
Impact of Acetate versus Citrate Dialysates on Intermediary Metabolism—A Targeted Metabolomics Approach
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Participants
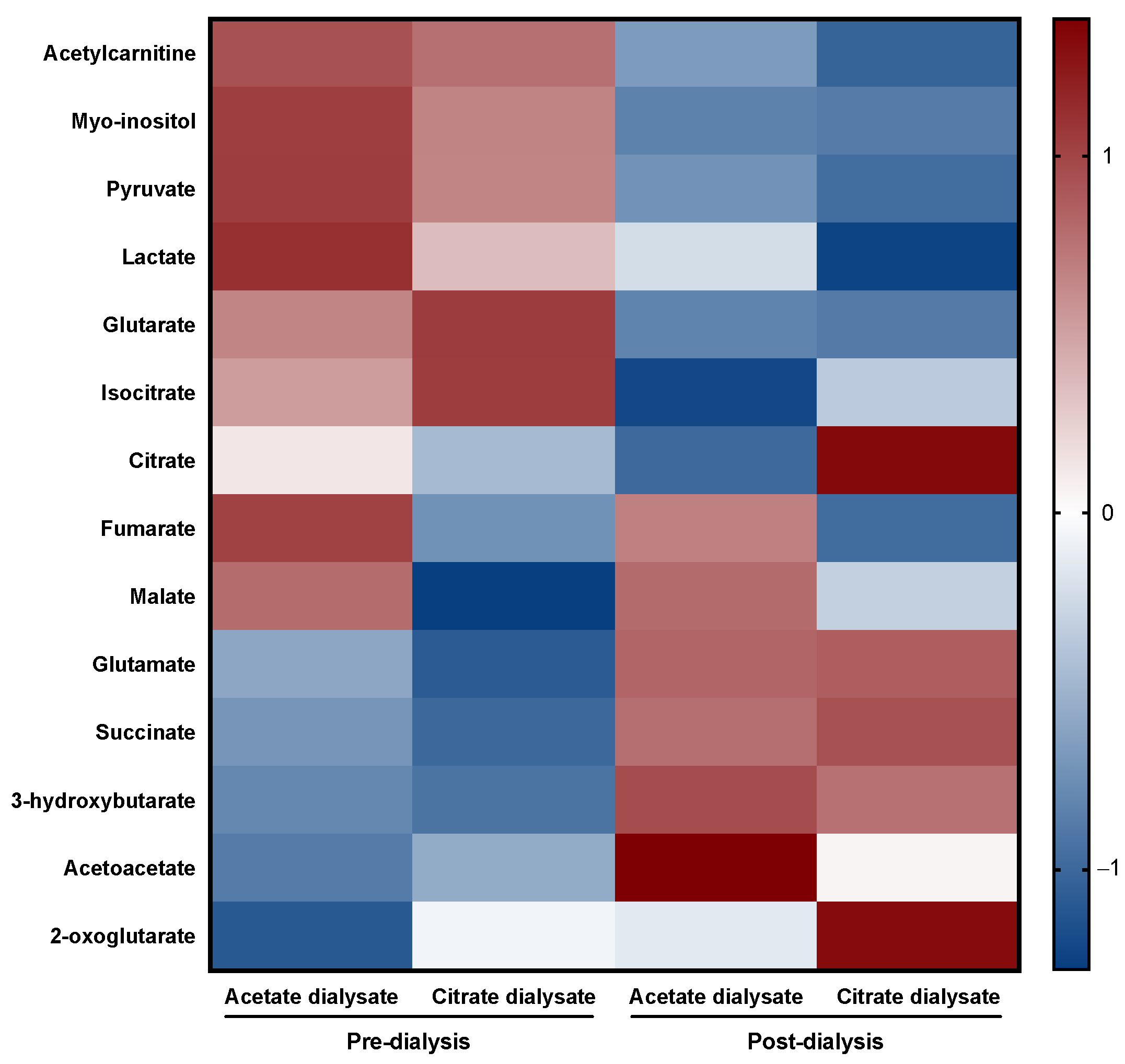
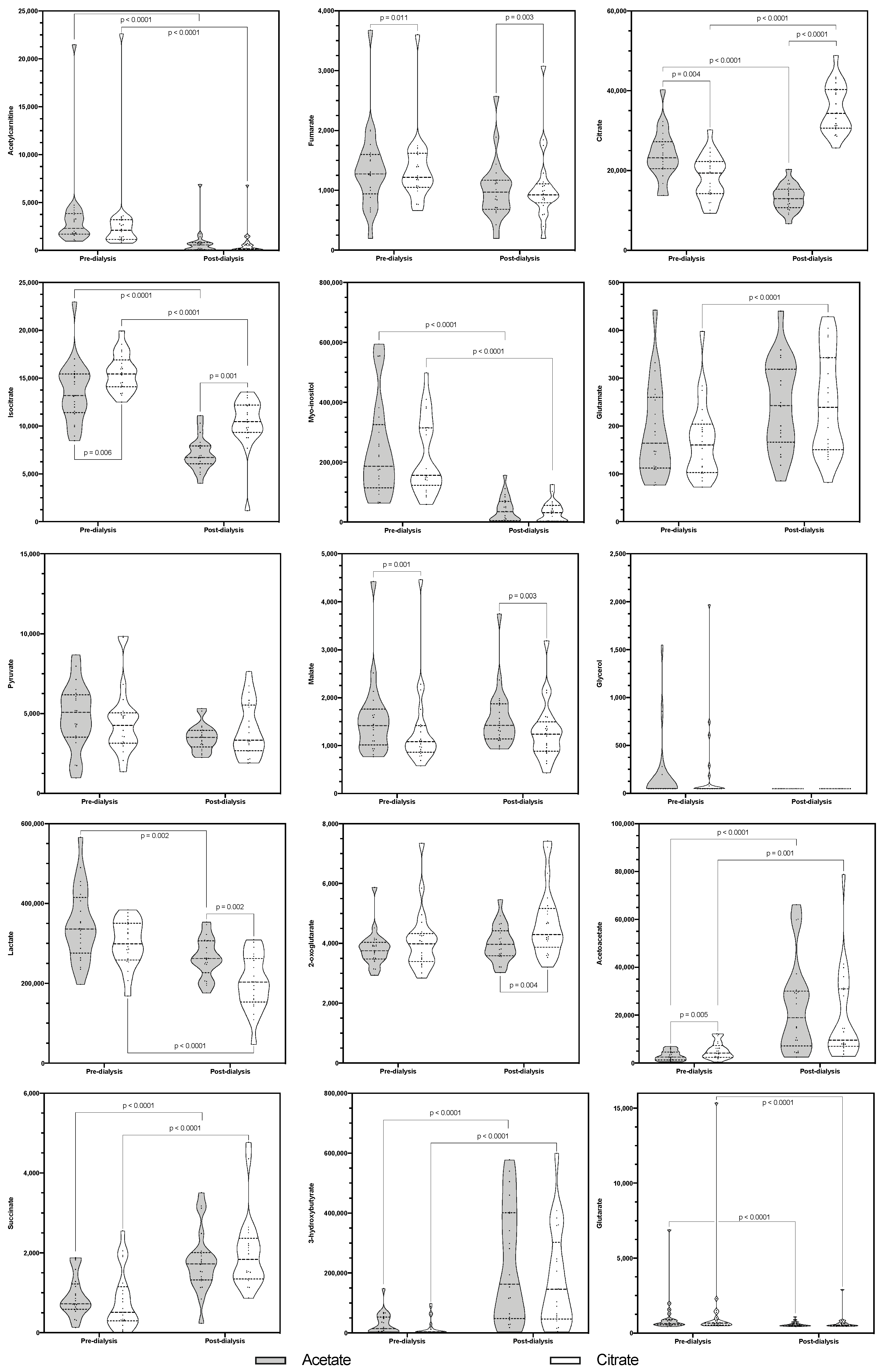
2.2. Metabolomic Analysis
2.2.1. Acetylcarnitine
2.2.2. Fumarate
2.2.3. Citrate
2.2.4. Isocitrate
2.2.5. Myo-Inositol
2.2.6. Glutamate
2.2.7. Pyruvate
2.2.8. Malate
2.2.9. Glycerol
2.2.10. Lactate
2.2.11. 2-Oxoglutarate
2.2.12. Acetoacetate
2.2.13. Succinate
2.2.14. 3-hydroxybutyrate
2.2.15. Glutarate
3. Discussion
3.1. First Carbon Oxidation Pathway of the TCA Cycle-Related Metabolites
3.2. Second Carbon Oxidation Pathway of the TCA-Cycle Related Metabolites
3.3. Glycolysis and Anaerobic Metabolism-Related Metabolites
3.4. Lipidic Metabolism-Related Metabolites
3.5. Amionoacidic Metabolism-Related Metabolites
3.6. Limitations
4. Materials and Methods
4.1. Study Design and Participants
4.2. Variables
4.3. Sample Preparation and Metabolomic Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stegmayr, B. Dialysis Procedures Alter Metabolic Conditions. Nutrients 2017, 9, 548. [Google Scholar] [CrossRef] [PubMed]
- Hocher, B.; Adamski, J. Metabolomics for clinical use and research in chronic kidney disease. Nat. Rev. Nephrol. 2017, 13, 269–284. Available online: https://pubmed.ncbi.nlm.nih.gov/28262773/ (accessed on 7 August 2021). [CrossRef] [PubMed]
- Zhu, S.; Zhang, F.; Shen, A.-W.; Sun, B.; Xia, T.-Y.; Chen, W.-S.; Tao, X.; Yu, S.-Q. Metabolomics Evaluation of Patients with Stage 5 Chronic Kidney Disease before Dialysis, Maintenance Hemodialysis, and Peritoneal Dialysis. Front. Physiol. 2021, 11, 630646. Available online: https://pubmed.ncbi.nlm.nih.gov/33551851/ (accessed on 7 August 2021). [CrossRef] [PubMed]
