
Accessing Voluntary HIV Testing in the Construction Industry: A Qualitative Analysis of Employee Interviews from the Test@Work Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Workplace Health Checks
2.3. Participants
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Qualitative Interviews
I thought it was really good, I think it is not something that you would go and naturally ask for, can I have one of those tests so if it is offered more people are likely to say yes because it is a good thing to get checked. (White male, age 26)
Well I think a lot of people would be afraid to get HIV tests done so I think it is good that it is being promoted more and more people can do it, get themselves checked before it is too late, so it is a good idea. (White male, age 38)
Just because… again just because it was available, I don’t feel I have any symptoms of it but erm you know I just thought why not, it’s here and I wouldn’t be sure where else to go? (White male, age 30)
Because you don’t have time with work hours…we don’t have time to go for check ups or see how you’re getting on at home so it is quite nice to be able to go and do it and not have to worry about not getting paid and everything else so that is really the reason why, make sure that I am healthy, and I am not too bad. (White male, age 48)
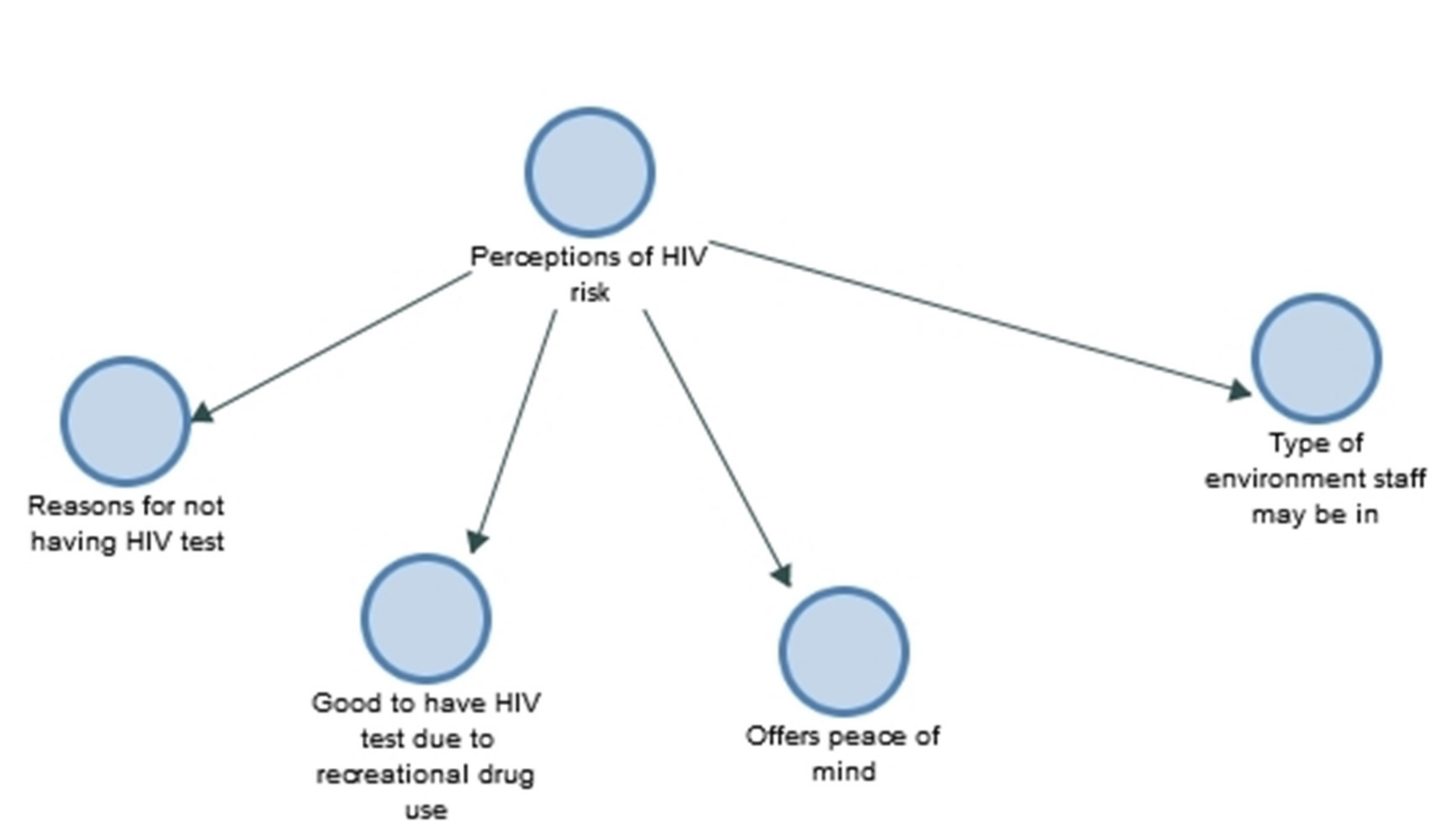
I say I think it is good to have it...Because it is not like you are offered it at the doctors or anything, you have to go and seek it but not… it is not offered, do you know what I mean? (White male, age 39)
It was good, it was nice and quick, it doesn’t impact much on the day which for sites like this is important, I thought that was quite good, everything else I was happy with. (White male, age 34)
I think the range of options that have been offered have been very good and a bit surprised by the HIV test, I didn’t realize that was going to be there but while it is there, why not use it. (White male, age 57)
I do think it is a really good idea erm and the only thing I would say is the HIV checks I think is great as well erm however say if somebody did have it, it would be really awkward to walk out because you see by their facial expressions, they would be like oh god like nightmare so that might be awkward in an office-based environment I would say. (White female, age 20)
Yes, well I don’t know, I have always understood HIV is for gays and things like that do you know what I mean? I might be wrong but that is how I have always looked at it you know I am not gay why should I need an HIV? (White male, age 57)
