Carbonic Anhydrase IX in Renal Cell Carcinoma, Implications for Disease Management

Abstract
:1. Introduction
2. Evidence Acquisition
3. Evidence Synthesis
3.1. Role of CAIX in RCC Pathophysiology
3.2. CAIX as a Diagnostic Marker
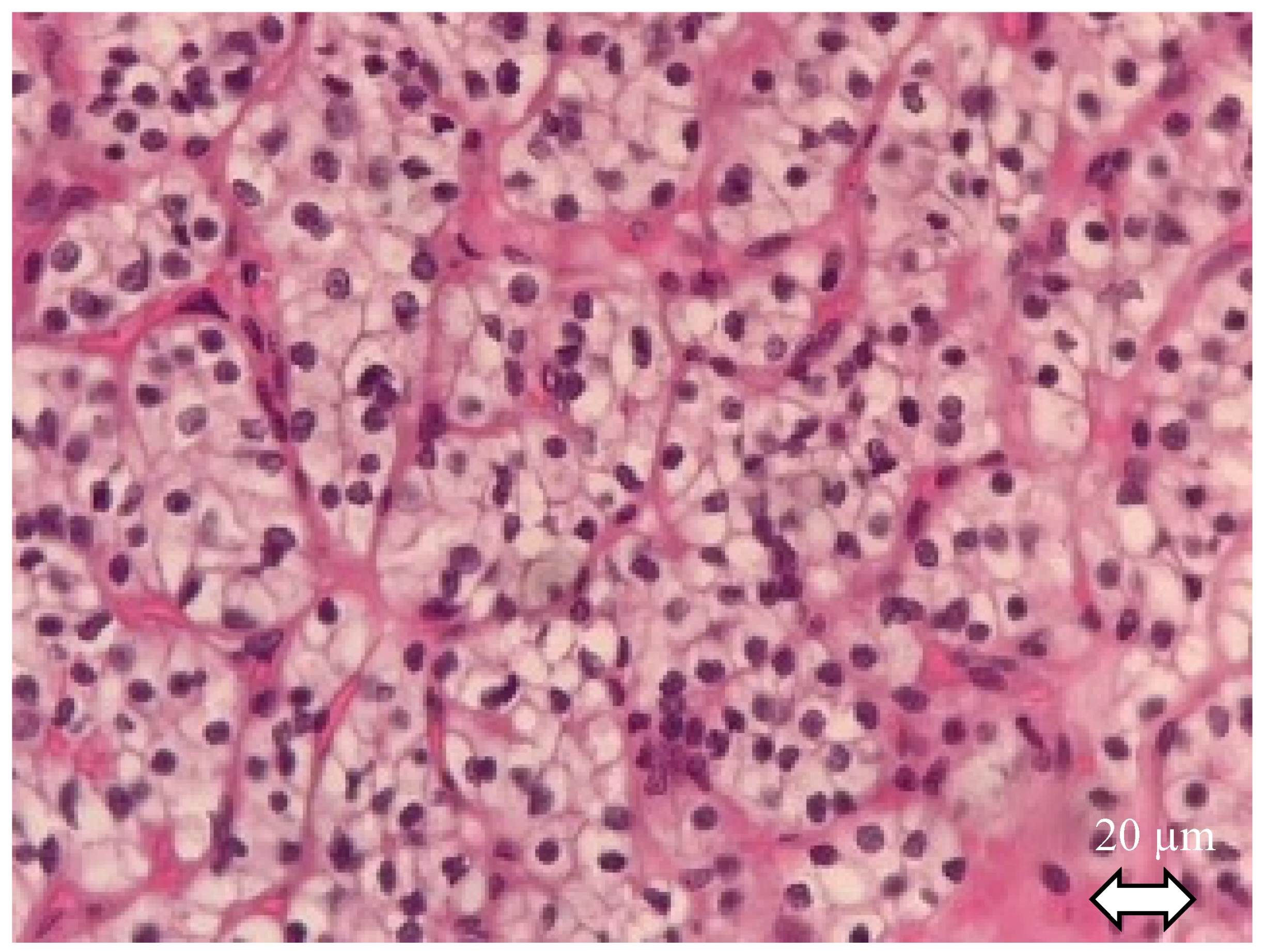
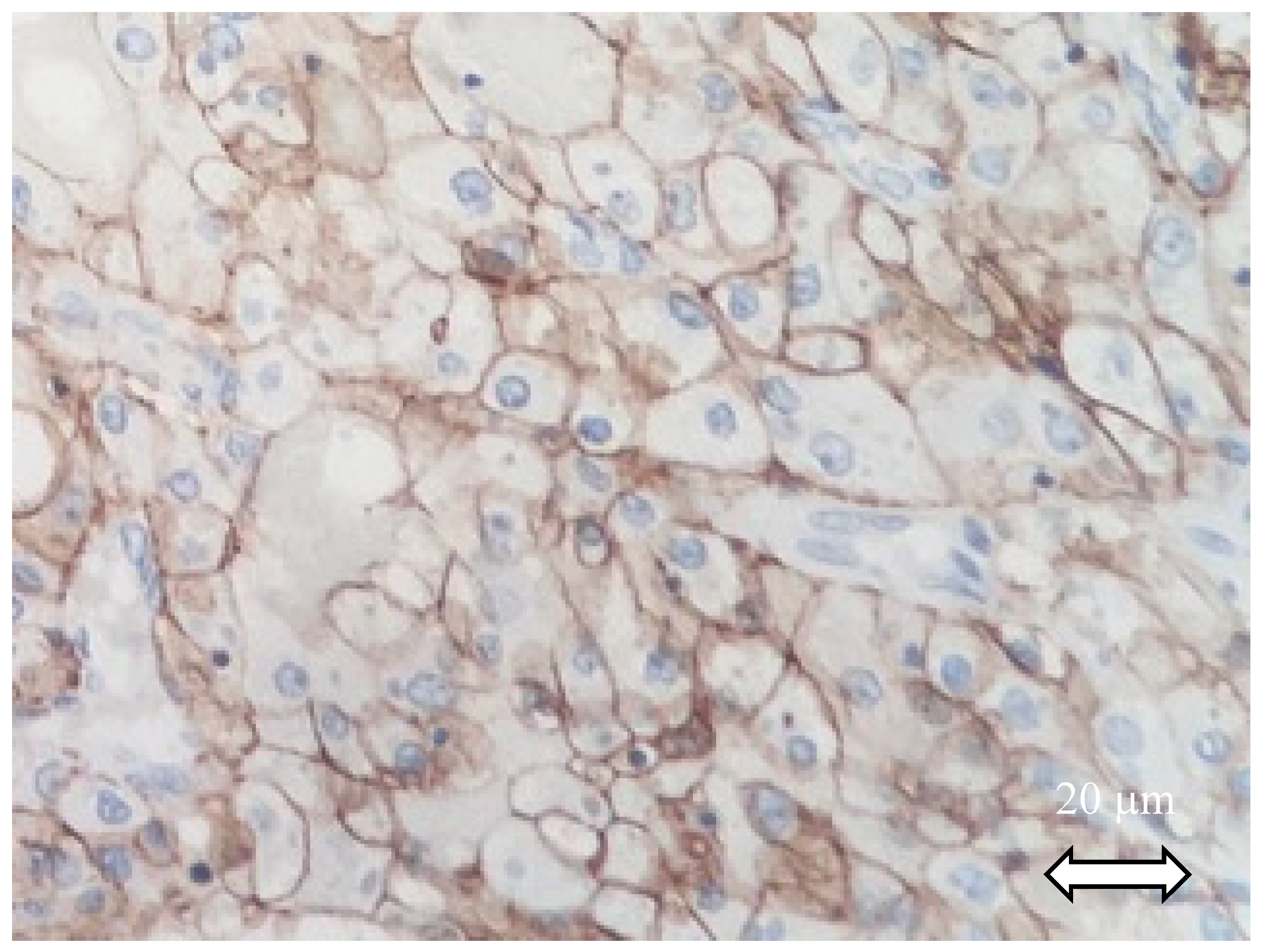
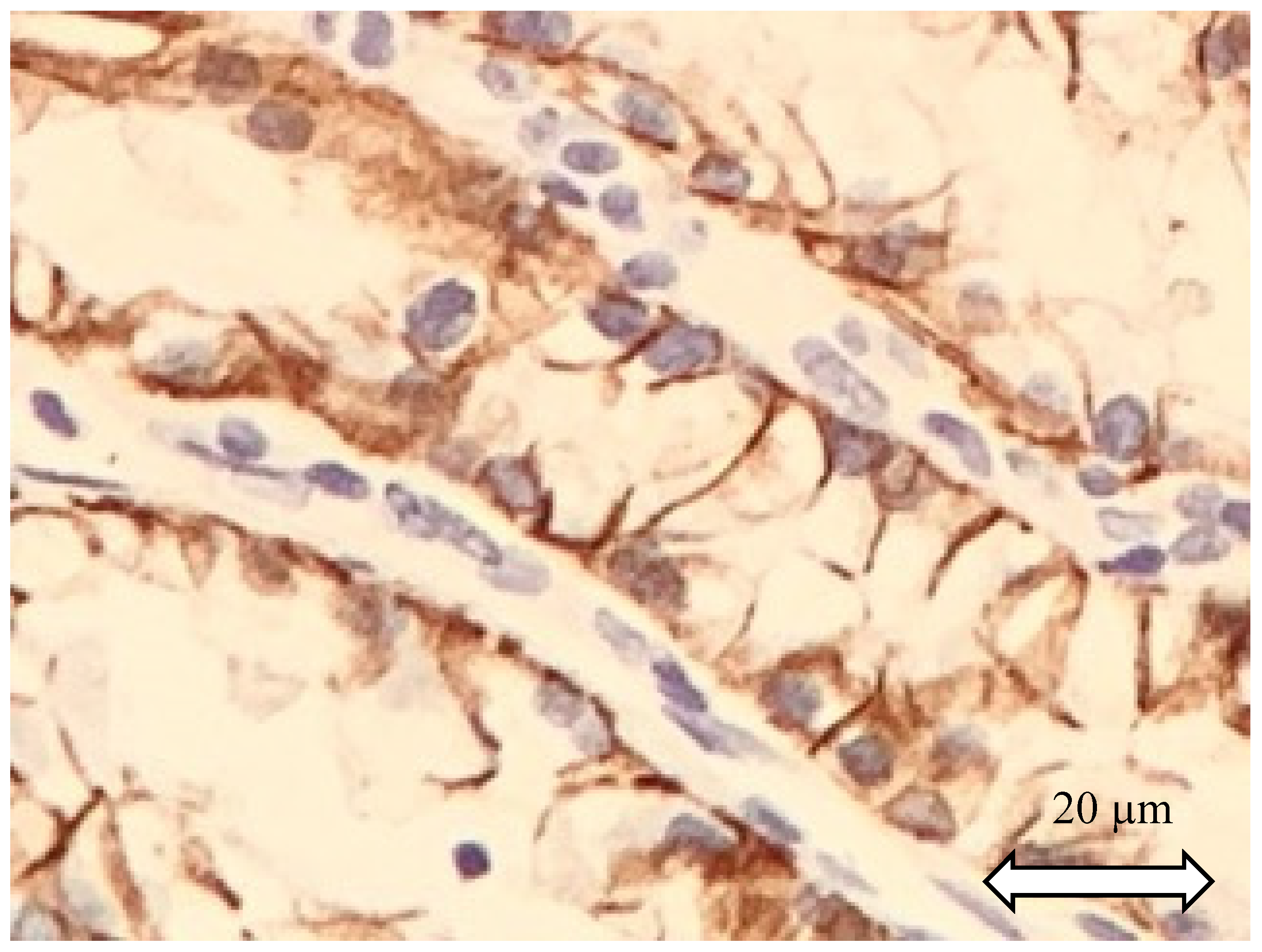
3.2.1. In Immunohistochemistry (IHC)
CAIX IHC Detection Permits Diagnosis of Histological Subtype
Prognostic Implication of CAIX Detection in IHC
CAIX Measured by Immunohistochemistry and Systemic Treatment Response Prediction
3.2.2. Value of Circulating CAIX
Diagnostic Value
Prognostic Value
3.2.3. CAIX and Imaging
CAIX and Conventional CT Scans
Positron Emission Tomography
Ultrasound Molecular Imaging (USMI)
Fluorescence for Facilitation of Peroperative Recognition
3.3. CAIX in Therapeutics
3.3.1. Vaccines and Immune-Mediating
