
Adverse Events of Percutaneous Microaxial Left Ventricular Assist Devices—A Retrospective, Single-Centre Cohort Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Definition of Adverse Events and Outcomes
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U. The ESC Textbook of Intensive and Acute Cardiovascular Care Cardiogenic Shock in Patients with Acute Coronary Syndromes; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Burzotta, F.; Trani, C.; Doshi, S.N.; Townend, J.; van Geuns, R.J.; Hunziker, P.; Schieffer, B.; Karatolios, K.; Moller, J.E.; Ribichini, F.L.; et al. Impella ventricular support in clinical practice: Collaborative viewpoint from a European expert user group. Int. J. Cardiol. 2015, 201, 684–691. [Google Scholar] [CrossRef]
- Rihal, C.S.; Naidu, S.S.; Givertz, M.M.; Szeto, W.Y.; Burke, J.A.; Kapur, N.K.; Kern, M.; Garratt, K.N.; Goldstein, J.A.; Dimas, V.; et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care (Endorsed by the American Heart Association, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’intervention). J. Card Fail. 2015, 21, 499–518. [Google Scholar] [CrossRef]
- Chieffo, A.; Burzotta, F.; Pappalardo, F.; Briguori, C.; Garbo, R.; Masiero, G.; Nicolini, E.; Ribichini, F.; Trani, C.; Alvarez, B.C.; et al. Clinical expert consensus document on the use of percutaneous left ventricular assist support devices during complex high-risk indicated PCI: Italian Society of Interventional Cardiology Working Group Endorsed by Spanish and Portuguese Interventional Cardiology Societies. Int. J. Cardiol. 2019, 293, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef] [Green Version]
- Burkhoff, D.; Sayer, G.; Doshi, D.; Uriel, N. Hemodynamics of Mechanical Circulatory Support. J. Am. Coll. Cardiol. 2015, 66, 2663–2674. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, W.W.; Kleiman, N.S.; Moses, J.; Henriques, J.P.; Dixon, S.; Massaro, J.; Palacios, I.; Maini, B.; Mulukutla, S.; Dzavik, V.; et al. A prospective, randomized clinical trial of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoing high-risk percutaneous coronary intervention: The PROTECT II study. Circulation 2012, 126, 1717–1727. [Google Scholar] [CrossRef]
- Bochaton, T.; Huot, L.; Elbaz, M.; Delmas, C.; Aissaoui, N.; Farhat, F.; Mewton, N.; Bonnefoy, E. Mechanical circulatory support with the Impella® LP5.0 pump and an intra-aortic balloon pump for cardiogenic shock in acute myocardial infarction: The IMPELLA-STIC randomized study. Arch. Cardiovasc. Dis. 2020, 113, 237–243. [Google Scholar] [CrossRef]
