
Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
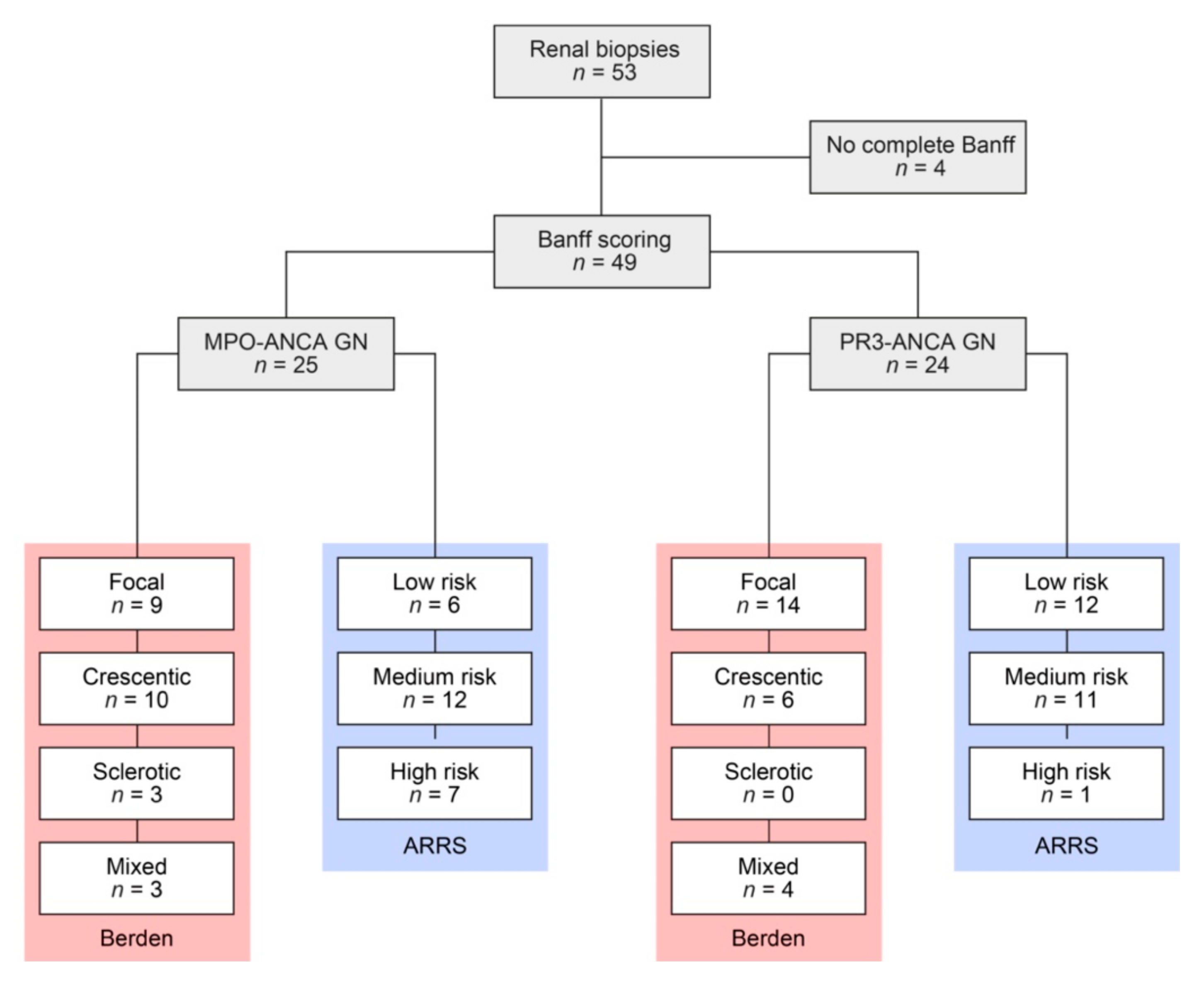
2.1. Study Population
2.2. Definitions
2.3. Renal Histopathology
2.4. Statistical Methods
3. Results
3.1. Study Population
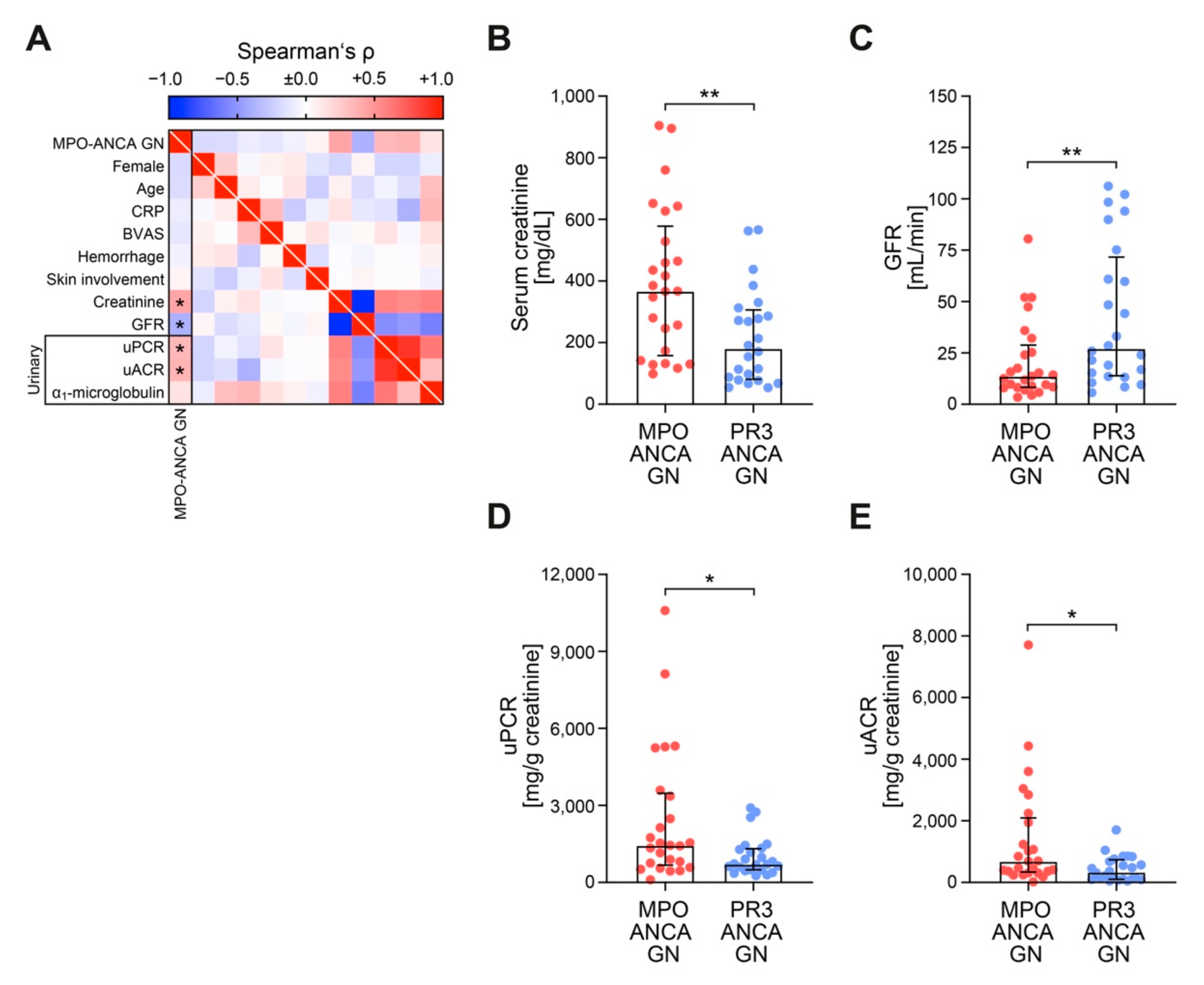
3.2. MPO-ANCA GN Shows More Severe Deterioration of Kidney Function Independent of Systemic Markers of AAV Disease Activity
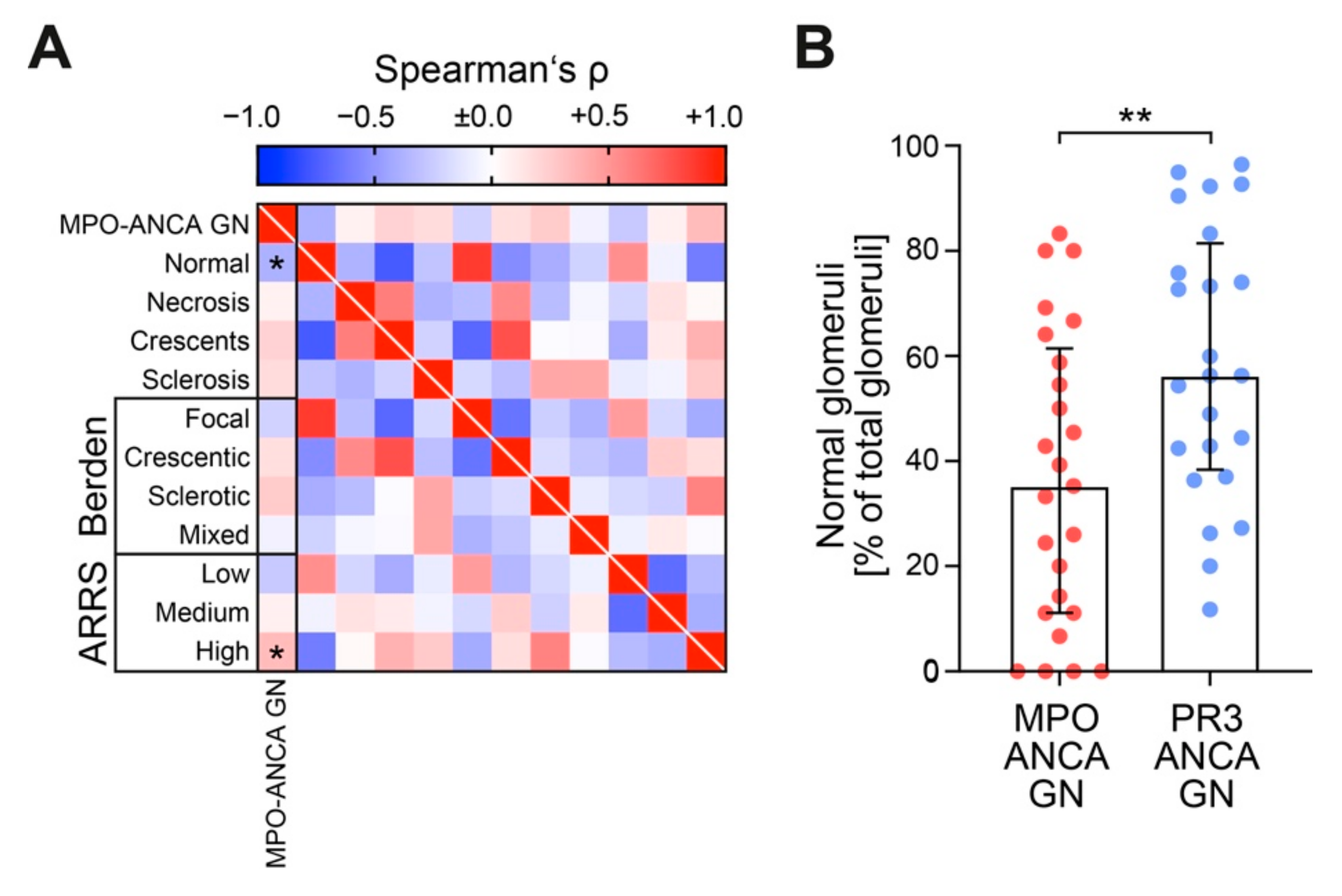
3.3. Histology of MPO-ANCA GN Reveals Decreased Fraction of Normal Glomeruli
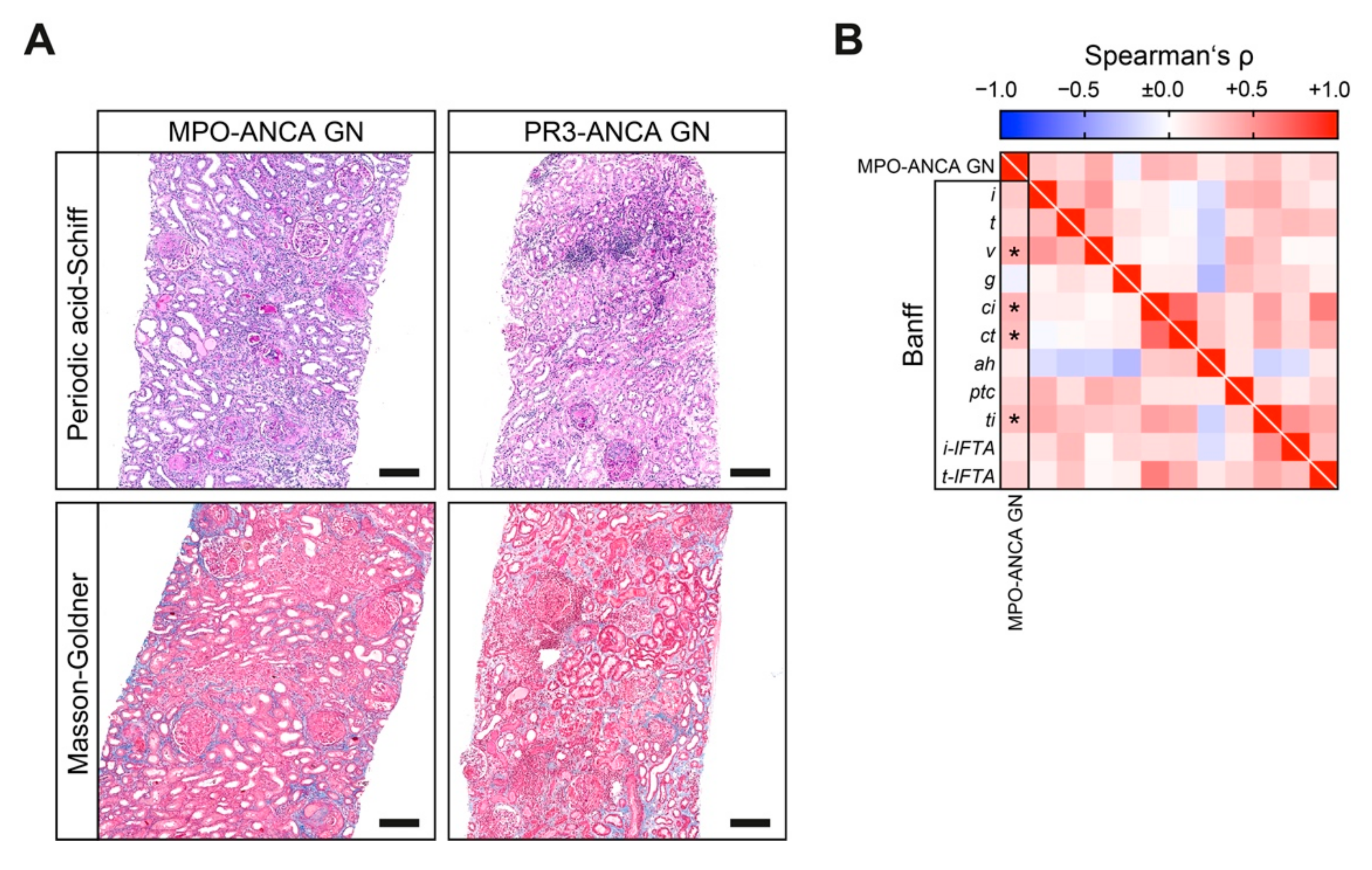
3.4. Banff Scoring Reveals Prominent Interstitial Vasculitis and Inflammation in MPO-ANCA GN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tervaert, J.W.C.; Damoiseaux, J. Fifty years of antineutrophil cytoplasmic antibodies (ANCA) testing: Do we need to revise the international consensus statement on testing and reporting on ANCA? APMIS 2009, 117, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Hruskova, Z.; Stel, V.S.; Jayne, D.; Aasarød, K.; De Meester, J.; Ekstrand, A.; Eller, K.; Heaf, J.G.; Hoitsma, A.; Jimenéz, C.M.; et al. Characteristics and Outcomes of Granulomatosis With Polyangiitis (Wegener) and Microscopic Polyangiitis Requiring Renal Replacement Therapy: Results From the European Renal Association–European Dialysis and Transplant Association Registry. Am. J. Kidney Dis. 2015, 66, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Klinger, H. Grenzformen der Periarteriitis nodosa. Frankf Z Pathol. 1931, 42, 455–480. [Google Scholar]
- Wegener, F. Über eine eigenartige rhinogene Granulomatose mit besonderer Beteiligung des Arteriensystems und der Nieren. Beitr Pathol Anat. 1939, 102, 36–68. [Google Scholar]