3.3.2. cG250/Girentuximab and Radioimmunotherapy
3.3.3. Sensitization to Radiotherapy Inhibiting CAIX Expression
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AbOmpA | Acinetobacter baumannii outer membrane protein A |
| ADCC | Antibody-dependent cell-mediated cytotoxicity |
| AdGMCA9 | adenovirus encoding the GMCSF-CAIX fusion gene |
| ADCP | Antibody-dependent cellular phagocytosis |
| AMACR | α-Methylacyl-CoA racemase |
| CAIX | Carbonic anhydrase IX |
| ccpRCC | Multilocular cystic renal neoplasm of low malignant potential |
| ccRCC | Clear cell renal cell carcinoma |
| CDC | Complement-dependent cytotoxicity |
| chRCC | Chromophobe renal cell carcinoma |
| CK | Cytokeratine |
| CT | Computed tomography |
| DC | Dendritic cell |
| FDG | Fluorodesoxyglucose |
| GMCF | Granulocyte-macrophage colony stimulating factor |
| HIF | Hypoxia inducible factor |
| HRE | Hypoxia responsive elements |
| IHC | Immunohistochemistry |
| MRI | Magnetic resonance imaging |
| PET | Positron emission tomography |
| pRCC | Papillary renal cell carcinoma |
| RCC | Renal cell carcinoma |
| pVHL | Von Hippel Lindau protein |
| RECIST | Response evaluation criteria in solid tumors |
| SD | Standard deviation |
| SUV | Standardized Uptake Value |
| TKI | Tyrosine kinase inhibitor |
| TFE3 | Transcription factor binding to IGHM enhancer 3 |
| USMI | Ultrasound molecular imaging |
| VEGFR | Vascular endothelial growth factor |
| WHO | World Health Organization |
References
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer Oxf. Engl. 1990, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Professionals, S.-O. EAU Guidelines: Renal Cell Carcinoma, Uroweb. Available online: https://uroweb.org/guideline/renal-cell-carcinoma/ (accessed on 3 August 2020).
