
Effects of Global Warming on Patients with Dementia, Motor Neuron or Parkinson’s Diseases: A Comparison among Cortical and Subcortical Disorders
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Data Collection
- -
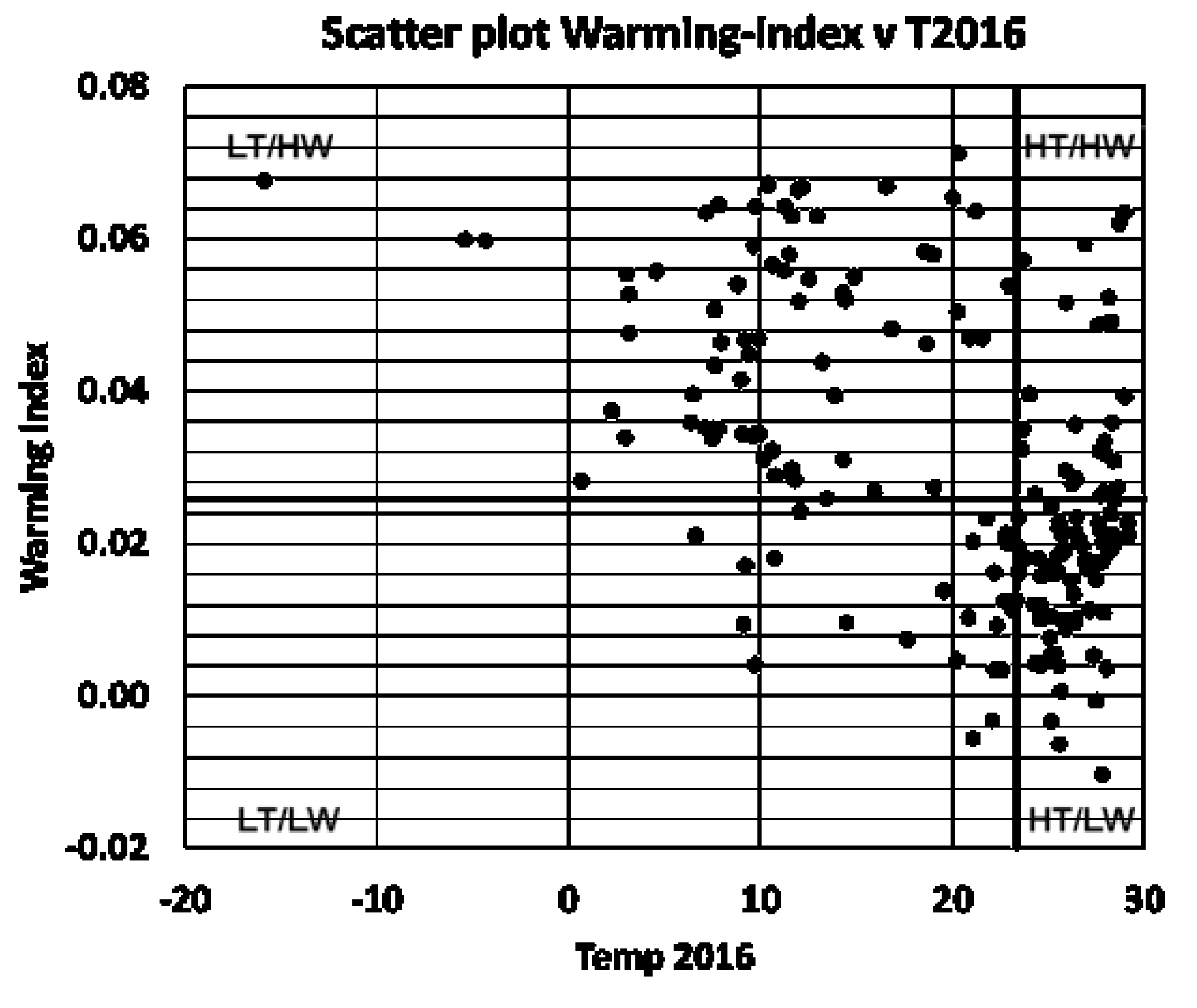
- The average temperature in 2016 (T2016) was computed as the annual mean 2 m temperature. The annual temperature in 2016 was used simply to cluster the countries in ‘warmer than the median’ or ‘colder than the median’ categories. Using the average temperature of 1990 (T1990) instead of T2016 would not change the conclusion of the work since a very small number of countries would move from one cluster to the other if T1990 was used instead of T2016. For each country, T2016 was computed as the average of the monthly temperatures of 2016 available in the data set:
- -
- The 1990–2016 warming index (WI1990–2016) can be seen in the slope of the linear regression curve, which fits the monthly 2 m temperature data from January 1990 to December 2016.
