
A Review of the Pathophysiology and Potential Biomarkers for Peripheral Artery Disease



Abstract
:1. Introduction
2. Epidemiology of PAD
3. Risk Factors for PAD
4. Current PAD Management Strategies
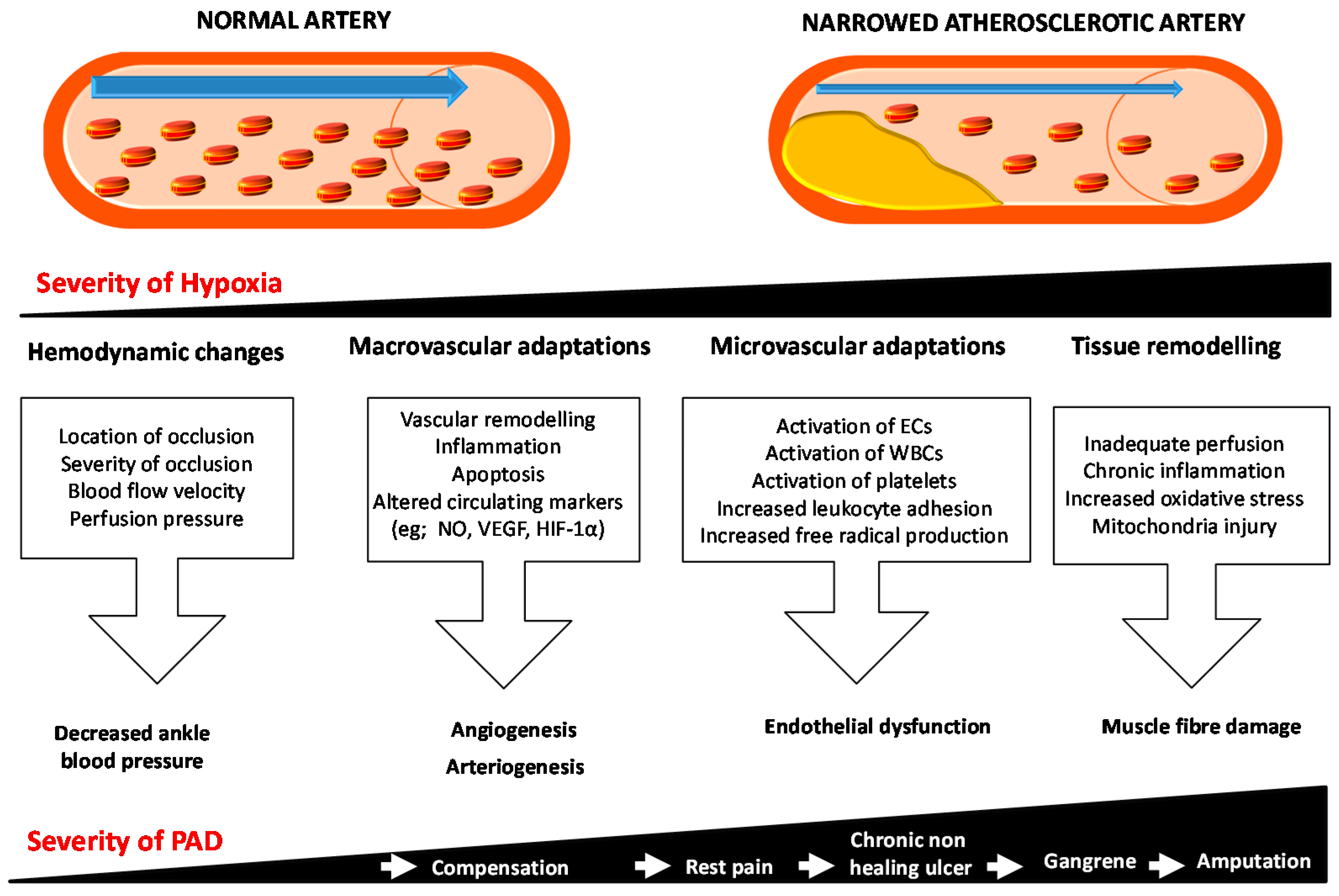
5. The Pathophysiological Response to Athero-Thombosis-Induced PAD

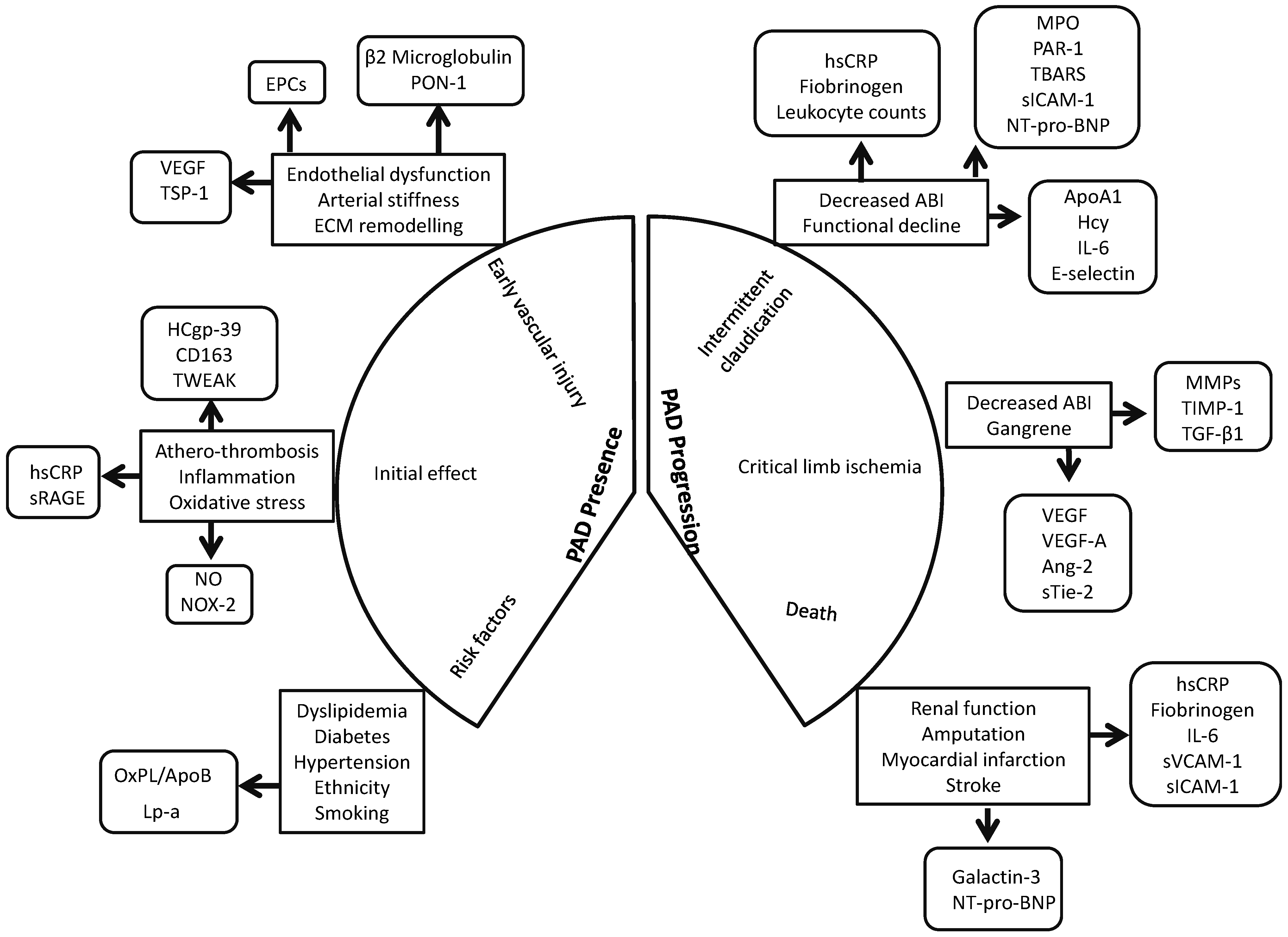
6. Potential Biomarkers for PAD
6.1. Circulating Markers Associated with the Presence of PAD

{kind=link}
{kind=link}
| Circulating Biomarkers Assessed | Sample Size (N) | Sample Studied | Association with PAD Presence | Refs. |
|---|---|---|---|---|
| B2M & cystatin C | CAD & PAD (197); CAD (81) & healthy controls (262) | Plasma | A biomarker panel comprising B2M, cystatin C, hsCRP and glucose were associated with PAD. | [65] |
| B2M, cystatin C, hsCRP & glucose | PAD (83) & controls (896) | Plasma | Levels of cystatin C and B2M but not hsCRP and glucose were significantly elevated in PAD patients. | [66] |
| aPWV, AIx & B2M | PAD (66) & healthy controls (66) | Plasma | B2M, aPWV and AIx were significantly increased in patients with PAD; among patients with PAD elevated B2M levels were independently associated with higher aortic stiffness. | [67] |
| hsCRP, fibrinogen & leukocyte count | The National Health and Nutrition Examination Survey 1999–2002 (4787 participants aged ≥ 40 years) | Blood | All 3 markers were independently associated with PAD. | [68] |
| hsCRP | PAD (82) & healthy controls (41) | Plasma | Increased hsCRP levels in PAD patients. | [69] |
| CD40 ligand, fibrinogen, Lp-PLA2 , osteoprotegerin, P-selectin, and TNF-R2, hsCRP, ICAM-1, IL-6, MCP-1 & MPO | Framingham Offspring Study participants (2800) | Plasma | IL-6 &TNF-R2 were associated with PAD independent of established risk factors. | [70] |
| VEGF-A, TNF-α & IL-8 | PAD (130) & controls (36) | Serum | Lower VEGF-A and higher TNF-α & IL-8 in PAD patients. | [71] |
| High molecular weight & total adiponectin | PAD (110) & healthy controls (230) | Plasma | Lower adiponectin in women with PAD. | [72] |
| OxPL/ApoB & Lp-a | Men with PAD (143), women with PAD (144) & controls (432) | Plasma | Increased levels of OxPL/ApoB and Lp-a were associated with PAD. | [73] |
| Lp-PLA2 activity | PAD (172) & healthy controls (787) | Plasma | Increased Lp-PLA2 activity in PAD patients. | [74] |
| Lp-PLA2 level | PAD (145) & healthy controls (837) | Plasma | Lp-PLA2 levels were significantly associated with PAD. | [75] |
| NOx &, sNOX2-dp | PAD (50) & healthy controls (50) | Serum | NOX2 up-regulation is associated with artery dysfunction in PAD. | [76] |
| NO | PAD (82) & healthy controls (41) | Plasma | Increased NO levels & hsCRP levels in PAD patients. | [69] |
| TBARS & ICAM-1 | PAD (31) & healthy controls (10) | Plasma | Increased in PAD. | [77] |
| Rho-kinase activity | PAD (40), combined CAD/PAD (40) & healthy controls (40) | Circulating leukocytes | Increased in PAD. | [78] |
| HCgp-39 | PAD (316) & healthy controls (39) | Plasma | Median levels of HCgp-39 were significantly higher in PAD patients. | [79] |
| CD163 & TWEAK | PAD (155) & healthy controls (251) | Plasma | Decreased TWEAK level and higher sCD163 levels in PAD patients. | [80] |
| PON-3 | PAD (118), CAD (72) & healthy controls (175) | Serum | Increased in PAD. | [81] |
| IL-6, E-selectin, MMP-2, MMP-9 & TGF-β1 | PAD (80) & healthy controls (3076) | Plasma | Increased levels of IL-6, E-selectin, MMP-2 & MMP-9 and reduced levels of TGF-β1 in PAD patients. | [82] |
| sRAGE | PAD (201) & healthy controls (201) | Plasma | Decreased levels of sRAGE in PAD patients. | [83] |
| VEGF | PAD (293) & healthy controls (26) | Serum | Higher levels of VEGF in PAD patients. | [84] |
| Ang2, sTie2, VEGF, sVEGFR-1 & PlGF | PAD (46) & healthy controls (23) | Plasma | Levels of VEGF and sTie2 were significantly increased in PAD patients. | [85] |
| VEGF, PlGF & TSP-1 | PAD (184) & healthy controls (330) | Plasma | Elevated TSP-1 levels associated with PAD. | [86] |
| VEGF-A, TNF-α & IL-8 | PAD (130) & controls (36) | Serum | PAD patients have lower circulating VEGF-A and higher levels of TNF-α and IL-8. | [71] |
| EPCs, CD133, VEGFR-2, MDA-LDL & pentraxin-3 | PAD (48) & healthy controls (22) | Serum & Plasma | EPCs and pentraxin-3 were increased in PAD patients; Cardiovascular events in PAD patients were associated with reduced EPC and increased MDA-LDL. | [87] |
| EPCs | PAD (45) & healthy controls (24) | Blood | The number and proliferative activity of circulating EPCs was significantly increased in PAD patients. | [88] |
6.1.1. Markers of Athero-Thrombosis and Inflammation
6.1.2. Markers of Oxidative Stress
6.1.3. Markers of Vascular Remodeling
6.1.4. Circulating Progenitor Cells
6.2. Markers Associated with the Severity and Outcome of PAD
| Circulating Biomarkers Assessed | Sample Size (N) | Sample Studied | Association with PAD Severity | Refs. |
|---|---|---|---|---|
| hsCRP, albumin, α-2 macroglobulin, fibrinogen, IL-1β, IL-1 receptor antagonist, IL-6, IL-6 receptor, IL-10, IL-18, TNF-α, & TGF-β | InCHIANTI study; PAD (955) | Serum | Higher levels of IL-1 receptor antagonist, IL-6, fibrinogen and hsCRP in PAD patients. | [107] |
| hsCRP, DD, TAT III & vWF | IC (132) & CLI (30) | Plasma | Higher levels of hsCRP, vWF, and TAT III in CLI compared to patients with IC. | [108] |
| hsCRP, fibrinogen & SAA | PAD (91) | Plasma | hsCRP, fibrinogen, and SAA levels were significantly associated with CLI; elevated hsCRP correlated with adverse graft-related or cardiovascular events. | [109] |
| hsCRP, DD, IL-6, VCAM-1, ICAM-1 & Hcy | Walking and Leg Circulation Study (WALCS); PAD (423) | Serum | Higher levels of inflammation markers and DD were associated with poorer lower extremity performance. | [110] |
| hsCRP, DD, SAA & fibrinogen | PAD (337) | Serum | Elevated baseline levels of inflammatory markers and DD were associated with greater decline in the physical performance. | [111] |
| hsCRP | PAD (225) | Plasma | A risk prediction model including hsCRP combined with traditional risk factors, renal function, and nutrition had excellent discriminatory ability in predicting all-cause mortality in patients with clinically advanced PAD undergoing bypass surgery. | [112] |
| hsCRP | PAD (118) | Plasma | Increased pre-procedural hsCRP levels were associated with major adverse limb events and late cardiovascular events. | [113] |