Yes, I had never had it done but I have been with my wife for 10 years now so although I am not sleeping with multiple partners it is just always something which is good to know. (White male, age 36)
I love sex, with women erm… and without condoms so I needed the HIV test. (White male, age 28)
I think it is positive, erm a lot of men on a building site are men, men who like to have a few drinks and might participate in recreational drugs erm… frequent sexual partners, so I think it is a very good thing for them to have that check. (Black male, age 52)
Just in general the HIV test, we do a lot of council work and we come across needles all around…So I had it [the HIV test] done just because I have never had that opportunity before. (White male, age 47)
There is a lot of blokes out there that don’t do anything about it until they have to. I think you should know, really, you should know what sort of physical health you’re in, especially in the job we do. (White male, age 47)
Erm just because it was here, and I thought I never normally go to the doctors… I don’t need to go to the doctors so I don’t go, and I don’t really weigh myself or know anything about any health issues that I might have or anything. (White male, age 27)
You don’t have time with work hours and studies we don’t have time to go for check-ups or see how you’re getting on at home, so it is quite nice to be able to go and do it and not have to worry about not getting paid and everything else. (White male, age 35)
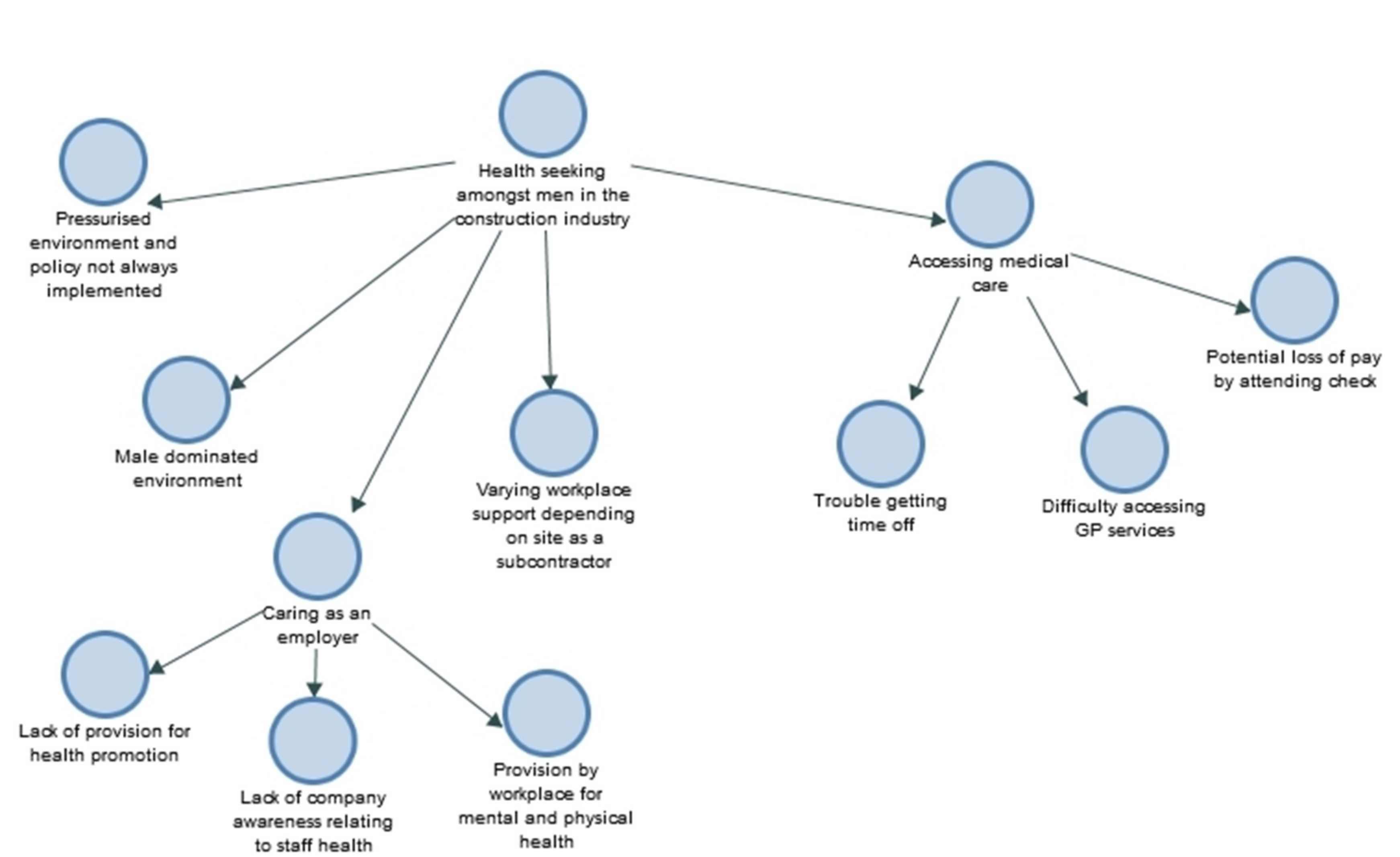
Due to the current economy social climate of Britain, it is tough for me to get in to my doctors…I would need to book time off work, and it would just become a bit stressful… well for me it is stressful so you know I just avoid the doctors like the plague to be honest with you. (White male, age 27)
So we have got mental health first aiders available, we have got different safe call numbers like confidential numbers available for people to use, we do run days like this or like health MOT days, I suppose we could be better at it maybe by I don’t know buying things that they need or having initiatives or making them take breaks for exercise, I don’t know, even for myself because I work quite long hours and I travel a lot, I come from Walsall, erm yes so it is quite a long commute so yes. (White female, age 27)
