
Midwives’ Experiences with and Perspectives on Online (Nutritional) Counselling and mHealth Applications for Pregnant Women; an Explorative Qualitative Study

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment and Data Collection
2.3. Analysis
3. Results
3.1. Midwives and Nutritional Counselling
Now the emphasis is on what you are not allowed to do and I find that annoying. ... with a few adjustments you can just do anything. I would like that, if it is approached in a much more positive way.(P4)
Well, then you are actually taking over the work of a dietician, yes, and I think it would be better to leave that to the specialists.(P9)
3.2. Midwives’ Experiences with mHealth
But in addition to this digitalisation, it is still very important that we continue to see the women and maintain physical contact. Especially the vulnerable group.(P4)
I always read the newsletters from our professionals’ organisation, but I cannot recall how much has been said about new technology regarding nutrition in recent months.(P5)
3.3. Future of mHealth in Midwifery Practices
You just see that these educated women do things like this, and like and download apps like that, and of course that’s not the group where the greatest health gains can be made. And that is of course just really very difficult about these kinds of innovations and digital things. We just don’t get to the Syrian women in the disadvantaged neighbourhood, I really don’t see that happening in the next ten years and I find that poignant.(P10)
No, where my fear is, it is that for some people it can lead to more loneliness, indeed to a healthier diet, but to more loneliness.(P11)
It’s just very easy to open the app instead of going all the way to Google.(P5)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
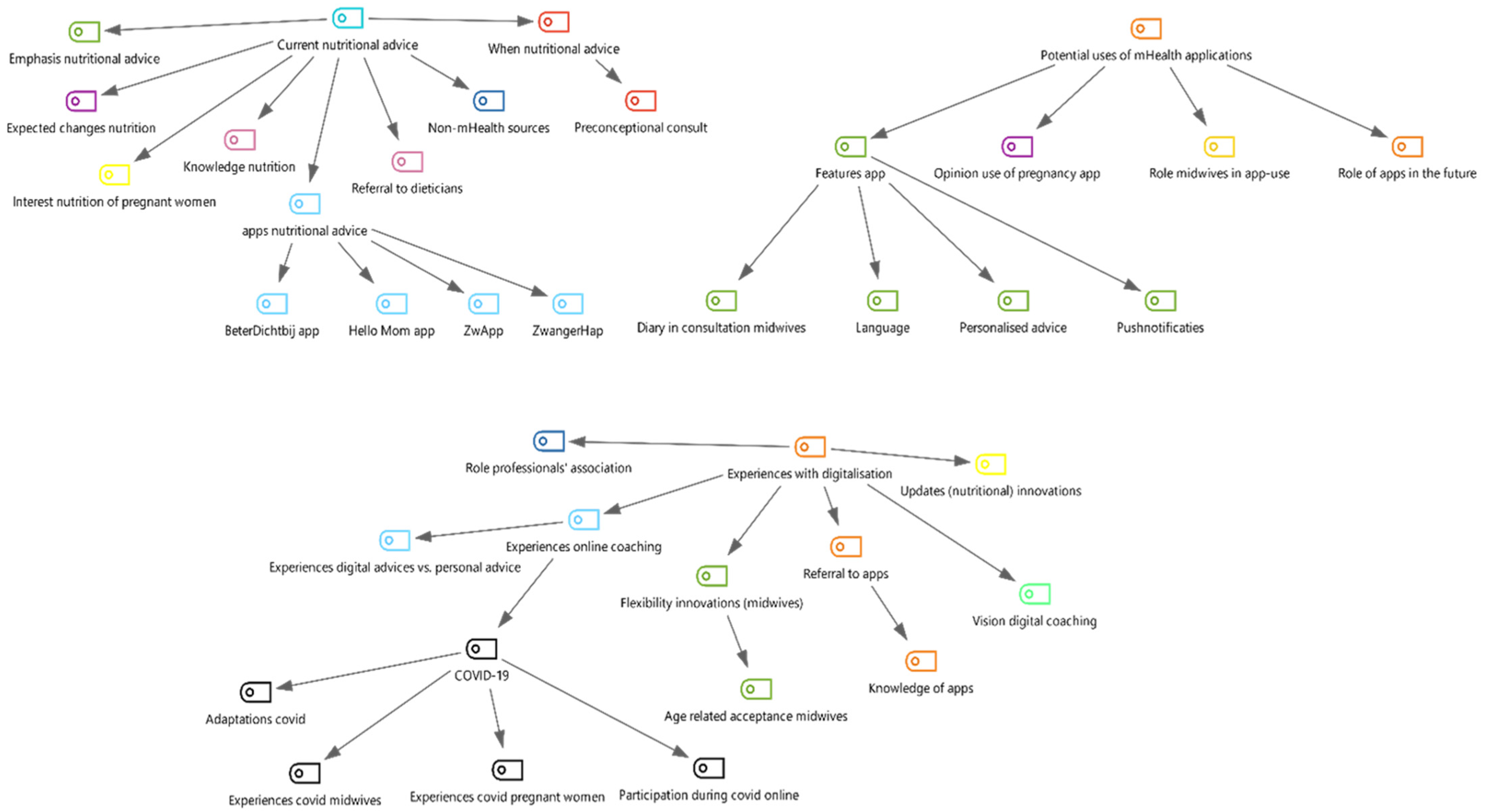
| Codes | Sub-Codes |
|---|---|
| Current nutritional advice | Pre-conceptional consult When nutritional advice Pregnant women’s interest in nutrition |
| Emphasis nutritional advice Nutritional knowledge Referral to dietician | |
| Non-mHealth sources Nutritional apps | |
| Expected changes nutrition | |
| Experiences with digitalisation | Role professionals’ association Experiences online counselling Experiences digital advice vs. personal advice COVID-19 |
| Updates (nutritional) innovations Flexibility and age-related acceptance of innovations | |
| Referral to apps Knowledge of apps | |
| Vision digital counselling | |
| Potential uses for mHealth apps | Opinion use of pregnancy app |
| Features apps | |
| Role midwives in app-use | |
| Role of apps in the future |

References
- Kind, K.L.; Moore, V.M.; Davies, M.J. Diet around conception and during pregnancy—Effects on fetal and neonatal outcomes. Reprod. Biomed. Online 2006, 12, 532–541. [Google Scholar] [CrossRef]
- Perazzolo, S.; Hirschmugl, B.; Wadsack, C.; Desoye, G.; Lewis, R.; Sengers, B.G. The influence of placental metabolism on fatty acid transfer to the fetus. J. Lipid Res. 2017, 58, 443–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simister, N.E.; Story, C.M. Human placental Fc receptors and the transmission of antibodies from mother to fetus. J. Reprod. Immunol. 1997, 37, 1–23. [Google Scholar] [CrossRef]
