
Effects of Caffeine and Caffeinated Beverages in Children, Adolescents and Young Adults: Short Review

Abstract
:1. Introduction
2. Materials and Methods
- The positive and adverse effects of different caffeine dosages in the body and in human performance;
- Short- and long-term effects of EDs in different age groups;
- Motivations for ED consumption;
- Effects of EDwA consumption among youngsters;
- The categories and topics selected for this publication were based on our interest; these topics are very popular in different research areas as well.
- Eligibility Criteria.
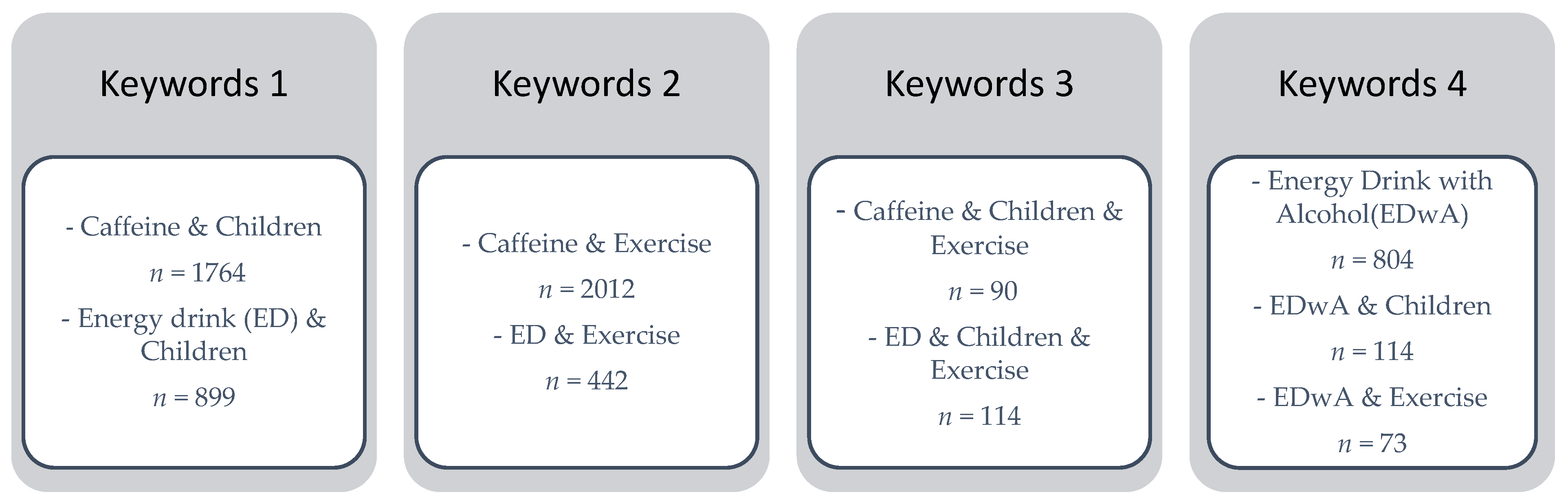
- When reviewing the literature, the following terms were important:
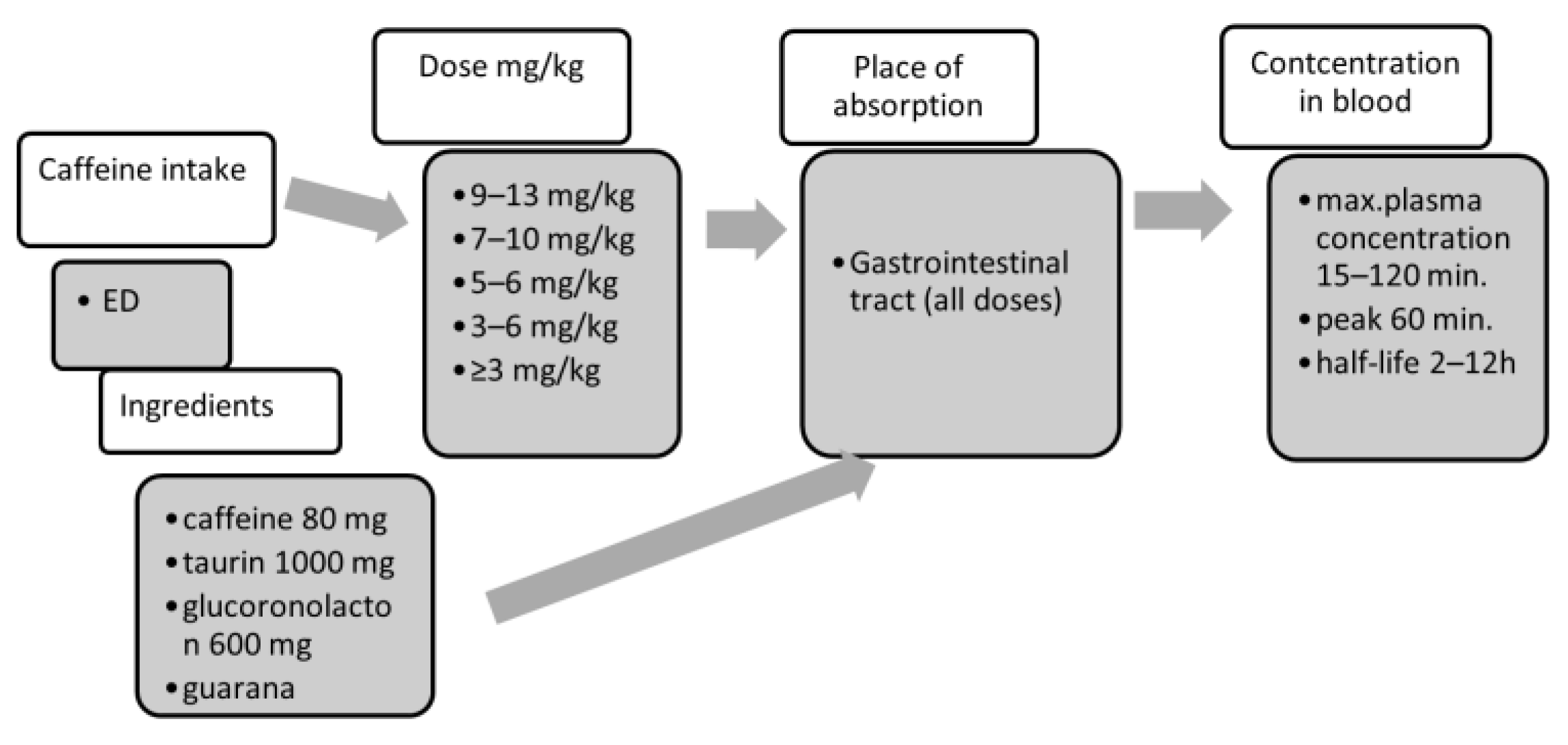
- Structure of caffeine, absorption, consumption;
- Caffeine-containing beverages;
- Positive and adverse physiological effects of caffeine;
- In special cases, animal studies were also included in the work.
