Unhealthy Levels of Phthalates and Bisphenol A in Mexican Pregnant Women with Gestational Diabetes and Its Association to Altered Expression of miRNAs Involved with Metabolic Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Samples
2.2. RNA Extraction
2.3. miRNA Expression
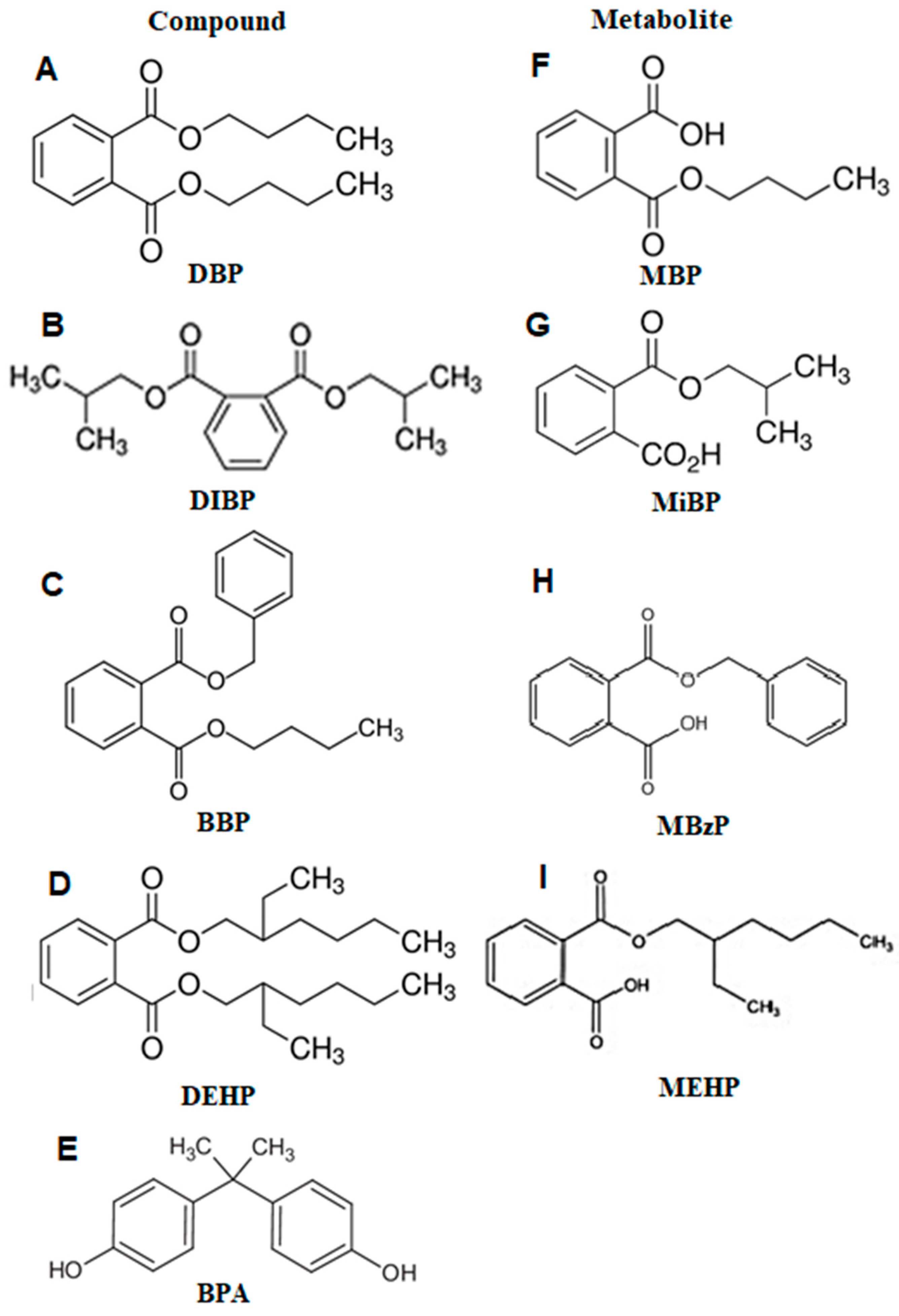
2.4. Phthalates Metabolites and Total BPA Assessment
2.5. Data Analysis
3. Results
3.1. Population Characteristics
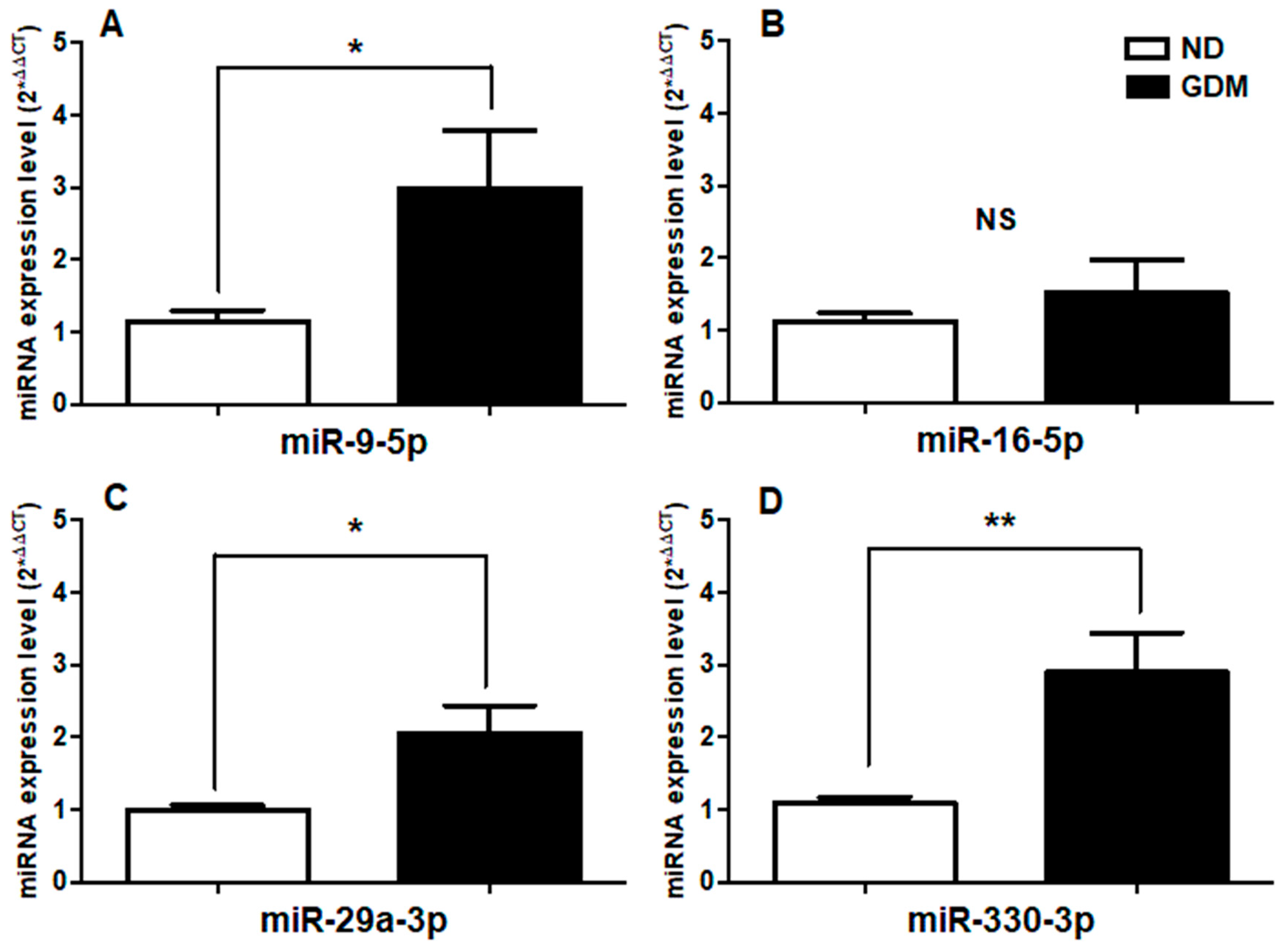
3.2. Up-Regulation of miR-9-5p, miR-29a-3p, and miR-330-3p in GDM Serum Samples of GDM Women
3.3. Phthalates Metabolites and Total BPA Urine Levels in Second Trimester Pregnant Women
3.4. Correlation between Phthalate Metabolites, Total BPA Urine Levels and Serum miRNA Expression Levels, and Clinical Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Definition, diagnosis and classification of Diabetes mellitus and its complications. Part I: Diagnosis and classification of Diabetes mellitus. 1999, pp. 1–59. Available online: https://apps.who.int/iris/handle/10665/66040 (accessed on 13 January 2019).
- ADA. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes. Diabetes Care 2019, 42, S13–S27. [Google Scholar] [CrossRef] [PubMed]
- Johns, E.; Denison, F.; Norman, J.; Reynolds, R. Gestational Diabetes Mellitus: Mechanisms, Treatment, and Complications. Trends Endocrinol Metab. 2018, 29, 743–754. [Google Scholar] [CrossRef]
- WHO. Global Reports in Diabetes; WHO Press, World Health Organization: Geneva, Switzerland, 2016; Available online: http://www.who.int (accessed on 25 January 2019).