- Falk, R.J.; Jennette, J.C. Anti-Neutrophil Cytoplasmic Autoantibodies with Specificity for Myeloperoxidase in Patients with Systemic Vasculitis and Idiopathic Necrotizing and Crescentic Glomerulonephritis. N. Engl. J. Med. 1988, 318, 1651–1657. [Google Scholar] [CrossRef]
- Tervaert, J.W.C.; Goldschmeding, R.; Elema, J.D.; Borne, A.E.G.K.V.D.; Kallenberg, C.G.M. Antimyeloperoxidase antibodies in the Churg-Strauss syndrome. Thorax 1991, 46, 70–71. [Google Scholar] [CrossRef] [Green Version]
- Tervaert, J.W.C.; Damoiseaux, J. Antineutrophil Cytoplasmic Autoantibodies: How Are They Detected and What Is Their Use for Diagnosis, Classification and Follow-up? Clin. Rev. Allergy Immunol. 2012, 43, 211–219. [Google Scholar] [CrossRef]
- Franssen, C.; Gans, R.; Kallenberg, C.; Hageluken, C.; Hoorntje, S. Disease spectrum of patients with antineutrophil cytoplasmic autoantibodies of defined specificity: Distinct differences between patients with anti-proteinase 3 and anti-myeloperoxidase autoantibodies. J. Intern. Med. 1998, 244, 209–216. [Google Scholar] [CrossRef]
- Berden, A.E.; Ferrario, F.; Hagen, E.C.; Jayne, D.R.; Jennette, J.C.; Joh, K.; Neumann, I.; Noël, L.-H.; Pusey, C.D.; Waldherr, R.; et al. Histopathologic Classification of ANCA-Associated Glomerulonephritis. J. Am. Soc. Nephrol. 2010, 21, 1628–1636. [Google Scholar] [CrossRef] [Green Version]
- Hilhorst, M.; Wilde, B.; Vriesman, P.V.B.; Van Paassen, P.; Tervaert, J.W.C. Estimating Renal Survival Using the ANCA-Associated GN Classification. J. Am. Soc. Nephrol. 2013, 24, 1371–1375. [Google Scholar] [CrossRef] [Green Version]