- Sources of information.
- Search for data was accomplished electronically, using mostly PubMed databases. Other scientific sources were also added in case of fulfilling search criteria.
- Search for information.
- 1.
- Selection of Studies
- 2.
- Data Collection
- 3.
- Synthesis of Results Data were analyzed with regard to the following topics:
3. Results
3.1. Timing of Caffeine Ingestion
3.2. Effects of Caffeine Consumption in Different Dosages
3.3. Products Containing Caffeine
3.3.1. Energy Drinks
3.3.2. Caffeine, EDs, and Physical Performance
3.3.3. Caffeine and Cognition
3.3.4. Children, Young Adults, and EDs
3.4. ED Consumption with Alcohol (EDwA)
3.5. Sence of Coherence and Depression
3.6. Motivations for ED Consumption
4. Conclusions
Author Contributions
Funding
Institutional Review Board
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BL | Blood lactate |
| BP | Blood Pressure |
| cAMP | Cyclic Adenosine Monophosphate |
| CBF | Cerebral Blood Flow |
| CNS | Central Nervous System |
| ED | Energy Drink |
| EDwA | Energy Drink with Alcohol |
| FFA | Free Fatty Acids |
| HR | Heart Rate |
| HRmax | Maximal Heart Rate |
| IQ | Intelligence Quotient |
| NO | Nitric Oxide |
| RPE | Perceived Exertion |
| VO2max | Maximal Oxygen Consumption |
| TTE | Time to Exhaustion |
References
- Samoggia, A.; Rezzaghi, T. The Consumption of Caffeine-Containing Products to Enhance Sports Performance: An Application of an Extended Model of the Theory of Planned Behavior. Nutrients 2021, 13, 344. [Google Scholar] [CrossRef]
- Biaggioni, I.T.; Paul, S.U.; Puckett, A.N.; Arzubiaga, C. Caffeine and theophylline as adenosine receptor antagonists in humans. J. Pharmacol. Exp. Ther. 1991, 258, 588–593. [Google Scholar] [PubMed]
- Cappelletti, S.; Daria, P.; Sani, G.; Aromatario, M. Cognitive and Physical Performance Enhancer or Psychoactive Drug? Curr. Neuropharmacol. 2015, 13, 71–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016, 71, 294–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mielgo-Ayuso, J.; Marques-Jiménez, D.; Refoyo, I.; Del-Coso, J.; León-Guereño, P.; Calleja-González, J. Effect of Caffeine Supplementation on Sports Performance Based on Differences between Sexes: A Systematic Review. Nutrients 2019, 11, 2313. [Google Scholar] [CrossRef] [Green Version]
- Tarnopolsky, M.A. Effect of caffeine on the neuromuscular system—Potential as an ergogenic aid. Appl. Physiol. Nutr. Metab. 2008, 33, 1284–1289. [Google Scholar] [CrossRef]
- Jodra, P.; Lago-Rodríguez, A.; Sánchez-Oliver, A.J.; López-Samanes, A.; Pérez-López, A.; Veiga-Herreros, P.; San Juan, A.F.; Domínguez, R. Effects of caffeine supplementation on physical performance and mood dimensions in elite and trained-recreational athletes. J. Int. Soc. Sports Nutr. 2020, 17, 2. [Google Scholar] [CrossRef] [Green Version]
- Rahnama, N.; Gaeini, A.A.; Kazemi, F. The effectiveness of two energy drinks on selected indices of maximal cardiorespiratory fitness and blood lactate levels in male athletes. J. Res. Med Sci. 2010, 15, 127–132. [Google Scholar]
- Goldstein, E.R.; Ziegenfuss, T.; Kalman, D.; Kreider, R.; Campbell, B.; Wilborn, C.; Taylor, L.; Willoughby, D.; Stout, J.; Graves, B.S.; et al. International society of sports nutrition position stand: Caffeine and performance. J. Int. Soc. Sports Nutr. 2010, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Higashi, Y. Coffee and Endothelial Function: A Coffee Paradox? Nutrients 2019, 11, 2104. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.F.; Parrish, T.B. Caffeine’s effects on cerebrovascular reactivity and coupling between cerebral blood flow and oxygen metabolism. NeuroImage 2009, 44, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Hasse, C.G.; Becka, M.; Kuhlmann, J.; Wensing, G. Influences of caffeine, acetazolamide and cognitve stimulation on cerebral blood flow velocities. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 549–556. [Google Scholar] [CrossRef]
- Childs, E.; de Wit, H. Subjective, behavioral, and physiological effects of acute caffeine in light, nondependent caffeine users. Psychopharmacology 2006, 185, 514–523. [Google Scholar] [CrossRef]
- Haskell, C.F.; Kennedy, D.O.; Milne, A.L.; Wesnes, K.A.; Scholey, A.B. The effects of L-theanine caffeine and their combination on cognition and mood. Biol. Psychol. 2008, 77, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Smit, H.J.; Rogers, P.J. Effects of low doses of caffeine on cognitive performance, mood and thirst in low and higher caffeine consumers. Psychopharmacology 2000, 152, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.J. Caffeine, mood and mental performance in everyday life. Nutr Bull. 2007, 32, 84–89. [Google Scholar] [CrossRef]
- Zhang, Y.; Coca, A.; Casa, D.J.; Antonio, J.; Green, J.M.; Bishop, P.A. Caffeine and diuresis during rest and exercise: A meta-analysis. J. Sci. Med. Sport 2015, 18, 569–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, L.E. Caffeine, body fluid-electrolyte balance, and exercise performance. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 189–206. [Google Scholar] [CrossRef]