- Ferrara, A. Increasing prevalence of gestational diabetes mellitus: A public health perspective. Diabetes Care 2007, 30, S141–S146. [Google Scholar] [CrossRef]
- Reyes-Muñoz, E.; Parra, A.; Castillo-Mora, A.; Ortega-Gonzalez, C. Impact of the International Association of Diabetes and Pregnancy Study Groups diagnostic criteria on the prevalence of gestational diabetes mellitus in urban Mexican women: A cross-sectional study. Endocrinol. Pract. 2011. [Google Scholar] [CrossRef]
- Dainelli, L.; Prieto-Patrón, A.; Silva-Zolezzi, I.; Sosa-Rubí, S.; Espino y Sosa, S.; Reyes-Muñoz, E.; López-Ridaura, R.; Detzel, P. Screening and management of gestational diabetes in Mexico: Results from a survey of multilocation, multi-health care institution practitioners. Diabetes Metab. Syndr. Obes. 2018, 11, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.; Darbinian, J.; Ferrara, A. Disparities in the risk of gestational diabetes by race-ethnicity and country of birth. Paediatr. Perinat. Epidemiol. 2010, 24, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, W.; Samoa, R.; Wotring, A. Gestational Diabetes in High-Risk Populations. Clin. Diabetes 2013, 31, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Reyes, E.; Martínez, N.; Parra, A.; Castillo-Mora, A.; Ortega-González, C. Early intensive obstetric and medical nutrition care is associated with decreased prepregnancy obesity impact on perinatal outcomes. Gynecol. Obstet. Investig. 2012, 73, 75–81. [Google Scholar] [CrossRef]
- Cypryk, K.; Pertyńska-Marczewska, M.; Szymczak, W.; Zawodniak-Szałapska, M.; Wilczyński, J.; Lewiński, A. Overweight and obesity as common risk factors for gestational diabetes mellitus (GDM), perinatal macrosomy in offspring and type-2 diabetes in mothers. Przegl. Lek. 2005, 62, 38–41. [Google Scholar]
- Kim, M.; Newton, K.; Knopp, R. Gestational Diabetes and the Incidence of Type 2 Diabetes A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef]
- Daly, B.; Toulis, K.; Thomas, N.; Gokhale, K.; Martin, J.; Webber, J.; Keerthy, D.; Jolly, K.; Saravanan, P.; Nirantharakumar, K. Increased risk of ischemic heart disease, hypertension, and type 2 diabetes in women with previous gestational diabetes mellitus, a target group in general practice for preventive interventions: A population-based cohort study. PLOS Med. 2018, 15, e1002488. [Google Scholar] [CrossRef] [PubMed]
- Gore, A.; Chappell, V.; Fenton, S.; Flaws, J.; Nadal, A.; Prins, G.; Toppari, J.; Zoeller, R. EDC-2: The Endocrine Society’s Second Scientific Statement on Endocrine-Disrupting Chemicals. Endocr. Rev. 2015, 36, E1–E150. [Google Scholar] [CrossRef] [PubMed]
- Bang, D.; Kyung, M.; Kim, M.; Jung, B.; Cho, M.; Choi, S.; Kim, Y.; Lim, S.; Lim, D.; Won, A.; et al. Human Risk Assessment of Endocrine-Disrupting Chemicals Derived from Plastic Food Containers. Compr. Rev. Food Sci. Food Saf. 2012, 11, 453–470. [Google Scholar] [CrossRef]
- Stojanoska, M.; Milosevic, N.; Milic, N.; Abenavoli, L. The influence of phthalates and bisphenol A on the obesity development and glucose metabolism disorders. Endocrine 2017, 55, 666–668. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.; Kauri, L.; Cakmak, S. The associations between phthalate exposure and insulin resistance, β-cell function and blood glucose control in a population-based sample. Sci. Total Environ. 2018, 612, 1287–1292. [Google Scholar] [CrossRef] [PubMed]
- Le Magueresse-Battistoni, B.; Multigner, L.; Beausoleil, C.; Rousselle, R. Effects of bisphenol A on metabolism and evidence of a mode of action mediated through endocrine disruption. Mol. Cell. Endocrinol. 2018, 475, 74–91. [Google Scholar] [CrossRef] [PubMed]
- Cantonwine, D.; Meeker, J.; Hu, H.; Sánchez, B.; Lamadrid-Figueroa, H.; Mercado-García, A.; Fortenberry, G.; Calafat, A.; Téllez-Rojo, M. Bisphenol a exposure in Mexico City and risk of prematurity: A pilot nested case control study. Environ. Health 2010, 9, 62. [Google Scholar] [CrossRef]
- Ashley-Martin, J.; Dodds, L.; Arbuckle, T.; Ettinger, A.; Shapiro, G.; Fisher, M.; Morisset, A.; Taback, S.; Bouchard, M.; Monnier, P.; et al. A birth cohort study to investigate the association between prenatal phthalate and bisphenol A exposures and fetal markers of metabolic dysfunction. Environ. Health 2014, 13, 84. [Google Scholar] [CrossRef]