- Haas, M.; Rastaldi, M.P.; Fervenza, F.C. Histologic classification of glomerular diseases: Clinicopathologic correlations, limitations exposed by validation studies, and suggestions for modification. Kidney Int. 2014, 85, 779–793. [Google Scholar] [CrossRef] [Green Version]
- Hauer, H.A.; Bajema, I.M.; Van Houwelingen, H.C.; Ferrario, F.; Noël, L.-H.; Waldherr, R.; Jayne, D.R.; Rasmussen, N.; Bruijn, J.A.; Hagen, E.C. Renal histology in ANCA-associated vasculitis: Differences between diagnostic and serologic subgroups. Kidney Int. 2002, 61, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Franssen, C.F.; Stegeman, C.A.; Oost-Kort, W.W.; Kallenberg, C.G.; Limburg, P.C.; Tiebosch, A.; De Jong, P.E.; Tervaert, J.W. Determinants of renal outcome in anti-myeloperoxidase-associated necrotizing crescentic glomerulonephritis. J. Am. Soc. Nephrol. 1998, 9, 1915–1923. [Google Scholar] [PubMed]
- Brix, S.R.; Noriega, M.; Tennstedt, P.; Vettorazzi, E.; Busch, M.; Nitschke, M.; Jabs, W.J.; Özcan, F.; Wendt, R.; Hausberg, M.; et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018, 94, 1177–1188. [Google Scholar] [CrossRef]
- Vizjak, A.; Rott, T.; Koselj-Kajtna, M.; Rozman, B.; Kaplan-Pavlovčič, S.; Ferluga, D. Histologic and immunohistologic study and clinical presentation of ANCA-associated glomerulonephritis with correlation to ANCA antigen specificity. Am. J. Kidney Dis. 2003, 41, 539–549. [Google Scholar] [CrossRef]
- Roufosse, C.; Simmonds, N.; Groningen, M.C.-V.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasińska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Korsten, P.; Ströbel, P.; Zeisberg, M.; Tampe, B. Histopathological Findings Predict Renal Recovery in Severe ANCA-Associated Vasculitis Requiring Intensive Care Treatment. Front. Med. 2020, 7. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef] [Green Version]