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Benej, M.; Pastorekova, S.; Pastorek, J. Carbonic anhydrase IX: Regulation and role in cancer. In Carbonic Anhydrase: Mechanism, Regulation, Links to Disease, and Industrial Applications; Frost, S.C., McKenna, R., Eds.; Springer: Dordrecht, The Netherlands, 2014; Volume 75, pp. 199–219. [Google Scholar]
- Tafreshi, N.K.; Lloyd, M.C.; Bui, M.M.; Gillies, R.J.; Morse, D.L. Carbonic Anhydrase IX as an Imaging and therapeutic target for tumors and metastases. In Carbonic Anhydrase: Mechanism, Regulation, Links to Disease, and Industrial Applications; Frost, S.C., McKenna, R., Eds.; Springer: Dordrecht, The Netherlands, 2014; Volume 75, pp. 221–254. [Google Scholar]
- Opavský, R.; Pastoreková, S.; Zelník, V.; Gibadulinová, A.; Stanbridge, E.J.; Závada, J.; Kettmann, R.; Pastorek, J. HumanMN/CA9Gene, a Novel Member of the Carbonic Anhydrase Family: Structure and Exon to Protein Domain Relationships. Genomics 1996, 33, 480–487. [Google Scholar] [CrossRef]
- Swietach, P.; Wigfield, S.; Cobden, P.; Supuran, C.T.; Harris, A.L.; Vaughan-Jones, R.D. Tumor-associated Carbonic Anhydrase 9 Spatially Coordinates Intracellular pH in Three-dimensional Multicellular Growths. J. Biol. Chem. 2008, 283, 20473–20483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wykoff, C.C.; Beasley, N.J.; Watson, P.H.; Turner, K.J.; Pastorek, J.; Sibtain, A.; Wilson, G.D.; Turley, H.; Talks, K.L.; Maxwell, P.H.; et al. Hypoxia-inducible expression of tumor-associated carbonic anhydrases. Cancer Res. 2000, 60, 7075–7083. [Google Scholar]
- Maxwell, P.H.; Wiesener, M.; Chang, G.W.; Clifford, S.C.; Vaux, E.C.; Cockman, M.E.; Wykoff, C.C.; Pugh, C.W.; Maher, E.R.; Ratcliffe, P.J. The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis. Nature 1999, 399, 271–275. [Google Scholar] [CrossRef]
- Pastoreková, S.; Parkkila, S.; Parkkila, A.K.; Opavský, R.; Zelník, V.; Saarnio, J.; Pastorek, J. Carbonic anhydrase IX, MN/CA IX: Analysis of stomach complementary DNA sequence and expression in human and rat alimentary tracts. Gastroenterology 1997, 112, 398–408. [Google Scholar] [CrossRef]
- Svastová, E.; Zilka, N.; Zat’ovicová, M.; Gibadulinová, A.; Ciampor, F.; Pastorek, J.; Pastoreková, S. Carbonic anhydrase IX reduces E-cadherin-mediated adhesion of MDCK cells via interaction with beta-catenin. Exp. Cell Res. 2003, 290, 332–345. [Google Scholar] [CrossRef]
- Renal Cell Carcinoma Overview. Available online: http://www.pathologyoutlines.com/topic/kidneytumormalignantrcc.html (accessed on 22 July 2020).