| hsCRP | Hemodialysis patients undergoing endovascular therapy for PAD (234) | Serum | Elevated pre-procedural hsCRP levels were associated with re-intervention or above ankle amputation and any-cause death after endovascular therapy. | [114] |
| hsCRP | European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk cohort; Healthy participants (18,450) | Serum | In the EPIC-Norfolk cohort, hsCRP was associated with nonfatal PAD events. | [115] |
| hsCRP, LDL & HDL | Total PAD (100); IC (73) | Blood | Walking disability in PAD was associated with arterial endothelial dysfunction; Endothelial dysfunction was more significantly associated with walking disability in IC. | [116] |
| ApoA-I, HDL, Hcy, folate & vitamin B12 | Elderly volunteers from rural Sicily (667) | Serum | Decreased ApoA-I and increased Hcy were predictors of ABI. | [91] |
| VCAM-1, ICAM-1 & MCP-1 | PAD (112) | Serum | Increased sVCAM-1 and sICAM-1 were associated with PAD. | [117] |
| ICAM-1, leptin, Apolipoprotein-CIII | PAD (148) | Serum | African American women with symptomatic PAD had an increased oxidative stress related markers compared with men. | [96] |
| MPO | PAD (406) | Plasma | Plasma level was useful for risk stratification of PAD. | [118] |
| TRAP-6-inducible P-selectin expression | PAD (108) | Blood | Low thrombin generation potential was associated with an 11.7-fold increased risk of future atherothrombotic events. | [119] |
| Galectin-3 | CLI (55) | Serum | Increased levels of Galectin-3 in CLI. | [120] |
| NT-pro-BNP | PCA (100), PAD (300) & healthy controls (300) | Serum | Patients with PCA had higher levels of NT pro-BNP than PAD and controls suggestive of an adverse hemodynamic milieu and increased risk for adverse cardiovascular outcomes. | [121] |
| NT-pro-BNP | PAD (481) | Serum | Higher levels of NT-pro-BNP were independently associated with a lower ordinal walking category or functional capacity. | [122] |
| Ang2, Tie2, VEGF, VEGFR-1 & PlGF | PAD (46) & healthy controls (23) | Plasma | Levels of VEGF and sTie2 were significantly increased in CLI. | [85] |
| VEGF-A 165b | PAD (18) | Serum | Increased anti-angiogenic VEGF-165b and a corresponding reduction in levels of the pro-angiogenic VEGF-A165a. | [123] |
6.2.1. Markers of Inflammation
6.2.2. Markers of Oxidative Stress and Endothelial Damage
6.2.3. Markers of Vascular Remodeling
7. Conclusions

Acknowledgments
Author Contributions
Conflicts of Interest
References
- Knowles, J.W.; Assimes, T.L.; Li, J.; Quertermous, T.; Cooke, J.P. Genetic susceptibility to peripheral arterial disease: A dark corner in vascular biology. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2068–2078. [Google Scholar] [CrossRef] [PubMed]
- Subherwal, S.; Patel, M.R.; Kober, L.; Peterson, E.D.; Bhatt, D.L.; Gislason, G.H.; Olsen, A.M.; Jones, W.S.; Torp-Pedersen, C.; Fosbol, E.L. Peripheral artery disease is a coronary heart disease risk equivalent among both men and women: Results from a nationwide study. Eur. J. Prev. Cardiol. 2015, 22, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Walker, T.G. Acute limb ischemia. Tech. Vasc. Interv. Radiol. 2009, 12, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.E.; Eikelboom, J.W.; Hankey, G.J. Peripheral arterial disease: Prognostic significance and prevention of atherothrombotic complications. Med. J. Aust. 2004, 181, 150–154. [Google Scholar] [PubMed]
- Bergiers, S.; Vaes, B.; Degryse, J. To screen or not to screen for peripheral arterial disease in subjects aged 80 and over in primary health care: A cross-sectional analysis from the belfrail study. BMC Family Pract. 2011, 12, 39. [Google Scholar] [CrossRef]
- Hirsch, A.T.; Criqui, M.H.; Treat-Jacobson, D.; Regensteiner, J.G.; Creager, M.A.; Olin, J.W.; Krook, S.H.; Hunninghake, D.B.; Comerota, A.J.; Walsh, M.E.; et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001, 286, 1317–1324. [Google Scholar] [CrossRef] [PubMed]
- Allison, M.A.; Ho, E.; Denenberg, J.O.; Langer, R.D.; Newman, A.B.; Fabsitz, R.R.; Criqui, M.H. Ethnic-specific prevalence of peripheral arterial disease in the united states. Am. J. Prev. Med. 2007, 32, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Erlinger, T.P. Prevalence of and risk factors for peripheral arterial disease in the united states: Results from the national health and nutrition examination survey, 1999–2000. Circulation 2004, 110, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Dohmen, A.; Eder, S.; Euringer, W.; Zeller, T.; Beyersdorf, F. Chronic critical limb ischemia. Dtsch. Arztebl. Int. 2012, 109, 95–101. [Google Scholar] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; Bell, K.; Caporusso, J.; Durand-Zaleski, I.; Komori, K.; et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur. J. Vasc. Endovasc. Surg. 2007, 33 (Suppl. S1), S1–S75. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S.; Pomposelli, F.B.; Clair, D.G.; Geraghty, P.J.; McKinsey, J.F.; Mills, J.L.; Moneta, G.L.; Murad, M.H.; Powell, R.J.; et al. Society for vascular surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: Management of asymptomatic disease and claudication. J. Vasc. Surg. 2015; 61, S2–S41. [Google Scholar]
- Hirsch, A.T.; Hartman, L.; Town, R.J.; Virnig, B.A. National health care costs of peripheral arterial disease in the medicare population. Vasc. Med. 2008, 13, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Adam, D.J.; Beard, J.D.; Cleveland, T.; Bell, J.; Bradbury, A.W.; Forbes, J.F.; Fowkes, F.G.; Gillepsie, I.; Ruckley, C.V.; Raab, G.; et al. Bypass versus angioplasty in severe ischaemia of the leg (basil): Multicentre, randomised controlled trial. Lancet 2005, 366, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- Lawall, H.; Bramlage, P.; Amann, B. Treatment of peripheral arterial disease using stem and progenitor cell therapy. J. Vasc. Surg. 2011, 53, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.; Olin, J.W.; Puschett, J.B.; et al. Acc/aha 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): A collaborative report from the american association for vascular surgery/society for vascular surgery, society for cardiovascular angiography and interventions, society for vascular medicine and biology, society of interventional radiology, and the acc/aha task force on practice guidelines (writing committee to develop guidelines for the management of patients with peripheral arterial disease): Endorsed by the american association of cardiovascular and pulmonary rehabilitation; national heart, lung, and blood institute; society for vascular nursing; transatlantic inter-society consensus; and vascular disease foundation. Circulation 2006, 113, e463–e654. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef] [PubMed]