- Franssen, C.F.; Gans, R.O.; Arends, B.; Hageluken, C.; Ter Wee, P.M.; Gerlag, P.G.; Hoorntje, S.J. Differences between anti-myeloperoxidase- and anti-proteinase 3-associated renal disease. Kidney Int. 1995, 47, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Falk, R.J.; Jennette, J.C. ANCA small-vessel vasculitis. J. Am. Soc. Nephrol. 1997, 8, 314–322. [Google Scholar] [PubMed]
- Hilhorst, M.; Wilde, B.; Van Paassen, P.; Winkens, B.; Vriesman, P.V.B.; Tervaert, J.W.C. Improved outcome in anti-neutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis: A 30-year follow-up study. Nephrol. Dial. Transplant. 2013, 28, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajema, I.M.; Hagen, E.C.; Hansen, B.E.; Waldherr, R.; Van Der Woude, F.J.; Bruijn, J.A.; Hermans, J.; Noël, L.H.; Ferrario, F. The renal histopathology in systemic vasculitis: An international survey study of inter- and intra-observer agreement. Nephrol. Dial. Transplant. 1996, 11, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Millet, A.; Pederzoli-Ribeil, M.; Guillevin, L.; Witko-Sarsat, V.; Mouthon, L. Antineutrophil cytoplasmic antibody-associated vasculitides: Is it time to split up the group? Ann. Rheum. Dis. 2013, 72, 1273–1279. [Google Scholar] [CrossRef] [Green Version]
- Kronbichler, A.; Lee, K.H.; Denicolo, S.; Choi, D.; Lee, H.; Ahn, D.; Kim, K.H.; Lee, J.H.; Kim, H.; Hwang, M.; et al. Immunopathogenesis of ANCA-Associated Vasculitis. Int. J. Mol. Sci. 2020, 21, 7319. [Google Scholar] [CrossRef]