- Kim, M.; Joo, J.W.; Lee, S.J.; Cho, Y.A.; Park, C.K.; Cho, N.H. Comprehensive Immunoprofiles of Renal Cell Carcinoma Subtypes. Cancers 2020, 12, 602. [Google Scholar] [CrossRef] [Green Version]
- Reuter, V.E.; Argani, P.; Zhou, M.; Delahunt, B.; Members of the ISUP Immunohistochemistry in Diagnostic Urologic Pathology Group. Best practices recommendations in the application of immunohistochemistry in the kidney tumors: Report from the International Society of Urologic Pathology consensus conference. Am. J. Surg. Pathol. 2014, 38, e35–e49. [Google Scholar] [CrossRef]
- Alshenawy, H.A. Immunohistochemical Panel for Differentiating Renal Cell Carcinoma with Clear and Papillary Features. Pathol. Oncol. Res. POR 2015, 21, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Bing, Z.; Lal, P.; Lu, S.; Ziober, A.; Tomaszewski, J.E. Role of carbonic anhydrase IX, α-methylacyl coenzyme a racemase, cytokeratin 7, and galectin-3 in the evaluation of renal neoplasms: A tissue microarray immunohistochemical study. Ann. Diagn. Pathol. 2013, 17, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Truong, L.D.; Shen, S.S. Immunohistochemical diagnosis of renal neoplasms. Arch. Pathol. Lab. Med. 2011, 135, 92–109. [Google Scholar] [CrossRef]
- Ingels, A.; Hew, M.; Algaba, F.; de Boer, O.J.; van Moorselaar, R.J.A.; Horenblas, S.; Zondervan, P.; de la Rosette, J.J.M.C.H.; Pilar Laguna Pes, M. Vimentin over-expression and carbonic anhydrase IX under-expression are independent predictors of recurrence, specific and overall survival in non-metastatic clear-cell renal carcinoma: A validation study. World J. Urol. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bui, M.H.T.; Seligson, D.; Han, K.; Pantuck, A.J.; Dorey, F.J.; Huang, Y.; Horvath, S.; Leibovich, B.C.; Chopra, S.; Liao, S.-Y.; et al. Carbonic anhydrase IX is an independent predictor of survival in advanced renal clear cell carcinoma: Implications for prognosis and therapy. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 802–811. [Google Scholar]
- Zhang, B.Y.; Thompson, R.H.; Lohse, C.M.; Dronca, R.S.; Cheville, J.C.; Kwon, E.D.; Leibovich, B.C. Carbonic anhydrase IX (CAIX) is not an independent predictor of outcome in patients with clear cell renal cell carcinoma (ccRCC) after long-term follow-up: CAIX is not an independent predictor of outcome in patients with ccRCC. BJU Int. 2013, 111, 1046–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zerati, M.; Leite, K.R.M.; Pontes-Junior, J.; Segre, C.C.; Reis, S.T.; Srougi, M.; Dall’Oglio, M.F. Carbonic Anhydrase IX is not a predictor of outcomes in non-metastatic clear cell renal cell carcinoma—A digital analysis of tissue microarray. Int. Braz J. Urol Off. J. Braz. Soc. Urol. 2013, 39, 484–492. [Google Scholar] [CrossRef] [Green Version]
- Büscheck, F.; Fraune, C.; Simon, R.; Kluth, M.; Hube-Magg, C.; Möller-Koop, C.; Shadanpour, N.; Bannenberg, C.; Eichelberg, C.; Höflmayer, D.; et al. Aberrant expression of membranous carbonic anhydrase IX (CAIX) is associated with unfavorable disease course in papillary and clear cell renal cell carcinoma. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 531.e19–531.e25. [Google Scholar] [CrossRef]
- Samberkar, S.; Rajandram, R.; Mun, K.S.; Samberkar, P.; Danaee, M.; Zulkafli, I.S. Carbonic anhydrase IX immunohistochemistry has potential to predict renal cell carcinoma outcomes: A systematic review and meta-analyses. Malays. J. Pathol. 2019, 41, 233–242. [Google Scholar]
- Patard, J.-J.; Fergelo, T.P.; Karakiewicz, P.I.; Klatte, T.; Trinh, Q.-D.; Rioux-Leclercq, N.; Said, J.W.; Belldegrun, A.S.; Pantuck, A.J. Low CAIX expression and absence of VHL gene mutation are associated with tumor aggressiveness and poor survival of clear cell renal cell carcinoma: CAIX and VHL Status in Kidney Cancer. Int. J. Cancer 2008, 123, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Chamie, K.; Klöpfer, P.; Bevan, P.; Störkel, S.; Said, J.; Fall, B.; Belldegrun, A.S.; Pantuck, A.J. Carbonic anhydrase-IX score is a novel biomarker that predicts recurrence and survival for high-risk, nonmetastatic renal cell carcinoma: Data from the phase III ARISER clinical trial. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 204.e25–204.e33. [Google Scholar] [CrossRef]