- Seifert, S.M.; Schaechter, J.L.; Hershorin, E.R.; Lipshultz, S.E. Health Effects of Energy Drinks on Children, Adolescents, and Young Adults. Pediarics 2011, 127, 511–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Ugalde, Y.C.; Romero-Palencia, A.; Román-Gutiérrez, A.D.; Ojeda-Ramírez, D.; Guzmán-Saldaña, R.M.E. Caffeine Consumption in Children: Innocuous or Deleterious? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2489. [Google Scholar] [CrossRef] [Green Version]
- Spriet, L.L. Exercise and Sport Performance with Low Doses of Caffeine. Sports Med. 2014, 44 (Suppl. S2), 175–184. [Google Scholar] [CrossRef] [Green Version]
- De Sanctis, V.; Soliman, N.; Soliman, A.T.; Elsedfy, H.; Di Maio, S.; El Kholy, M.; Fiscina, B. Caffeinated energy drink consumption among adolescents and potential health consequences associated with their use: A significant public health hazard. Acta Biomed. 2017, 88, 222–231. [Google Scholar]
- Ágoston, C.; Urbán, R.; Király, O.; Griffiths, M.D.; Rogers, P.J.; Demetrovics, Z. Why do you drink caffeine? The development of the Motives for Caffeine Consumption Questionnaire (MCCQ) and its relationship with gender, age and the types of caffeinated beverages. Int. J. Ment. Health Addict. 2018, 16, 981–999. [Google Scholar] [CrossRef] [Green Version]
- Krieger, D.R.; Kalman, D.S.; Feldman, S.; Arnillas, L.; Goldberg, D.; Gisbert, O.; Nader, S. The Safety, Pharmacokinetics, and Nervous System Effects of Two Natural Sources of Caffeine in Healthy Adult Males. Clin. Transl. Sci. 2016, 9, 246–251. [Google Scholar] [CrossRef]
- Temple, J.L.; Bernard, C.; Lipshultz, S.E.; Czachor, J.D.; Westphal, J.A.; Mestre, M.A. The Safety of Ingested Caffeine: A Comprehensive Review. Front. Psychiatry 2017, 8, 80. [Google Scholar] [CrossRef] [Green Version]
- Laquale, K.M. Red Bull: The other energy drink and its effect on performance. Movement Arts, Health Promotion and Leisure Studies Faculty Publications. Athl. Ther. Today 2007, 12, 43–45. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, A.B.; Randell, R.K.; Jeukendup, A.E. The metabolic and performance effects of caffeine compared to coffee during endurance exercise. PLoS ONE 2013, 8, e59561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, T.E.; Spriet, L.L. Metabolic, catecholamine and exercise performance responses to varying doses of caffeine. J. Appl. Physiol. 1995, 78, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.B.; Greenblatt, D.J.; Ehrenberg, B.L.; Goddard, J.E.; Cotreau, M.M.; Harmatz, J.S.; Shader, R.I. Dose-dependent pharmacokinetics and psychomotor effects of caffeine in humans. J. Clin. Pharmacol. 1997, 37, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Kerrigan, S.; Lindsey, T. Fatal caffeine overdose: Two case reports. Forensic Sci. Int. 2005, 153, 67–69. [Google Scholar] [CrossRef]
- Willson, C. The clinical toxicology of caffeine: A review and case study. Toxicol. Rep. 2018, 5, 1140–1152. [Google Scholar] [CrossRef]
- Graham, T.E.; Helge, J.W.; MacLean, D.A.; Kiens, B.; Richter, E.A. Caffeine ingestion does not alter carbohydrate or fat metabolism in skeletal muscle during exercise. J. Physiol. 2000, 529, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Bedi, N.; Dewan, P.; Gupta, P. Energy drinks: Potions of illusion. Indian Pediatr. 2014, 51, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Alsunni, A.A. Energy Drink Consumption: Beneficial and Adverse Health Effects. Int. J. Health Sci. 2015, 9, 468–474. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. Are the current guidelines on caffeine use in sport optimal for everyone? Inter-individual variation in caffeine ergogenicity, and a move towards personalised sports nutrition. Sports Med. 2018, 48, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Smith, A. Effects of caffeine on human behavior. Food Chem. Toxicol. 2002, 40, 1243–1255. [Google Scholar] [CrossRef]
- Higgins, J.P.; Babu, K.M. Caffeine reduces myocardial blood flow during exercise. Am. J. Med. 2013, 126, 730.e1-8. [Google Scholar] [CrossRef]
- Nowak, D.; Goslinski, M. Assessment of Antioxidant Properties of Classic Energy Drinks in Comparison with Fruit Energy Drinks. Foods 2020, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, D.; Rodricks, J.V.; Mariano, G.F.; Chowdhury, F. Caffeine and cardiovascular health. Regul. Toxicol. Pharmacol. 2017, 89, 165–185. [Google Scholar] [CrossRef]
- Curran, C.P.; Marczinski, C.A. Taurine, caffeine, and energy drinks: Reviewing the risks to the adolescent brain. Birth Defects Res. 2017, 109, 1640–1648. [Google Scholar] [CrossRef] [PubMed]
- Arenas-Jal, M.; Sune-Negre, J.M.; Perez-Lozano, P.; Garcia, E. Trends in the food and sports nutrition industry: A review. Crit. Rev. Food Sci. Nutr. 2021, 60, 1–17. [Google Scholar] [CrossRef]
- Reissig, C.J.; Strain, E.C.; Griffiths, R.R. Caffeinated energy drinks—A growing problem. Drug Alcohol Depend 2009, 99, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Sim, S.; Choi, H.G. High stress, lack of sleep, low school performance, and suicide attempts are associated with high energy drink intake in adolescents. PLoS ONE 2017, 12, e0187759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolk, B.J.; Ganetsky, M.; Babu, K.M. Toxicity of energy drinks. Curr. Opin. Pediatr. 2012, 24, 243–251. [Google Scholar] [CrossRef]
- Thomson, B.; Schiess, S. Risk Profile: Caffeine in Energy Drinks and Energy Shots. 2011. Available online: www.nzfsa.govt.nz/science/risk-profiles/fw10002-caffeine-inbeverages-risk-profile.pdf (accessed on 5 November 2021).
