
Effect of Elevated Ambient Temperature on Maternal, Foetal, and Neonatal Outcomes: A Scoping Review



Abstract
:1. Introduction
- (1)
- What are the magnitude, characteristics, and trends of research on elevated ambient temperature and maternal, foetal, and neonatal outcomes?
- (2)
- What adverse maternal, foetal, and neonatal outcomes are being explored by research for their relationships with elevated ambient temperature; what are the findings?
- (3)
- What gestational periods are particularly susceptible to elevated ambient temperatures during pregnancy?
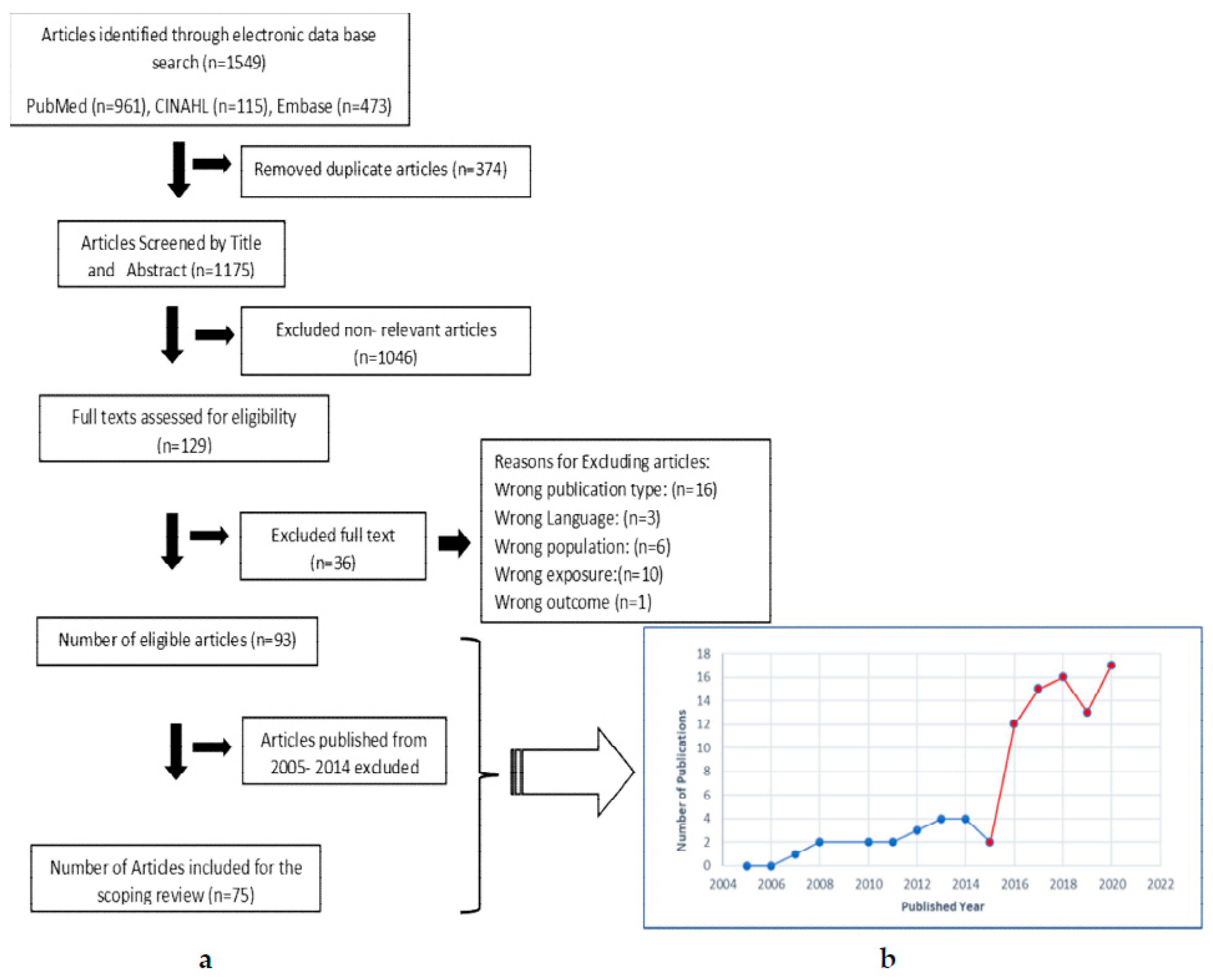
2. Materials and Methods
2.1. Search Strategies
2.2. Inclusion/Exclusion Criteria and Identification of Relevant Studies
2.2.1. Inclusion Criteria
- Studies that included pregnant women and/or neonates in the study population;
- Studies that directly addressed the relationship between elevated ambient temperatures (e.g., heatwave, extreme temperature, various high ambient temperatures), and pregnancy and birth outcomes in any stage of pregnancy;
- Studies that examined one or more maternal, foetal, or neonatal outcomes;
- Original research studies published in the English language;
- All types of study designs;
- Articles published between January 2005–November 2020 (the initial collection of articles generated using this time frame).
2.2.2. Exclusion Criteria
- Studies that did not include pregnant women or neonates in the study population;
- Studies that showed associations between other indicators of climate change or heat sources such as hot baths, saunas, or experimental temperatures;
- Studies that did not examine adverse maternal, foetal, or neonatal health outcomes;
- Reviews and grey literature;
- Articles published in languages other than English language;
- Articles published before 2005.