Especially with this self-employment game it is like… you know you are kind of out here fending for yourself, so it is kind of good to you know just have that… because obviously you have got corporate companies that have people on the books and they tend to like look after their own… some places do, some places don’t but you know being self-employed you kind of… in the long grass on your own you know. (White male, age 32)
Erm - it depends for me because I work from site-to-site different erm contractors because I subcontract so it varies on the employer (White male, age 33)
I think it is vital really because I think well especially being in construction it is a male-dominated environment, I think a lot of men sort of have that stigma around attending a GP or somewhere to find out about their health in general. (White male, age 25)
I think more needs to be done by employers because I think particularly in the construction industry it is almost an attitude of man up or ship out type of thing and there is too much aggression in the workplace, I think. (White male, age 54)
There certainly is you know they treat us poorly and they will not get a lot out of us and guys are going off sick because the pressure…the bullying within the management filtering down to us…(White male, age 52)
Erm yes I think it [the health check] is good….but there is… a hypocrisy...is it ironic? I don’t know, that work is the biggest cause of stress I think for a lot of instances so I guess it is good that they are allowing us to do it – but working culture probably needs to change I think at the minute, in this industry it does, it is ridiculous. (South Asian male, age 40)
Because my boss gave me time off to come in and do it, if not I probably wouldn’t have come. (White male, age 22)
I think it is a good thing to do, it really is a good thing to do, we don’t do enough of it. It is the first one I have done here in 18 months, but my previous employer had done them a few times. Especially in construction where it is a male orientated industry, we and we’re not very good about health and going to the doctors, I think as men so… I am certainly not……and I think the HIV testing is a good thing as well because as you said a lot of people won’t be thinking that is even an issue when actually they could have it without even realizing so. (White female, age 26)
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV & AIDS Statistics: 2020 Fact Sheet; UNAIDS: Geneva, Switzerland, 2020. [Google Scholar]
- Public Health England. HIV in the United Kingdom: Towards Zero 2030; Public Health England: London, UK, 2020.