- Ellison, R.C.; Singer, M.R.; Moore, L.L. Current caffeine intake of young children: Amount and sources. J. Am. Diet. Assoc. 1995, 95, 802–803. [Google Scholar] [CrossRef]
- Morgan, K.J.; Stults, V.J.; Zabik, M.E. Amount and dietary sources of caffeine and saccharin intake by individuals 5–18 years. Regul. Toxicol. Pharmacol. 1982, 2, 296–307. [Google Scholar] [CrossRef]
- Grasser, E.K.; Yepuri, G.; Dulloo, A.G.; Montani, J.P. Cardio- and cerebrovascular responses to the energy drink Red Bull in young adults: A randomized cross-over study. Eur. J. Nutr. 2014, 53, 1561–1571. [Google Scholar] [CrossRef] [Green Version]
- Nowaczewska, M.; Wiciński, M.; Kaźmierczak, W. The Ambiguous Role of Caffeine in Migraine Headache: From Trigger to Treatment. Nutrients 2020, 12, 2259. [Google Scholar] [CrossRef]
- Overstreet, D.S.; Penn, T.M.; Cable, S.T.; Aroke, E.N.; Goodin, B.R. Higher habitual dietary caffeine consumption is related to lower experimental pain sensitivity in a community-based sample. Psychopharmacology 2018, 235, 3167–3176. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Diener, H.C.; Robbins, M.S.; Garas, S.Y.; Patel, K. Caffeine in the management of patients with headache. J. Headache Pain 2017, 18, 107. [Google Scholar] [CrossRef]
- Woojae, K. Debunking the Effects of Taurine in Red Bull Energy Drink. Nutr. Bytes 2003, 9, 1. [Google Scholar]
- Alford, C.; Cox, H.; Wescott, R. The effects of red bull energy drink on human performance and mood. Amino Acids 2001, 21, 139–150. [Google Scholar] [CrossRef]
- Seidl, R.; Peyrl, A.; Nicham, R.; Hauser, E. A taurine and caffeine-containing drink stimulates cognitive performance and well-being. Amino Acids 2000, 19, 635–642. [Google Scholar] [CrossRef]
- Campbell, B.; Wilborn, C.; La Bounty, P.; Taylor, L.; Nelson, M.; Greenwood, M.; Ziegenfuss, T.N.; Lopez, H.L.; Hoffman, J.R.; Stout, J.R.; et al. International Society of Sports Nutrition position stand: Energy drinks. J. Int. Soc. Sports Nutr. 2013, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kammerer, M.; Jaramillo, J.A.; García, A.; Calderín, J.C.; Valbuena, L.H. Effects of energy drink major bioactive compounds on the performance of young adults in fitness and cognitive tests: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2014, 11, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breda, J.J.; Whiting, S.H.; Encarnação, R.; Norberg, S.; Jones, R.; Reinap, M.; Jewell, J. Energy drink consumption in europe: A review of the risks, adverse health effects, and policy options to respond. Front. Public Health 2014, 2, 134. [Google Scholar] [CrossRef]
- Higgins, J.P.; Yarlagadda, S.; Yang, B. Cardiovascular Complications of Energy Drinks. Beverages 2015, 1, 104. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Ortiz, B.L. Energy drink ingredients and their effect on endothelial function: A Review. Int. J. Clin. Cardiolol. 2014, 1, 1–6. [Google Scholar] [CrossRef]
- Watson, E.J.; Banks, S.; Coates, A.M.; Kohler, M.J. The Relationship between Caffeine, Sleep, and Behavior in Children. J. Clin. Sleep Med. 2017, 13, 533–543. [Google Scholar] [CrossRef] [Green Version]
- Heckman, M.A.; Weil, J.; Gonzalez de Mejia, E. Caffeine (1, 3, 7-trimethylxanthine) in foods: A comprehensive review on consumption, functionality, safety, and regulatory matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef]
- Babu, K.M.; Church, R.J.; Lewander, W. Energy drinks: The new eye-opener for adolescents. Clin. Pediatr. Emerg. Med. 2008, 9, 35–42. [Google Scholar] [CrossRef]
- Scholey, A.; Kennedy, D. Cognitive and physiological effects of an „energy drink”: An evaluation of the whole drink and of glucose, caffeine and herbal flavouring fractions. Psychopharmacology 2004, 176, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Geiß, K.; Jester, I.; Falke, W.; Hamm, M.; Waag, K. The effect of a taurine containing drink on performance in 10 endurance-athletes. Amino Acids 1994, 7, 45–56. [Google Scholar] [CrossRef]
- Rashti, S.L.; Ratamess, N.L.; Kang, J.; Faigenbaum, A.D.; Chilakos, A.; Hoffman, J.R. Thermogenic effect of meltdown RTD™ energy drink in young healthy women: A double blind, cross-over design study. Lipids Health Dis. 2009, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, J.R.; Kang, J.; Ratamess, N.A.; Hoffman, M.W.; Tranchina, C.P.; Faigenbaum, A.D. Examination of a high energy, pre-exercise supplement on exercise performance. J. Internat. Soc. Sports Nutr. 2009, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Burke, L.M. Caffeine and sports performance. Appl. Physiol. Nutr. Metab. 2008, 33, 1319–1934. [Google Scholar] [CrossRef] [PubMed]
- Pickering, C.; Kiely, J. Are low doses of caffeine as ergogenic as higher doses? A critical review highlighting the need for comparison with current best practice in caffeine research. Nutrition 2019, 67, 110535. [Google Scholar] [CrossRef] [PubMed]
- Turley, K.R.; Gerst, J.W. Effects of caffeine on physiological responses to exercise in young boys and girls. Med. Sci. Sports Exerc. 2006, 38, 520–526. [Google Scholar] [CrossRef]
- Del Coso, J.; Salinero, J.J.; González-Millán, C.; Abián-Vicén, J.; Pérez-González, B. Dose response effects of a caffeine-containing energy drink on muscle performance: A repeated measures design. J. Int. Soc. Sports Nutr. 2012, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Astorino, T.A.; Matera, A.J.; Basinger, J.; Evans, M.; Schurman, T.; Marquez, R. Effects of red bull energy drink on repeated sprint performance in women athletes. Amino Acids 2012, 42, 1803–1808. [Google Scholar] [CrossRef]
- Turley, K.; Eusse, P.A.; Thomas, M.M.; Townsend, J.R.; Morton, A.B. Effects of different doses of caffeine on anaerobic exercise in boys. Pediatr. Exerc. Sci. 2015, 27, 50–56. [Google Scholar] [CrossRef]
- Paton, C.; Costa, V.; Guglielmo, L. Effects of caffeine chewing gum on race performance and physiology in male and female cyclists. J. Sports Sci. 2015, 33, 1076–1083. [Google Scholar] [CrossRef]