2.3. Data Extraction
3. Results
3.1. The Magnitude, Characteristics, and Trends of Research on Elevated Ambient Temperature and Maternal, Foetal, and Neonatal Outcomes
3.2. Relationships between Elevated Ambient Temperature and Maternal, Foetal, and Neonatal Outcomes
3.2.1. Elevated Ambient Temperature-Associated Adverse Neonatal Outcomes
Preterm Birth (PTB)
Low Birth Weight (LBW)
Stillbirth
Neonatal Mortality
Neonatal Morbidity
Small for Gestational Age (SGA)
International Normalised Ratio (INR) of Neonates
Newborn Telomere Length
3.2.2. Elevated Ambient Temperature-Associated Adverse Foetal Outcomes
Congenital Anomalies
Reduced Placental Weight and Volume
Miscarriage
3.2.3. Elevated Ambient Temperature-Associated Adverse Maternal Outcomes
Gestational Diabetes Mellitus (GDM)
Hypertensive Disorders
Premature Rupture of Membrane (PROM)
Placental Abruption
Maternal Stress
Cardiovascular Risk at Labour
Bacteriuria
3.3. Elevated Temperature Exposure and Suceptible Gestational Periods
4. Discussion
4.1. Principal Findings
- (i)
- Eight types of adverse neonatal outcomes (PTB, LBW, stillbirth, neonatal mortality, neonatal morbidity, SGA, newborn telomere length, and newborn INR levels).
- (ii)
- Three types of adverse foetal outcomes (congenital anomalies, reduced placental weight and volume and miscarriages), and
- (iii)
- Seven types of adverse maternal outcomes (GDM, hypertensive disorders in pregnancy, placental abruption, PROM, cardiovascular events at labour, bacteriuria, and maternal stress).
4.2. Gaps and Recommendations for Future Research
4.3. Limitations of the Scoping Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Exposure Window | Number of Studies |
|---|---|
| Same day (Lag 0) | 18 |
| 1 day before the case (Lag 0–1) | 12 |
| 2 days before the case (Lag 0–2) | 14 |
| 3 days before the case (Lag 0–3) | 11 |
| 4 days before the case (Lag 0–4) | 11 |
| 5 days before the case (Lag 0–5) | 10 |
| 6days before the case (Lag 0–6) | 10 |
| Last week of pregnancy (Lag 0–7) | 21 |
| 2 weeks before delivery (Lag 0–14) | 4 |
| 3 weeks before delivery (0–21) | 3 |
| Last month of pregnancy (lag 0–28) | 16 |
| 1st trimester | 22 |
| 2nd trimester | 23 |
| 3rd trimester | 21 |
| Entire pregnancy | 19 |
| Pre–conception(3 months prior to LMP) | 8 |
| 1month prior to LMP | 1 |
| Conception date | 1 |
| 0–8 weeks of pregnancy | 1 |
| Week 1 (0–7days) of gestation | 2 |
| Weeks 2–8 | 1 |
| Weeks 3–4 | 1 |
| Weeks 3–8 | 2 |
| Weeks 8–14 | 1 |
| 1st month of gestation | 6 |
| 2nd month of gestation | 2 |
| 3rd month of gestation | 2 |
| Gestation week 20 to birth | 1 |
| 0–36 weeks | 2 |
| Gestation week 22–26 | 1 |
| Gestation week 27–29 | 1 |
| Gestation week 30–32 | 1 |
| Gestation week 33–35 | 1 |
| Gestation week 36 | 1 |
| Gestation week 37–38 | 1 |
| Gestation week 39–43 | 1 |
| 0–28days after birth | 3 |
| Not stated | 1 |
References
- Romanello, M.; McGushin, A.; Di Napoli, C.; Drummond, P.; Hughes, N.; Jamart, L.; Kennard, H.; Lampard, P.; Rodriguez, B.S.; Arnell, N.; et al. The 2021 Report of the Lancet Countdown on Health and Climate Change: Code Red for a Healthy Future. Lancet 2021, 398, 1619–1662. [Google Scholar] [CrossRef]
- WHO. COP26 Special Report on Climate Change and Health: The Health Argument for Climate Action; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Perkins-Kirkpatrick, S.E.; Lewis, S.C. Increasing Trends in Regional Heatwaves. Nat. Commun. 2020, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chambers, J. Global and Cross-Country Analysis of Exposure of Vulnerable Populations to Heatwaves from 1980 to 2018. Clim. Chang. 2020, 163, 539–558. [Google Scholar] [CrossRef]
- Åström, D.O.; Schifano, P.; Asta, F.; Lallo, A.; Michelozzi, P.; Rocklöv, J.; Forsberg, B. The Effect of Heat Waves on Mortality in Susceptible Groups: A Cohort Study of a Mediterranean and a Northern European City. Environ. Health 2015, 14, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cil, G.; Cameron, T.A. Potential Climate Change Health Risks from Increases in Heat Waves: Abnormal Birth Outcomes and Adverse Maternal Health Conditions. Risk Anal. 2017, 37, 2066–2079. [Google Scholar] [CrossRef]