- Varu, V.N.; Hogg, M.E.; Kibbe, M.R. Critical limb ischemia. J. Vasc. Surg. 2010, 51, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.F.; Weinberg, M.D.; Olin, J.W. Peripheral artery disease. Part 1: Clinical evaluation and noninvasive diagnosis. Nat. Rev. Cardiol. 2011, 8, 405–418. [Google Scholar] [CrossRef] [PubMed]
- Cheshire, N.J.; Wolfe, J.H.; Noone, M.A.; Davies, L.; Drummond, M. The economics of femorocrural reconstruction for critical leg ischemia with and without autologous vein. J. Vasc. Surg. 1992, 15, 167–174, discussion 174–165. [Google Scholar] [CrossRef] [PubMed]
- Albers, M.; Fratezi, A.C.; de Luccia, N. Assessment of quality of life of patients with severe ischemia as a result of infrainguinal arterial occlusive disease. J. Vasc. Surg. 1992, 16, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Schuler, J.J.; Flanigan, D.P.; Holcroft, J.W.; Ursprung, J.J.; Mohrland, J.S.; Pyke, J. Efficacy of prostaglandin E1 in the treatment of lower extremity ischemic ulcers secondary to peripheral vascular occlusive disease. Results of a prospective randomized, double-blind, multicenter clinical trial. J. Vasc. Surg. 1984, 1, 160–170. [Google Scholar] [PubMed]
- Santilli, J.D.; Santilli, S.M. Chronic critical limb ischemia: Diagnosis, treatment and prognosis. Am. Fam. Physician 1999, 59, 1899–1908. [Google Scholar] [PubMed]
- Arnold, T.E.; Kerstein, M.D. Secondary distal extension of infrainguinal bypass: Long-term limb and patient survival. Ann. Vasc. Surg. 2000, 14, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Brumberg, R.S.; Back, M.R.; Armstrong, P.A.; Cuthbertson, D.; Shames, M.L.; Johnson, B.L.; Bandyk, D.F. The relative importance of graft surveillance and warfarin therapy in infrainguinal prosthetic bypass failure. J. Vasc. Surg. 2007, 46, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.G. Critical limb ischemia: Cell and molecular therapies for limb salvage. Methodist DeBakey Cardiovasc. J. 2012, 8, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Sigvant, B.; Wiberg-Hedman, K.; Bergqvist, D.; Rolandsson, O.; Andersson, B.; Persson, E.; Wahlberg, E. A population-based study of peripheral arterial disease prevalence with special focus on critical limb ischemia and sex differences. J. Vasc. Surg. 2007, 45, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Peacock, J.M.; Keo, H.H.; Duval, S.; Baumgartner, I.; Oldenburg, N.C.; Jaff, M.R.; Henry, T.D.; Yu, X.; Hirsch, A.T. The incidence and health economic burden of ischemic amputation in minnesota, 2005–2008. Prev. Chronic Dis. 2011, 8, A141. [Google Scholar] [PubMed]
- Meijer, W.T.; Grobbee, D.E.; Hunink, M.G.; Hofman, A.; Hoes, A.W. Determinants of peripheral arterial disease in the elderly: The rotterdam study. Arch. Intern. Med. 2000, 160, 2934–2938. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Marinopoulos, S.; Berkenblit, G.; Rami, T.; Brancati, F.L.; Powe, N.R.; Golden, S.H. Meta-analysis: Glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann. Intern. Med. 2004, 141, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Wildman, R.P.; Reynolds, K.; Desalvo, K.B.; Chen, J.; Fonseca, V. Relationship between HbA1c level and peripheral arterial disease. Diabetes Care 2005, 28, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Lo, R.C.; Bensley, R.P.; Dahlberg, S.E.; Matyal, R.; Hamdan, A.D.; Wyers, M.; Chaikof, E.L.; Schermerhorn, M.L. Presentation, treatment, and outcome differences between men and women undergoing revascularization or amputation for lower extremity peripheral arterial disease. J. Vasc. Surg. 2014, 59, 409–418. [Google Scholar] [CrossRef] [PubMed]
- McGinigle, K.L.; Kalbaugh, C.A.; Marston, W.A. Living in a medically underserved county is an independent risk factor for major limb amputation. J. Vasc. Surg. 2014, 59, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Fadini, G.P.; Agostini, C.; Avogaro, A. Autologous stem cell therapy for peripheral arterial disease meta-analysis and systematic review of the literature. Atherosclerosis 2010, 209, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Lawall, H.; Bramlage, P.; Amann, B. Stem cell and progenitor cell therapy in peripheral artery disease. A critical appraisal. Thromb. Haemost. 2010, 103, 696–709. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.R.; Rodriguez, A.J.; Moxon, J.V.; Cunningham, M.A.; McDermott, M.M.; Myers, J.; Leeper, N.J.; Jones, R.E.; Golledge, J. Association of lower extremity performance with cardiovascular and all-cause mortality in patients with peripheral artery disease: A systematic review and meta-analysis. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [PubMed]
- Aranguren, X.L.; Verfaillie, C.M.; Luttun, A. Emerging hurdles in stem cell therapy for peripheral vascular disease. J. Mol. Med. 2009, 87, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.S.; Dolor, R.J.; Hasselblad, V.; Vemulapalli, S.; Subherwal, S.; Schmit, K.; Heidenfelder, B.; Patel, M.R. Comparative effectiveness of endovascular and surgical revascularization for patients with peripheral artery disease and critical limb ischemia: Systematic review of revascularization in critical limb ischemia. Am. Heart. J. 2014, 167, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Tongers, J.; Losordo, D.W. Human studies of angiogenic gene therapy. Circ. Res. 2009, 105, 724–736. [Google Scholar] [CrossRef] [PubMed]
- De Haro, J.; Acin, F.; Lopez-Quintana, A.; Florez, A.; Martinez-Aguilar, E.; Varela, C. Meta-analysis of randomized, controlled clinical trials in angiogenesis: Gene and cell therapy in peripheral arterial disease. Heart Vessels 2009, 24, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Matoba, S.; Tatsumi, T.; Murohara, T.; Imaizumi, T.; Katsuda, Y.; Ito, M.; Saito, Y.; Uemura, S.; Suzuki, H.; Fukumoto, S.; et al. Long-term clinical outcome after intramuscular implantation of bone marrow mononuclear cells (therapeutic angiogenesis by cell transplantation (TACT) trial) in patients with chronic limb ischemia. Am. Heart. J. 2008, 156, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Powell, R.J.; Marston, W.A.; Berceli, S.A.; Guzman, R.; Henry, T.D.; Longcore, A.T.; Stern, T.P.; Watling, S.; Bartel, R.L. Cellular therapy with ixmyelocel-T to treat critical limb ischemia: The randomized, double-blind, placebo-controlled RESTORE-CLI trial. Mol. Ther. J. Am. Soc. Gene Ther. 2012, 20, 1280–1286. [Google Scholar] [CrossRef]