- Suvi, S.; Timpmann, S.; Tamm, M.; Aedma, M.; Kreegipuu, K.; Ööpik, V. Effects of caffeine on endurance capacity and psychological state in young females and males exercising in the heat. Appl. Physiol. Nutr. Metab. 2016, 42, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Skinner, T.L.; Desbrow, B.; Arapova, J.; Schaumberg, M.A.; Osborne, J.; Grant, G.D.; Anoopkumar-Dukie, S.; Leveritt, M.D. Women experience the same ergogenic response to caffeine as men. Med. Sci. Sports Exerc. 2019, 51, 1195–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adan, A.; Prat, G.; Fabbri, M.; Sanchez-Turet, M. Early effects of caffeinated and decaffeinated coffee on subjective state and gender differences. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1698–1703. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, D.J.; Lessard, S.J.; Coffe, V.G.; Churchley, E.G.; Wootton, A.M.; Ng, T.; Watt, M.J.; Hawley, J.A. High rates of muscle glycogen resynthesis after exhaustive exercise when carbohydrate is coingested with caffeine. J. Appl. Physiol. (1985) 2008, 105, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Garcia, E.; van Dam, R.M.; Willett, W.C.; Rimm, E.B.; Manson, J.E.; Stampfer, M.J.; Rexrode, K.M.; Hu, F.B. Coffee consumption and coronary heart disease in men and women: A prospective cohort study. Circulation 2006, 113, 2045–2053. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, A.T.; Gervino, E.V.; Nakao, S.; Come, P.C.; Silverman, K.J.; Grossman, W. The effect of caffeine on exercise tolerance and left ventricular function in patients with coronary artery disease. Ann. Intern. Med. 1989, 110, 593–598. [Google Scholar] [CrossRef]
- Chen, H.Y.; Wang, H.S.; Tung, K.; Chao, H.H. Effects of gender difference and caffeine supplementation on anaerobic muscle performance. Int. J. Sports Med. 2015, 36, 974–978. [Google Scholar] [CrossRef]
- Dawes, J.; Ocker, L.B.; Temple, D.R.; Spaniol, F.; Murray, A.M.; Bonnette, R. Effect of a pre-exercise energy drink (Redline®) on upper-body muscular endurance performance. J. Int. Soc. Sports Nutr. 2011, 8 (Suppl. S1), P18. [Google Scholar] [CrossRef] [Green Version]
- Sanders, G.J.; Peveler, W.; Holmer, B.; Peacock, C.A. The effect of three different energy drinks on oxygen consumption and perceived exertion during treadmill exercise. J. Int. Soc. Sports Nutr. 2015, 12 (Suppl. S1), P1. [Google Scholar] [CrossRef] [Green Version]
- Goel, V.; Manjunatha, S.; Pai, K.M. Effect of red bull energy drink on auditory reaction time and maximal voluntary contraction. Indian J. Physiol. Pharmacol. 2014, 58, 17–21. [Google Scholar]
- Cunha, R.A.; Agostinho, P.M. Chronic caffeine consumption prevents memory disturbance in different animal models of memory decline. J. Alzheimers Dis. 2010, 20 (Suppl. S1), 95–116. [Google Scholar] [CrossRef] [Green Version]
- Einöther, S.J.; Giesbrecht, T. Caffeine as an attention enhancer: Reviewing existing assumptions. Psychopharmacology 2013, 225, 251–274. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.J.; Heatherley, S.V.; Mullings, E.L.; Smith, J.E. Faster but not smarter: Effects of caffeine and caffeine withdrawal on alertness and performance. Psychopharmacology 2013, 226, 229–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, R.R.; Mumford, G.K. Caffeine reinforcement, discrimination, tolerance, and physical dependence in laboratory animals and humans. In Handbook of Experimental Pharmacology; Schuster, C.R., Kuhar, M.J., Eds.; Springer: Berlin/Heidelberg, Germany, 1996; pp. 315–341. [Google Scholar]
- Lieberman, H.R. Nutrition, brain function and cognitive performance. Appetite 2003, 40, 245–254. [Google Scholar] [CrossRef]
- Kennedy, D.; Scholey, A. A glucose-caffeine ‘energy drink’ ameliorates subjective and performance deficits during prolonged cognitive demand. Appetite 2004, 42, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Nehlig, A. Is caffeine a cognitive enhancer? J. Alzheimers Dis. 2010, 20, S85–S94. [Google Scholar] [CrossRef] [Green Version]
- Childs, E.; de Wit, H. Enhanced mood and psychomotor performance by a caffeine-containing energy capsule in fatigued individuals. Exp. Clin. Psychopharm. 2008, 16, 13–21. [Google Scholar] [CrossRef]
- Howard, M.A.; Marczinski, C.A. Acute effects of a glucose energy drink on behavioral control. Exp. Clin. Psychopharmacol. 2010, 18, 553–561. [Google Scholar] [CrossRef]
- Marczinski, C.A.; Stamates, A.L.; Ossege, J.; Maloney, S.F.; Bardgett, M.E.; Brown, C.J. Subjective State, Blood Pressure, and Behavioral Control Changes Produced by an “Energy Shot”. J. Caffeine Res. 2014, 4, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boere, J.J.; Fellinger, L.; Huizinga, D.J.H.; Wong, S.F.; Bijleveld, E. Performance pressure and caffeine both affect cognitive performance, but likely through independent mechanisms. Brain Cogn. 2016, 102, 26–32. [Google Scholar] [CrossRef]
- Galéra, C.; Bernard, J.Y.; van der Waerden, J.; Bouvard, M.P.; Lioret, S.; Forhan, A.; De Agostini, M.; Melchior, M.; Heude, B. EDEN Mother-Child Cohort Study Group. Prenatal Caffeine Exposure and Child IQ at Age 5.5 Years: The EDEN Mother-Child Cohort. Biol. Psychiatry 2016, 80, 720–726. [Google Scholar] [CrossRef]
- Serrano, M.I.; Goicoechea, C.; Serrano, J.S.; Serrano-Martino, M.C.; Sánchez, E.; Martín, M.I. Age-related changes in the antinociception induced by taurine in mice. Pharmacol. Biochem. Behav. 2002, 73, 863–867. [Google Scholar] [CrossRef]
- Heatherley, S.V.; Hancock, K.M.; Rogers, P.J. Psychostimulant and other effects of caffeine in 9- to 11-year-old children. J. Child. Psychol. Psychiatry 2006, 27, 135–142. [Google Scholar] [CrossRef]
- European Food Safety Authority. EFSA Explains Risk Assessment. Caffeine. Available online: https://www.efsa.europa.eu/en/corporate/pub/efsaexplainscaffeine150527 (accessed on 11 January 2021).