- Xu, Z.; Sheffield, P.E.; Su, H.; Wang, X.; Bi, Y.; Tong, S. The Impact of Heat Waves on Children’s Health: A Systematic Review. Int. J. Biometeorol. 2014, 58, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Agay-Shay, K.; Friger, M.; Linn, S.; Peled, A.; Amitai, Y.; Peretz, C. Ambient Temperature and Congenital Heart Defects. Hum. Reprod. 2013, 28, 2289–2297. [Google Scholar] [CrossRef] [Green Version]
- Strand, L.B.; Barnett, A.G.; Tong, S. The Influence of Season and Ambient Temperature on Birth Outcomes: A Review of the Epidemiological Literature. Environ. Res. 2011, 111, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Poeran, J.; Birnie, E.; Steegers, E.A.P.; Bonsel, G.J. The Impact of Extremes in Outdoor Temperature and Sunshine Exposure on Birth Weight. J. Environ. Health 2016, 78, 92–101. [Google Scholar]
- Asta, F.; Michelozzi, P.; Cesaroni, G.; De Sario, M.; Badaloni, C.; Davoli, M.; Schifano, P. The Modifying Role of Socioeconomic Position and Greenness on the Short-Term Effect of Heat and Air Pollution on Preterm Births in Rome, 2001–2013. Int. J. Environ. Res. Public Health 2019, 16, 2497. [Google Scholar] [CrossRef] [Green Version]
- Gronlund, C.J.; Yang, A.J.; Conlon, K.C.; Bergmans, R.S.; Le, H.Q.; Batterman, S.A.; Wahl, R.L.; Cameron, L.; O’Neill, M.S. Time Series Analysis of Total and Direct Associations between High Temperatures and Preterm Births in Detroit, Michigan. BMJ Open 2020, 10, e032476. [Google Scholar] [CrossRef]
- Li, S.; Wang, J.; Xu, Z.; Wang, X.; Xu, G.; Zhang, J.; Shen, X.; Tong, S. Exploring Associations of Maternal Exposure to Ambient Temperature with Duration of Gestation and Birth Weight: A Prospective Study. BMC Pregnancy Childbirth 2018, 18, 513. [Google Scholar] [CrossRef]
- Auger, N.; Fraser, W.D.; Arbour, L.; Bilodeau-Bertrand, M.; Kosatsky, T. Elevated Ambient Temperatures and Risk of Neural Tube Defects. Occup. Environ. Med. 2017, 74, 315–320. [Google Scholar] [CrossRef]
- Ha, S.; Liu, D.; Zhu, Y.; Kim, S.S.; Sherman, S.; Grantz, K.L.; Mendola, P. Ambient Temperature and Stillbirth: A Multi-Center Retrospective Cohort Study. Environ. Health Perspect. 2017, 125, 067011. [Google Scholar] [CrossRef] [PubMed]
- Chiefari, E.; Pastore, I.; Puccio, L.; Caroleo, P.; Oliverio, R.; Vero, A.; Foti, D.P.; Vero, R.; Brunetti, A. Impact of Seasonality on Gestational Diabetes Mellitus. Endocr. Metab. Immune Disord. Drug Targets 2017, 17, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, A.; Claesson, R.; Ignell, C.; Shaat, N.; Berntorp, K. Seasonal Pattern in the Diagnosis of Gestational Diabetes Mellitus in Southern Sweden. J. Diabetes Res. 2016, 2016, 1–6. [Google Scholar] [CrossRef]
- Retnakaran, R.; Ye, C.; Kramer, C.K.; Hanley, A.J.; Connelly, P.W.; Sermer, M.; Zinman, B. Impact of Daily Incremental Change in Environmental Temperature on Beta Cell Function and the Risk of Gestational Diabetes in Pregnant Women. Diabetologia 2018, 61, 2633–2642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, T.; Chen, P.; Mu, Y.; Li, X.; Di, B.; Li, J.; Qu, Y.; Tang, J.; Liang, J.; Mu, D. Association between Ambient Temperature and Hypertensive Disorders in Pregnancy in China. Nat. Commun. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Chersich, M.F.; Pham, M.D.; Areal, A.; Haghighi, M.M.; Manyuchi, A.; Swift, C.P.; Wernecke, B.; Robinson, M.; Hetem, R.; Boeckmann, M.; et al. Associations between High Temperatures in Pregnancy and Risk of Preterm Birth, Low Birth Weight, and Stillbirths: Systematic Review and Meta-Analysis. BMJ 2020, 371, m3811. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, C.; Wang, L. Temperature Exposure during Pregnancy and Birth Outcomes: An Updated Systematic Review of Epidemiological Evidence. Environ. Pollut. 2017, 225, 700–712. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Chou, D.; Oestergaard, M.; Say, L.; Moller, A.-B.; Kinney, M.; Lawn, J.; The Born Too Soon Preterm Birth Action Group. Born Too Soon: The Global Epidemiology of 15 Million Preterm Births. Reprod. Health 2013, 10 (Suppl. 1), S2. [Google Scholar] [CrossRef] [Green Version]
- Walani, S.R. Global Burden of Preterm birth. Int. J. Gynecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- World Health Organization. News: Preterm Birth. Available online: http://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 1 December 2018).