- Tostain, J.; Li, G.; Gentil-Perret, A.; Gigante, M. Carbonic anhydrase 9 in clear cell renal cell carcinoma: A marker for diagnosis, prognosis and treatment. Eur. J. Cancer Oxf. Engl. 1990, 46, 3141–3148. [Google Scholar] [CrossRef] [PubMed]
- Atkins, M.; Regan, M.; McDermott, D.; Mier, J.; Stanbridge, E.; Youmans, A.; Febbo, P.; Upton, M.; Lechpammer, M.; Signoretti, S. Carbonic anhydrase IX expression predicts outcome of interleukin 2 therapy for renal cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2005, 11, 3714–3721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; Grünwald, V.; Gillessen, S.; Horwich, A. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choueiri, T.K.; Regan, M.M.; Rosenberg, J.E.; Oh, W.K.; Clement, J.; Amato, A.M.; McDermott, D.; Cho, D.C.; Atkins, M.B.; Signoretti, S. Carbonic anhydrase IX and pathological features as predictors of outcome in patients with metastatic clear-cell renal cell carcinoma receiving vascular endothelial growth factor-targeted therapy. BJU Int. 2010, 106, 772–778. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Cheng, S.; Qu, A.Q.; Pastorek, J.; Atkins, M.B.; Signoretti, S. Carbonic anhydrase IX as a potential biomarker of efficacy in metastatic clear-cell renal cell carcinoma patients receiving sorafenib or placebo: Analysis from the treatment approaches in renal cancer global evaluation trial (TARGET). Urol. Oncol. 2013, 31, 1788–1793. [Google Scholar] [CrossRef] [Green Version]
- Lucarini, L.; Magnelli, L.; Schiavone, N.; Crisci, A.; Innocenti, A.; Puccetti, L.; Cianchi, F.; Peri, S.; Supuran, C.T.; Papucci, L.; et al. Plasmatic carbonic anhydrase IX as a diagnostic marker for clear cell renal cell carcinoma. J. Enzyme Inhib. Med. Chem. 2018, 33, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Pirinççi, N.; Kaya, T.Y.; Kaba, M.; Ozan, T.; Geçit, İ.; Özveren, H.; Eren, H.; Ceylan, K. Serum adenosine deaminase, catalase, and carbonic anhydrase activities in patients with renal cell carcinoma. Redox Rep. Commun. Free Radic. Res. 2017, 22, 252–256. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Feng, G.; Gentil-Perret, A.; Genin, C.; Tostain, J. Serum carbonic anhydrase 9 level is associated with postoperative recurrence of conventional renal cell cancer. J. Urol. 2008, 180, 510–513, discussion 513–514. [Google Scholar] [CrossRef]
- Liu, S.; Tian, Z.; Zhang, L.; Hou, S.; Hu, S.; Wu, J.; Jing, Y.; Sun, H.; Yu, F.; Zhao, L.; et al. Combined cell surface carbonic anhydrase 9 and CD147 antigens enable high-efficiency capture of circulating tumor cells in clear cell renal cell carcinoma patients. Oncotarget 2016, 7, 59877–59891. [Google Scholar] [CrossRef] [PubMed]
- Ingels, A.; Barret, E.; Sanchez-Salas, R.; Galiano, M.; Rozet, F.; Lenoir, S.; Weber, N.; Audenet, F.; Cathelineau, X. Percutaneous Renal Biopsies for Small Renal Masses: Complex Tumors on Nephrometry Should Be the First Targets. Clin. Genitourin. Cancer 2016, 14, e457–e462. [Google Scholar] [CrossRef] [PubMed]
- Gerlinger, M.; Rowan, A.J.; Horswell, S.; Larkin, J.; Endesfelder, D.; Gronroos, E.; Martinez, P.; Matthews, N.; Stewart, A.; Tarpey, P.; et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 2012, 366, 883–892. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.-Y.; Ding, H.-J.; Chen, J.-H.; Chao, C.-H.; Lu, Y.-Y.; Lin, W.-Y.; Kao, C.-H. Meta-analysis of the diagnostic performance of [18F]FDG-PET and PET/CT in renal cell carcinoma. Cancer Imaging 2012, 12, 464–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Muselaers, S.; Mulders, P.; Oosterwijk, E.; Oyen, W.; Boerman, O. Molecular imaging and carbonic anhydrase IX-targeted radioimmunotherapy in clear cell renal cell carcinoma. Immunotherapy 2013, 5, 489–495. [Google Scholar] [CrossRef]
- Zhu, L.; Wang, L.; Liu, Y.; Xu, D.; Fang, K.; Guo, Y. CAIX aptamer-functionalized targeted nanobubbles for ultrasound molecular imaging of various tumors. Int. J. Nanomedicine 2018, 13, 6481–6495. [Google Scholar] [CrossRef] [Green Version]
- Young, J.R.; Coy, H.; Kim, H.J.; Douek, M.; Sisk, A.; Pantuck, A.J.; Raman, S.S. Association of the Gross Appearance of Intratumoral Vascularity at MDCT with the Carbonic Anhydrase IX Score in Clear Cell Renal Cell Carcinoma. Am. J. Roentgenol. 2018, 211, 1254–1258. [Google Scholar] [CrossRef]