- Rush, D. Effects of changes in protein and calorie intake during pregnancy on the growth of the human fetus. In Effectiveness and Satisfaction in Antenatal Care; Enkin, M., Chalmers, I., Eds.; Oxford University Press: Oxford, UK, 1982; p. 92. [Google Scholar]
- Looman, M.; Berg, C.V.D.; Geelen, A.; Samlal, R.A.K.; Heijligenberg, R.; Gunnewiek, J.M.T.K.; Balvers, M.G.J.; Leendertz-Eggen, C.L.; Wijnberger, L.D.E.; Feskens, E.J.M.; et al. Supplement use and dietary sources of folate, vitamin D, and n-3 fatty acids during preconception: The GLIMP2 study. Nutrients 2018, 10, 962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ter Borg, S.; Koopman, N.; Verkaik-Kloosterman, J. Food consumption, nutrient intake and status during the first 1000 days of life in the netherlands: A systematic review. Nutrients 2019, 11, 860. [Google Scholar] [CrossRef] [Green Version]
- Brouwer-Brolsma, E.M.; Vrijkotte, T.G.M.; Feskens, E.J.M. Maternal vitamin D concentrations are associated with faster childhood reaction time and response speed, but not with motor fluency and flexibility, at the age of 5–6 years: The Amsterdam Born Children and their Development (ABCD) Study. Br. J. Nutr. 2018, 120, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Looman, M.; Geelen, A.; Samlal, R.A.K.; Heijligenberg, R.; Gunnewiek, J.M.T.K.; Balvers, M.G.J.; Wijnberger, L.D.E.; Brouwer-Brolsma, E.M.; Feskens, E.J.M. Changes in micronutrient intake and status, diet quality and glucose tolerance from preconception to the second trimester of pregnancy. Nutrients 2019, 11, 460. [Google Scholar] [CrossRef] [Green Version]
- Naninck, E.F.G.; Stijger, P.C.; Brouwer-Brolsma, E.M. The importance of maternal folate status for brain development and function of offspring. Adv. Nutr. 2019, 10, 502–519. [Google Scholar] [CrossRef] [PubMed]
- Pet, M.A.; Brouwer-Brolsma, E.M. The impact of maternal vitamin d status on offspring brain development and function: A systematic review. Adv. Nutr. 2016, 7, 665–678. [Google Scholar] [CrossRef] [Green Version]
- Brouwer-Brolsma, E.; Van De Rest, O.; Godschalk, R.; Zeegers, M.; Gielen, M.; De Groot, R. Associations between maternal long-chain polyunsaturated fatty acid concentrations and child cognition at 7 years of age: The MEFAB birth cohort. Prostaglandin Leukot. Essent. Fat. Acids 2017, 126, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Eurostat. Individuals—Mobile Internet Access [Internet]. Available online: http://appsso.eurostat.ec.europa.eu/nui/show.do?query=BOOKMARK_DS-056936_QID_3FA90C8F_UID_-F171EB0&layout=TIME,C,X,0;GEO,L,Y,0;INDIC_IS,L,Z,0;UNIT,L,Z,1;IND_TYPE,L,Z,2;INDICATORS,C,Z,3;&zSelection=DS-056936INDIC_IS,I_IUMP;DS-056936UNIT,PC_IND;DS-056936IN (accessed on 31 August 2020).
- Buijink, A.W.G.; Visser, B.J.; Marshall, L. Medical apps for smartphones: Lack of evidence undermines quality and safety. Evid.-Based Med. 2013, 18, 90–92. [Google Scholar] [CrossRef]