- WHO. Global Nutrition Targets 2025: Low Birth Weight Policy Brief; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Hug, L.; You, D.; Blencowe, H.; Mishra, A.; Wang, Z.; Fix, M.J.; Wakefield, J.; Moran, A.C.; Gaigbe-Togbe, V.; Suzuki, E.; et al. Global, Regional, and National Estimates and Trends in Stillbirths from 2000 to 2019: A Systematic Assessment. Lancet 2021, 398, 772–785. [Google Scholar] [CrossRef]
- Bekkar, B.; Pacheco, S.; Basu, R.; DeNicola, N. Association of Air Pollution and Heat Exposure with Preterm Birth, Low Birth Weight, and Stillbirth in the US. JAMA Netw. Open 2020, 3, e208243. [Google Scholar] [CrossRef] [PubMed]
- Carolan-Olah, M.; Frankowska, D. High Environmental Temperature and Preterm Birth: A Review of the Evidence. Midwifery 2014, 30, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Sexton, J.; Andrews, C.; Carruthers, S.; Kumar, S.; Flenady, V.; Lieske, S. Systematic Review of Ambient Temperature Exposure during Pregnancy and Stillbirth: Methods and Evidence. Environ. Res. 2021, 197, 111037. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- World Bank Data Help Desk. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 20 December 2021).
- Mohammadi, D.; Naghshineh, E.; Sarsangi, A.; Sakhvidi, M.J.Z. Environmental Extreme Temperature and Daily Preterm Birth in Sabzevar, Iran: A Time-Series Analysis. Environ. Health Prev. Med. 2019, 24, 5. [Google Scholar] [CrossRef]
- Schifano, P.; Asta, F.; Dadvand, P.; Davoli, M.; Basagana, X.; Michelozzi, P. Heat and Air Pollution Exposure as Triggers of Delivery: A Survival Analysis of Population-Based Pregnancy Cohorts in Rome and Barcelona. Environ. Int. 2016, 88, 153–159. [Google Scholar] [CrossRef]
- Basu, R.; Pearson, D.; Sie, L.; Broadwin, R. A Case-Crossover Study of Temperature and Infant Mortality in California. Paediatr. Perinat. Epidemiol. 2015, 29, 407–415. [Google Scholar] [CrossRef]
- Basu, R.; Rau, R.; Pearson, D.; Malig, B. Temperature and Term Low Birth Weight in California. Am. J. Epidemiol. 2018, 187, 2306–2314. [Google Scholar] [CrossRef]
- Basu, R.; Sarovar, V.; Malig, B.J. Association between High Ambient Temperature and Risk of Stillbirth in California. Am. J. Epidemiol. 2016, 183, 894–901. [Google Scholar] [CrossRef]
- Rammah, A.; Whitworth, K.W.; Han, I.; Chan, W.; Hess, J.W.; Symanski, E. Temperature, Placental Abruption and Stillbirth. Environ. Int. 2019, 131, 105067. [Google Scholar] [CrossRef]
- Soim, A.; Sheridan, S.C.; Hwang, S.; Hsu, W.; Fisher, S.C.; Shaw, G.M.; Feldkamp, M.L.; Romitti, P.A.; Reefhuis, J.; Langlois, P.H.; et al. A Population-Based Case-Control Study of the Association between Weather-Related Extreme Heat Events and Orofacial Clefts. Birth Defects Res. 2018, 110, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Diaz, J.; Ortiz, C.; Carmona, R.; Sáez, M.; Linares, C. Short Term Effect of Air Pollution, Noise and Heat Waves on Preterm Births in Madrid (Spain). Environ. Res. 2016, 145, 162–168. [Google Scholar] [CrossRef]
- Ilango, S.D.; Weaver, M.; Sheridan, P.; Schwarz, L.; Clemesha, R.E.; Bruckner, T.; Basu, R.; Gershunov, A.; Benmarhnia, T. Extreme Heat Episodes and Risk of Preterm Birth in California, 2005–2013. Environ. Int. 2020, 137, 105541. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, W.R.; Soim, A.; Zhang, W.; Lin, Z.; Lu, Y.; Lipton, E.A.; Xiao, J.; Dong, G.-H.; Lin, S. A Population-Based Case–Control Study of the Association between Weather-Related Extreme Heat Events and Low Birthweight. J. Dev. Orig. Health Dis. 2021, 12, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Lin, Z.; Ou, Y.; Soim, A.; Shrestha, S.; Lu, Y.; Sheridan, S.; Luben, T.J.; Fitzgerald, E.; Bell, E. Maternal Ambient Heat Exposure during Early Pregnancy in Summer and Spring and Congenital Heart Defects—A Large US Population-Based, Case-Control Study. Environ. Int. 2018, 118, 211–221. [Google Scholar] [CrossRef]
- Mathew, S.; Mathur, D.; Chang, A.B.; McDonald, E.; Singh, G.R.; Nur, D.; Gerritsen, R. Examining the Effects of Ambient Temperature on Pre-Term Birth in Central Australia. Int. J. Environ. Res. Public Health 2017, 14, 147. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.L.; Hardeman, R.R. Association of Summer Heat Waves and the Probability of Preterm Birth in Minnesota: An Exploration of the Intersection of Race and Education. Int. J. Environ. Res. Public Health 2020, 17, 6391. [Google Scholar] [CrossRef]