- Coats, P.; Wadsworth, R. Marriage of resistance and conduit arteries breeds critical limb ischemia. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H1044–H1050. [Google Scholar] [CrossRef] [PubMed]
- Scholz, D.; Ziegelhoeffer, T.; Helisch, A.; Wagner, S.; Friedrich, C.; Podzuweit, T.; Schaper, W. Contribution of arteriogenesis and angiogenesis to postocclusive hindlimb perfusion in mice. J. Mol. Cell. Cardiol. 2002, 34, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Kuang, S.; Gillespie, M.A.; Rudnicki, M.A. Niche regulation of muscle satellite cell self-renewal and differentiation. Cell Stem Cell 2008, 2, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Badimon, L.; Vilahur, G. Thrombosis formation on atherosclerotic lesions and plaque rupture. J. Intern. Med. 2014, 276, 618–632. [Google Scholar] [CrossRef] [PubMed]
- Popovic, M.; Smiljanic, K.; Dobutovic, B.; Syrovets, T.; Simmet, T.; Isenovic, E.R. Thrombin and vascular inflammation. Mol. Cell. Biochem. 2012, 359, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Franchini, M.; Targher, G. Arterial thrombus formation in cardiovascular disease. Nat. Rev. Cardiol. 2011, 8, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Koutakis, P.; Myers, S.A.; Cluff, K.; Ha, D.M.; Haynatzki, G.; McComb, R.D.; Uchida, K.; Miserlis, D.; Papoutsi, E.; Johanning, J.M.; et al. Abnormal myofiber morphology and limb dysfunction in claudication. J. Surg. Res. 2015. [Google Scholar] [CrossRef]
- Pipinos, I.I.; Judge, A.R.; Selsby, J.T.; Zhu, Z.; Swanson, S.A.; Nella, A.A.; Dodd, S.L. The myopathy of peripheral arterial occlusive disease: Part 1. Functional and histomorphological changes and evidence for mitochondrial dysfunction. Vasc. Endovasc. Surg. 2007, 41, 481–489. [Google Scholar] [CrossRef]
- Pipinos, I.I.; Judge, A.R.; Selsby, J.T.; Zhu, Z.; Swanson, S.A.; Nella, A.A.; Dodd, S.L. The myopathy of peripheral arterial occlusive disease: Part 2. Oxidative stress, neuropathy, and shift in muscle fiber type. Vasc. Endovasc. Surg. 2008, 42, 101–112. [Google Scholar] [CrossRef]
- Hickman, P.; Harrison, D.K.; Hill, A.; McLaren, M.; Tamei, H.; McCollum, P.T.; Belch, J.J. Exercise in patients with intermittent claudication results in the generation of oxygen derived free radicals and endothelial damage. Adv. Exp. Med. Biol. 1994, 361, 565–570. [Google Scholar] [PubMed]
- Bhat, H.K.; Hiatt, W.R.; Hoppel, C.L.; Brass, E.P. Skeletal muscle mitochondrial DNA injury in patients with unilateral peripheral arterial disease. Circulation 1999, 99, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Scholz, D.; Cai, W.J.; Schaper, W. Arteriogenesis, a new concept of vascular adaptation in occlusive disease. Angiogenesis 2001, 4, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Pipp, F.; Boehm, S.; Cai, W.J.; Adili, F.; Ziegler, B.; Karanovic, G.; Ritter, R.; Balzer, J.; Scheler, C.; Schaper, W.; et al. Elevated fluid shear stress enhances postocclusive collateral artery growth and gene expression in the pig hind limb. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1664–1668. [Google Scholar] [CrossRef] [PubMed]
- Tronc, F.; Wassef, M.; Esposito, B.; Henrion, D.; Glagov, S.; Tedgui, A. Role of no in flow-induced remodeling of the rabbit common carotid artery. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 1256–1262. [Google Scholar] [CrossRef] [PubMed]
- Tronc, F.; Mallat, Z.; Lehoux, S.; Wassef, M.; Esposito, B.; Tedgui, A. Role of matrix metalloproteinases in blood flow-induced arterial enlargement: Interaction with no. Arterioscler. Thromb. Vasc. Biol. 2000, 20, E120–E126. [Google Scholar] [CrossRef] [PubMed]
- Dragneva, G.; Korpisalo, P.; Yla-Herttuala, S. Promoting blood vessel growth in ischemic diseases: Challenges in translating preclinical potential into clinical success. Dis. Model. Mech. 2013, 6, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, M.; Nakagami, H.; Taniyama, Y.; Morishita, R. Gene therapy for peripheral arterial disease. Expert Opin. Biol. Ther. 2014, 14, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, M.; Nakagami, H.; Koriyama, H.; Morishita, R. Gene therapy and cell-based therapies for therapeutic angiogenesis in peripheral artery disease. Biol. Med. Res. Int. 2013, 2013, 186215. [Google Scholar]
- Henry, T.D.; Hirsch, A.T.; Goldman, J.; Wang, Y.L.; Lips, D.L.; McMillan, W.D.; Duval, S.; Biggs, T.A.; Keo, H.H. Safety of a non-viral plasmid-encoding dual isoforms of hepatocyte growth factor in critical limb ischemia patients: A phase I study. Gene Ther. 2011, 18, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Lara-Hernandez, R.; Lozano-Vilardell, P.; Blanes, P.; Torreguitart-Mirada, N.; Galmes, A.; Besalduch, J. Safety and efficacy of therapeutic angiogenesis as a novel treatment in patients with critical limb ischemia. Ann. Vasc. Surg. 2010, 24, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Mohler, E.R., 3rd; Treat-Jacobson, D.; Reilly, M.P.; Cunningham, K.E.; Miani, M.; Criqui, M.H.; Hiatt, W.R.; Hirsch, A.T. Utility and barriers to performance of the ankle-brachial index in primary care practice. Vasc. Med. 2004, 9, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Haigh, K.J.; Bingley, J.; Golledge, J.; Walker, P.J. Barriers to screening and diagnosis of peripheral artery disease by general practitioners. Vasc. Med. 2013, 18, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Fung, E.T.; Wilson, A.M.; Zhang, F.; Harris, N.; Edwards, K.A.; Olin, J.W.; Cooke, J.P. A biomarker panel for peripheral arterial disease. Vasc. Med. 2008, 13, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, W.R.; Zakharyan, A.; Fung, E.T.; Crutcher, G.; Smith, A.; Stanford, C.; Cooke, J. A validated biomarker panel to identify peripheral artery disease. Vasc. Med. 2012, 17, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Kals, J.; Zagura, M.; Serg, M.; Kampus, P.; Zilmer, K.; Unt, E.; Lieberg, J.; Eha, J.; Peetsalu, A.; Zilmer, M. β-2-microglobulin, a novel biomarker of peripheral arterial disease, independently predicts aortic stiffness in these patients. Scand. J. Clin. Lab. Investig. 2011, 71, 257–263. [Google Scholar] [CrossRef]