- Ouweneel, D.M.; Eriksen, E.; Sjauw, K.D.; van Dongen, I.M.; Hirsch, A.; Packer, E.J.; Vis, M.M.; Wykrzykowska, J.J.; Koch, K.T.; Baan, J.; et al. Percutaneous mechanical circulatory support versus intra-aortic balloon pump in cardiogenic shock after acute myocardial infarction. J. Am. Coll. Cardiol. 2017, 69, 278–287. [Google Scholar] [CrossRef]
- Amin, A.P.; Spertus, J.A.; Curtis, J.P.; Desai, N.; Masoudi, F.A.; Bach, R.G.; McNeely, C.; Al-Badarin, F.; House, J.A.; Kulkarni, H.; et al. The evolving landscape of Impella use in the United States among patients undergoing percutaneous coronary intervention with mechanical circulatory support. Circulation 2020, 141, 273–284. [Google Scholar] [CrossRef]
- Wernly, B.; Seelmaier, C.; Leistner, D.; Stahli, B.E.; Pretsch, I.; Lichtenauer, M.; Jung, C.; Hoppe, U.C.; Landmesser, U.; Thiele, H.; et al. Mechanical circulatory support with Impella versus intra-aortic balloon pump or medical treatment in cardiogenic shock-a critical appraisal of current data. Clin. Res. Cardiol. 2019, 108, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Dhruva, S.S.; Ross, J.S.; Mortazavi, B.J.; Hurley, N.C.; Krumholz, H.M.; Curtis, J.P.; Berkowitz, A.; Masoudi, F.A.; Messenger, J.C.; Parzynski, C.S.; et al. Association of use of an intravascular microaxial left ventricular assist device vs intra-aortic balloon pump with in-hospital mortality and major bleeding among patients with acute myocardial infarction complicated by cardiogenic shock. JAMA 2020, 323, 734–745. [Google Scholar] [CrossRef] [PubMed]
- Chieffo, A.; Ancona, M.B.; Burzotta, F.; Pazzanese, V.; Briguori, C.; Trani, C.; Piva, T.; De Marco, F.; Di Biasi, M.; Pagnotta, P.; et al. Observational multicentre registry of patients treated with IMPella mechanical circulatory support device in ITaly: The IMP-IT registry. EuroIntervention 2020, 15, e1343–e1350. [Google Scholar] [CrossRef] [Green Version]
- Hunziker, L.; Radovanovic, D.; Jeger, R.; Pedrazzini, G.; Cuculi, F.; Urban, P.; Erne, P.; Rickli, H.; Pilgrim, T. Twenty-Year trends in the incidence and outcome of cardiogenic shock in AMIS Plus Registry. Circ. Cardiovasc. Interv. 2019, 12, e007293. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Section 2: AKI Definition. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4089595/ (accessed on 21 June 2021).