- Kronbichler, A.; Jayne, D.R. ANCA Renal Risk Score: Is prediction of end-stage renal disease at baseline possible? Kidney Int. 2018, 94, 1045–1047. [Google Scholar] [CrossRef]
- Kronbichler, A.; Jayne, D.R.W. Estimating the epidemiology of anti-neutrophil cytoplasm antibody-associated renal vasculitis and the role of histologic chronicity in predicting renal outcomes. Nephrol. Dial. Transplant. 2019, 34, 1429–1432. [Google Scholar] [CrossRef]
- Neumann, I.; Kain, R.; Regele, H.; Soleiman, A.; Kandutsch, S.; Meisl, F.T. Histological and clinical predictors of early and late renal outcome in ANCA-associated vasculitis. Nephrol. Dial. Transplant. 2005, 20, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Ford, S.L.; Polkinghorne, K.R.; Longano, A.; Dowling, J.; Dayan, S.; Kerr, P.G.; Holdsworth, S.R.; Kitching, A.R.; Summers, S.A. Histopathologic and Clinical Predictors of Kidney Outcomes in ANCA-Associated Vasculitis. Am. J. Kidney Dis. 2014, 63, 227–235. [Google Scholar] [CrossRef]
- Córdova-Sánchez, B.M.; Mejía-Vilet, J.M.; Morales-Buenrostro, L.E.; Loyola-Rodríguez, G.; Uribe-Uribe, N.O.; Correa-Rotter, R. Clinical presentation and outcome prediction of clinical, serological, and histopathological classification schemes in ANCA-associated vasculitis with renal involvement. Clin. Rheumatol. 2016, 35, 1805–1816. [Google Scholar] [CrossRef]
- van Daalen, E.E. Podocytes and Proteinuria in ANCA-Associated Glomerulonephritis: A Case-Control Study. Front. Immunol. 2019, 10, 1405. [Google Scholar] [CrossRef]