- Elizalde, V.; García-Fabila, M.; Campuzano, M.; Bustamante-Montes, P. Prenatal exposure to phthalates. Maternal anemia, pregnancy duration and neonatal somatometry. Clin. Investig. Ginecol. Obstet. 2012, 39, 133–180. [Google Scholar]
- Lee, B.; Park, H.; Hong, Y.; Ha, M.; Kim, Y.; Chang, N.; Kim, B.; Kim, Y.; Yu, S.; Ha, E. Prenatal bisphenol A and birth outcomes: MOCEH (Mothers and Children’s Environmental Health) study. Int. J. Hyg. Environ. Health 2014, 217, 328–334. [Google Scholar] [CrossRef]
- Ding, G.; Wang, C.; Vinturache, A.; Zhao, S.; Pan, R.; Han, W.; Chen, L.; Wang, W.; Yuan, T.; Gao, Y.; et al. Prenatal low-level phenol exposures and birth outcomes in China. Sci. Total Environ. 2017, 31, 607–608, 1400–1407. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Li, S. Epigenetic effects of environmental chemicals bisphenol A and phthalates. Int. J. Mol. Sci. 2012, 13, 10143–10153. [Google Scholar] [CrossRef] [PubMed]
- Vrijens, K.; Bollati, V.; Nawrot, T. MicroRNAs as Potential Signatures of Environmental Exposure or Effect: A Systematic Review. Environ. Health Perspect. 2015, 123, 399–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohel, M. Extracellular/Circulating MicroRNAs: Release Mechanisms, Functions and Challenges. Achiev. Life Sci. 2016, 10, 175–186. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Dong, J.; Jiang, T.; Shi, Z.; Yu, B.; Zhu, Y.; Chen, D.; Xu, J.; Huo, R.; Dai, J.; et al. Early Second-Trimester Serum MiRNA Profiling Predicts Gestational Diabetes Mellitus. PLoS ONE 2011, 6, e23925. [Google Scholar] [CrossRef]
- Zhu, Y.; Tian, F.; Li, H.; Zhou, Y.; Lu, J.; Ge, Q. Profiling maternal plasma microRNA expression in early pregnancy to predict gestational diabetes mellitus. Int. J. Gynaecol. Obstet. 2015, 130, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Song, L.; Zhou, L.; Wu, J.; Sheng, C.; Chen, H.; Liu, Y.; Gao, S.; Huang, W. A MicroRNA Signature in Gestational Diabetes Mellitus Associated with Risk of Macrosomia. Cell. Physiol. Biochem. 2015, 37, 243–252. [Google Scholar] [CrossRef]
- Sebastiani, G.; Guarino, E.; Grieco, G.; Formichi, C.; Delli Poggi, C.; Ceccarelli, E.; Dotta, F. Circulating microRNA (miRNA) Expression Profiling in Plasma of Patients with Gestational Diabetes Mellitus Reveals Up-regulation of miRNA miR-330-3p. Front. Endocrinol. 2017, 8, 345. [Google Scholar] [CrossRef]
- Zampetaki, A.; Kiechl, S.; Drozdov, I.; Willeit, P.; Mayr, U.; Prokopi, M.; Mayr, A.; Weger, S.; Oberhollenzer, F.; Bonora, E.; et al. Plasma microRNA profiling reveals loss of endothelial miR-126 and other microRNAs in type 2 diabetes. Circ. Res. 2010, 107, 810–817. [Google Scholar] [CrossRef]
- Calafat, A.; Ye, X.; Wong, L.; Reidy, J.; Needham, L. Exposure of the U.S. population to bisphenol A and 4-tertiary-octylphenol: 2003–2004. Environ. Health Perspect. 2008, 116, 39–44. [Google Scholar] [CrossRef]
- Silva, M.; Slakman, A.; Reidy, J.; Preau, J.; Herbert, A.; Samandar, E.; Needham, L.; Calafat, A. Analysis of human urine for fifteen phthalate metabolites using automated solid-phase extraction. J. Chromatogr. B 2004, 805, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Sliwinska, A.; Kasinska, M.; Drzewoski, J. MicroRNAs and metabolic disorders—Where are we heading? Arch. Med. Sci. 2017, 13, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Guarino, E.; Delli Poggi, C.; Grieco, G.; Cenci, V.; Ceccarelli, E.; Crisci, I.; Sebastiani, G.; Dotta, F. Circulating MicroRNAs as Biomarkers of Gestational Diabetes Mellitus: Updates and Perspectives. Int. J. Endocrinol. 2018, 2018, 6380463. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhu, X. miR-9-5p plays an important role in gestational diabetes mellitus (GDM) progression by targeting HK-2. Int. J. Clin. Exp. Med. 2018, 11, 6694–6701. [Google Scholar]
- Kong, L.; Zhu, J.; Han, W.; Jiang, X.; Xu, M.; Zhao, Y.; Dong, Q.; Pang, Z.; Guan, Q.; Gao, L.; et al. Significance of serum microRNAs in pre-diabetes and newly diagnosed type 2 diabetes: A clinical study. Acta Diabetol. 2011, 48, 61–69. [Google Scholar] [CrossRef]