- Wang, J.; Tong, S.; Williams, G.; Pan, X. Exposure to Heat Wave during Pregnancy and Adverse Birth Outcomes: An Exploration of Susceptible Windows. Epidemiology 2019, 30, S115–S121. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Li, B.; Benmarhnia, T.; Hajat, S.; Ren, M.; Liu, T.; Knibbs, L.D.; Zhang, H.; Bao, J.; Zhang, Y.; et al. Independent and Combined Effects of Heatwaves and PM2.5 on Preterm Birth in Guangzhou, China: A Survival Analysis. Environ. Health Perspect. 2020, 128, 017006. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Spero, T.L.; Nolte, C.G.; Garcia, V.C.; Lin, Z.; Romitti, P.A.; Shaw, G.M.; Sheridan, S.C.; Feldkamp, M.L.; Woomert, A.; et al. Projected Changes in Maternal Heat Exposure During Early Pregnancy and the Associated Congenital Heart Defect Burden in the United States. J. Am. Heart Assoc. 2019, 8, e010995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auger, N.; Fraser, W.D.; Sauve, R.; Bilodeau-Bertrand, M.; Kosatsky, T. Risk of Congenital Heart Defects after Ambient Heat Exposure Early in Pregnancy. Environ. Health Perspect. 2017, 125, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Auger, N.; Fraser, W.D.; Smargiassi, A.; Bilodeau-Bertrand, M.; Kosatsky, T. Elevated Outdoor Temperatures and Risk of Stillbirth. Int. J. Epidemiol. 2016, 46, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Cox, B.; Vicedo-Cabrera, A.M.; Gasparrini, A.; Roels, H.A.; Martens, E.; Vangronsveld, J.; Forsberg, B.; Nawrot, T.S. Ambient Temperature as a Trigger of Preterm Delivery in a Temperate Climate. J. Epidemiol. Commun. Health 2016, 70, 1191–1199. [Google Scholar] [CrossRef] [Green Version]
- Iijima, S.; Sekii, K.; Baba, T.; Ueno, D.; Ohishi, A. Seasonal Variation in the International Normalized Ratio of Neonates and Its Relationship with Ambient Temperature. BMC Pediatr. 2016, 16, 97. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Chen, G.; Jaakkola, J.J.; Williams, G.; Guo, Y. Temporal Change in the Impacts of Ambient Temperature on Preterm Birth and Stillbirth: Brisbane, 1994–2013. Sci. Total Environ. 2018, 634, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, W.; Xu, J.; Luo, Z.; Ye, X.; Yan, C.; Liu, Z.; Tong, S. Association between Temperature and Maternal Stress during Pregnancy. Environ. Res. 2017, 158, 421–430. [Google Scholar] [CrossRef]
- Molina-Vega, M.; Gutiérrez-Repiso, C.; Muñoz-Garach, A.; Lima-Rubio, F.; Morcillo, S.; Tinahones, F.J.; Picón-César, M.J. Relationship between Environmental Temperature and the Diagnosis and Treatment of Gestational Diabetes Mellitus: An Observational Retrospective Study. Sci. Total Environ. 2020, 744, 140994. [Google Scholar] [CrossRef]
- Ngo, N.S.; Horton, R. Climate Change and Fetal Health: The Impacts of Exposure to Extreme Temperatures in New York City. Environ. Res. 2016, 144, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Ranjbaran, M.; Mohammadi, R.; Yaseri, M.; Kamari, M.; Yazdani, K. Ambient Temperature and Air Pollution, and the Risk of Preterm Birth in Tehran, Iran: A Time Series Study. J. Matern. Neonatal Med. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vicedo-Cabrera, A.M.; Olsson, D.; Forsberg, B. Exposure to Seasonal Temperatures during the Last Month of Gestation and the Risk of Preterm Birth in Stockholm. Int. J. Environ. Res. Public Health 2015, 12, 3962–3978. [Google Scholar] [CrossRef] [Green Version]
- Walfisch, A.; Kabakov, E.; Friger, M.; Sheiner, E. Trends, Seasonality and Effect of Ambient Temperature on Preterm Delivery. J. Matern. Fetal Neonatal Med. 2017, 30, 2483–2487. [Google Scholar] [CrossRef] [PubMed]
- Ward, A.; Clark, J.; McLeod, J.; Woodul, R.; Moser, H.; Konrad, C. The Impact of Heat Exposure on Reduced Gestational Age in Pregnant Women in North Carolina, 2011–2015. Int. J. Biometeorol. 2019, 63, 1611–1620. [Google Scholar] [CrossRef] [PubMed]
- Booth, G.L.; Luo, J.; Park, A.L.; Feig, D.S.; Moineddin, R.; Ray, J.G. Influence of Environmental Temperature on Risk of Gestational Diabetes. Can. Med Assoc. J. 2017, 189, E682–E689. [Google Scholar] [CrossRef] [Green Version]
- Guo, T.; Wang, Y.; Zhang, H.; Zhang, Y.; Zhao, J.; Wang, Y.; Xie, X.; Wang, L.; Zhang, Q.; Liu, D.; et al. The Association between Ambient Temperature and the Risk of Preterm Birth in China. Sci. Total Environ. 2018, 613–614, 439–446. [Google Scholar] [CrossRef]
- Ha, S.; Nguyen, K.; Liu, D.; Männistö, T.; Nobles, C.; Sherman, S.; Mendola, P. Ambient Temperature and Risk of Cardiovascular Events at Labor and Delivery: A Case-Crossover Study. Environ. Res. 2017, 159, 622–628. [Google Scholar] [CrossRef]