- Brown, H.M.; Bucher, T.; Collins, C.E.; Rollo, M.E. A review of pregnancy iPhone apps assessing their quality, inclusion of behaviour change techniques, and nutrition information. Matern. Child Nutr. 2019, 15, e12768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgart, D.C. Smartphones in clinical practice, medical education, and research. Arch. Intern. Med. 2011, 171, 1294. [Google Scholar] [CrossRef] [Green Version]
- Khamisy-Farah, R.; Furstenau, L.; Kong, J.; Wu, J.; Bragazzi, N. Gynecology meets big data in the disruptive innovation medical era: State-of-art and future prospects. Int. J. Environ. Res. Public Heal. 2021, 18, 5058. [Google Scholar] [CrossRef] [PubMed]
- Lupton, D.; Pedersen, S. An Australian survey of women’s use of pregnancy and parenting apps. Women Birth 2016, 29, 368–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripp, N.; Hainey, K.; Liu, A.; Poulton, A.; Peek, M.; Kim, J.; Nanan, R. An emerging model of maternity care: Smartphone, midwife, doctor? Women Birth 2014, 27, 64–67. [Google Scholar] [CrossRef]
- Van Dijk, M.R.; Huijgen, N.A.; Willemsen, S.P.; Laven, J.S.; Steegers, E.A.; Steegers-Theunissen, R.P. Impact of an mHealth platform for pregnancy on nutrition and lifestyle of the reproductive population: A survey. JMIR mHealth uHealth 2016, 4, e53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainscough, K.M.; O’Brien, E.C.; Lindsay, K.L.; Kennelly, M.A.; O’Sullivan, E.J.; O’Brien, O.A.; McCarthy, M.; De Vito, G.; McAuliffe, F.M. Nutrition, behavior change and physical activity outcomes from the PEARS RCT—An mHealth-supported, lifestyle intervention among pregnant women with overweight and obesity. Front. Endocrinol. (Lausanne) 2020, 10, 938. [Google Scholar] [CrossRef]
- Overdijkink, S.B.; Velu, A.V.; Rosman, A.N.; Van Beukering, M.D.; Kok, M.; Steegers-Theunissen, R.P. The usability and effectiveness of mobile health technology–based lifestyle and medical intervention apps supporting health care during pregnancy: Systematic review. JMIR mHealth uHealth 2018, 6, e109. [Google Scholar] [CrossRef] [Green Version]
- Dodd, J.M.; Louise, J.; Cramp, C.; Grivell, R.M.; Moran, L.J.; Deussen, A.R. Evaluation of a smartphone nutrition and physical activity application to provide lifestyle advice to pregnant women: The SNAPP randomised trial. Matern. Child Nutr. 2018, 14, e12502. [Google Scholar] [CrossRef] [Green Version]
- Free, C.; Phillips, G.; Watson, L.; Galli, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technologies to improve health care service delivery processes: A systematic review and meta-analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical framework. Implement Sci. 2012, 7, 1–17. [Google Scholar]