- Wander, P.; Boyko, E.; Hevner, K.; Parikh, V.; Tadesse, M.; Sorensen, K.; Williams, M.; Enquobahrie, D. Circulating early and mid-pregnancy microRNAs and risk of gestational diabetes. Diabetes Res. Clin. Pract. 2017, 132, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Massart, J.; Sjögren, R.; Lundell, L.; Mudry, J.; Franck, N.; O’Gorman, D.; Egan, B.; Zierath, J.; Krook, A. Altered miR-29 Expression in Type 2 Diabetes Influences Glucose and Lipid Metabolism in Skeletal Muscle. Diabetes 2017, 66, 1807–1818. [Google Scholar] [CrossRef] [Green Version]
- Esteves, J.; Enguita, F.; Machado, U. MicroRNAs mediated regulation of skeletal muscle GLUT4 expression and translocation in insulin resistance. J. Diabetes Res. 2017, 2017, 6380463. [Google Scholar] [CrossRef]
- Ludwig, N.; Leidinger, P.; Becker, K.; Backes, C.; Fehlmann, T.; Pallasch, C.; Rheinheimer, S.; Meder, B.; Stähler, C.; Meese, E.; et al. Distribution of miRNA expression across human tissues. Nucleic Acids Res. 2016, 44, 3865–3877. [Google Scholar] [CrossRef]
- Lamadrid-Romero, M.; Solís, K.; Cruz-Reséndiz, M.; Pérez, J.; Díaz, N.; Flores-Herrera, H.; García-López, G.; Perichart, O.; Reyes-Muñoz, E.; Arenas-Huertero, F.; et al. Central nervous system development related microRNAs levels increase in the serum of gestational diabetic women during the first trimester of pregnancy. Neurosci. Res. 2018, 130, 8–22. [Google Scholar] [CrossRef]
- Dluzen, D.; Noren Hooten, N.; Zhang, Y.; Kim, Y.; Glover, F.; Tajuddin, S.; Jacob, K.; Zonderman, A.; Evans, M. Racial differences in microRNA and gene expression in hypertensive women. Sci. Rep. 2016, 6, 35815. [Google Scholar] [CrossRef]
- Yang, T.; Peterson, K.; Meeker, J.; Sánchez, B.; Zhang, Z.; Cantoral, A.; Solano, M.; Tellez-Rojo, M. Bisphenol A and phthalates in utero and in childhood: Association with child BMI z-score and adiposity. Environ. Res. 2017, 156, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Peterson, K.; Meeker, J.; Sánchez, B.; Zhang, Z.; Cantoral, A.; Solano, M.; Tellez-Rojo, M. Exposure to Bisphenol A and phthalates metabolites in the third trimester of pregnancy and BMI trajectories. Pediatr. Obes. 2018, 13, 550–557. [Google Scholar] [CrossRef] [PubMed]
- LaRocca, J.; Binder, AM.; McElrath, T.; Michels, K. First-Trimester Urine Concentrations of Phthalate Metabolites and Phenols and Placenta miRNA Expression in a Cohort of U.S. Women. Environ. Health Perspect. 2015, 124, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.; Arbuckle, T.; Mallick, R.; LeBlanc, A.; Hauser, R.; Feeley, M.; Koniecki, D.; Ramsay, T.; Provencher, G.; Bérubé, R.; et al. Bisphenol A and phthalate metabolite urinary concentrations: Daily and across pregnancy variability. J. Expo. Sci. Environ. Epidemiol. 2014, 25, 231–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adibi, J.; Whyatt, R.; Williams, P.; Calafat, A.; Camann, D.; Herrick, R.; Nelson, H.; Bhat, H.; Perera, F.; Silva, M.; et al. Characterization of phthalate exposure among pregnant women assessed by repeat air and urine samples. Environ. Health Perspect. 2008, 116, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, R.; Ferguson, K.; Sheppard, L.; James-Todd, T.; Butts, S.; Chandrasekaran, S.; Swan, S.; Barrett, E.; Nguyen, R.; Bush, N.; et al. Maternal urinary phthalate metabolites in relation to gestational diabetes and glucose intolerance during pregnancy. Environ. Int. 2019, 123, 588–596. [Google Scholar] [CrossRef]
- Peng, F.; Ji, W.; Zhu, F.; Peng, D.; Yang, M.; Liu, R.; Pu, Y.; Yin, L. A study on phthalate metabolites, bisphenol A and nonylphenol in the urine of Chinese women with unexplained recurrent spontaneous abortion. Environ. Res. 2016, 150, 622–628. [Google Scholar] [CrossRef]
- Noor, N.; Ferguson, K.; Meeker, J.; Seely, E.; Hauser, R.; James-Todd, T.; McElrath, T. Pregnancy phthalate metabolite concentrations and infant birth weight by gradations of maternal glucose tolerance. Int. J. Hyg. Environ. Health 2019, 222, 395–401. [Google Scholar] [CrossRef]
- ECHA. Annex XV Restriction Report Proposal for a Restriction Substance Names: Four Phthalates (DEHP, BBP, DBP, DIBP). 2016. Available online: https://echa.europa.eu/documents/10162/e06ddac2-5ff7-4863-83d5-2fb071a1ec13 (accessed on 23 March 2019).
- EPA. Phthalate Strategy Environmental Project No. 1488. 2013. Available online: https://www2.mst.dk/udgiv/publications/2013/06/978-87-93026-22-3.pdf (accessed on 23 March 2019).