- Kalantari, S.; Nafar, M. An update of urine and blood metabolomics in chronic kidney disease. Biomark. Med. 2019, 13, 577–597. Available online: https://pubmed.ncbi.nlm.nih.gov/31140832/ (accessed on 7 August 2021). [CrossRef]
- Tamura, M.K.; Chertow, G.M.; Depner, T.A.; Nissenson, A.R.; Schiller, B.; Mehta, R.L.; Liu, S.; Sirich, T.L. Metabolic Profiling of Impaired Cognitive Function in Patients Receiving Dialysis. J. Am. Soc. Nephrol. 2016, 27, 3780–3787. Available online: https://pubmed.ncbi.nlm.nih.gov/27444566/ (accessed on 7 August 2021). [CrossRef] [Green Version]
- Hu, J.-R.; Grams, M.E.; Coresh, J.; Hwang, S.; Kovesdy, C.P.; Guallar, E.; Rhee, E.P.; Shafi, T. Serum Metabolites and Cardiac Death in Patients on Hemodialysis. Clin. J. Am. Soc. Nephrol. 2019, 14, 747–749. Available online: https://pubmed.ncbi.nlm.nih.gov/30962187/ (accessed on 7 August 2021). [CrossRef]
- Petitclerc, T.; Diab, R.; le Roy, F.; Mercadal, L.; Hmida, J. Hémodialyse sans acétate: Qu’est-ce vraiment? Néphrologie Thérapeutique 2011, 7, 92–98. [Google Scholar] [CrossRef]
- Sánchez-Canel, J.J.; Hernández-Jaras, J.; Pons-Prades, R. A Randomized Controlled Study on the Effects of Acetate-Free Biofiltration on Organic Anions and Acid-Base Balance in Hemodialysis Patients. Ther. Apher. Dial. 2015, 19, 63–72. [Google Scholar] [CrossRef]
- Broseta, J.J.; López-Romero, L.C.; Cerveró, A.; Devesa-Such, R.; Soldevila, A.; Bea-Granell, S.; Sánchez-Pérez, P.; Hernández-Jaras, J. Improvements in Inflammation and Calcium Balance of Citrate versus Acetate as Dialysate Buffer in Maintenance Hemodialysis: A Unicentric, Cross-Over, Prospective Study. Blood Purif. 2021, 50, 914–920. [Google Scholar] [CrossRef]
- Dellepiane, S.; Medica, D.; Guarena, C.; Musso, T.; Quercia, A.D.; Leonardi, G.; Marengo, M.; Migliori, M.; Panichi, V.; Biancone, L.; et al. Citrate anion improves chronic dialysis efficacy, reduces systemic inflammation and prevents Chemerin-mediated microvascular injury. Sci. Rep. 2019, 9, 10622. [Google Scholar] [CrossRef]