- Chatterjee, S.; Wetterslev, J.; Sharma, A.; Lichstein, E.; Mukherjee, D. Association of blood transfusion with increased mortality in myocardial infarction: A meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern. Med. 2013, 173, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Mehta, S.R.; Anand, S.S.; Xie, C.; Fox, K.A.; Yusuf, S. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation 2006, 114, 774–782. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.S.; Emerson, D.; Ramzy, D.; Akhmerov, A.; Megna, D.; Esmailian, F.; Kobashigawa, J.; Cole, R.M.; Moriguchi, J.; Trento, A. A New Paradigm in Mechanical Circulatory Support: 100-Patient Experience. Ann. Thorac. Surg. 2020, 109, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, W.W.; Schreiber, T.; Wohns, D.H.; Rihal, C.; Naidu, S.S.; Civitello, A.B.; Dixon, S.R.; Massaro, J.M.; Maini, B.; Ohman, E.M. The current use of Impella 2.5 in acute myocardial infarction complicated by cardiogenic shock: Results from the USpella Registry. J. Interv. Cardiol. 2014, 27, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.G.; Matthews, R.; Maini, B.; Dixon, S.; Vetrovec, G.; Wohns, D.; Palacios, I.; Popma, J.; Ohman, E.M.; Schreiber, T.; et al. Percutaneous left ventricular assist device for high-risk percutaneous coronary interventions: Real-world versus clinical trial experience. Am. Heart J. 2015, 170, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.B.; Goldstein, J.; Milano, C.; Morris, L.D.; Kormos, R.L.; Bhama, J.; Kapur, N.K.; Bansal, A.; Garcia, J.; Baker, J.N.; et al. Benefits of a novel percutaneous ventricular assist device for right heart failure: The prospective RECOVER RIGHT study of the Impella RP device. J. Heart Lung Transpl. 2015, 34, 1549–1560. [Google Scholar] [CrossRef]
- Maini, B.; Naidu, S.S.; Mulukutla, S.; Kleiman, N.; Schreiber, T.; Wohns, D.; Dixon, S.; Rihal, C.; Dave, R.; O’Neill, W. Real-world use of the Impella 2.5 circulatory support system in complex high-risk percutaneous coronary intervention: The USpella Registry. Catheter. Cardiovasc. Interv. 2012, 80, 717–725. [Google Scholar] [CrossRef]
- Badiye, A.P.; Hernandez, G.A.; Novoa, I.; Chaparro, S.V. Incidence of hemolysis in patients with cardiogenic shock treated with Impella percutaneous left ventricular assist device. Asaio J. 2016, 62, 11–14. [Google Scholar] [CrossRef]
- Subramaniam, A.V.; Barsness, G.W.; Vallabhajosyula, S. Complications of temporary percutaneous mechanical circulatory support for cardiogenic shock: An appraisal of contemporary literature. Cardiol. Ther. 2019, 8, 211–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, S.R.; Henriques, J.P.; Mauri, L.; Sjauw, K.; Civitello, A.; Kar, B.; Loyalka, P.; Resnic, F.S.; Teirstein, P.; Makkar, R.; et al. A prospective feasibility trial investigating the use of the Impella 2.5 system in patients undergoing high-risk percutaneous coronary intervention (The PROTECT I Trial): Initial U.S. experience. JACC Cardiovasc. Interv. 