- Rihova, Z.; Jancova, E.; Merta, M.; Rysava, R.; Reiterova, J.; Zabka, J.; Tesař, V. Long-Term Outcome of Patients with Antineutrophil Cytoplasmic Autoantibody-Associated Vasculitis with Renal Involvement. Kidney Blood Press. Res. 2005, 28, 144–152. [Google Scholar] [CrossRef]
- de Lind van Wijngaarden, R.A.; Hauer, H.A.; Wolterbeek, R.; Jayne, D.R.; Gaskin, G.; Rasmussen, N.; Noël, L.-H.; Ferrario, F.; Waldherr, R.; Hagen, E.C.; et al. Clinical and Histologic Determinants of Renal Outcome in ANCA-Associated Vasculitis: A Prospective Analysis of 100 Patients with Severe Renal Involvement. J. Am. Soc. Nephrol. 2006, 17, 2264–2274. [Google Scholar] [CrossRef]
- De Joode, A.A.E.; Sanders, J.S.F.; Stegeman, C.A. Renal Survival in Proteinase 3 and Myeloperoxidase ANCA-Associated Systemic Vasculitis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1709–1717. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| No. of kidney biopsies | 49 |
| Clinical data | |
| Female sex—no. (%) | 22 (44.9) |
| Age (IQR)—years | 66 (55–74.5) |
| Disease activity | |
| CRP (IQR)—mg/L | 63.6 (23.4–109) |
| BVAS (IQR)—points | 18 (15–21) |
| Pulmonary hemorrhage—no. (%) | 7 (14.3) |
| Skin involvement—no. (%) | 7 (14.3) |
| Kidney injury | |
| Serum creatinine (IQR)—μmol/L | 272 (123–437) |
| GFR (IQR)—mL/min/1.73 m2 | 17.6 (9.7–47.9) |
| Urinary findings | |
| uPCR (IQR)—mg/g creatinine | 977 (573–1939) |
| uACR (IQR)—mg/g creatinine | 458 (202–938) |
| α1-microglobulin (IQR)—mg/g creatinine | 69.6 (34.9–174) |
| Glomerular lesions | |
| Median total glomeruli (IQR)—no. | 17 (11–28) |
| Median normal glomeruli (IQR)—% | 45.5 (25.2–73) |
| Median glomerular necrosis (IQR)—% | 15.2 (0–44.7) |
| Median glomerular crescents (IQR)—% | 33.3 (10–55.1) |
| Median glomerular sclerosis (IQR)—% | 5.1 (0–26.5) |