- Gabutti, L.; Lucchini, B.; Marone, C.; Alberio, L.; Burnier, M. Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis: Consequences on haemodynamics, coagulation, acid-base status, and electrolytes. BMC Nephrol. 2009, 10, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-García, R.; Chamond, R.R.; Ortiz, P.D.S.; Albalate, M.; Carretero, M.P.; Ortega, M.; Caro, M.C.R.; Arroyo, R.A. Citrate dialysate does not induce oxidative stress or inflammation in vitro as compared to acetate dialysate. Nefrologia 2017, 37, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Grundström, G.; Christensson, A.; Alquist, M.; Nilsson, L.G.; Segelmark, M. Replacement of acetate with citrate in dialysis fluid: A randomized clinical trial of short term safety and fluid biocompatibility. BMC Nephrol. 2013, 14, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sands, J.J.; Kotanko, P.; Segal, J.H.; Ho, C.-H.; Usvat, L.; Young, A.; Carter, M.; Sergeyeva, O.; Korth, L.; Maunsell, E.; et al. Effects of citrate acid concentrate (Citrasate®) on heparin N requirements and hemodialysis adequacy: A multicenter, prospective noninferiority trial. Blood Purif. 2012, 33, 199–204. [Google Scholar] [CrossRef]
- Trakarnvanich, T.; Thirathanakul, S.; Sriphueng, N.; Thumrongthongjaroon, P.; Kurathong, S.; Ngamvichchukorn, T. The effect of citrate on clot formation, dialyzer reuse, and anemia in hemodialysis patients. Blood Purif. 2019, 47, 361–368. [Google Scholar] [CrossRef]
- Rocha, A.D.; Padua, V.C.; Oliveira, E.; Guimaraes, M.M.; Lugon, J.R.; Strogoff de Matos, J.P. Effects of citrate-enriched bicarbonate based dialysate on anticoagulation and dialyzer reuse in maintenance hemodialysis patients. Hemodial. Int. 2014, 18, 467–472. [Google Scholar] [CrossRef]