2009, 2, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Monteagudo-Vela, M.; Simon, A.; Riesgo Gil, F.; Rosenberg, A.; Dalby, M.; Kabir, T.; Garcia Saez, D.; Panoulas, V. Clinical indications of IMPELLA short-term mechanical circulatory support in a tertiary Centre. Cardiovasc. Revasc. Med. 2019, 21, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E.; Guyton, A.C. Red Blood Cells, Anemia, and Polycythemia Guyton and Hall Textbook of Medical Physiology, 12th ed.; Saunders: Philadelphia, PA, USA; Elsevier: Amsterdam, The Netherlands, 2011; p. 1120. [Google Scholar]
- Schrage, B.; Ibrahim, K.; Loehn, T.; Werner, N.; Sinning, J.M.; Pappalardo, F.; Pieri, M.; Skurk, C.; Lauten, A.; Landmesser, U.; et al. Impella support for acute myocardial infarction complicated by cardiogenic shock. Circulation 2019, 139, 1249–1258. [Google Scholar] [CrossRef] [PubMed]
- Manzo-Silberman, S.; Fichet, J.; Mathonnet, A.; Varenne, O.; Ricome, S.; Chaib, A.; Zuber, B.; Spaulding, C.; Cariou, A. Percutaneous left ventricular assistance in post cardiac arrest shock: Comparison of intra aortic blood pump and IMPELLA Recover LP2.5. Resuscitation 2013, 84, 609–615. [Google Scholar] [CrossRef]
- Goldfarb, M.; Czer, L.S.; Lam, L.D.; Moriguchi, J.; Arabia, F.A.; Volod, O. High molecular weight von Willebrand factor multimer loss and bleeding in patients with short-term mechanical circulatory support devices: A case series. J. Extra Corpor. Technol. 2018, 50, 77–82. [Google Scholar]
- Flierl, U.; Tongers, J.; Berliner, D.; Sieweke, J.T.; Zauner, F.; Wingert, C.; Riehle, C.; Bauersachs, J.; Schäfer, A. Acquired von Willebrand syndrome in cardiogenic shock patients on mechanical circulatory microaxial pump support. PLoS ONE 2017, 12, e0183193. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.E.; Haglund, N.A.; Tricarico, N.M.; Keebler, M.E.; Maltais, S. Development of acquired von Willebrand syndrome during short-term micro axial pump support: Implications for bleeding in a patient bridged to a long-term continuous-flow left ventricular assist device. Asaio J. 2014, 60, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, T.; Wah Htun, W.; Blank, N.; Telila, T.; Mercado, N.; Briasoulis, A.; Kaki, A.; Kondur, A.; Munir, A.; Grines, C. Real-world supported unprotected left main percutaneous coronary intervention with impella device; data from the USpella registry. Catheter. Cardiovasc. Interv. 