| Berden score | |
| Focal class—no. (%) | 23 (46.9) |
| Crescentic class—no. (%) | 16 (32.7) |
| Sclerotic class—no. (%) | 3 (6.1) |
| Mixed class—no. (%) | 7 (14.3) |
| ARRS | |
| Low risk—no. (%) | 18 (36.7) |
| Medium risk—no. (%) | 23 (46.9) |
| High risk—no. (%) | 8 (16.3) |
| MPO-ANCA GN | PR3-ANCA GN | p Value | |
|---|---|---|---|
| No. of kidney biopsies | 25 | 24 | 0.2012 |
| Clinical data | |||
| Female sex—no. (%) | 9 (36) | 13 (54) | 0.2012 |
| Age (IQR)—years | 61 (52–70) | 69.5 (55–76) | 0.2222 |
| Disease activity | |||
| CRP (IQR)—mg/L | 57.4 (24–102) | 67.6 (21.9–118) | 0.5354 |
| BVAS (IQR)—points | 18 (14–21) | 19 (16–20.8) | 0.3929 |
| Pulmonary hemorrhage—no. (%) | 3 (12) | 4 (16.7) | 0.4607 |
| Skin involvement—no. (%) | 4 (16) | 3 (12.5) | 0.7263 |
| Kidney injury | |||
| Serum creatinine (IQR)—μmol/L | 367 (158–578) | 181 (80.9–306) | 0.0027 |
| GFR (IQR)—mL/min/1.73 m2 | 13.7 (8.3–28.8) | 27.2 (14–71.6) | 0.0076 |
| Urinary findings | |||
| uPCR (IQR)—mg/g creatinine | 1446 (671–3476) | 719 (490–1319) | 0.0199 |
| uACR (IQR)—mg/g creatinine | 692 (337–2097) | 338 (103–739) | 0.0119 |
| α1−microglobulin (IQR)—mg/g creatinine | 101 (34.9–205) | 62.7 (36.7–122) | 0.3479 |
| MPO-ANCA GN | PR3-ANCA GN | p Value | |
|---|---|---|---|
| No. of kidney biopsies | 25 | 24 | |
| Glomerular lesions | |||
| Median normal glomeruli (IQR)—% | 35.3 (11.1–61.5) | 56.3 (38.4–81.4) | 0.0071 |
| Median glomerular necrosis (IQR)—% | 16.7 (0–48.3) | 14.2 (0.9–43.5) | 0.6704 |
| Median glomerular crescents (IQR)—% | 37.5 (14.8–69.1) | 27.9 (8.2–49.7) | 0.1355 |
| Median glomerular sclerosis (IQR)—% | 10 (0–38.2) | 4.4 (0–17.2) | 0.2401 |