2.2. Subjects
2.3. Statistical Analyses
3. Results
3.1. Climate Indices
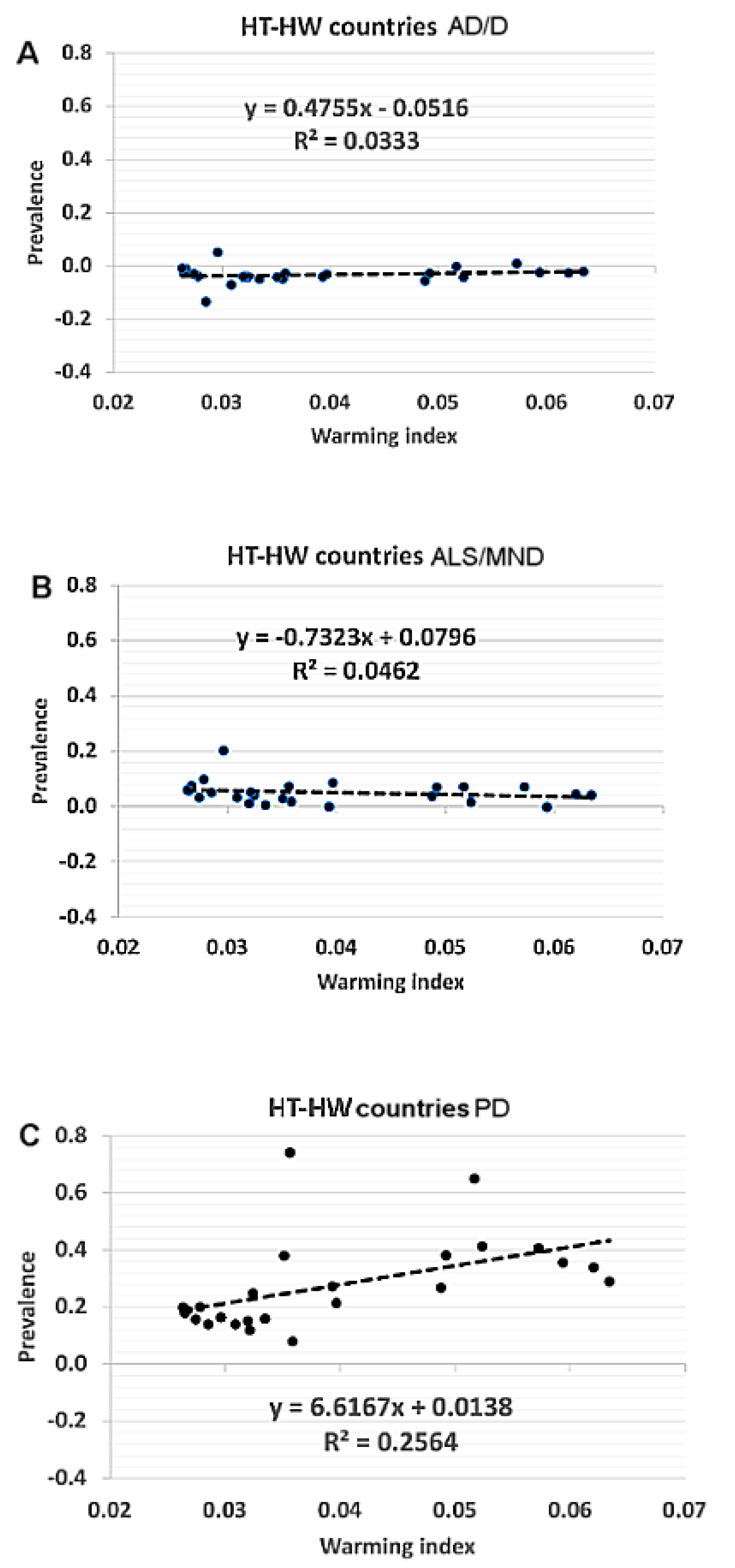
3.2. Epidemiological Indices Related to Country Clusters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Shukla, P.R.; Skea, J.; Slade, R.; Pathak, M.; Khourdajie, A.A.; van Diemen, R.; McCollum, D.; Abdulla, A.; Akimoto, K.; Babiker, M.; et al. IPCC: Summary for Policymakers. In Climate Change 2022: Mitigation of Climate Change. Contribution of Working Group III to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge UK; New York, NY, USA, 2022; Available online: https://www.ipcc.ch/report/sixth-assessment-report-working-group-3/ (accessed on 1 September 2021). [CrossRef]
- Butler, C. Climate change, health and existential risks to civilization: A comprehensive review (1989–2013). Int. J. Environ. Res. Public. Health 2018, 15, 2266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Bongioanni, P.; Del Carratore, R.; Corbianco, S.; Diana, A.; Cavallini, G.; Masciandaro, S.; Dini, M.; Buizza, R. Climate change and neurodegenerative diseases. Environ. Res. 2021, 201, 111511. [Google Scholar] [CrossRef] [PubMed]
- Amiri, M.; Peinkhofer, C.; Othman, M.H.; De Vecchi, T.; Nersesjan, V.; Kondziella, D. Global warming and neurological practice: Systematic review. PeerJ 2021, 9, e11941. [Google Scholar] [CrossRef]
- Farugia, T.L.; Cuni-Lopez, C.; White, A.R. Potential Impacts of Extreme Heat and Bushfires on Dementia. J. Alzheimers Dis. 2021, 79, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.G.; Kato, R.; Zhou, C.; Abdelhamid, M.; Shaaban, E.I.A.; Yamashita, H.; Michikawa, M. Sustained high body temperature exacerbates cognitive function and Alzheimer’s disease-related pathologies. Sci. Rep. 2022, 12, 12273. [Google Scholar] [CrossRef]
- Boopathy, L.A.; Jacob-Tomas, S.; Alecki, C.; Vera, M. Mechanisms tailoring the expression of heat shock proteins to proteostasis challenges. J. Biol. Chem. 2022, 298, 101796. [Google Scholar] [CrossRef]
- Shadfar, S.; Brocardo, M.; Atkin, J.D. The complex mechanisms by which neurons die following DNA damage in neurodegenerative diseases. Int.J. Mol. Sci. 2022, 23, 2484. [Google Scholar] [CrossRef]
- Buizza, R.; Del Carratore, R.; Bongioanni, P. Evidence of climate change impact on Parkinson’s disease. J. Clim. Chang. Health 2022, 6, 100130. [Google Scholar] [CrossRef]
- Nichols, E.; Szoeke, C.E.I.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Murray, C.J. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef] [Green Version]
- Logroscino, G.; Piccininni, M.; Marin, B.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Alahdab, F.; Asgedom, S.W.; Awasthi, A.; Chaiah, Y.; et al. Global, regional, and national burden of motor neuron diseases 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 1083–1097. [Google Scholar] [CrossRef] [Green Version]