- Wang, X.; Wang, X.; Chen, Q.; Luo, Z.; Zhao, S.; Wang, W.; Zhang, H.; Zhang, J.; Ouyang, F. Urinary Bisphenol A Concentration and Gestational Diabetes Mellitus in Chinese Women. Epidemiology 2017, 28, S41–S47. [Google Scholar] [CrossRef]
- Acconcia, F.; Pallottini, V.; Marino, M. Molecular Mechanisms of Action of BPA. Dose-Response 2015, 13, 1559325815610582. [Google Scholar] [CrossRef] [PubMed]
- Tiano, J.; Delghingaro-Augusto, V.; Le, C.; Liu, S.; Kaw, M.; Khuder, S.; Latour, M.; Bhatt, S.; Korach, K.; Najjar, S.; et al. Estrogen receptor activation reduces lipid synthesis in pancreatic islets and prevents beta cell failure in rodent models of type 2 diabetes. J. Clin. Investig. 2011, 121, 3331–3342. [Google Scholar] [CrossRef] [PubMed]
- Weldingh, N.; Jørgensen-Kaur, L.; Becher, R.; Holme, J.; Bodin, J.; Nygaard, U.; Bølling, A. Bisphenol A Is More Potent than Phthalate Metabolites in Reducing Pancreatic β-Cell Function. BioMed Res. Int. 2017, 2017, 4614379. [Google Scholar] [CrossRef] [PubMed]
- García-Arévalo, M.; Alonso-Magdalena, P.; Servitja, J.; Boronat-Belda, T.; Merino, B.; Villar-Pazos, S.; Medina-Gómez, G.; Novials, A.; Quesada, I.; Nadal, Á. Maternal Exposure to Bisphenol-A During Pregnancy Increases Pancreatic β-Cell Growth During Early Life in Male Mice Offspring. Endocrinology 2016, 157, 4158–4171. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Magdalena, P.; García-Arévalo, M.; Quesada, I.; Nadal, Á. Bisphenol-A treatment during pregnancy in mice: A new window of susceptibility for the development of diabetes in mothers later in life. Endocrinology 2015, 156, 1659–1670. [Google Scholar] [CrossRef]
- Moon, M.; Jeong, I.; Jung Oh, T.; Ahn, H.; Kim, H.; Park, Y.; Jang, H.; Park, K. Long-term oral exposure to bisphenol A induces glucose intolerance and insulin resistance. J. Endocrinol. 2015, 226, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Chailurkit, L.; Tengpraettanakorn, P.; Chanprasertyotin, S.; Ongphiphadhanakul, B. Is bisphenol A exposure associated with the development of glucose intolerance and increased insulin resistance in Thais? Nutr. Health 2017, 23, 185–191. [Google Scholar] [CrossRef]
- Fisher, B.; Frederiksen, H.; Andersson, A.; Juul, A.; Thankamony, A.; Ong, K.; Dunger, D.; Hughes, I.; Acerini, C. Serum Phthalate and Triclosan Levels Have Opposing Associations with Risk Factors for Gestational Diabetes Mellitus. Front. Endocrinol. 2018, 9, 99. [Google Scholar] [CrossRef]
- Somm, E.; Schwitzgebel, V.; Toulotte, A.; Cederroth, C.; Combescure, C.; Nef, S. Perinatal exposure to bisphenol A alters early adipogenesis in the rat. Environ. Health Perspect. 2009, 117, 1549–1555. [Google Scholar] [CrossRef]
- Wei, J.; Lin, Y.; Li, Y.; Ying, C.; Chen, J.; Song, L. Perinatal exposure to bisphenol A at reference dose predisposes offspring to metabolic syndrome in adult rats on a high-fat diet. Endocrinology 2011, 152, 3049–3061. [Google Scholar] [CrossRef]
- Xu, X.; Tan, L.; Himi, T.; Sadamatsu, M.; Tsutsumi, S.; Akaike, M. Changed preference for sweet taste in adulthood induced by perinatal exposure to bisphenol A: A prob-able link to overweight and obesity. Neurotoxicol. Teratol. 2011, 33, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Harley, K.; Aguilar Schall, R.; Chevrier, J.; Tyler, K.; Aguirre, H.; Bradman, A.; Holland, N.; Lustig, R.; Calafat, A.; Eskenazi, B. Prenatal and postnatal bisphenol A exposure and body mass index in childhood in the CHAMACOS cohort. Environ. Health Perspect. 