- Wildman, R.P.; Muntner, P.; Chen, J.; Sutton-Tyrrell, K.; He, J. Relation of inflammation to peripheral arterial disease in the national health and nutrition examination survey, 1999–2002. Am. J. Cardiol. 2005, 96, 1579–1583. [Google Scholar] [CrossRef] [PubMed]
- De Haro Miralles, J.; Martinez-Aguilar, E.; Florez, A.; Varela, C.; Bleda, S.; Acin, F. Nitric oxide: Link between endothelial dysfunction and inflammation in patients with peripheral arterial disease of the lower limbs. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Murabito, J.M.; Keyes, M.J.; Guo, C.Y.; Keaney, J.F., Jr.; Vasan, R.S.; D’Agostino, R.B., Sr.; Benjamin, E.J. Cross-sectional relations of multiple inflammatory biomarkers to peripheral arterial disease: The framingham offspring study. Atherosclerosis 2009, 203, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.W.; Parker, D.E.; Montgomery, P.S.; Sosnowska, D.; Casanegra, A.I.; Esponda, O.L.; Ungvari, Z.; Csiszar, A.; Sonntag, W.E. Impaired vascular endothelial growth factor a and inflammation in patients with peripheral artery disease. Angiology 2014, 65, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.Y.; Cook, N.R.; Britton, K.A.; Kim, E.; Creager, M.A.; Ridker, P.M.; Pradhan, A.D. High-molecular-weight and total adiponectin levels and incident symptomatic peripheral artery disease in women: A prospective investigation. Circulation 2011, 124, 2303–2311. [Google Scholar] [CrossRef] [PubMed]
- Bertoia, M.L.; Pai, J.K.; Lee, J.H.; Taleb, A.; Joosten, M.M.; Mittleman, M.A.; Yang, X.; Witztum, J.L.; Rimm, E.B.; Tsimikas, S.; et al. Oxidation-specific biomarkers and risk of peripheral artery disease. J. Am. Coll. Cardiol. 2013, 61, 2169–2179. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.S.; Ballantyne, C.M.; Davidson, M.H.; Johnson, J.L.; Tarka, E.A.; Lawrence, D.; Trivedi, T.; Zalewski, A.; Mohler, E.R., 3rd. Peripheral artery disease, biomarkers, and darapladib. Am. Heart J. 2011, 161, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Li, S.B.; Yang, F.; Jing, L.; Ma, J.; Jia, Y.D.; Dong, S.Y.; Zheng, W.F.; Zhao, L.S. Correlation between plasma lipoprotein-associated phospholipase A2 and peripheral arterial disease. Exp. Ther. Med. 2013, 5, 1451–1455. [Google Scholar] [PubMed]
- Loffredo, L.; Carnevale, R.; Cangemi, R.; Angelico, F.; Augelletti, T.; di Santo, S.; Calabrese, C.M.; della Volpe, L.; Pignatelli, P.; Perri, L.; et al. Nox2 up-regulation is associated with artery dysfunction in patients with peripheral artery disease. Int. J. Cardiol. 2013, 165, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Silvestro, A.; Scopacasa, F.; Oliva, G.; de Cristofaro, T.; Iuliano, L.; Brevetti, G. Vitamin C prevents endothelial dysfunction induced by acute exercise in patients with intermittent claudication. Atherosclerosis 2002, 165, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Jiang, X.; Liao, J.K.; Yan, B.P. Elevated Rho-kinase activity as a marker indicating atherosclerosis and inflammation burden in polyvascular disease patients with concomitant coronary and peripheral arterial disease. Clin. Cardiol. 2013, 36, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Batinic, K.; Hobaus, C.; Grujicic, M.; Steffan, A.; Jelic, F.; Lorant, D.; Hortenhuber, T.; Hoellerl, F.; Brix, J.M.; Schernthaner, G.; et al. Ykl-40 is elevated in patients with peripheral arterial disease and diabetes or pre-diabetes. Atherosclerosis 2012, 222, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.A.; Dejouvencel, T.; Labreuche, J.; Smadja, D.M.; Dussiot, M.; Martin-Ventura, J.L.; Egido, J.; Gaussem, P.; Emmerich, J.; Michel, J.B.; et al. Peripheral artery disease is associated with a high cd163/tweak plasma ratio. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Rull, A.; Garcia, R.; Fernandez-Sender, L.; Garcia-Heredia, A.; Aragones, G.; Beltran-Debon, R.; Marsillach, J.; Alegret, J.M.; Martin-Paredero, V.; Mackness, B.; et al. Serum paraoxonase-3 concentration is associated with insulin sensitivity in peripheral artery disease and with inflammation in coronary artery disease. Atherosclerosis 2012, 220, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, S.S.; Anzaldi, M.; Fiore, V.; Simili, M.; Puccia, G.; Libra, M.; Malaponte, G.; Neri, S. Patients with unrecognized peripheral arterial disease (PAD) assessed by ankle-brachial index (ABI) present a defined profile of proinflammatory markers compared to healthy subjects. Cytokine 2012, 59, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Catalano, M.; Cortelazzo, A.; Santi, R.; Contino, L.; Demicheli, M.; Yilmaz, Y.; Zorzetto, M.; Campo, I.; Lanati, N.; Emanuele, E. The Pro12Ala polymorphism of peroxisome proliferator-activated receptor-γ2 gene is associated with plasma levels of soluble rage (receptor for advanced glycation endproducts) and the presence of peripheral arterial disease. Clin. Biochem. 2008, 41, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Stehr, A.; Topel, I.; Muller, S.; Unverdorben, K.; Geissler, E.K.; Kasprzak, P.M.; Schlitt, H.J.; Steinbauer, M. Vegf: A surrogate marker for peripheral vascular disease. Eur. J. Vasc. Endovasc. Surg. 2010, 39, 330–332. [Google Scholar] [CrossRef] [PubMed]
- Findley, C.M.; Mitchell, R.G.; Duscha, B.D.; Annex, B.H.; Kontos, C.D. Plasma levels of soluble Tie2 and vascular endothelial growth factor distinguish critical limb ischemia from intermittent claudication in patients with peripheral arterial disease. J. Am. Coll. Cardiol. 2008, 52, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Smadja, D.M.; D’Audigier, C.; Bieche, I.; Evrard, S.; Mauge, L.; Dias, J.V.; Labreuche, J.; Laurendeau, I.; Marsac, B.; Dizier, B.; et al. Thrombospondin-1 is a plasmatic marker of peripheral arterial disease that modulates endothelial progenitor cell angiogenic properties. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Morishita, T.; Uzui, H.; Nakano, A.; Mitsuke, Y.; Geshi, T.; Ueda, T.; Lee, J.D. Number of endothelial progenitor cells in peripheral artery disease as a marker of severity and association with pentraxin-3, malondialdehyde-modified low-density lipoprotein and membrane type-1 matrix metalloproteinase. J. Atheroscler. Thromb. 2012, 19, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Delva, P.; de Marchi, S.; Prior, M.; Degan, M.; Lechi, A.; Trettene, M.; Arosio, E. Endothelial progenitor cells in patients with severe peripheral arterial disease. Endothelium 2008, 15, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Stampfer, M.J.; Rifai, N. Novel risk factors for systemic atherosclerosis: A comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein-a, and standard cholesterol screening as predictors of peripheral arterial disease. JAMA 2001, 285, 2481–2485. [Google Scholar] [CrossRef] [PubMed]