- Zucconi, S.; Volpato, C.; Adinolfi, F.; Gandini, E.; Gentile, E.; Loi, A.; Fioriti, L. Gathering Consumption Data on Specific Consumer Groups of Energy Drinks. EFSA Parma: Supporting Publications 2013. Available online: https://doi.org/10.2903/sp.efsa.2013.EN-394 (accessed on 12 January 2021). [CrossRef] [Green Version]
- Reid, J.L.; Hammond, D.; McCrory, C.; Dubin, J.A.; Leatherdale, S.T. Use of caffeinated energy drinks among secondary school students in Ontario: Prevalence and correlates of using energy drinks and mixing with alcohol. Can. J. Public Health 2015, 106, e101–e108. [Google Scholar] [CrossRef]
- Beckford, K.; Grimes, C.A.; Riddell, L.J. Australian children’s consumption of caffeinated, formulated beverages: A cross-sectional analysis. BMC Public Health 2015, 15, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, B.M.; Hayley, A.; Miller, P. Adolescent energy drink consumption: An Australian perspective. Appetite 2016, 105, 638–642. [Google Scholar] [CrossRef]
- Visram, S.; Cheetham, M.; Riby, D.M.; Stephen, J.; Crossley, S.J.; Lake, A.A. Consumption of energy drinks by children and young people: A rapid review examining evidence of physical effects and consumer attitudes. BMJ Open 2016, 6, e010380. [Google Scholar] [CrossRef] [Green Version]
- Terry-McElrath, Y.M.; O’Malley, P.M.; Johnston, L.D. Energy drinks, soft drinks, and substance use among United States secondary school students. J. Addict. Med. 2014, 8, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, L.D.; Scherr, R.E. Risk of Energy Drink Consumption to Adolescent Health. Am. J. Lifestyle Med. 2019, 13, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.E.; Dermen, K.H.; Lucke, J.F. Caffeinated energy drink use by U.S. adolescents aged 13–17: Anational profile. Psychol. Addict. Behav. 2018, 32, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Leal, W.E.; Jackson, D.B. Energy drinks and escalation in drug use severity: An emergent hazard to adolescent health. Prev. Med. 2018, 111, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, H.A.; Boak, A.; Ilie, G.; Mann, R.E. Energy drink consumption and associations with demographic characteristics, drug use and injury among adolescents. J. Public Health 2013, 104, e496–e501. [Google Scholar] [CrossRef]
- Azagba, S.; Langille, D.; Asbridge, M. An emerging adolescent health risk: Caffeinated energy drink consumption patterns among high school students. Prev. Med. 2014, 62, 54–59. [Google Scholar] [CrossRef]
- Schwartz, D.L.; Glistad-Hayden, K.; Caroll-Scott, A.; Grilo, S.A.; McCaslin, C.; Schwartz, M.; Ickovics, J.R. Energy drinks and youth self-reported hyperactivity/inattention symptoms. Acad. Pediatr. 2015, 15, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Kristjansson, A.L.; Sigfusdottir, I.D.; Frost, S.S.; James, J.E. Adolescent caffeine consumption and self-reported violence and conduct disorder. J. Youth Adolesc. 2013, 42, 1053–1062. [Google Scholar] [CrossRef]
- Van Batenburg-Eddes, T.; Lee, N.C.; Weeda, W.D.; Krabbendam, L.; Huizinga, M. The potential adverse effect of energy drinks on executive functions in early adolescence. Front. Psychol. 2014, 5, 457. [Google Scholar] [CrossRef] [Green Version]
- Huhtinen, H.; Lindfors, P.; Rimpelä, A. Adolescents’ use of energy drinks and caffeine induced health complaints in Finland. Eur. J. Public Health 2013, 23 (Suppl. S1), 166. [Google Scholar] [CrossRef] [Green Version]
- Dörner, J. MRI Tecnique Shows How Energy Drinks Alter Hear Function. Available online: www.auntminnie.com/Redirect/Redirect.aspx?ItemId=105781 (accessed on 26 November 2016).
- Schneider, M.B.; Benjamin, H.J. Sports drinks and energy drinks for children and adolescents: Are they appropriate? Pediatrics 2011, 127, 1182–1189. [Google Scholar]
- Kozik, T.M.; Shah, S.; Bhattacharyya, M.; Franklin, T.T.; Connolly, T.F.; Chien, W.; Charos, G.S.; Pelter, M.M. Cardiovascular responses to energy drinks in a healthy population: The C-energy study. Am. J. Emerg. Med. 2016, 34, 1205–1209. [Google Scholar] [CrossRef] [PubMed]
- Svatikova, A.; Covassin, N.; Somers, K.R.; Somers, K.V.; Soucek, F.; Kara, T.; Bukartyk, J. A randomized trial of cardiovascular responses to energy drink consumption in healthy adults. JAMA 2015, 314, 2079–2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Degirmenci, N.; Fossum, I.N.; Strand, T.A.; Holten-Andersen, M.N. Consumption of energy drinks among adolescents in Norway: A cross-sectional study. BMC Public Health 2018, 18, 1391. [Google Scholar] [CrossRef]
- Silva, A.C.; de Oliveira Ribeiro, N.P.; de Mello Schier, A.R.; Pereira, V.M.; Vilarim, M.M.; Pessoa, T.M.; Arias-Carrión, O.; Machado, S.; Nardi, A.E. Caffeine and suicide: A systematic review. CNS Neurol. Disord. Drug Targets. 2014, 13, 937–944. [Google Scholar] [CrossRef]
- Kristjansson, A.L.; Sigfusdottir, I.D.; Mann, M.J.; James, J.E. Caffeinated sugar-sweetened beverages and common physical complaints in Icelandic children aged 10–12 years. Prev. Med. 2014, 58, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Nordt, S.P.; Vilke, G.M.; Clark, R.F.; Lee Cantrell, F.; Chan, T.C.; Galinato, M.; Nguyen, V.; Castillo, E.M. Energy drink use and adverse effects among emergency department patients. JCH 2012, 37, 976–981. [Google Scholar] [CrossRef]
- Park, S.; Lee, Y.; Lee, J.H. Association between energy drink intake, sleep, stress, and suicidality in Korean adolescents: Energy drink use in isolation or in combination with junk food consumption. Nutr. J. 2016, 15, 87. [Google Scholar] [CrossRef] [Green Version]
- LaBotz, M.; Bernard, A. Griesemer and council on sports medicine and fitness Use of Performance-Enhancing Substances. Pediatrics 2016, 138, e20161300. [Google Scholar] [CrossRef] [Green Version]
- Thomson, B.M.; Campbell, D.M.; Cressey, P.; Egan, U.; Horn, B. Energy drink consumption and impact on caffeine risk. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess 2014, 31, 1476–1488. [Google Scholar] [CrossRef]
- Seifert, S.M.; Seifert, S.A.; Schaechter, J.L.; Bronstein, A.C.; Benson, B.E.; Hershorin, E.R.; Arheart, K.L.; Franco, V.I.; Lipshultz, S.E. An analysis of energy-drink toxicity in the National Poison Data System. Clin. Toxicol. 2013, 51, 566–574. [Google Scholar] [CrossRef]