- Zarbock, A.; Küllmar, M.; Kindgen-Milles, D.; Wempe, C.; Gerss, J.; Brandenburger, T.; Dimski, T.; Tyczynski, B.; Jahn, M.; Mülling, N.; et al. Effect of Regional Citrate Anticoagulation vs Systemic Heparin Anticoagulation during Continuous Kidney Replacement Therapy on Dialysis Filter Life Span and Mortality among Critically Ill Patients with Acute Kidney Injury: A Randomized Clinical Trial. JAMA—J. Am. Med. Assoc. 2020, 324, 1629–1639. Available online: https://pubmed.ncbi.nlm.nih.gov/33095849/ (accessed on 7 August 2021). [CrossRef]
- Yamakawa, M.; Yamamoto, T.; Kishimoto, T.; Mizutani, Y.; Yatsuboshi, M.; Nishitani, H.; Hirata, S.; Horiuchi, N.; Maekawa, M. Serum levels of acetate and TCA cycle intermediates during hemodialysis in relation to symptoms. Nephron 1982, 32, 155–161. Available online: https://pubmed.ncbi.nlm.nih.gov/7177293/ (accessed on 29 December 2021). [CrossRef]
- Kuragano, T.; Kida, A.; Furuta, M.; Yahiro, M.; Kitamura, R.; Otaki, Y.; Nonoguchi, H.; Matsumoto, A.; Nakanishi, T. Effects of Acetate-Free Citrate-Containing Dialysate on Metabolic Acidosis, Anemia, and Malnutrition in Hemodialysis Patients. Artif. Organs 2012, 36, 282–290. [Google Scholar] [CrossRef]
- Lorenz, G.; Mayer, C.C.; Bachmann, Q.; Stryeck, S.; Braunisch, M.C.; Haller, B.; Carbajo-Lozoya, J.; Schmidt, A.; Witthauer, S.; Abuzahu, J.; et al. Acetate-free, citrate-acidified bicarbonate dialysis improves serum calcification propensity—A preliminary study. Nephrol. Dial. Transplant. 2018, 33, 2043–2051. Available online: https://academic.oup.com/ndt/advance-article/doi/10.1093/ndt/gfy134/5025720 (accessed on 20 June 2018). [CrossRef]
