21.8) | 12.5 (7.0, 31.3) | 0.963 |
| LDH (IU/L) | 507.0 (396.3, 569.3) | 527.0 (428.5, 674.5) | 0.211 |
| Procalcitonin (ng/mL) | 0.4 (0.1, 0.7) | 0.3 (0.1, 0.5) | 0.782 |
| Fibrinogen (mg/dL) | 488.0 (414.8, 587.0) | 445.0 (369.0, 615.0) | 0.414 |
| D-dimer (ng/mL) | 487.0 (294.0, 651.5) | 527.0 (294.0, 4301.5) | 0.185 |
| Ferritin (ng/mL) | 455.6 (365.0, 985.8) | 1098.2 (731.0, 1893.4) | 0.003 |
| CRP (mg/L) | 111.6 (61.7, 144.6) | 117.2 (59.7, 210.3) | 0.490 |
| IL-6 (pg/mL) | 100.9 (18.9, 143.8) | 65.1 (19.4, 191.5) | 0.855 |
| Soluble IL2 receptor (U/mL) | 867.0 (726.8, 1073.8) | 1036.0 (754.0, 1364.3) | 0.135 |
| Hospital day | 15.0 (11.3, 19.0) | 22.0 (18.0, 32.0) | <0.001 |
| Mortality | 3 (15.0) | 7 (24.1) | 0.496 |
| Univariable | Adjusted | |||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age, years | 1.077 | 0.983–1.180 | 0.113 | 1.023 | 0.942–1.112 | 0.585 |
| Sex, male | 1.622 | 0.405–6.493 | 0.495 | |||
| Initial P/F ratio | 0.999 | 0.993–1.005 | 0.781 | 0.997 | 0.990–1.004 | 0.340 |
| Δ WBC | 1.102 | 0.970–1.251 | 0.136 | |||
| Δ lymphocyte | 0.319 | 0.083–1.227 | 0.096 | 0.741 | 0.096–5.713 | 0.779 |
| Δ Platelet | 0.994 | 0.990–0.999 | 0.019 | 0.993 | 0.986–1.001 | 0.069 |
| Δ LDH (IU/L) | 1.003 | 0.999–1.006 | 0.140 | |||
| Δ Fibrinogen (mg/dL) | 1.001 | 0.999–1.003 | 0.385 | |||
| Δ Ferritin (ng/mL) | 0.999 | 0.997–1.001 | 0.502 | |||
| Δ CRP (mg/L) | 1.003 | 0.996–1.011 | 0.367 | |||
| Δ IL-6/SD | 1.664 | 0.896–3.088 | 0.107 | 1.234 | 0.594–2.564 | 0.573 |
| Δ sIL-2R/SD | 3.145 | 1.177–8.406 | 0.022 | 3.225 | 1.151–9.037 | 0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, H.J.; Leem, A.Y.; Chung, K.S.; Ahn, J.Y.; Jung, J.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Lee, S.H. Soluble IL-2R Levels Predict in-Hospital Mortality in COVID-19 Patients with Respiratory Failure. J. Clin. Med. 2021, 10, 4242. https://doi.org/10.3390/jcm10184242
Jang HJ, Leem AY, Chung KS, Ahn JY, Jung JY, Kang YA, Park MS, Kim YS, Lee SH. Soluble IL-2R Levels Predict in-Hospital Mortality in COVID-19 Patients with Respiratory Failure. Journal of Clinical Medicine. 2021; 10(18):4242. https://doi.org/10.3390/jcm10184242
Chicago/Turabian StyleJang, Hye Jin, Ah Young Leem, Kyung Soo Chung, Jin Young Ahn, Ji Ye Jung, Young Ae Kang, Moo Suk Park, Young Sam Kim, and Su Hwan Lee. 2021. "Soluble IL-2R Levels Predict in-Hospital Mortality in COVID-19 Patients with Respiratory Failure" Journal of Clinical Medicine 10, no. 18: 4242. https://doi.org/10.3390/jcm10184242