- McLellan, T.M.; Lieberman, H.R. Do energy drinks contain active components other than caffeine? Nutr. Rev. 2012, 70, 730–744. [Google Scholar] [CrossRef] [PubMed]
- Shao, A.; Hathcock, J.N. Risk assessment for the amino acids taurine, L-glutamin and L-arginine. Regul. Toxicol. Pharmacol. 2008, 50, 376–399. [Google Scholar] [CrossRef]
- Caine, J.J.; Geracioti, T.D. Taurine, energy drinks, and neuroendocrine effects. Cleve. Clin. J. Med. 2016, 83, 895–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Idrissi, A.; Trenkner, E. Taurine regulates mitochondrial calcium homeostasis. Adv. Exp. Med. Biol. 2003, 526, 527–536. [Google Scholar]
- Baum, M.; Weiss, M. The influence of a taurine containing drink on cardiac parameters before and after exercise measured by echocardiography. Amino Acids 2001, 20, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Soós, R.; Tékus, É.; Bodó, D.; Wilhelm, M. Side effects of energy drinks and caffeinated beverages. In Book of Abstracts of the 21st Annual Congress of the European College of Sport Science, Vienna, Austria, 6–9 June 2016; Baca, A., Wessner, B., Diketmüller, R., Tschan, H., Hofmann, M., Kornfeind, P., Tsolakidis, E., Eds.; European College of Sport Science: Vienna, Austria, 2016. [Google Scholar]
- Tóth, Á.; Soós, R.; Szovák, E.; Najbauer, N.M.; Tényi, D.; Csábí, G.; Wilhelm, M. Energy Drink Consumption, Depression, and Salutogenic Sense of Coherence among Adolescents and Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, J.L.; Mc Crory, C.; White, C.M.; Martineau, C.; Vanderkooy, P.; Fenton, N.; Hammond, D. Consumption of Caffeinated Energy Drinks Among Youth and Young Adults in Canada. Prev. Med. Rep. 2016, 5, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Blanck, H.M.; Sherry, B.; Brener, N.; O’Toole, T. Factors associated with sugar-sweetened beverage intake among United States high school students. J. Nutr. 2012, 142, 306–312. [Google Scholar] [CrossRef] [Green Version]
- Temple, J.L. Review: Trends, Safety, and Recommendations for Caffeine Use in Children and Adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 2018, 58, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Magnezi, R.; Bergman, L.C.; Grinvald-Fogel, H.; Cohen, H.A. A survey of energy drink and alcohol mixed with energy drink consumption. Isr. J. Health Policy Res. 2015, 4, 55. [Google Scholar] [CrossRef] [Green Version]
- Lebacq, T.; Desnouck, V.; Dujeu, M.; Holmberg, E.; Pedroni, C. Determinants of energy drink consumption in adolescents: Identification of sex-specific patterns. Public Health 2020, 185, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Gradvohl, E.; Vida, K.; Rácz, J. Fill it up: Combined consumption of alcohol with energy drinks and its correlation with risk taking behaviour among young adults. Orv. Hetil. 2015, 156, 1100–1108. (In Hungarian) [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck, J.D.; Peck, B.M.; Skaggs, V.J.; Fukushima, M.; Kaplan, H.B. Socio-environmental factors associated with pubertal development in female adolescents: The role of prepubertal tobacco and alcohol use. J. Adolesc. Health 2011, 48, 241–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, M.A.; Oinonen, K.A. Age at menarche is associated with divergent alcohol use patterns in early adolescence and early adulthood. J. Adolesc. 2011, 34, 1065–1076. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.L.; Ziegler, A.M.; Graczyk, M.S.; Bendlin, A.; Sion, T.; Vattana, K. Cardiovascular responses to caffeine by gender and pubertal stage. Pediatrics 2014, 134, e112–e119. [Google Scholar] [CrossRef] [Green Version]
- Temple, J.L.; Ziegler, A.M.; Martin, C.; de Wit, H. Subjective responses to caffeine are influenced by caffeine dose, sex, and pubertal stage. J. Caffeine Res. 2015, 5, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Marczinski, C.A.; Fillmore, M.T.; Henges, A.L.; Ramsey, M.A.; Young, C.R. Mixing an energy drink with an alcoholic beverage increase motivation for more alcohol in college students. Alcohol. Clin. Exp. Res. 2013, 37, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Marczinski, C.A.; Fillmore, M.T.; Stamates, A.L.; Maloney, S.F. The Desire to Drink Alcohol is Enhanced with High Caffeine Energy Drink Mixers. Alcohol. Clin. Exp. Res. 2016, 40, 1982–1990. [Google Scholar] [CrossRef] [Green Version]
- Rossheim, M.E.; Thombs, D.L.; Weiler, R.M.; Barry, A.E.; Suzuki, S.; Walters, S.T.; Barnett, T.E.; Paxton, R.J.; Pealer, L.N.; Cannell, B. Alcohol mixed with energy drink: Use may be a consequence of heavy drinking. Addict. Behav. 2016, 57, 55–61. [Google Scholar] [CrossRef]
- Blankson, K.; Thompson, A.M.; Ahrendt, D.M.; Patrick, V. Energy drinks: What teenagers (and their doctors) should know. Pediatr. Rev. 2013, 34, 55–62. [Google Scholar] [CrossRef]
- Verster, J.C.; Benjaminsen, J.M.; van Lanen, J.H.; van Stavel, N.M.; Olivier, B. Effects of mixing alcohol with energy drink on objective and subjective intoxication: Results from a Dutch on-premise study. Psychopharmacology 2015, 232, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonar, E.E.; Cunningham, R.M.; Polshkova, S.; Chermack, S.T.; Blow, F.C.; Walton, M.A. Alcohol and energy drink use among adolescents seeking emergency department care. Addict. Behav. 2015, 43, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalese, M.; Denoth, F.; Siciliano, V.; Bastiani, L.; Cotichini, R.; Cutilli, A.; Molinaro, S. Energy Drink and Alcohol mixed Energy Drink use among high school adolescents: Association with risk taking behavior, social characteristics. Addict. Behav. 2017, 72, 93–99. [Google Scholar] [CrossRef]
- Miller, K.E. Energy Drinks, Race, and Problem Behaviors among College Students. J. Adolesc. Health 2008, 43, 490–497. [Google Scholar] [CrossRef] [Green Version]
- Miyake, E.R.; Marmorstein, N.R. Energy drink consumption and later alcohol use among early adolescents. Addict. Behav. 2015, 43, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.T.; Vendruscolo, L.F.; Takahashi, R.N. Binge-like ingestion of a combination of an energy drink and alcohol leads to cognitive deficits and motivational changes. Pharmacol. Biochem. Behav. 2015, 136, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Ericson, M.; Ulenius, L.; Adermark, L.; Söderpalm, B. Minor Adaptations of Ethanol-Induced Release of Taurine Following Chronic Ethanol Intake in the Rat. Adv. Exp. Med. Biol. 2017, 975, 217–224. [Google Scholar]