- Bryland, A.; Wieslander, A.; Carlsson, O.; Hellmark, T.; Godaly, G. Citrate treatment reduces endothelial death and inflammation under hyperglycaemic conditions. Diabetes Vasc. Dis. Res. 2012, 9, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fournier, G.; Potier, J.; Thébaud, H.E.; Majdalani, G.; Ton-That, H.; Man, N.K. Substitution of acetic acid for hydrochloric acid in the bicarbonate buffered dialysate. Artif. Organs 1998, 22, 608–613. Available online: https://pubmed.ncbi.nlm.nih.gov/9684700/ (accessed on 7 July 2022). [CrossRef] [PubMed]
- Kishimoto, T.; Yamamoto, T.; Yamamoto, K.; Yamagami, S.; Nishitani, H.; Mizutani, Y.; Yamakawa, M.; Maekawa, M. Acetate Kinetics during Hemodialysis and Hemofiltration. Blood Purif. 1984, 2, 81–87. Available online: https://www.karger.com/Article/FullText/169316 (accessed on 7 July 2022). [CrossRef]
- Hernández-Jaras, J.; Estrada, A.; García-Cantón, C.; Traver, J. Equilibrio ácido-base y aniones orgánicos: Diferencias en biofiltración con acetato (bf) y hemodiálisis con bicarbonato. Nefrología 1994, 14, 591–597. Available online: https://www.revistanefrologia.com/es-equilibrio-acido-base-aniones-organicos-diferencias-articulo-X0211699594006762 (accessed on 11 July 2022).
- Lundquist, F. Production and utilization of free acetate in man. Nature 1962, 193, 579–580. Available online: https://pubmed.ncbi.nlm.nih.gov/14467396/ (accessed on 29 December 2021). [CrossRef]
- Hoffmann, G.F.; Meier-Augenstein, W.; Stöckler, S.; Surtees, R.; Rating, D.; Nyhan, W.L. Physiology and pathophysiology of organic acids in cerebrospinal fluid. J. Inherit. Metab. Dis. 1993, 16, 648–669. Available online: https://pubmed.ncbi.nlm.nih.gov/8412012/ (accessed on 6 July 2022). [CrossRef]
- Zordoky, B.; Sung, M.M.; Ezekowitz, J.; Mandal, R.; Han, B.; Bjorndahl, T.C.; Bouatra, S.; Anderson, T.; Oudit, G.Y.; Wishart, D.S.; et al. Metabolomic fingerprint of heart failure with preserved ejection fraction. PLoS ONE 2015, 10, e0124844. Available online: https://pubmed.ncbi.nlm.nih.gov/26010610/ (accessed on 6 July 2022).