- Lindenberg, L.; Mena, E.; Choyke, P.L.; Bouchelouche, K. PET imaging in renal cancer. Curr. Opin. Oncol. 2019, 31, 216–221. [Google Scholar] [CrossRef]
- Hekman, M.C.H.; Rijpkema, M.; Aarntzen, E.H.; Mulder, S.F.; Langenhuijsen, J.F.; Oosterwijk, E.; Boerman, O.C.; Oyen, W.J.G.; Mulders, P.F.A. Positron Emission Tomography/Computed Tomography with 89Zr-girentuximab Can Aid in Diagnostic Dilemmas of Clear Cell Renal Cell Carcinoma Suspicion. Eur. Urol. 2018, 74, 257–260. [Google Scholar] [CrossRef]
- Minn, I.; Koo, S.M.; Lee, H.S.; Brummet, M.; Rowe, S.P.; Gorin, M.A.; Sysa-Shah, P.; Lewis, W.D.; Ahn, H.-H.; Wang, Y.; et al. [64Cu]XYIMSR-06: A dual-motif CAIX ligand for PET imaging of clear cell renal cell carcinoma. Oncotarget 2016, 7, 56471–56479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkbey, B.; Lindenberg, M.L.; Adler, S.; Kurdziel, K.A.; McKinney, Y.L.; Weaver, J.; Vocke, C.D.; Anver, M.; Bratslavsky, G.; Eclarinal, P.; et al. PET/CT imaging of renal cell carcinoma with (18)F-VM4-037: A phase II pilot study. Abdom. Radiol. N. Y. 2016, 41, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Muselaers, C.H.J.; Rijpkema, M.; Bos, D.L.; Langenhuijsen, J.F.; Oyen, W.J.G.; Mulders, P.F.A.; Oosterwijk, E.; Boerman, O.C. Radionuclide and Fluorescence Imaging of Clear Cell Renal Cell Carcinoma Using Dual Labeled Anti-Carbonic Anhydrase IX Antibody G250. J. Urol. 2015, 194, 532–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hekman, M.C.; Rijpkema, M.; Muselaers, C.H.; Oosterwijk, E.; Hulsbergen-Van de Kaa, C.A.; Boerman, O.C.; Oyen, W.J.; Langenhuijsen, J.F.; Mulders, P.F. Tumor-targeted Dual-modality Imaging to Improve Intraoperative Visualization of Clear Cell Renal Cell Carcinoma: A First in Man Study. Theranostics 2018, 8, 2161–2170. [Google Scholar] [CrossRef] [PubMed]
- Shuch, B.; Li, Z.; Belldegrun, A.S. Carbonic anhydrase IX and renal cell carcinoma: Prognosis, response to systemic therapy, and future vaccine strategies. BJU Int. 2008, 101, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.R.; Yang, E.K.; Kim, S.H.; Moon, D.C.; Kim, H.J.; Lee, J.C.; Kim, D.Y. Immunostimulatory activity of dendritic cells pulsed with carbonic anhydrase IX and Acinetobacter baumannii outer membrane protein A for renal cell carcinoma. J. Microbiol. Seoul Korea 2011, 49, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.-R.; Yang, E.-K.; Kim, D.-Y.; Kim, S.-H.; Moon, D.-C.; Lee, J.-H.; Kim, H.-J.; Lee, J.-C. Generation of anti-tumour immune response using dendritic cells pulsed with carbonic anhydrase IX-Acinetobacter baumannii outer membrane protein A fusion proteins against renal cell carcinoma. Clin. Exp. Immunol. 2012, 167, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Birkhäuser, F.D.; Koya, R.C.; Neufeld, C.; Rampersaud, E.N.; Lu, X.; Micewicz, E.D.; Chodon, T.; Atefi, M.; Kroeger, N.; Chandramouli, G.V.R.; et al. Dendritic cell-based immunotherapy in prevention and treatment of renal cell carcinoma: Efficacy, safety, and activity of Ad-GM·CAIX in immunocompetent mouse models. J. Immunother. Hagerstown Md 1997, 36, 102–111. [Google Scholar] [CrossRef]
- Faiena, I.; Zomorodian, N.; Comin-Anduix, B.; Sachadeva, A.; Bot, A.; Kabinnivar, F.; Said, J.W.; Cheung-Lau, G.; Pang, J.; Macabali, M.; et al. A phase I, open-label, dose-escalation and cohort expansion study evaluating the safety and immune response to autologous dendritic cells transduced with AdGMCA9 in patients with metastatic renal cell carcinoma. J. Clin. Oncol. 2018, 36, 653. [Google Scholar] [CrossRef]
- Chang, D.-K.; Moniz, R.J.; Xu, Z.; Sun, J.; Signoretti, S.; Zhu, Q.; Marasco, W.A. Human anti-CAIX antibodies mediate immune cell inhibition of renal cell carcinoma in vitro and in a humanized mouse model in vivo. Mol. Cancer 2015, 14, 119. [Google Scholar] [CrossRef] [Green Version]