- Michie, S.; Johnston, M.; Abraham, C.; Lawton, R.; Parker, D.; Walker, A. Making psychological theory useful for implementing evidence based practice: A consensus approach. Qual. Saf. Heal. Care 2005, 14, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, J.J.; O’Connor, D.; Curran, J. Theories of behaviour change synthesised into a set of theoretical groupings: Introducing a thematic series on the theoretical domains framework. Implement Sci. 2012, 7, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sissions, A.; Grant, A.; Kirkland, A.; Currie, S. Using the theoretical domains framework to explore primary health care practitioner’s perspectives and experiences of preconception physical activity guidance and promotion. Psychol. Heal. Med. 2020, 25, 844–854. [Google Scholar] [CrossRef]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Francis, J.J.; Johnston, M.; Robertson, C.; Glidewell, L.; Entwistle, V.; Eccles, M.P.; Grimshaw, J. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Heal. 2010, 25, 1229–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jersey, S.J.; Nicholson, J.M.; Callaway, L.K.; Daniels, L.A. An observational study of nutrition and physical activity behaviours, knowledge, and advice in pregnancy. BMC Pregnancy Childbirth 2013, 13, 115. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.; Kennedy, L.; Tocque, K.; Jones, S. Eating for 1, Healthy and Active for 2; feasibility of delivering novel, compact training for midwives to build knowledge and confidence in giving nutrition, physical activity and weight management advice during pregnancy. BMC Pregnancy Childbirth 2014, 14, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasiloglou, M.F.; Christodoulidis, S.; Reber, E.; Stathopoulou, T.; Lu, Y.; Stanga, Z.; Mougiakakou, S. What healthcare professionals think of ″Nutrition & Diet″ apps: An international survey. Nutrients 2020, 12, 2214. [Google Scholar] [CrossRef]
- Willcox, J.C.; Van Der Pligt, P.; Ball, K.; Wilkinson, S.A.; Lappas, M.; McCarthy, E.A.; Campbell, K.J. Views of women and health professionals on mHealth lifestyle interventions in pregnancy: A qualitative investigation. JMIR mHealth uHealth 2015, 3, e99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verkasalo, H.; Lopez-Nicolas, C.; Molina-Castillo, F.-J.; Bouwman, H. Analysis of users and non-users of smartphone applications. Telemat. Inform. 2010, 27, 242–255. [Google Scholar] [CrossRef]
- Chang, T.R.; Kaasinen, E.; Kaipainen, K. What influences users’ decisions to take apps into use? A framework for evaluating persuasive and engaging design in mobile apps for well-being. In Proceedings of the 11th International Conference on Mobile and Ubiquitous Multimedia, Ulm, Germany, 4–6 December 2012; MUM: New York, NY, USA, 2012. [Google Scholar]
- Dennison, L.; Morrison, L.; Conway, G.; Yardley, L. Opportunities and challenges for smartphone applications in supporting health behavior change: Qualitative study. J. Med. Internet Res. 2013, 15, e86. [Google Scholar] [CrossRef] [PubMed]
- Brouwer-Brolsma, E.M.; Lucassen, D.; de Rijk, M.G.; Slotegraaf, A.; Perenboom, C.; Borgonjen, K.; Siebelink, E.; Feskens, E.J.M.; de Vries, J.H.M. Dietary intake assessment: From traditional paper-pencil questionnaires to technology-based tools. In Environmental Software Systems Data Science in Action; Athanasiadis, I.N., Frysinger, S.P., Schimak, G., Knibbe, W.J., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 7–23. [Google Scholar]