- Moxon, J.V.; Liu, D.; Wong, G.; Weir, J.M.; Behl-Gilhotra, R.; Bradshaw, B.; Kingwell, B.A.; Meikle, P.J.; Golledge, J. Comparison of the serum lipidome in patients with abdominal aortic aneurysm and peripheral artery disease. Circ. Cardiovasc. Genet. 2014, 7, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Gueant-Rodriguez, R.M.; Spada, R.; Moreno-Garcia, M.; Anello, G.; Bosco, P.; Lagrost, L.; Romano, A.; Elia, M.; Gueant, J.L. Homocysteine is a determinant of ApoA–I and both are associated with ankle brachial index, in an ambulatory elderly population. Atherosclerosis 2011, 214, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Homocysteine Lowering Trialists’ Collaboration. Lowering blood homocysteine with folic acid based supplements: Meta-analysis of randomised trials. BMJ, 1998; 316, 894–898. [Google Scholar]
- Group, V.T.S. The vitatops (vitamins to prevent stroke) trial: Rationale and design of an international, large, simple, randomised trial of homocysteine-lowering multivitamin therapy in patients with recent transient ischaemic attack or stroke. Cerebrovasc. Dis. 2002, 13, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Loland, K.H.; Bleie, O.; Blix, A.J.; Strand, E.; Ueland, P.M.; Refsum, H.; Ebbing, M.; Nordrehaug, J.E.; Nygard, O. Effect of homocysteine-lowering B vitamin treatment on angiographic progression of coronary artery disease: A western norway B vitamin intervention trial (wenbit) substudy. Am. J. Cardiol. 2010, 105, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Pasqualini, L.; Cortese, C.; Marchesi, S.; Siepi, D.; Pirro, M.; Vaudo, G.; Liberatoscioli, L.; Gnasso, A.; Schillaci, G.; Mannarino, E. Paraoxonase-1 activity modulates endothelial function in patients with peripheral arterial disease. Atherosclerosis 2005, 183, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.W.; Parker, D.E.; Montgomery, P.S.; Sosnowska, D.; Casanegra, A.I.; Ungvari, Z.; Csiszar, A.; Sonntag, W.E. Gender and racial differences in endothelial oxidative stress and inflammation in patients with symptomatic peripheral artery disease. J. Vasc. Surg. 2014. [Google Scholar] [CrossRef]
- Pipinos, II; Judge, A.R.; Zhu, Z.; Selsby, J.T.; Swanson, S.A.; Johanning, J.M.; Baxter, B.T.; Lynch, T.G.; Dodd, S.L. Mitochondrial defects and oxidative damage in patients with peripheral arterial disease. Free Radic. Biol. Med. 2006, 41, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.J.; Mackay, I.R.; Hill, A.; Jennings, P.; McCollum, P. Oxidative stress is present in atherosclerotic peripheral arterial disease and further increased by diabetes mellitus. Int. Angiol. 1995, 14, 385–388. [Google Scholar] [PubMed]
- Kals, J.; Kampus, P.; Kals, M.; Pulges, A.; Teesalu, R.; Zilmer, K.; Kullisaar, T.; Salum, T.; Eha, J.; Zilmer, M. Inflammation and oxidative stress are associated differently with endothelial function and arterial stiffness in healthy subjects and in patients with atherosclerosis. Scan. J. Clin. Lab. Investig. 2008, 68, 594–601. [Google Scholar] [CrossRef]
- Gliemann, L.; Nyberg, M.; Hellsten, Y. Nitric oxide and reactive oxygen species in limb vascular function: What is the effect of physical activity? Free Radic. Res. 2014, 48, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Casey, D.P.; Joyner, M.J. Local control of skeletal muscle blood flow during exercise: Influence of available oxygen. J. Appl. Physiol. 2011, 111, 1527–1538. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Pignatelli, P.; Cangemi, R.; Andreozzi, P.; Panico, M.A.; Meloni, V.; Violi, F. Imbalance between nitric oxide generation and oxidative stress in patients with peripheral arterial disease: Effect of an antioxidant treatment. J. Vasc. Surg. 2006, 44, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Boger, R.H.; Bode-Boger, S.M.; Thiele, W.; Junker, W.; Alexander, K.; Frolich, J.C. Biochemical evidence for impaired nitric oxide synthesis in patients with peripheral arterial occlusive disease. Circulation 1997, 95, 2068–2074. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.J.; Casale, G.P.; Koutakis, P.; Nella, A.A.; Swanson, S.A.; Zhu, Z.; Miserlis, D.; Johanning, J.M.; Pipinos, I.I. Oxidative damage and myofiber degeneration in the gastrocnemius of patients with peripheral arterial disease. J. Trans. Med. 2013, 11, 230. [Google Scholar] [CrossRef]
- Sen, S.; McDonald, S.P.; Coates, P.T.; Bonder, C.S. Endothelial progenitor cells: Novel biomarker and promising cell therapy for cardiovascular disease. Clin. Sci. 2011, 120, 263–283. [Google Scholar] [PubMed]
- Shinsato, T.; Miyata, M.; Kubozono, T.; Ikeda, Y.; Fujita, S.; Kuwahata, S.; Akasaki, Y.; Hamasaki, S.; Fujiwara, H.; Tei, C. Waon therapy mobilizes CD34+ cells and improves peripheral arterial disease. J. Cardiol. 2010, 56, 361–366. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Guralnik, J.M.; Corsi, A.; Albay, M.; Macchi, C.; Bandinelli, S.; Ferrucci, L. Patterns of inflammation associated with peripheral arterial disease: The inchianti study. Am. Heart J. 2005, 150, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Cassar, K.; Bachoo, P.; Ford, I.; Greaves, M.; Brittenden, J. Markers of coagulation activation, endothelial stimulation and inflammation in patients with peripheral arterial disease. Eur. J. Vasc. Endovasc. Surg. 2005, 29, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Owens, C.D.; Ridker, P.M.; Belkin, M.; Hamdan, A.D.; Pomposelli, F.; Logerfo, F.; Creager, M.A.; Conte, M.S. Elevated C-reactive protein levels are associated with postoperative events in patients undergoing lower extremity vein bypass surgery. J. Vasc. Surg. 2007, 45, 2–9, discussion 9. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Liu, K.; Ferrucci, L.; Tian, L.; Guralnik, J.M.; Green, D.; Tan, J.; Liao, Y.; Pearce, W.H.; Schneider, J.R.; et al. Circulating blood markers and functional impairment in peripheral arterial disease. J. Am. Geriatr. Soc. 2008, 56, 1504–1510. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Ferrucci, L.; Liu, K.; Criqui, M.H.; Greenland, P.; Green, D.; Guralnik, J.M.; Ridker, P.M.; Taylor, L.M.; Rifai, N.; et al. D-dimer and inflammatory markers as predictors of functional decline in men and women with and without peripheral arterial disease. J. Am. Geriatr. Soc. 2005, 53, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Owens, C.D.; Kim, J.M.; Hevelone, N.D.; Gasper, W.J.; Belkin, M.; Creager, M.A.; Conte, M.S. An integrated biochemical prediction model of all-cause mortality in patients undergoing lower extremity bypass surgery for advanced peripheral artery disease. J. Vasc. Surg. 2012, 56, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Stone, P.A.; Schlarb, H.; Campbell, J.E.; Williams, D.; Thompson, S.N.; John, M.; Campbell, J.R.; AbuRahma, A.F. C-reactive protein and brain natriuretic peptide as predictors of adverse events after lower extremity endovascular revascularization. J. Vasc. Surg. 2014, 60, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Kumada, Y.; Toriyama, T.; Aoyama, T.; Takahashi, H.; Murohara, T. Prognostic values of C-reactive protein levels on clinical outcome after endovascular therapy in hemodialysis patients with peripheral artery disease. J. Vasc. Surg. 2010, 52, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Van Wijk, D.F.; Boekholdt, S.M.; Wareham, N.J.; Ahmadi-Abhari, S.; Kastelein, J.J.; Stroes, E.S.; Khaw, K.T. C-reactive protein, fatal and nonfatal coronary artery disease, stroke, and peripheral artery disease in the prospective EPIC-norfolk cohort study. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2888–2894. [Google Scholar] [CrossRef] [PubMed]
- Grenon, S.M.; Chong, K.; Alley, H.; Nosova, E.; Gasper, W.; Hiramoto, J.; Boscardin, W.J.; Owens, C.D. Walking disability in patients with peripheral artery disease is associated with arterial endothelial function. J. Vasc. Surg. 2014, 59, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.H.; Chen, Y.S.; Shu, K.H.; Chang, H.R.; Chou, M.C. Higher serum levels of soluble intracellular cell adhesion molecule-1 and soluble vascular cell adhesion molecule predict peripheral artery disease in haemodialysis patients. Nephrology 2012, 17, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Haslacher, H.; Perkmann, T.; Gruenewald, J.; Exner, M.; Endler, G.; Scheichenberger, V.; Wagner, O.; Schillinger, M. Plasma myeloperoxidase level and peripheral arterial disease. Eur. J. Clin. Investig. 2012, 42, 463–469. [Google Scholar] [CrossRef]
- Gremmel, T.; Koppensteiner, R.; Ay, C.; Panzer, S. Residual thrombin generation potential is inversely linked to the occurrence of atherothrombotic events in patients with peripheral arterial disease. Eur. J. Clin. Investig. 2014, 44, 319–324. [Google Scholar] [CrossRef]
- Sheu, J.J.; Lin, P.Y.; Sung, P.H.; Chen, Y.C.; Leu, S.; Chen, Y.L.; Tsai, T.H.; Chai, H.T.; Chua, S.; Chang, H.W.; et al. Levels and values of lipoprotein-associated phospholipase A2, galectin-3, RhoA/ROCK, and endothelial progenitor cells in critical limb ischemia: Pharmaco-therapeutic role of cilostazol and clopidogrel combination therapy. J. Transl. Med. 2014, 12, 101. [Google Scholar] [CrossRef] [PubMed]
- Jouni, H.; Rodeheffer, R.J.; Kullo, I.J. Increased serum N-terminal pro-B-type natriuretic peptide levels in patients with medial arterial calcification and poorly compressible leg arteries. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Jouni, H.; Khaleghi, M.; Bailey, K.R.; Kullo, I.J. Serum N-terminal pro-B-type natriuretic peptide levels are associated with functional capacity in patients with peripheral arterial disease. Angiology 2012, 63, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, R.; Nakamura, K.; MacLauchlan, S.; Ngo, D.T.; Shimizu, I.; Fuster, J.J.; Katanasaka, Y.; Yoshida, S.; Qiu, Y.; Yamaguchi, T.P.; et al. An antiangiogenic isoform of VEGF-A contributes to impaired vascularization in peripheral artery disease. Nat. Med. 2014, 20, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Lloyd-Jones, D.M. The role of biomarkers and genetics in peripheral arterial disease. J. Am. Coll. Cardiol. 2009, 54, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Virginio, V.W.; Nunes, V.S.; Moura, F.A.; Menezes, F.H.; Andreollo, N.A.; Rogerio, F.; Scherrer, D.Z.; Quintao, E.C.; Nakandakare, E.; Petrucci, O.; et al. Arterial tissue and plasma concentration of enzymatic-driven oxysterols are associated with severe peripheral atherosclerotic disease and systemic inflammatory activity. Free Radic. Res. 2015, 49, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Owens, C.D.; Kim, J.M.; Hevelone, N.D.; Hamdan, A.; Raffetto, J.D.; Creager, M.A.; Conte, M.S. Novel adipokines, high molecular weight adiponectin and resistin, are associated with outcomes following lower extremity revascularization with autogenous vein. J. Vasc. Surg. 2010, 51, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Hewing, B.; Parathath, S.; Barrett, T.; Chung, W.K.; Astudillo, Y.M.; Hamada, T.; Ramkhelawon, B.; Tallant, T.C.; Yusufishaq, M.S.; Didonato, J.A.; et al. Effects of native and myeloperoxidase-modified apolipoprotein A–I on reverse cholesterol transport and atherosclerosis in mice. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Desikan, R.; Ying, Z.; Gushchina, L.; Kampfrath, T.; Deiuliis, J.; Wang, A.; Xu, X.; Zhong, J.; Rao, X.; et al. Effects of a novel pharmacologic inhibitor of myeloperoxidase in a mouse atherosclerosis model. PLoS ONE 2012, 7, e50767. [Google Scholar] [CrossRef] [PubMed]
- Van Kimmenade, R.R.; Januzzi, J.L., Jr. Emerging biomarkers in heart failure. Clin. Chem. 2012, 58, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Madrigal-Matute, J.; Lindholt, J.S.; Fernandez-Garcia, C.E.; Benito-Martin, A.; Burillo, E.; Zalba, G.; Beloqui, O.; Llamas-Granda, P.; Ortiz, A.; Egido, J.; et al. Galectin-3, a biomarker linking oxidative stress and inflammation with the clinical outcomes of patients with atherothrombosis. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [PubMed]