- Oosterwijk-Wakka, J.C.; Kats-Ugurlu, G.; Leenders, W.P.J.; Kiemeney, L.A.L.M.; Old, L.J.; Mulders, P.F.A.; Oosterwijk, E. Effect of tyrosine kinase inhibitor treatment of renal cell carcinoma on the accumulation of carbonic anhydrase IX-specific chimeric monoclonal antibody cG250. BJU Int. 2011, 107, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Oosterwijk-Wakka, J.C.; Boerman, O.C.; Mulders, P.F.A.; Oosterwijk, E. Application of monoclonal antibody G250 recognizing carbonic anhydrase IX in renal cell carcinoma. Int. J. Mol. Sci. 2013, 14, 11402–11423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stillebroer, A.B.; Boerman, O.C.; Desar, I.M.E.; Boers-Sonderen, M.J.; van Herpen, C.M.L.; Langenhuijsen, J.F.; Smith-Jones, P.M.; Oosterwijk, E.; Oyen, W.J.G.; Mulders, P.F.A. Phase 1 Radioimmunotherapy Study with Lutetium 177–labeled Anti-Carbonic Anhydrase IX Monoclonal Antibody Girentuximab in Patients with Advanced Renal Cell Carcinoma. Eur. Urol. 2013, 64, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Muselaers, C.H.J.; Boers-Sonderen, M.J.; van Oostenbrugge, T.J.; Boerman, O.C.; Desar, I.M.E.; Stillebroer, A.B.; Mulder, S.F.; van Herpen, C.M.L.; Langenhuijsen, J.F.; Oosterwijk, E.; et al. Phase 2 Study of Lutetium 177-Labeled Anti-Carbonic Anhydrase IX Monoclonal Antibody Girentuximab in Patients with Advanced Renal Cell Carcinoma. Eur. Urol. 2016, 69, 767–770. [Google Scholar] [CrossRef]
- Pal, S.K.; Agarwal, N. Kidney cancer: Finding a niche for girentuximab in metastatic renal cell carcinoma. Nat. Rev. Urol. 2016, 13, 442–443. [Google Scholar] [CrossRef]
- Duivenvoorden, W.C.M.; Hopmans, S.N.; Gallino, D.; Farrell, T.; Gerdes, C.; Glennie, D.; Lukka, H.; Pinthus, J.H. Inhibition of carbonic anhydrase IX (CA9) sensitizes renal cell carcinoma to ionizing radiation. Oncol. Rep. 2015, 34, 1968–1976. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Common CAIX Expression in Immunohistochemistry | ||
|---|---|---|
| RCC subtype | CAIX | CK7 |
| ccRCC | +++ | − |
| pRCCI | − | + |
| pRCCII | +/− | +/− |
| chRCC | − | + |
| ccpRCC | + | + |
| multilocular cystic renal neoplasms | +/− | + |
| Predictive value of CAIX expression | ||
| Study | RCC subtype | Results |
| Ingels et al. [19] | ccRCC | CAIX expression < 30% in IHC associated with diminished OS, PFS and DFS |
| Bui et al. [20] | ccRCC | Low CAIX expression associated with unfavorable disease course |
| Buschek et al. [23] | ccRCC | High CAIX expression was associated with better outcomes |
| Buschek et al. [23] | pRCC | Abnormal expression of CAIX was associated with diminished PFS |
| Samberkar et al. [24] | ccRCC | High CAIX expression associated with lower tumor grade and stage, N0, favorable ECOG score |
| Chamie et al. [26] | ccRCC | High CAIX score > 200 associated with prolonged DFS and OS |
| USMI | |||
|---|---|---|---|
| Study | product | abilities | limitations |
| Zhu et al. [41] | CAIX aptamer functionalized nanobubbles | Enhance vascularization and parenchyma in CAIX-expressive tumors | Preclinical data only |
| PET imaging | |||
| Study | product | abilities | limitations |
| Lindenberg et al. [43] Hekman et al. [44] | Girentuximab/cG250 | Good sensitivity and specificity for ccRCC many labeling possibilities with several isotopes (124I, 131I, 111In, 89Zr etc.) | Slow pharmacokinetics, acquisition within 2 to 6 days |
| Lindenberg et al. [43] | 18FDG | Detection of metastasis | Low sensitivity for primary tumor |
| Minn et al. [45] | 64Cu-XYIMSR-06 | Fast pharmacokinetics, acquisition within 1 h to 1 day | Preclinical data only |
| Turkbey et al. [46] | 18F-VM4-037 | Sensitivity for metastasis detection could be better than 18FDG | Low sensitivity for primary tumor |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courcier, J.; de la Taille, A.; Nourieh, M.; Leguerney, I.; Lassau, N.; Ingels, A. Carbonic Anhydrase IX in Renal Cell Carcinoma, Implications for Disease Management. Int. J. Mol. Sci. 2020, 21, 7146. https://doi.org/10.3390/ijms21197146
Courcier J, de la Taille A, Nourieh M, Leguerney I, Lassau N, Ingels A. Carbonic Anhydrase IX in Renal Cell Carcinoma, Implications for Disease Management. International Journal of Molecular Sciences. 2020; 21(19):7146. https://doi.org/10.3390/ijms21197146
Chicago/Turabian StyleCourcier, Jean, Alexandre de la Taille, Maya Nourieh, Ingrid Leguerney, Nathalie Lassau, and Alexandre Ingels. 2020. "Carbonic Anhydrase IX in Renal Cell Carcinoma, Implications for Disease Management" International Journal of Molecular Sciences 21, no. 19: 7146. https://doi.org/10.3390/ijms21197146