- Ha, S.; Liu, D.; Zhu, Y.; Kim, S.S.; Sherman, S.; Mendola, P. Ambient Temperature and Early Delivery of Singleton Pregnancies. Environ. Health Perspect. 2017, 125, 453–459. [Google Scholar] [CrossRef]
- Ha, S.; Liu, D.; Zhu, Y.; Sherman, S.; Mendola, P. Acute Associations between Outdoor Temperature and Premature Rupture of Membranes. Epidemiology 2018, 29, 175–182. [Google Scholar] [CrossRef]
- He, J.-R.; Liu, Y.; Xia, X.-Y.; Ma, W.-J.; Lin, H.-L.; Kan, H.-D.; Lu, J.-H.; Feng, Q.; Mo, W.-J.; Wang, P.; et al. Ambient Temperature and the Risk of Preterm Birth in Guangzhou, China (2001–2011). Environ. Health Perspect. 2016, 124, 1100–1106. [Google Scholar] [CrossRef] [Green Version]
- Jhun, I.; Mata, D.; Nordio, F.; Lee, M.; Schwartz, J.; Zanobetti, A. Ambient Temperature and Sudden Infant Death Syndrome in the United States. Epidemiology 2017, 28, 728–734. [Google Scholar] [CrossRef]
- Junkka, J.; Karlsson, L.; Lundevaller, E.; Schumann, B. Climate Vulnerability of Swedish Newborns: Gender Differences and Time Trends of Temperature-Related Neonatal Mortality, 1880–1950. Environ. Res. 2021, 192, 110400. [Google Scholar] [CrossRef]
- Liang, Z.; Lin, Y.; Ma, Y.; Zhang, L.; Zhang, X.; Li, L.; Zhang, S.; Cheng, Y.; Zhou, X.; Lin, H.; et al. The Association between Ambient Temperature and Preterm Birth in Shenzhen, China: A Distributed Lag Non-Linear Time Series Analysis. Environ. Health 2016, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Xiao, J.; Sun, X.; Chen, Q.; Yao, Z.; Feng, B.; Cao, G.; Guo, L.; He, G.; Hu, J.; et al. Associations of Maternal Ambient Temperature Exposures during Pregnancy with the Risk of Preterm Birth and the Effect Modification of Birth Order during the New Baby Boom: A Birth Cohort Study in Guangzhou, China. Int. J. Hyg. Environ. Health 2020, 225, 113481. [Google Scholar] [CrossRef] [PubMed]
- Meek, C.L.; Devoy, B.; Simmons, D.; Patient, C.; Aiken, A.R.; Murphy, H.R.; Aiken, C.E. Seasonal Variations in Incidence and Maternal–Fetal Outcomes of Gestational Diabetes. Diabet. Med. 2020, 37, 674–680. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Spangler, K.R.; Weinberger, K.R.; Yanosky, J.D.; Braun, J.M.; Wellenius, G.A. Ambient Temperature and Markers of Fetal Growth: A Retrospective Observational Study of 29 Million U.S. Singleton Births. Environ. Health Perspect. 2019, 127, 067005. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Lu, J.; Wang, E.; Lu, M.; An, Z.; Liu, Y.; Zeng, X.; Li, W.; Li, H.; Xu, D.; et al. Short-Term Effects of Ambient Temperature on the Risk of Premature Rupture of Membranes in Xinxiang, China: A Time-Series Analysis. Sci. Total Environ. 2019, 689, 1329–1335. [Google Scholar] [CrossRef]
- Su, W.-L.; Lu, C.-L.; Martini, S.; Hsu, Y.-H.; Li, C.-Y. A Population-Based Study on the Prevalence of Gestational Diabetes Mellitus in Association with Temperature in Taiwan. Sci. Total Environ. 2020, 714, 136747. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Luo, X.; Cao, G.; Zhao, C.; Xiao, J.; Liu, X.; Dong, M.; Wang, J.; Zeng, W.; Guo, L.; et al. Associations of Ambient Temperature Exposure during Pregnancy with the Risk of Miscarriage and the Modification Effects of Greenness in Guangdong, China. Sci. Total Environ. 2020, 702, 134988. [Google Scholar] [CrossRef]
- Wang, J.; Liu, X.; Dong, M.; Sun, X.; Xiao, J.; Zeng, W.; Hu, J.; Li, X.; Guo, L.; Rong, Z.; et al. Associations of Maternal Ambient Temperature Exposures during Pregnancy with the Placental Weight, Volume and PFR: A Birth Cohort Study in Guangzhou, China. Environ. Int. 2020, 139, 105682. [Google Scholar] [CrossRef]
- Wang, Y.-Y.; Li, Q.; Guo, Y.; Zhou, H.; Wang, Q.-M.; Shen, H.-P.; Zhang, Y.-P.; Yan, D.-H.; Li, S.; Chen, G.; et al. Ambient Temperature and the Risk of Preterm Birth: A National Birth Cohort Study in the Mainland China. Environ. Int. 2020, 142, 105851. [Google Scholar] [CrossRef]
- Weng, Y.-H.; Yang, C.-Y.; Chiu, Y.-W. Adverse Neonatal Outcomes in Relation to Ambient Temperatures at Birth: A Nationwide Survey in Taiwan. Arch. Environ. Occup. Health 2018, 73, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Yitshak-Sade, M.; Novack, L.; Landau, D.; Kloog, I.; Sarov, B.; Hershkovitz, R.; Karakis, I. Relationship of Ambient Air Pollutants and Hazardous Household Factors with Birth Weight among Bedouin-Arabs. Chemosphere 2016, 160, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Zhang, W.; Lu, C.; Norbäck, D.; Deng, Q. An Epidemiological Assessment of the Effect of Ambient Temperature on the Incidence of Preterm Births: Identifying Windows of Susceptibility during Pregnancy. J. Therm. Biol. 2018, 74, 201–207. [Google Scholar] [CrossRef]