2017, 90, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Sjauw, K.D.; Konorza, T.; Erbel, R.; Danna, P.L.; Viecca, M.; Minden, H.H.; Butter, C.; Engstrom, T.; Hassager, C.; Machado, F.P.; et al. Supported high-risk percutaneous coronary intervention with the Impella 2.5 device the Europella registry. J. Am. Coll. Cardiol. 2009, 54, 2430–2434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaherty, M.P.; Pant, S.; Patel, S.V.; Kilgore, T.; Dassanayaka, S.; Loughran, J.H.; Rawasia, W.; Dawn, B.; Cheng, A.; Bartoli, C.R. Hemodynamic support with a microaxial percutaneous left ventricular assist device (Impella) protects against acute kidney injury in patients undergoing high-risk percutaneous coronary intervention. Circ. Res. 2017, 120, 692–700. [Google Scholar] [CrossRef]
- Lauten, A.; Engstrom, A.E.; Jung, C.; Empen, K.; Erne, P.; Cook, S.; Windecker, S.; Bergmann, M.W.; Klingenberg, R.; Luscher, T.F.; et al. Percutaneous left-ventricular support with the Impella-2.5-assist device in acute cardiogenic shock: Results of the Impella-EUROSHOCK-registry. Circ. Heart Fail. 2013, 6, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Baumann, S.; Werner, N.; Al-Rashid, F.; Schafer, A.; Bauer, T.; Sotoudeh, R.; Bojara, W.; Shamekhi, J.; Sinning, J.M.; Becher, T.; et al. Six months follow-up of protected high-risk percutaneous coronary intervention with the microaxial Impella pump: Results from the German Impella registry. Coron. Artery Dis. 2020, 31, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Karami, M.; den Uil, C.A.; Ouweneel, D.M.; Scholte, N.T.; Engstrom, A.E.; Akin, S.; Lagrand, W.K.; Vlaar, A.P.; Jewbali, L.S.; Henriques, J.P. Mechanical circulatory support in cardiogenic shock from acute myocardial infarction: Impella CP/5.0 versus ECMO. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Rios, S.A.; Bravo, C.A.; Weinreich, M.; Olmedo, W.; Villablanca, P.; Villela, M.A.; Ramakrishna, H.; Hirji, S.; Robles, O.A.; Mahato, P.; et al. Meta-Analysis and trial sequential analysis comparing percutaneous ventricular assist devices versus intra-aortic balloon pump during high-risk percutaneous coronary intervention or cardiogenic shock. Am. J. Cardiol. 2018, 122, 1330–1338. [Google Scholar] [CrossRef]
- Vallabhajosyula, S.; Dunlay, S.M.; Prasad, A.; Kashani, K.; Sakhuja, A.; Gersh, B.J.; Jaffe, A.S.; Holmes, D.R.; Barsness, G.W., Jr. Acute noncardiac organ failure in acute myocardial infarction with cardiogenic shock. J. Am. Coll. Cardiol. 2019, 73, 1781–1791. [Google Scholar] [CrossRef] [PubMed]