- Krahe, T.E.; Filgueiras, C.C.; da Silva Quaresma, R.; Schibuola, H.G.; Abreu-Villaça, Y.; Manhães, A.C.; Ribeiro-Carvalho, A. Energy drink enhances the behavioral effects of alcohol in adolescent mice. Neurosci. Lett. 2017, 651, 102–108. [Google Scholar] [CrossRef]
- Malinauskas, B.M.; Aeby, V.G.; Overton, R.F.; Carpenter-Aeby, T.; Barber-Heidal, K. A survey of energy drink comsumption patterns among college students. Nutr. J. 2007, 6, 35. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.J.; Alford, C.; Verster, J.C.; Stewart, K. Motives for mixing alcohol with energy drinks and other non-alcoholic beverages and its effects on overall alcohol consumption among UK students. Appetite 2016, 96, 588–597. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Dose (mg/day) | Effects |
|---|---|---|
| Kaplan et al., 1997 [29] Willson, 2018 [31] Smith, 2002 [36] | 250 mg | increased arousal, alertness, concentration, well-being |
| Kaplan et al., 1997 [29] Willson, 2018 [31] | 500 mg | increase nervousness, anxiety, excitement, irritability, nausea, paresthesia, tremor, perspiration, palpitations, restlessness, possibly dizziness |
| Higgins-Babu, 2013 [37] | 400 mg/day | safe dose for adults |
| Nowak-Goslinski, 2019 [38] Turnbull et al., 2017 [39] | ~600 mg/day | reversible cardiovascular effects |
| Bedi et al., 2014 [33] Alsunni, 2015 [34] | 200 mg | nervousness, insomnia, problems of digestion, muscle cramps, and periods of unreasonable alertness muscle cramps, and periods of unreasonable alertness |
| Willson, 2018 [31] | ≤1000 mg/day | toxic symptoms hyperactivity, headaches, nausea, dizyness, trembling, spasm, extrasystole, tachycardia |
| Willson, 2018 [31] | ~2000 mg/day | toxic symptoms, requires hospitalization, ventricular fibrillation cardiovascular symptoms |
| Willson, 2018 [31] | ~3000 mg/day | lethal |
| Authors | Dose (mg/kg) | Effects |
| Mielgo-Ayuso et al., 2019. [5] Pickering-Kiely 2018 [35] Goldstein et al., 2010 [9] | 3–6 mg/kg | positive effects increase physical performance |
| Mielgo-Ayuso et al., 2019 [5] | 9–13 mg/kg | no positive effect in physical performance |
| Graham et al., 1995 [28] Spiret, 2014 [21] | ~10–13 mg/kg | troubling side effects of gastrointestinal upset, nervousness, mental confusion, inability to focus, and disturbed sleeping |
| Kaplan et al., 1997 [29] Kerrigan-Lingsey, 2005 [30] Willson, 2018 [31] | ~7–10 mg/kg | chills, flushing, nausea, headache, palpitations and tremor |
| Graham et al., 1995 [28] Spiret, 2014 [21] | 3 mg/kg | no negative effect in physiological responses |
| Authors | N | Dose (mg/day) | Effects |
|---|---|---|---|
| Rashti et al., 2009 [65] | n = 10 | ED (230 mg) | no change in mood alertness and concentration |
| Alford et al., 2001 [53] | not given | increased aerobic and anaerobic performance | |
| Seifert et al., 2011 [19] | not given | 12.5–100 mg/day | increased aerobic capacity improved reaction time |
| Authors | Dose (mg/kg) | Effects | |
| Mielgo-Ayuso et al., 2019 [5]; Pickering- Kiely, 2018 [35]; Goldstein et al., 2010 [9] | n = 20 | 3–6 mg/kg | positive effects increased physical performance |
| Mielgo-Ayuso et al., 2019 [5] | not given | 9–13 mg/kg | no positive effect in physical performance |
| Spiret, 2014 [21] | not given | ~10–13 mg/kg |
ergogenic effects in endurance-type activities increased heart rates higher blood lactate levels |
| Paton et al., 2015 [73] Mielgo-Ayuso, 2019 [5] | n = 20 | 3–4 mg/kg | improves mean and sprint performance power in male and female cyclists |
| Suvi et al., 2016 [74] Mielgo-Ayuso, 2019 [5] | n = 23 | 6 mg/kg | increases HR and blood lactate reduces ratings of perceived exertion and fatigue in males no positive effect in endurance capacity |
| Skinner et al., 2019 [75] | n = 27 | 3 mg/kg | enhanced endurance exercise performance in women |
| Chen et al., 2015 [80] Mielgo-Ayuso et al., 2019 [5] | n = 20 | 6 mg/kg | ergogenic effect of caffeine on muscle power and muscle endurance |
| Authors | Country/n | Years | ED/EDwA | Significant Correlations with Different Symptoms/Syndromes |
|---|---|---|---|---|
| Huhtinen et al., 2013 [113] | Iceland n = 11,267 | 10–12 years | ED | headaches, sleep disturbances, fatigue |
| Kristjansson et al., 2014 [120] | Finnland n = 5840 in 2007 | 12–18 years | ED | stomach pains headaches insomnia |
| Gradvohl et al., 2015 [138] | Hungary n = 1066 in 2013 | students 18–24 years | EDwA | Binge drinking |
| Park et al., 2016 [122] | Korea n = 68,043 | 12–18 years | ED | sleep dissatisfaction severe stress depressive mood suicide attempts |
| Soós et al., 2016 [131] | Hungary n = 1495 | 10–26 years | ED EDwA | rapid HR insomnia weakness, shiver headache |
| Kim et al., 2017 [43] | Korea n = 121,106 in 2014–2015 | 13–18 years | ED | stress inadequate sleep low school performance suicide attempts |
| Scalase et al., 2017 [139] | Italy n = 30,588 in 2016 | 15–18 years | ED EDwA | daily smoking binge drinking use of cannabis and other psychotropic drugs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soós, R.; Gyebrovszki, Á.; Tóth, Á.; Jeges, S.; Wilhelm, M. Effects of Caffeine and Caffeinated Beverages in Children, Adolescents and Young Adults: Short Review. Int. J. Environ. Res. Public Health 2021, 18, 12389. https://doi.org/10.3390/ijerph182312389
Soós R, Gyebrovszki Á, Tóth Á, Jeges S, Wilhelm M. Effects of Caffeine and Caffeinated Beverages in Children, Adolescents and Young Adults: Short Review. International Journal of Environmental Research and Public Health. 2021; 18(23):12389. https://doi.org/10.3390/ijerph182312389
Chicago/Turabian StyleSoós, Rita, Ádám Gyebrovszki, Ákos Tóth, Sára Jeges, and Márta Wilhelm. 2021. "Effects of Caffeine and Caffeinated Beverages in Children, Adolescents and Young Adults: Short Review" International Journal of Environmental Research and Public Health 18, no. 23: 12389. https://doi.org/10.3390/ijerph182312389