- Wu, N.; Yang, M.; Gaur, U.; Xu, H.; Yao, Y.; Li, D. Alpha-Ketoglutarate: Physiological Functions and Applications. Biomol Ther 2016, 24, 1–8. Available online: https://pubmed.ncbi.nlm.nih.gov/26759695/ (accessed on 6 July 2022). [CrossRef] [Green Version]
- Psychogios, N.; Hau, D.D.; Peng, J.; Guo, A.C.; Mandal, R.; Bouatra, S.; Sinelnikov, I.; Krishnamurthy, R.; Eisner, R.; Gautam, B.; et al. The human serum metabolome. PLoS ONE 2011, 6, e16957. Available online: https://pubmed.ncbi.nlm.nih.gov/21359215/ (accessed on 6 July 2022). [CrossRef] [Green Version]
- Martínez-Reyes, I.; Chandel, N.S. Mitochondrial TCA cycle metabolites control physiology and disease. Nat. Commun. 2020, 11, 102. Available online: https://www.nature.com/articles/s41467-019-13668-3 (accessed on 6 July 2022). [CrossRef] [Green Version]
- Klysz, D.; Tai, X.; Robert, P.A.; Craveiro, M.; Cretenet, G.; Oburoglu, L.; Mongellaz, C.; Floess, S.; Fritz, V.; Matias, M.I.; et al. Glutamine-dependent α-ketoglutarate production regulates the balance between T helper 1 cell and regulatory T cell generation. Sci. Signal. 2015, 8, ra97. Available online: https://pubmed.ncbi.nlm.nih.gov/26420908/ (accessed on 6 July 2022). [CrossRef] [PubMed] [Green Version]
- Sargent, J.A.; Marano, M.; Marano, S.; Gennari, F.J. Acid-base homeostasis during hemodialysis: New insights into the mystery of bicarbonate disappearance during treatment. Semin. Dial. 2018, 31, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Bellinghieri, G.; Santoro, D.; Calvani, M.; Mallamace, A.; Savica, V. Carnitine and hemodialysis. Am. J. Kidney Dis. 2003, 41, S116–S122. Available online: https://pubmed.ncbi.nlm.nih.gov/12612967/ (accessed on 6 July 2022). [CrossRef] [PubMed] [Green Version]
- Virmani, A.; Binienda, Z. Role of carnitine esters in brain neuropathology. Mol. Aspects Med. 2004, 25, 533–549. Available online: https://pubmed.ncbi.nlm.nih.gov/15363640/ (accessed on 6 July 2022). [CrossRef]
- Blomqvist, G.; Alvarsson, M.; Grill, V.; Von Heijne, G.; Ingvar, M.; Thorell, J.O.; Stone-Elander, S.; Widén, L.; Ekberg, K. Effect of acute hyperketonemia on the cerebral uptake of ketone bodies in nondiabetic subjects and IDDM patients. Am. J. Physiol. Endocrinol. Metab. 2002, 283, E20–E28. Available online: https://pubmed.ncbi.nlm.nih.gov/12067838/ (accessed on 6 July 2022). [CrossRef] [Green Version]
- Burns, S.F.; Broom, D.R.; Miyashita, M.; Ueda, C.; Stensel, D.J. Increased postprandial triacylglycerol concentrations following resistance exercise. Med. Sci. Sports Exerc. 2006, 38, 527–533. Available online: https://pubmed.ncbi.nlm.nih.gov/16540841/ (accessed on 6 July 2022). [CrossRef]
- Obokata, M.; Negishi, K.; Sunaga, H.; Ishida, H.; Ito, K.; Ogawa, T.; Iso, T.; Ando, Y.; Kurabayashi, M. Association between circulating ketone bodies and worse outcomes in hemodialysis patients. J. Am. Heart Assoc. 2017, 6, e006885. [Google Scholar] [CrossRef] [Green Version]
- Trabado, S.; Al-Salameh, A.; Croixmarie, V.; Masson, P.; Corruble, E.; Fève, B.; Colle, R.; Ripoll, L.; Walther, B.; Boursier-Neyret, C.; et al. The human plasma-metabolome: Reference values in 800 French healthy volunteers; impact of cholesterol, gender and age. PLoS ONE 2017, 12, e0173615. Available online: https://pubmed.ncbi.nlm.nih.gov/28278231/ (accessed on 6 July 2022). [CrossRef] [Green Version]