- Tarvasmäki, T.; Haapio, M.; Mebazaa, A.; Sionis, A.; Silva-Cardoso, J.; Tolppanen, H.; Lindholm, M.G.; Pulkki, K.; Parissis, J.; Harjola, V.P.; et al. Acute kidney injury in cardiogenic shock: Definitions, incidence, haemodynamic alterations, and mortality. Eur. J. Heart Fail. 2018, 20, 572–581. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, S.R.; Kandler, K.; Nielsen, R.V.; Jakobsen, P.C.; Ranucci, M.; Ravn, H.B. Association between transfusion of blood products and acute kidney injury following cardiac surgery. Acta Anaesthesiol Scand. 2020, 64, 1397–1404. [Google Scholar] [CrossRef]
- Ouweneel, D.M.; de Brabander, J.; Karami, M.; Sjauw, K.D.; Engström, A.E.; Vis, M.M.; Wykrzykowska, J.J.; Beijk, M.A.; Koch, K.T.; Baan, J.; et al. Real-life use of left ventricular circulatory support with Impella in cardiogenic shock after acute myocardial infarction: 12 years AMC experience. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 338–349. [Google Scholar] [CrossRef] [Green Version]
- Seyfarth, M.; Sibbing, D.; Bauer, I.; Frohlich, G.; Bott-Flugel, L.; Byrne, R.; Dirschinger, J.; Kastrati, A.; Schomig, A. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J. Am. Coll. Cardiol. 2008, 52, 1584–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics, n = 281 | n (%), Median (IQR) |
|---|---|
| Age, years | 65 (57–75) |
| Male | 210 (74.7) |
| Length of ICU stay, days | 7 (4–11) |
| Length of stay of patients that left ICU alive, days | 8 (5–13.5) |
| SAPS II score | 63.5 (47–77) |
| Resuscitation before Impella® insertion | 113 (40.2) |
| Immediate cardiac surgery prior to Impella® insertion | 25 (8.9) |
| CABG only | 13 (52) |
| Valve surgery | 5 (20) |
| Other | 7 (28) |
| Urgent (24 h), emergency (12 h), and salvage surgery | 15 (60) |
| Elective surgery | 10 (40) |
| Anticoagulation and Antiplatelet Treatment | |
| DAPT | 171 (60.9) |
| In patients with bleeding complications (n = 198) | 104 (52.5) |
| In patients without bleeding complications (n = 83) | 67 (80.7) |
| Heparin, unfractionated and therapeutic | 244 (86.8) |
| In patients with bleeding complications (n = 198) | 175 (88.4) |
| In patients without bleeding complications (n = 83) | 69 (83.1) |
| aPTT (n = 231) | 82 (54–181) |
| In patients with bleeding complications | 95 (58–181) |
| In patients without bleeding complications | 64 (46–106) |
| INR (n = 280) | 1.35 (1.2–1.8) |
| In patients with bleeding complications | 1.4 (1.2–1.9) |
| In patients without bleeding complications | 1.2 (1.1–1.5) |
| Indication for Impella® Use | |
| CS acute myocardial infarction | 196 (69.8) |
| CS ischemic without acute myocardial infarction | 8 (2.9) |
| CS valvular | 18 (6.4) |
| CS cardiomyopathy | 19 (6.8) |