| Berden score | |||
| Focal class—no. (%) | 9 (36) | 14 (58.3) | |
| Crescentic class—no. (%) | 10 (40) | 6 (25) | |
| Sclerotic class—no. (%) | 3 (12) | 0 (0) | |
| Mixed class—no. (%) | 3 (12) | 4 (16.7) | 0.1569 |
| ARRS | |||
| Low risk—no. (%) | 6 (24) | 12 (50) | |
| Medium risk—no. (%) | 12 (48) | 11 (45.8) | |
| High risk—no. (%) | 7 (28) | 1 (4.2) | 0.0383 |
| Banff Lesion Score | Spearman’s ρ | p Value |
|---|---|---|
| Interstitial inflammation: i | 0.254 | 0.0783 |
| Tubulitis: t | 0.182 | 0.2104 |
| Arteritis: v | 0.401 | 0.0085 |
| Glomerulitis: g | −0.065 | 0.6559 |
| Interstitial fibrosis: ci | 0.351 | 0.0135 |
| Tubular atrophy: ct | 0.316 | 0.0272 |
| Arteriolar hyalinosis: ah | 0.109 | 0.4675 |
| Peritubular capillaritis: ptc | 0.195 | 0.1784 |
| Total inflammation: ti | 0.305 | 0.0330 |
| Inflammation in areas of IFTA: i-IFTA | 0.130 | 0.3742 |
| Tubulitis in areas of IFTA: t-IFTA | 0.209 | 0.1496 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hakroush, S.; Kluge, I.A.; Ströbel, P.; Korsten, P.; Tampe, D.; Tampe, B. Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis. J. Clin. Med. 2021, 10, 1231. https://doi.org/10.3390/jcm10061231
Hakroush S, Kluge IA, Ströbel P, Korsten P, Tampe D, Tampe B. Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis. Journal of Clinical Medicine. 2021; 10(6):1231. https://doi.org/10.3390/jcm10061231
Chicago/Turabian StyleHakroush, Samy, Ingmar Alexander Kluge, Philipp Ströbel, Peter Korsten, Désirée Tampe, and Björn Tampe. 2021. "Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis" Journal of Clinical Medicine 10, no. 6: 1231. https://doi.org/10.3390/jcm10061231