- Hendriks, F.K.; Smeets, J.S.J.; Broers, N.J.H.; van Kranenburg, J.M.X.; van der Sande, F.M.; Kooman, J.P.; van Loon, L.J.C. End-Stage Renal Disease Patients Lose a Substantial Amount of Amino Acids during Hemodialysis. J. Nutr. 2020, 150, 1160–1166. Available online: https://academic.oup.com/jn/article/150/5/1160/5719508 (accessed on 8 July 2022). [CrossRef] [Green Version]
- Lim, V.S.; Bier, D.M.; Flanigan, M.J.; Sum-Ping, S.T. The effect of hemodialysis on protein metabolism. A leucine kinetic study. J. Clin. Investig. 1993, 91, 2429–2436. Available online: https://pubmed.ncbi.nlm.nih.gov/8514855/ (accessed on 8 July 2022). [CrossRef]



{kind=link}
{kind=link}
| Metabolite (µg/L) | Acetate Dialysate | Citrate Dialysate | ||
|---|---|---|---|---|
| Pre-Dialysis | Post-Dialysis | Pre-Dialysis | Post-Dialysis | |
| Acetylcarnitine | 2292.83 (1698.3–3835.64) | 565.12 (75–814.56) | 2108.21 (1138.39–3206.01) | 164.52 (75–643.1) |
| Fumarate | 1275.33 (940.83–1597.34) | 1215.87 (1050.27–1617.92) | 968.72 (682.95–1169.75) | 924.19 (790.46–1109.45) |
| Citrate | 23,930.01 ± 6243.63 | 13,151.82 ± 3245.25 | 18,312.77 ± 5534.11 | 35,351.74 ± 6126.8 |
| Isocitrate | 13,181.79 (11,407.72–15,441.07) | 6717.97 (6051.02–7927.15) | 15,438.28 (14,109.91–16,918.49) | 10,463.95 (9330.3–12,195.79) |
| Myo-inositol | 186,825.86 (115,033.27–325,459.59) | 34,635.77 (4328.17–69,297.23) | 156,509.77 (123,131.02–315,150.31) | 31,586.57 (3125–55,889.43) |
| Glutamate | 164.33 (112.36–260.19) | 242.62 (166.44–318.71) | 160.35 (102.76–204.39) | 239.09 (150.69–342.67) |
| Pyruvate | 5075.38 (3526.28–6168.7) | 3509.35 (2905.18–3952.23) | 4253.1 (3135.06–5031.68) | 3322.45 (2664.53–5529.55) |
| Malate | 1418.21 (1015.39–1760.36) | 1418.82 (1138.72–1869.07) | 1080.15 (860.11–1416.11) | 1238.32 (879.48–1496.05) |
| Glycerol | 48.5 (48.5–48.5) | 48.5 (48.5–48.5) | 48.5 (48.5–129.6) | 48.5 (48.5–48.5) |
| Lactate | 347,331.76 ± 91,933.58 | 263,698.08 ± 49,573.01 | 299,899.63 ± 57,695.8 | 200,315.81 ± 68,510.44 |
| 2-oxoglutarate | 3755.05 (3476.57–4032.21) | 3968.36 (3587–4421.18) | 3984.51 (3393.35–4323.3) | 4290.49 (3868.34–5168.94) |
| Acetoacetate | 2473.04 (1277.63–4600.98) | 18,926.55 (7189.31–30,038.77) | 4166.43 (2374.53–7277.45) | 9580.02 (6992.68–30,978.53) |
| Succinate | 722.6 (588.57–1221.9) | 1725.48 (1325.02–2012.26) | 515.06 (297.41–1150.89) | 1838.29 (1344.81–2370.32) |
| 3-hydroxybutyrate | 14,338.64 (3125–53,089.27) | 162,982.81 (48,176.41–401,805.24) | 3125 (3125–23,132.58) | 146,012.84 (46,441.35–303,043.91) |
| Glutarate | 636.45 (548.76–906.39) | 530.86 (480.5–618.66) | 664.43 (528.85–922.1) | 526.83 (479.83–668.31) |
| Fresenius ACF 3A5 | Fresenius Smartbag CA 211.5 | |
|---|---|---|
| Sodium (mmol/L) | 140 | 138 |
| Potassium (mmol/L) | 2 | 2 |
| Calcium (mmol/mL) | 1.5 | 1.5 |
| Magnesium (mmol/mL) | 0.5 | 0.5 |
| Chloride (mmol/mL) | 106 | 109 |
| Acetate (mmol/L) | 4 | - |
| Citrate (mmol/L) | - | 1 |
| Glucose (g/L) | 1 | 1 |
| Bicarbonate (mmol/L) | 35 | 32 |