| CS other diagnosis (rhythmogenic, myocarditis) | 34 (12.1) |
| No CS (after ECMO removal, surgery under Impella® support, etc.) | 6 (2.1) |
| Type of Impella® | |
| Impella 2.5® | 143 (50.9) |
| Impella CP® | 123 (43.8) |
| Impella 5.0® | 6 (2.1) |
| Not available | 9 (3.2) |
| Additional Impella® RP | 4 (1.4) |
| Change of Impella® to another type | 8 (2.9) |
| Duration of Impella® support, h (median, IQR) | 72 (35–121) |
| Escalation therapy (ECMO, LVAD, or heart transplantation) | 18 (6.4) |
| ECMO and additional Impella® as LV vent | 9 (3.2) |
| Cardiac Function and Outcome Parameters | |
| LVEF prior to Impella® implantation | 28 (20–40) |
| LVEF at discharge/last before death | 35 (25–43) |
| In-hospital death | 25 (15–35) |
| Patients discharged from hospital | 40 (32–45.5) |
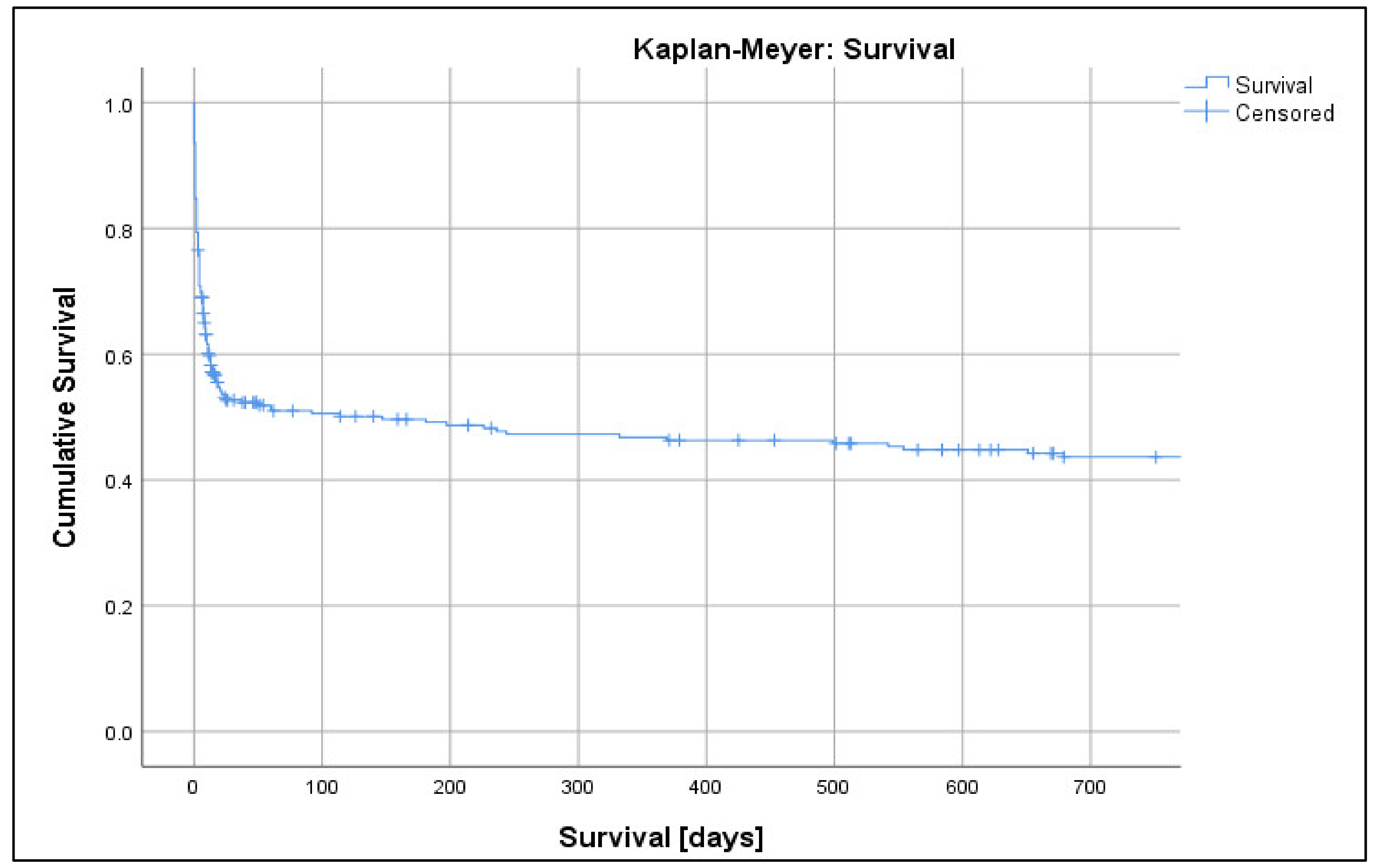
| Mortality Data, n = 281 | n (%), Median (IQR) |
|---|---|
| Survived | 91 (32.4) |
| Deaths | 165 (58.7) |
| Not available | 25 (8.9) |
| In hospital | 134 (47.7) |
| 1-day mortality | 43 (15.3) |
| 3-day mortality | 66 (23.5) |
| 7-day mortality | 95 (33.8) |
| 30-day mortality | 129 (45.9) |
| 90-day mortality | 133 (47.3) |
| 1-year mortality | 142 (50.5) |
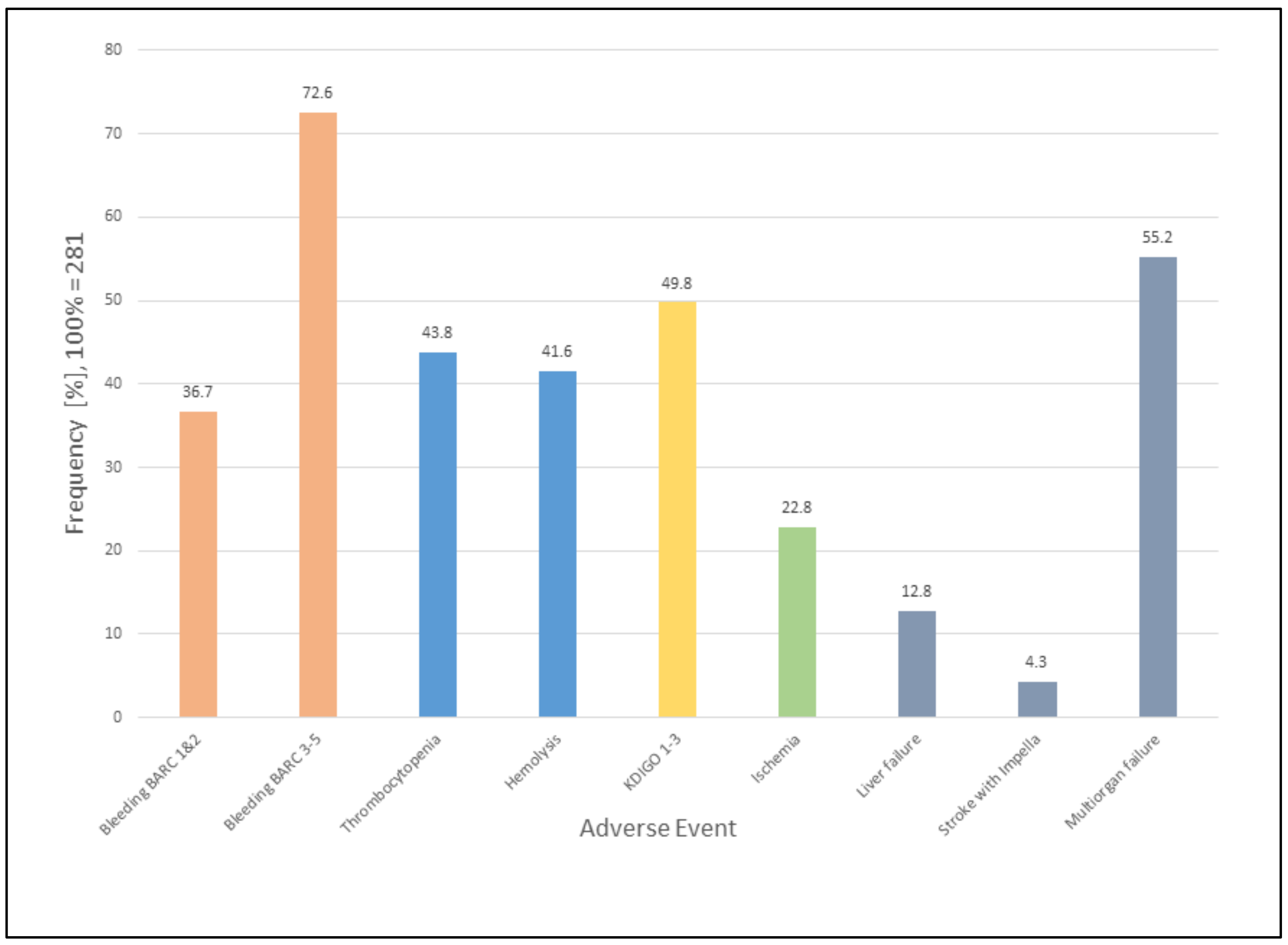
| Adverse Events | |
| Bleeding * | |
| No bleeding | 83 (29.5) |
| BARC types 1 and 2 | 103 (36.7) |
| BARC type 3 | 175 (62.3) |
| BARC type 4 | 24 (8.5) |
| BARC type 5 | 5 (1.8) |
| Number of all patients needing transfusions † | 163 (58) |
| Number of RBC transfusions, units (n = 163, median (IQR)) | 4 (2–12) |
| Stroke within one year | 21 (7.5) |
| Stroke during Impella® therapy | 12 (4.3) |
| Ischemic complications (non-central nervous system) ‡ | 56 (19.9) |
| Intestinal ischemia | 25 (8.9) |
| Limb ischemia | 36 (12.8) |
| Thrombotic complications (jugular venous) | 3 (1.1) |
| Worsening of the valve function‡ | 22 (7.8) |
| Aortic valve | 6 (2.1) |
| Mitral valve | 14 (5) |
| New posterior mitral valve chordal rupture | 4 (1.4) |
| Hemorrhagic shock | 9 (3.2) |
| Associated with cardiac surgery (included in BARC type 3 bleeding) | 4 (1.4) |
| All vascular complications (aneurysms, dissections, or arteriovenous fistulas) | 12 (4.3) |
| Vascular complications without surgery | 4 (1.4) |
| Organ Failure Assessment | n (%) |
|---|---|
| Pre-existing chronic kidney disease (not CS related) | 40 (14.2) |
| KDIGO Stage with missing values | |
| 0 | 141 (50.2) |
| 1 | 38 (13.5) |
| 2 | 38 (13.5) |
| 3 * | 64 (22.8) |
| KDIGO Stage 3 + RRT with missing values (n = 64) | 41 (64.1 †) |
| KDIGO Stage without missing values (n = 273) | 273 (97.2) |
| 0 | 141 (51.7 †) |