- Dorsey, A.E.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.P.; Lee, C.T.C. Climatic factors associated with amyotrophic lateral sclerosis: A spatial analysis from Taiwan. Geospat. Health 2013, 8, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zammit, C.; Torzhenskaya, N.; Ozarkar, P.D.; Agius, J.C. Neurological disorders vis-a-vis climate change. Early Hum. Dev. 2021, 155, 105217. [Google Scholar] [CrossRef] [PubMed]
- Vasta, R.; Chia, R.; Traynor, B.J.; Chiò, A. Unraveling the complex interplay between genes, environment, and climate in ALS. EBioMedicine 2022, 75, 103795. [Google Scholar] [CrossRef]
- McMichael, C. Human mobility, climate change, and health: Unpacking the connections. Lancet Planet Health 2020, 4, e217–e218. [Google Scholar] [CrossRef]
- Okumiya, K.; Wada, T.; Fujisawa, M.; Ishine, M.; Garcia del Saz, E.; Hirata, Y.; Kuzuhara, S.; Kokubo, Y.; Seguchi, H.; Sakamoto, R.; et al. Amyotrophic lateral sclerosis and parkinsonism in Papua, Indonesia. 2001–2012 survey results. BMJ Open 2014, 4, e004353. [Google Scholar] [CrossRef] [Green Version]
- Eyer, G.C.; Di Santo, S.; Hewer, E.; Andereggen, L.; Seiler, S.; Widmer, H.R. Co-Expression of Nogo-A in dopaminergic neurons of the human substantia nigra pars compacta is reduced in Parkinson’s disease. Cells 2021, 10, 3368. [Google Scholar] [CrossRef]
- Chan, C.S.; Gertler, T.S.; Surmeier, D. A molecular basis for the increased vulnerability of substantia nigra dopamine neurons in aging and Parkinson’s disease: Vulnerability of DA Neurons. Mov. Disord. 2010, 25, S63–S70. [Google Scholar] [CrossRef]
- Ortner, N.J.; Bock, G.; Dougalis, A.; Kharitonova, M.; Duda, J.; Hess, S.; Tuluc, P.; Pomberger, T.; Stefanova, N.; Pitterl, F.; et al. Lower affinity of isradipine for L-Type Ca2+ channels during substantia nigra dopamine neuron-like activity: Implications for neuroprotection in Parkinson’s disease. J. Neurosci. 2017, 37, 6761–6777. [Google Scholar] [CrossRef] [Green Version]
- Pissadaki, E.K.; Bolam, J.P. The energy cost of action potential propagation in dopamine neurons: Clues to susceptibility in Parkinson’s disease. Front. Comput. Neurosci. 2013, 18, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surmeier, D.J.; Obeso, J.A.; Halliday, G.M. Selective neuronal vulnerability in Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 101–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, G.; Reyes, P.F.; Golden, G.T.; Randall, L.; Woltjer, C.H.; Montine, T.J.; Zhang, J. Mitochondrial DNA deletions/rearrangements in Parkinson disease and related neurodegenerative disorders. J. Neuropathol. Exp. Neurol. 2002, 61, 634–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrer, I.; Perez, E.; Dalfo, E.; Barrachina, M. Abnormal levels of prohibitin and ATP synthase in the substantia nigra and frontal cortex in Parkinson’s disease. Neurosci. Lett. 2007, 415, 205–209. [Google Scholar] [CrossRef]