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, G.; Kim, J.; Lin, S.; Hua, J.; Seto, E. A focused review of smartphone diet-tracking apps: Usability, functionality, coherence with behavior change theory, and comparative validity of nutrient intake and energy estimates. JMIR mHealth uHealth 2019, 7, e9232. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.-H.; Andrade, J.E.; Chapman-Novakofski, K.M. The use of mobile apps to improve nutrition outcomes: A systematic literature review. J. Telemed. Telecare 2015, 21, 243–253. [Google Scholar] [CrossRef]
- Rogers, Y.; Sharp, H.; Preece, J. Interaction Design: Beyond Human-Computer Interaction; John Wiley & Sons: New York, NY, USA, 2011. [Google Scholar]
- Chen, J.; Lieffers, J.; Bauman, A.; Hanning, R.; Allman-Farinelli, M. Designing Health apps to support dietetic professional practice and their patients: Qualitative results from an international survey. JMIR mHealth uHealth 2017, 5, e40. [Google Scholar] [CrossRef]
- De Leo, A.; Bayes, S.; Bloxsome, D.; Butt, J. Exploring the usability of the COM-B model and Theoretical Domains Framework (TDF) to define the helpers of and hindrances to evidence-based practice in midwifery. Implement Sci. Commun. 2021, 2, 1–8. [Google Scholar] [CrossRef]
| Participant Number | Age in Years | Workplace | Employment | Work Area |
|---|---|---|---|---|
| P1 | 38 | Primary care | Full time | Rural |
| P2 | 53 | Hospital | Full time | Urban |
| P3 | 27 | Primary care | Full time | Rural |
| P4 | 35 | Hospital | Full time | Urban |
| P5 | 22 | Primary care | Full time | Urban |
| P6 | 60 | Primary care | Full time | Urban |
| P7 | 21 | Primary care | Full time | Urban |
| P8 | 29 | Combined | Full time | Urban |
| P9 | 23 | Primary care | Full time | Urban |
| P10 | 25 | Primary care | Part-time | Urban |
| P11 | 49 | Primary care | Part-time | Rural |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wit, R.F.; Lucassen, D.A.; Beulen, Y.H.; Faessen, J.P.M.; Bos-de Vos, M.; van Dongen, J.M.; Feskens, E.J.M.; Wagemakers, A.; Brouwer-Brolsma, E.M. Midwives’ Experiences with and Perspectives on Online (Nutritional) Counselling and mHealth Applications for Pregnant Women; an Explorative Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 6733. https://doi.org/10.3390/ijerph18136733
Wit RF, Lucassen DA, Beulen YH, Faessen JPM, Bos-de Vos M, van Dongen JM, Feskens EJM, Wagemakers A, Brouwer-Brolsma EM. Midwives’ Experiences with and Perspectives on Online (Nutritional) Counselling and mHealth Applications for Pregnant Women; an Explorative Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(13):6733. https://doi.org/10.3390/ijerph18136733
Chicago/Turabian StyleWit, Renate F., Desiree A. Lucassen, Yvette H. Beulen, Janine P. M. Faessen, Marina Bos-de Vos, Johanna M. van Dongen, Edith J. M. Feskens, Annemarie Wagemakers, and Elske M. Brouwer-Brolsma. 2021. "Midwives’ Experiences with and Perspectives on Online (Nutritional) Counselling and mHealth Applications for Pregnant Women; an Explorative Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 13: 6733. https://doi.org/10.3390/ijerph18136733