| 1 | 38 (13.9 †) |
| 2 | 38 (13.9 †) |
| 3 | 56 (20.5 †) |
| KDIGO Stage 3 + RRT without missing values (n = 56) | 39 (69.6 †) |
| KDIGO Stage for patients with hemolysis (n = 117) | |
| 0 | 40 (34.2 †) |
| 1 | 22 (18.8 †) |
| 2 | 21 (18 †) |
| 3 | 34 (29.1 †) |
| KDIGO Stage for patients without hemolysis (n = 93) | |
| 0 | 61 (65.6 †) |
| 1 | 8 (8.6 †) |
| 2 | 10 (10.8 †) |
| 3 | 13 (14 †) |
| RRT received | 97 (34.5) |
| Regular dialysis prior to hospitalisation | 3 (1.1) |
| RRT and death (n = 97) | 97 (34.5) |
| In hospital | 64 (66†) |
| After hospitalisation | 9 (9.3 †) |
| Liver failure | 36 (12.8) |
| Multiorgan failure | |
| two organs | 67 (23.8) |
| ≥ three organs | 88 (31.3) |
| Hemolysis and Thrombocytopenia | n (%), Median (IQR) |
|---|---|
| Hemolysis | 117 (41.6) |
| Hemolysis without missing values (n = 210) | 117 (55.7) |
| Thrombocytopenia | 123 (43.8) |
| Nadir of platelets, 109/l | |
| With missing values (n = 279) | 108 (60.5–158.5) |
| Without missing values (n = 271) | 104 (60–157) |
| Nadir of platelets for patients with thrombocytopenia, 109/l | |
| With missing values (n = 131) | 62 (36.5–78) |
| Without missing values (n = 123) | 60 (34.5–76) |
| Nadir of platelets & bleeding, 109/l | |
| With missing values (n = 170) | 74 (42.75–131) |
| Without missing values (n = 168) | 74 (44.25–131) |
| Nadir of platelets and no bleeding, 109/l | |
| With missing values (n = 109) | 146 (103–203) |
| Without missing values (n = 103) | 143 (103–199) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaiser, A.S.; Fahrni, G.; Hollinger, A.; Knobel, D.T.; Bovey, Y.; Zellweger, N.M.; Buser, A.; Santer, D.; Pargger, H.; Gebhard, C.E.; et al. Adverse Events of Percutaneous Microaxial Left Ventricular Assist Devices—A Retrospective, Single-Centre Cohort Study. J. Clin. Med. 2021, 10, 3710. https://doi.org/10.3390/jcm10163710
Zaiser AS, Fahrni G, Hollinger A, Knobel DT, Bovey Y, Zellweger NM, Buser A, Santer D, Pargger H, Gebhard CE, et al. Adverse Events of Percutaneous Microaxial Left Ventricular Assist Devices—A Retrospective, Single-Centre Cohort Study. Journal of Clinical Medicine. 2021; 10(16):3710. https://doi.org/10.3390/jcm10163710
Chicago/Turabian StyleZaiser, Anna S., Gregor Fahrni, Alexa Hollinger, Demian T. Knobel, Yann Bovey, Núria M. Zellweger, Andreas Buser, David Santer, Hans Pargger, Caroline E. Gebhard, and et al. 2021. "Adverse Events of Percutaneous Microaxial Left Ventricular Assist Devices—A Retrospective, Single-Centre Cohort Study" Journal of Clinical Medicine 10, no. 16: 3710. https://doi.org/10.3390/jcm10163710