- Sun, S.; Weinberger, K.R.; Spangler, K.R.; Eliot, M.N.; Braun, J.M.; Wellenius, G.A. Ambient Temperature and Preterm Birth: A Retrospective Study of 32 Million US Singleton Births. Environ. Int. 2019, 126, 7–13. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Kosatsky, T.; Smargiassi, A.; Bilodeau-Bertrand, M.; Auger, N. Heat and Pregnancy-Related Emergencies: Risk of Placental Abruption during Hot Weather. Environ. Int. 2018, 111, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Martens, D.S.; Plusquin, M.; Cox, B.; Nawrot, T.S. Early Biological Aging and Fetal Exposure to High and Low Ambient Temperature: A Birth Cohort Study. Environ. Health Perspect. 2019, 127, 117001. [Google Scholar] [CrossRef]
- Spolter, F.; Kloog, I.; Dorman, M.; Novack, L.; Erez, O.; Raz, R. Prenatal Exposure to Ambient Air Temperature and Risk of Early Delivery. Environ. Int. 2020, 142, 105824. [Google Scholar] [CrossRef]
- Babalola, O.; Razzaque, A.; Bishai, D. Temperature Extremes and Infant Mortality in Bangladesh: Hotter Months, Lower Mortality. PLoS ONE 2018, 13, e0189252. [Google Scholar] [CrossRef] [Green Version]
- Kilinc, M.F.; Cakmak, S.; Demir, D.O.; Doluoglu, O.G.; Yildiz, Y.; Horasanli, K.; Dalkilic, A. Does Maternal Exposure during Pregnancy to Higher Ambient Temperature Increase the Risk of Hypospadias? J. Pediatr. Urol. 2016, 12, 407.e1–407.e6. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.; Lundevaller, E.; Schumann, B. The Association between Cold Extremes and Neonatal Mortality in Swedish Sápmi from 1800 to 1895. Glob. Health Action 2019, 12, 1623609. [Google Scholar] [CrossRef] [Green Version]
- Minisha, F.; Mohamed, M.; Abdulmunem, D.; El Awad, S.; Zidan, M.; Abreo, M.; Ahmad, S.; Fender, G. Bacteriuria in Pregnancy Varies with the Ambiance: A Retrospective Observational Study at a Tertiary Hospital in Doha, Qatar. J. Périnat. Med. 2019, 48, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Molina, O.; Saldarriaga, V. The Perils of Climate Change: In Utero Exposure to Temperature Variability and Birth Outcomes in the Andean Region. Econ. Hum. Biol. 2017, 24, 111–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasileiou, V.; Kyratzoglou, E.; Paschou, S.A.; Kyprianou, M.; Anastasiou, E. The Impact of Environmental Temperature on the Diagnosis of Gestational Diabetes Mellitus. Eur. J. Endocrinol. 2018, 178, 209–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Feric, Z.; Cordero, J.F.; Meeker, J.D.; Alshawabkeh, A. Potential Influence of Temperature and Precipitation on Preterm Birth Rate in Puerto Rico. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kanner, J.; Williams, A.D.; Nobles, C.; Ha, S.; Ouidir, M.; Sherman, S.; Mendola, P. Ambient Temperature and Stillbirth: Risks Associated with Chronic Extreme Temperature and Acute Temperature Change. Environ. Res. 2020, 189, 109958. [Google Scholar] [CrossRef]
- Son, J.-Y.; Lee, J.-T.; Lane, K.J.; Bell, M.L. Impacts of High Temperature on Adverse Birth Outcomes in Seoul, Korea: Disparities by Individual- and Community-Level Characteristics. Environ. Res. 2019, 168, 460–466. [Google Scholar] [CrossRef]
- Zhong, Q.; Lu, C.; Zhang, W.; Zheng, X.; Deng, Q. Preterm Birth and Ambient Temperature: Strong Association during Night-Time and Warm Seasons. J. Therm. Biol. 2018, 78, 381–390. [Google Scholar] [CrossRef]
- Ha, S.; Zhu, Y.; Liu, D.; Sherman, S.; Mendola, P. Ambient Temperature and Air Quality in Relation to Small for Gestational Age and Term Low Birthweight. Environ. Res. 2017, 155, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Asamoah, B.; Kjellstrom, T.; Östergren, P.-O. Is Ambient Heat Exposure Levels Associated with Miscarriage or Stillbirths in Hot Regions? A Cross-Sectional Study Using Survey Data from the Ghana Maternal Health Survey 2007. Int. J. Biometeorol. 2018, 62, 319–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, J.; Horgan, G.; Bhattacharya, S. Placental Weight and Efficiency in Relation to Maternal Body Mass Index and the Risk of Pregnancy Complications in Women Delivering Singleton Babies. Placenta 2012, 33, 611–618. [Google Scholar] [CrossRef]
- Preston, E.V.; Eberle, C.; Brown, F.M.; James-Todd, T. Climate Factors and Gestational Diabetes Mellitus Risk–A Systematic Review. Environ. Health 2020, 19, 1–19. [Google Scholar] [CrossRef]
- Haghighi, M.M.; Wright, C.Y.; Ayer, J.; Urban, M.F.; Pham, M.D.; Boeckmann, M.; Areal, A.; Wernecke, B.; Swift, C.P.; Robinson, M.; et al. Impacts of High Environmental Temperatures on Congenital Anomalies: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4910. [Google Scholar] [CrossRef]