2013, 121, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Fabian, E.; Wang, X.; Engel, F.; Li, H.; Landsiedel, R.; Ravenzwaay, B. Activities of xenobiotic metabolizing enzymes in rat placenta and liver in vitro. Toxicol. In Vitro 2016, 33, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Saxena, A.; Isganaitis, E.; James-Todd, T. Gender and racial/ethnic differences in the associations of urinary phthalate metabolites with markers of diabetes risk: National Health and Nutrition Examination Survey 2001–2008. Environ. Health 2014, 13, 6. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Nondiabetic Pregnant Women (n = 22) | Pregnant Women with GDM (n = 18) | p Value |
|---|---|---|---|
| Maternal Age (years) | 31.86 ± 5.1 | 34.11 ± 4.5 | 0.15 |
| Weeks of gestation at sampling | 18.92 ± 6.13 | 23.25 ± 5.43 | 0.13 |
| Pregestational BMI (kg/m2) | 30.15 ± 6. 6 | 29.47 ± 5.2 | 0.72 |
| Parity | 2.0 ± 1.3 | 2.6 ± 0.9 | 0.02 |
| First | 45% | 11.1% | |
| Second | 35% | 33.3% | |
| Third or more | 20% | 55.6% | |
| Pregnancy length (weeks) | 38.56 ± 1.57 | 37.39 ± 2.55 | 0.13 |
| OGTC (75 g) | |||
| Fasting plasma glucose (mg/dL) | 77.76 ± 9.3 | 99.89 ± 2.91 | <0.0001 |
| 1 h plasma glucose (mg/dL) | 129.6 ± 28.44 | 207.3 ± 24.87 | <0.0001 |
| 2 h plasma glucose (mg/dL) | 176.6 ± 17.93 | 180.0 ± 27.65 | <0.0001 |
| Chemical | GM | Minimum | Percentiles | Maximum | |||
|---|---|---|---|---|---|---|---|
| (95% CI) | 25th | 50th | 75th | 90th | |||
| Unadjusted | |||||||
| BPA | 35.22 (21.80–56.91) | 4.9 | 22.9 | 39.10 | 67.70 | 112.4 | 123.9 |
| MBzP | 1.86 (1.26–2.73) | 0.5 | 0.5 | 1.75 | 4.82 | 11.88 | 46.5 |
| MBP | 101.3 (78.48–130.8) | 24.0 | 58.73 | 105.3 | 153.4 | 243.2 | 1012 |
| MiBP | 10.35 (7.35–14.56) | 0.6 | 5.0 | 10.50 | 18.30 | 41.6 | 99.60 |
| MEHP | 12,837 (11426–14422) | 4976 | 10,648 | 13,049 | 15,814 | 20,675 | 24,524 |
| Adjusted | |||||||
| BPA | 31.19 (20.71–46.99) | 8.2 | 20.09 | 39.28 | 49.69 | 77.15 | 77.92 |
| MBzP | 1.71 (1.25–2.33) | 0.33 | 0.73 | 1.7 | 3.44 | 8.77 | 12.63 |
| MBP | 93.15 (81.14–106.9) | 35.43 | 64.20 | 97.34 | 118.2 | 174.5 | 210.4 |
| MiBP | 9.89 (7.68–12.75) | 1.15 | 6.29 | 10.36 | 16.62 | 29.49 | 46.03 |
| MEHP | 11,732 (9341–14,735) | 2141 | 7681 | 10,711 | 18,388 | 32,689 | 47,071 |
| Chemical | ND (n = 22) | GDM (n = 18) | ND | GDM | p value |
|---|---|---|---|---|---|
| Detection Frequency (%) | Detection Frequency (%) | GM (95% CI) | GM (95% CI) | ||
| Unadjusted | |||||
| BPA | 36.3 | 33 | 47.86 (26.94–85.03) | 23.4 (9.24–59.26) | 0.18 |
| MBzP | 100 | 100 | 1.83 (1.09–3.06) | 1.58 (0.92–2.7) | 0.67 |
| MBP | 100 | 100 | 102.7 (72.74–145.0) | 87.75 (62.79–122.6) | 0.53 |
| MiBP | 100 | 94.4 | 9.09 (5.41–15.27) | 9.7 (6.52–14.43) | 0.81 |
| MEHP | 100 | 100 | 13,135 (10,861–15,884) | 11,586 (10,408–12,898) | 0.03 |
| Adjusted | |||||
| BPA | 36.3 | 33 | 46.08 (30.99–68.52) | 19.79 (10.01–39.09) | 0.02 |
| MBzP | 100 | 100 | 1.75 (1.1–2.78) | 1.66 (1.05–2.61) | 0.98 |
| MBP | 100 | 100 | 94.22 (77.4–114.7) | 91.97 (74.22–114.0) | 0.94 |
| MiBP | 100 | 94.4 | 8.95 (6.06–13.23) | 11.19 (7.99–15.65) | 0.42 |
| MEHP | 100 | 100 | 11,855 (8200–17,138) | 11,582 (8778–15,282) | 0.72 |
| Chemical | mir-16 | mir-29a | Pregestational BMI | |||
|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |
| MBzP | ||||||
| ND | 0.2211 | 0.4737 * | −0.2496 | 0.01053 | −0.03088 | −0.04545 |
| GDM | 0.3274 | 0.1961 | 0.2107 | 0.1084 | 0.2233 | 0.1373 |
| MBP | ||||||
| ND | 0.07544 | 0.1744 | −0.7140 *** | −0.5418 * | −0.1545 | −0.2692 |