- González-Hernández, T.; Cruz-Muros, I.; Afonso-Oramas, D.; Salas-Hernandez, J.; Castro-Hernandez, J. Vulnerability of mesostriatal dopaminergic neurons in Parkinson’s disease. Front. Neuroanat. 2010, 4, 140. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.; Li, Y. Association of autonomic symptoms with cerebrospinal fluid biomarkers in Parkinson disease and scans without evidence of dopaminergic deficit. Medicine 2021, 100, e24837. [Google Scholar] [CrossRef]
- Contreras, C.; Nogueiras, R.; Diéguez, C.; Medina-Gómez, G.; López, M. Hypothalamus and thermogenesis: Heating the BAT, browning the WAT. Mol. Cell Endocrinol. 2016, 438, 107–115. [Google Scholar] [CrossRef]
- Feldmann, H.M.; Golozoubova, V.; Cannon, B.; Nedergaard, J. UCP1 ablation induces obesity and abolishes diet-induced thermogenesis in mice exempt from thermal stress by living at thermoneutrality. Cell Metab. 2009, 9, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Meng, X.; Yang, C.; Fang, D.; Wang, X.; An, J.; Zhang, J.; Wang, L.; Lu, T.; Ruan, H.-B.; et al. Brown adipose tissue activation in a rat model of Parkinson’s disease. Am. J. Physiol-Endocrinol. Metab. 2017, 313, e731–e736. [Google Scholar] [CrossRef]
- Lian, H.; Zhou, L.; Zhang, Y.; Song, Y.H.; Zhang, Y.M.; Zheng, H.C.; Wang, Z.Y. Increased energy expenditure and activated Β3-AR-CAMP-PKA signaling pathway in the interscapular brown adipose tissue of 6-OHDA -induced Parkinson’s disease model rats. Anat. Rec. 2020, 304, 704–713. [Google Scholar] [CrossRef]
- Collins, S. β-adrenoceptor signaling networks in adipocytes for recruiting stored fat and energy expenditure. Front. Endocrinol. 2012, 2, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yong, V.W.; Tan, Y.J.; Ng, Y.D.; Choo, X.Y.; Sugumaran, K.; Chinna, K.; Shah, M.N.D.; Aman, R.R.A.R.; Moy, F.M.; Ramli, N.M.; et al. Progressive and accelerated weight and body fat loss in Parkinson’s disease: A three-year prospective longitudinal study. Park. Relat. Disord. 2020, 77, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Tournissac, M.; Leclerc, M.; Valentin-Escalera, J.; Vandal, M.; Bosoi, C.R.; Planel, E.; Calon, F. Metabolic determinants of Alzheimer’s disease: A focus on thermoregulation. Ageing Res. Rev. 2021, 72, 101462. [Google Scholar] [CrossRef] [PubMed]
- Di Micco, J.A.; Zaretsky, D.V. The dorsomedial hypothalamus: A new player in thermoregulation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 292, R47–R63. [Google Scholar] [CrossRef] [Green Version]