| In-use dilution | 1 + 44 | 1 + 44 |
| Metabolite | Chemical Formula | Molecular Mass (g/mol) | Biochemical Class | Main Metabolic Pathways |
|---|---|---|---|---|
| Acetylcarnitine | C9H17NO4 | 203.236 | Fatty acid esters | Oxidation of fatty acids |
| Fumarate | C4H4O4 | 116.072 | Dicarboxylic acids and derivatives | TCA cycle (2nd carbon oxidation), electron transport chain |
| Citrate | C6H8O7 | 189.1 | Tricarboxylic acids and derivatives | TCA cycle (1st carbon oxidation), transfer of acetyl groups into mitochondria |
| Isocitrate | C6H8O7 | 189.1 | Tricarboxylic acids and derivatives | TCA cycle (1st carbon oxidation) |
| Myo-inositol | C6H12O6 | 180.16 | Alcohols and polyols | Inositol phosphate metabolism, secondary messenger in signal transduction pathways |
| Glutamate | C5H9NO4 | 147.13 | Amino acids, peptides, and analogues | Aminoacidic metabolism |
| Pyruvate | C3H4O3 | 88.06 | Alpha-keto acids and derivatives | Glycolysis, gluconeogenesis, lipogenesis |
| Malate | C4H6O5 | 134.08 | Beta hydroxy acids and derivatives | TCA cycle (2nd carbon oxidation), gluconeogenesis, pyruvate metabolism |
| Glycerol | C3H8O3 | 92.09 | Carbohydrates and carbohydrate conjugates | Triglyceride metabolism |
| Lactate | C3H6O3 | 90.08 | Alpha hydroxy acids and derivatives | Gluconeogenesis, pyruvate metabolism |
| 2-oxoglutarate | C5H6O5 | 146.11 | Gamma-keto acids and derivatives | TCA cycle (1st carbon oxidation), aminoacidic metabolism |
| Acetoacetate | C4H6O3 | 101.08 | Short-chain keto acids and derivatives | Ketone body metabolism, fatty acid biosynthesis |
| Succinate | C4H6O4 | 118.09 | Dicarboxylic acids and derivatives | TCA cycle (2nd carbon oxidation), electron transport chain |
| 3-hydroxybutyrate | C4H8O3 | 103.1 | Beta hydroxy acids and derivatives | Ketone body metabolism, fatty acid biosynthesis |
| Glutarate | C5H8O4 | 147.13 | Dicarboxylic acids and derivatives | Aminoacidic metabolism |
| TCA: Krebs tricarboxylic acid. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Broseta, J.J.; Roca, M.; Rodríguez-Espinosa, D.; López-Romero, L.C.; Gómez-Bori, A.; Cuadrado-Payán, E.; Devesa-Such, R.; Soldevila, A.; Bea-Granell, S.; Sánchez-Pérez, P.; et al. Impact of Acetate versus Citrate Dialysates on Intermediary Metabolism—A Targeted Metabolomics Approach. Int. J. Mol. Sci. 2022, 23, 11693. https://doi.org/10.3390/ijms231911693
Broseta JJ, Roca M, Rodríguez-Espinosa D, López-Romero LC, Gómez-Bori A, Cuadrado-Payán E, Devesa-Such R, Soldevila A, Bea-Granell S, Sánchez-Pérez P, et al. Impact of Acetate versus Citrate Dialysates on Intermediary Metabolism—A Targeted Metabolomics Approach. International Journal of Molecular Sciences. 2022; 23(19):11693. https://doi.org/10.3390/ijms231911693
Chicago/Turabian StyleBroseta, José Jesús, Marta Roca, Diana Rodríguez-Espinosa, Luis Carlos López-Romero, Aina Gómez-Bori, Elena Cuadrado-Payán, Ramón Devesa-Such, Amparo Soldevila, Sergio Bea-Granell, Pilar Sánchez-Pérez, and et al. 2022. "Impact of Acetate versus Citrate Dialysates on Intermediary Metabolism—A Targeted Metabolomics Approach" International Journal of Molecular Sciences 23, no. 19: 11693. https://doi.org/10.3390/ijms231911693