| GDM | 0.06127 | −0.2328 | 0.1785 | −0.1517 | 0.2425 | 0.01342 |
| MiBP | ||||||
| ND | −0.2737 | −0.1596 | −0.6719 ** | −0.3789 | 0.1403 | 0.1870 |
| GDM | −0.04290 | −0.06176 | 0.4165 | 0.1005 | −0.1104 | −0.3382 |
| MEHP | ||||||
| ND | −0.3947 | −0.1035 | 0.2947 | 0.4912 * | −0.08182 | −0.09351 |
| GDM | −0.05882 | −0.3627 | −0.05882 | −0.2735 | 0.7143 | −0.1723 |
| BPA | ||||||
| ND | 0.1786 | 0.7143 | 0.08571 | 0.5000 | 0.8810 ** | 0.5714 |
| GDM | 0.02857 | −0.02857 | −0.4857 | −0.6571 | 0.7143 | 0.4857 |
| Population | Country | Trimester | GM (μg/L) | Ref. | ||||
|---|---|---|---|---|---|---|---|---|
| BPA | MEHP | MBP | MBzP | MiBP | ||||
| This study (N = 40) | Mexico | 2nd | 35.22 | 12837 | 101.3 | 1.86 | 10.35 | |
| Harvard Epigenetic Birth Cohort (HEBC) and the Predictors of Preeclampsia Study (POPS) (N = 179) | USA | 1st | 1.36 | 4.38 | - | 5.34 | 5.74 | [46] |
| The Plastics and Personal-care Products use in Pregnancy (P4) study (N = 70) | Canada | 1st | 1.14 | 2.24 | 16.2 | 9.85 | 7.40 | [47] |
| 2nd | 1.31 | 2.09 | 19.16 | 8.80 | - | |||
| 3rd | 1.31 | 2.26 | 22.63 | 10.70 | - | |||
| Early Life Exposure in Mexico to Environmental Toxicants (ELEMENT study) (N = 60) | Mexico | 3rd | 1.52 | - | - | - | - | [19] |
| Mothers and Children’s Environmental Health (MOCEH) study (N = 757) | Korea | 3rd | 1.29 | - | - | - | - | [22] |
| The Early Life in Mexico to Environmental Toxicants (ELEMENT Study) (N = 249) | Mexico | 3rd | 0.74 | 5.20 | 56.90 | 4.50 | 1.99 | [44] |
| Columbia Center for Children’s Environmental Health (CCCEH) cohort (N = 246) | USA | 3rd | - | 4.80 | - | 17.50 | 9.50 | [48] |
| The Infant Development and Environment Study (TIDES) (N = 668) | USA | 1st | - | 2.50 | - | 4.30 | 5.20 | [49] |
| 3rd | - | 2.10 | - | 4.80 | 7.20 | |||
| Unnamed Cohort (N = 30) | China | 3rd | - | 4.43 | 4.15 | 0.46 | 2.96 | [50] |
| LifeCodes Study (N = 350) | USA | 1st | - | - | 14.20 | 5.50 | 6.10 | [51] |
| 2nd | - | - | 15.20 | 6.00 | 6.50 | |||
| 3rd | - | - | 16.30 | 6.70 | 7.00 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Ibarra, A.; Martínez-Razo, L.D.; Vázquez-Martínez, E.R.; Martínez-Cruz, N.; Flores-Ramírez, R.; García-Gómez, E.; López-López, M.; Ortega-González, C.; Camacho-Arroyo, I.; Cerbón, M. Unhealthy Levels of Phthalates and Bisphenol A in Mexican Pregnant Women with Gestational Diabetes and Its Association to Altered Expression of miRNAs Involved with Metabolic Disease. Int. J. Mol. Sci. 2019, 20, 3343. https://doi.org/10.3390/ijms20133343
Martínez-Ibarra A, Martínez-Razo LD, Vázquez-Martínez ER, Martínez-Cruz N, Flores-Ramírez R, García-Gómez E, López-López M, Ortega-González C, Camacho-Arroyo I, Cerbón M. Unhealthy Levels of Phthalates and Bisphenol A in Mexican Pregnant Women with Gestational Diabetes and Its Association to Altered Expression of miRNAs Involved with Metabolic Disease. International Journal of Molecular Sciences. 2019; 20(13):3343. https://doi.org/10.3390/ijms20133343
Chicago/Turabian StyleMartínez-Ibarra, Alejandra, Luis Daniel Martínez-Razo, Edgar Ricardo Vázquez-Martínez, Nayeli Martínez-Cruz, Rogelio Flores-Ramírez, Elizabeth García-Gómez, Marisol López-López, Carlos Ortega-González, Ignacio Camacho-Arroyo, and Marco Cerbón. 2019. "Unhealthy Levels of Phthalates and Bisphenol A in Mexican Pregnant Women with Gestational Diabetes and Its Association to Altered Expression of miRNAs Involved with Metabolic Disease" International Journal of Molecular Sciences 20, no. 13: 3343. https://doi.org/10.3390/ijms20133343