- Politis, M.; Piccini, P.; Pavese, N.; Koh, S.B.; Brooks, D.J. Evidence of dopamine dysfunction in the hypothalamus of patients with Parkinson’s disease: An in vivo 11C-raclopride PET study. Exp. Neurol. 2018, 214, 112–116. [Google Scholar] [CrossRef]
- Vercruysse, P.; Vieau, D.; Blum, D.; Petersén, Å.; Dupuis, L. Hypothalamic alterations in neurodegenerative diseases and their relation to abnormal energy metabolism. Front. Mol. Neurosci. 2018, 11, 2. [Google Scholar] [CrossRef] [Green Version]
- Claflin, K.E.; Flippo, K.H.; Sullivan, A.I.; Meghan, C.; BoluZhou, N.; Neff, T.J.; Jensen-Cody, S.O.; Potthoff, M.J. Conditional gene targeting using UCP1-Cre mice directly targets the central nervous system beyond thermogenic adipose tissues. Mol. Metab. 2022, 55, 101405. [Google Scholar] [CrossRef]
- Mendoza-Velásquez, J.J.; Flores-Vázquez, J.F.; Barrón-Velázquez, E.; Sosa-Ortiz, A.L.; Illigens, B.M.W.; Siepmann, T. Autonomic dysfunction in α-synucleinopathies. Front. Neurol. 2019, 10, 363. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prevalence | HT-LW | HT-HW | LT-HW | LT-LW |
|---|---|---|---|---|
| AD/D | −0.031 | −0.031 | −0.016 | −0.040 |
| ALS/MND | 0.062 | 0.044 | 0.065 | 0.071 |
| PD | 0.152 | 0.215 | 0.122 | 0.157 |
| (A) AD/D Prevalence | HT-HW | HT-LW | LT-HW | LT-LW |
|---|---|---|---|---|
| HT-HW | 100.0% | 35.5% | 81.0% | 6.4% |
| HT-LW | 100.0% | 63.4% | 0.1% | |
| LT-HW | 100.0% | 11.3% | ||
| LT-LW | 100.0% | |||
| (B) ALS/MND Prevalence | HT-HW | HT-LW | LT-HW | LT-LW |
| HT-HW | 100.0% | 8.2% | 0.8% | 0.5% |
| HT-LW | 100.0% | 0.3% | 0.3% | |
| LT-HW | 100.0% | 88.8% | ||
| LT-LW | 100.0% | |||
| (C) PD Prevalence | HT-HW | HT-LW | LT-HW | LT-LW |
| HT-HW | 100.0% | 0.0% | 4.1% | 0.1% |
| HT-LW | 100.0% | 86.7% | 13.3% | |
| LT-HW | 100.0% | 47.0% | ||
| LT-LW | 100.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bongioanni, P.; Del Carratore, R.; Dolciotti, C.; Diana, A.; Buizza, R. Effects of Global Warming on Patients with Dementia, Motor Neuron or Parkinson’s Diseases: A Comparison among Cortical and Subcortical Disorders. Int. J. Environ. Res. Public Health 2022, 19, 13429. https://doi.org/10.3390/ijerph192013429
Bongioanni P, Del Carratore R, Dolciotti C, Diana A, Buizza R. Effects of Global Warming on Patients with Dementia, Motor Neuron or Parkinson’s Diseases: A Comparison among Cortical and Subcortical Disorders. International Journal of Environmental Research and Public Health. 2022; 19(20):13429. https://doi.org/10.3390/ijerph192013429
Chicago/Turabian StyleBongioanni, Paolo, Renata Del Carratore, Cristina Dolciotti, Andrea Diana, and Roberto Buizza. 2022. "Effects of Global Warming on Patients with Dementia, Motor Neuron or Parkinson’s Diseases: A Comparison among Cortical and Subcortical Disorders" International Journal of Environmental Research and Public Health 19, no. 20: 13429. https://doi.org/10.3390/ijerph192013429