- Hackshaw, A. Small Studies: Strengths and Limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Kloog, I. Air Pollution, Ambient Temperature, Green Space and Preterm Birth. Curr. Opin. Pediatr. 2019, 31, 237–243. [Google Scholar] [CrossRef] [PubMed]
- McElroy, S.; Ilango, S.; Dimitrova, A.; Gershunov, A.; Benmarhnia, T. Extreme Heat, Preterm Birth, and Stillbirth: A Global Analysis across 14 Lower-Middle Income Countries. Environ. Int. 2021, 158, 106902. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Bloom, M.S.; Lin, S.; Ren, M.; Hajat, S.; Wang, Q.; Zhang, W.; Ho, H.C.; Zhao, Q.; Lin, Y.; et al. Temperature Variation and Preterm Birth among Live Singleton Deliveries in Shenzhen, China: A Time-to-Event Analysis. Environ. Res. 2021, 195, 110834. [Google Scholar] [CrossRef] [PubMed]
- Yackerson, N.; Piura, B.; Sheiner, E. The Influence of Meteorological Factors on the Emergence of Preterm Delivery and Preterm Premature Rupture of Membrane. J. Perinatol. 2008, 28, 707–711. [Google Scholar] [CrossRef]
- Wu, M.; Song, L.; Zheng, X.; Zhang, L.; Liu, B.; Wang, L.; Li, H.; Xiong, C.; Cao, Z.; Wang, Y.; et al. Prenatal Exposure of Diurnal Temperature Range and Preterm Birth: FINDINGS from a Birth Cohort Study in China. Sci. Total Environ. 2019, 656, 1102–1107. [Google Scholar] [CrossRef]
- Mora, C.; Dousset, B.; Caldwell, I.R.; Powell, F.E.; Geronimo, R.C.; Bielecki, C.R.; Counsell, C.W.W.; Dietrich, B.S.; Johnston, E.T.; Louis, L.V.; et al. Global Risk of Deadly Heat. Nat. Clim. Chang. 2017, 7, 501–506. [Google Scholar] [CrossRef]
- Poursafa, P.; Keikha, M.; Kelishadi, R. Systematic Review on Adverse Birth Outcomes of Climate Change. J. Res. Med. Sci. Off. J. Isfahan Univ. 2015, 20, 397–402. [Google Scholar]



| Temperature Exposure | Temperature Metrics | Number of Studies | Reference |
|---|---|---|---|
| Daily temperature exposure | Maximum daily temperature | 26 | [10,13,14,18,32,38,39,40,41,42,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59] |
| Minimum daily temperature | 16 | [10,13,18,39,41,43,50,51,52,53,54,55,56,57,58,59] | |
| Mean daily temperature | 35 | [15,16,18,32,41,46,51,52,53,54,55,56,57,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80] | |
| Weekly temperature exposure | Maximumweekly temperature | 3 | [14,48,81] |
| Mean weekly temperature | 4 | [15,19,82,83] | |
| Monthly temperature exposure | Maximum monthly temperature | 2 | [84,85] |
| Mean monthly temperature | 10 | [17,51,52,84,85,86,87,88,89,90] | |
| Hourly temperature exposure | Hourly ambient temperature | 3 | [91,92,93] |
| Trimester-specific exposures | Trimester-specific temperature | 3 | [75,76,94] |
| Apparent temperature exposure | Apparent temperature index | 1 | [32] |
| Daily maximum apparent temperature (MAT) | 2 | [11,33] | |
| Mean apparent daily temperature | 5 | [12,34,35,36,37] | |
| Mean apparent weekly temperature | 1 | [35] | |
| Mean apparent monthly temperature | 1 | [35] | |
| Universal apparent maximum temperature (UATmax) | 1 | [38] | |
| Heatindex/Heatwave/ Extreme heatevents exposure | Wet-bulb globe temperature (WBGT) | 1 | [95] |
| Dry temperature | 2 | [44,58] | |
| Wet temperature | 1 | [58] | |
| Mean heat index (HI) | 1 | [59] | |
| Heatwave/extreme heat events | 12 | [6,32,38,39,40,41,42,43,44,45,46,47] |
| Season | Percentage |
|---|---|
| Studies conducted only in summer months or warm months, or hot months | 34.67% |
| Studies conducted in both warm and cold months | 25.33% |
| Studies conducted in the summer and spring months | 2.67% |
| Studies conducted in all four seasons | 22.67% |
| Season not stated | 14.67% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalugoda, Y.; Kuppa, J.; Phung, H.; Rutherford, S.; Phung, D. Effect of Elevated Ambient Temperature on Maternal, Foetal, and Neonatal Outcomes: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 1771. https://doi.org/10.3390/ijerph19031771
Dalugoda Y, Kuppa J, Phung H, Rutherford S, Phung D. Effect of Elevated Ambient Temperature on Maternal, Foetal, and Neonatal Outcomes: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(3):1771. https://doi.org/10.3390/ijerph19031771
Chicago/Turabian StyleDalugoda, Yohani, Jyothi Kuppa, Hai Phung, Shannon Rutherford, and Dung Phung. 2022. "Effect of Elevated Ambient Temperature on Maternal, Foetal, and Neonatal Outcomes: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 3: 1771. https://doi.org/10.3390/ijerph19031771