- Bachle, A.C.; Morsdorf, P.; Rezaeian, F.; Ong, M.F.; Harder, Y.; Menger, M.D. N-acetylcysteine attenuates leukocytic inflammation and microvascular perfusion failure in critically ischemic random pattern flaps. Microvasc. Res. 2011, 82, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Ozmen, S.; Ayhan, S.; Demir, Y.; Siemionow, M.; Atabay, K. Impact of gradual blood flow increase on ischaemia-reperfusion injury in the rat cremaster microcirculation model. J. Plast. Reconstr. Aesthet. Surg. 2008, 61, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Turton, E.P.; Coughlin, P.A.; Kester, R.C.; Scott, D.J. Exercise training reduces the acute inflammatory response associated with claudication. Eur. J. Vasc. Endovasc. Surg. 2002, 23, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Svensson, P.; de Faire, U.; Niklasson, U.; Hansson, L.O.; Ostergren, J. Plasma NT-probnp concentration is related to ambulatory pulse pressure in peripheral arterial disease. Blood Press. 2005, 14, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Mueller, T.; Dieplinger, B.; Poelz, W.; Endler, G.; Wagner, O.F.; Haltmayer, M. Amino-terminal pro-B-type natriuretic peptide as predictor of mortality in patients with symptomatic peripheral arterial disease: 5-Year follow-up data from the linz peripheral arterial disease study. Clin. Chem. 2009, 55, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Marz, W.; Tiran, B.; Seelhorst, U.; Wellnitz, B.; Bauersachs, J.; Winkelmann, B.R.; Boehm, B.O.; Team, L.S. N-terminal pro-B-type natriuretic peptide predicts total and cardiovascular mortality in individuals with or without stable coronary artery disease: The ludwigshafen risk and cardiovascular health study. Clin. Chem. 2007, 53, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Lehto, S.; Niskanen, L.; Suhonen, M.; Ronnemaa, T.; Laakso, M. Medial artery calcification. A neglected harbinger of cardiovascular complications in non-insulin-dependent diabetes mellitus. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Demer, L.L.; Tintut, Y. Vascular calcification: Pathobiology of a multifaceted disease. Circulation 2008, 117, 2938–2948. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, W.C.; Han, K.H.; Schneider, T.M.; Hennigar, R.A. Prevalence of nonatheromatous lesions in peripheral arterial disease. Arterioscler. Thromb. Vasc. Biol. 2014, 35, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Bleda, S.; de Haro, J.; Acin, F.; Varela, C.; Esparza, L. Enhanced vascular endothelial growth factor gene expression in ischaemic skin of critical limb ischaemia patients. Int. J. Vasc. Med. 2012, 2012, 691528. [Google Scholar] [PubMed]
- Jones, W.S.; Duscha, B.D.; Robbins, J.L.; Duggan, N.N.; Regensteiner, J.G.; Kraus, W.E.; Hiatt, W.R.; Dokun, A.O.; Annex, B.H. Alteration in angiogenic and anti-angiogenic forms of vascular endothelial growth factor-A in skeletal muscle of patients with intermittent claudication following exercise training. Vasc. Med. 2012, 17, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Ingber, D.E. Mechanical signaling and the cellular response to extracellular matrix in angiogenesis and cardiovascular physiology. Circ. Res. 2002, 91, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Silvestre, J.S.; Mallat, Z.; Tamarat, R.; Duriez, M.; Tedgui, A.; Levy, B.I. Regulation of matrix metalloproteinase activity in ischemic tissue by interleukin-10: Role in ischemia-induced angiogenesis. Circ. Res. 2001, 89, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, M.; Ishikawa, O. Hypoxic conditions decrease the mrna expression of proalpha1(I) and (III) collagens and increase matrix metalloproteinases-1 of dermal fibroblasts in three-dimensional cultures. J. Dermatol. Sci. 2000, 24, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Baum, O.; Ganster, M.; Baumgartner, I.; Nieselt, K.; Djonov, V. Basement membrane remodeling in skeletal muscles of patients with limb ischemia involves regulation of matrix metalloproteinases and tissue inhibitor of matrix metalloproteinases. J. Vasc. Res. 2007, 44, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Busti, C.; Falcinelli, E.; Momi, S.; Gresele, P. Matrix metalloproteinases and peripheral arterial disease. Intern. Emerg. Med. 2010, 5, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Gagne, P.J.; Tihonov, N.; Li, X.; Glaser, J.; Qiao, J.; Silberstein, M.; Yee, H.; Gagne, E.; Brooks, P. Temporal exposure of cryptic collagen epitopes within ischemic muscle during hindlimb reperfusion. Am. J. Pathol. 2005, 167, 1349–1359. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.H.; Chen, Y.H.; Wang, C.H.; Chen, J.S.; Tsai, H.Y.; Lin, F.Y.; Lo, W.Y.; Wu, T.C.; Sata, M.; Chen, J.W.; et al. Matrix metalloproteinase-9 is essential for ischemia-induced neovascularization by modulating bone marrow-derived endothelial progenitor cells. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- Szuba, A.; Oka, R.K.; Harada, R.; Cooke, J.P. Limb hemodynamics are not predictive of functional capacity in patients with pad. Vasc. Med. 2006, 11, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Modrall, J.G.; Parker, B.J.; Swann, A.; Welborn, M.B., 3rd; Anthony, T. Correlation between ankle-brachial index, symptoms, and health-related quality of life in patients with peripheral vascular disease. J. Vasc. Surg. 2004, 39, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.M.; Trollope, A.F.; Golledge, J. The relevance of epigenetics to occlusive cerebral and peripheral arterial disease. Clin. Sci. 2015, 128, 537–558. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krishna, S.M.; Moxon, J.V.; Golledge, J. A Review of the Pathophysiology and Potential Biomarkers for Peripheral Artery Disease. Int. J. Mol. Sci. 2015, 16, 11294-11322. https://doi.org/10.3390/ijms160511294
Krishna SM, Moxon JV, Golledge J. A Review of the Pathophysiology and Potential Biomarkers for Peripheral Artery Disease. International Journal of Molecular Sciences. 2015; 16(5):11294-11322. https://doi.org/10.3390/ijms160511294
Chicago/Turabian StyleKrishna, Smriti Murali, Joseph V. Moxon, and Jonathan Golledge. 2015. "A Review of the Pathophysiology and Potential Biomarkers for Peripheral Artery Disease" International Journal of Molecular Sciences 16, no. 5: 11294-11322. https://doi.org/10.3390/ijms160511294