- Burton, J. WHO Healthy Workplace Framework and Model: Background and Supporting Literatureand Practices; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Poscia, A.; Moscato, U.; La Milia, D.I.; Milovanovic, S.; Stojanovic, J.; Borghini, A.; Collamati, A.; Ricciardi, G.; Magnavita, N. Workplace health promotion for older workers: A systematic literature review. BMC Health Serv. Res. 2016, 16 (Suppl 5), 329. [Google Scholar] [CrossRef] [Green Version]
- Proper, K.I.; van Oostrom, S.H. The effectiveness of workplace health promotion interventions on physical and mental health outcomes—A systematic review of reviews. Scand. J. Work Environ. Health 2019, 45, 546–559. [Google Scholar] [CrossRef] [Green Version]
- Rongen, A.; Robroek, S.J.W.; van Lenthe, F.J.; Burdorf, A. Workplace health promotion: A meta-analysis of effectiveness. Am. J. Prev. Med. 2013, 44, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Bennett, E.; Mark, E.B. Evaluation of occupational health checks for hospital employees. Int. J. Workplace Health Manag. 2014, 7, 247–266. [Google Scholar] [CrossRef]
- Bali, V.; Yermilov, I.; Koyama, A.; Legorreta, A.P. Secondary prevention of diabetes through workplace health screening. Occup. Med. 2018, 68, 610–616. [Google Scholar] [CrossRef]
- van Doorn, D.; Richardson, N.; Osborne, A.; Blake, C. The impact of a workplace cardiovascular health screening programme ‘Farmers Have Hearts’ on health behaviour change among Irish farmers. Work 2019, 63, 113–123. [Google Scholar] [CrossRef]
- Blake, H.; Banerjee, A.; Evans, C. Employer attitudes towards general health checks and HIV testing in the workplace. Public Health 2018, 156, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Bowen, P.; Govender, R.; Edwards, P.; Cattell, K. HIV testing of construction workers in the Western Cape, South Africa. Aids Care 2015, 27, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Bowen, P.; Govender, R.; Edwards, P.; Lake, A. HIV infection in the South African construction industry. Psychol. Health Med. 2018, 23, 612–618. [Google Scholar] [CrossRef]
- Bowen, P.; Govender, R.; Edwards, P.J.; Cattell, K. An explanatory model of attitudinal fear of HIV/AIDS testing in the construction industry. Eng. Constr. Archit. Manag. 2016, 23, 92–112. [Google Scholar] [CrossRef]
- Bowen, P.A.; Govender, R.; Edwards, P.J.; Cattell, K. An integrated model of HIV/AIDS testing behaviour in the construction industry. Constr. Manag. Econ. 2014, 32, 1106–1129. [Google Scholar] [CrossRef]
- Bowen, P.; Cattell, K.; Edwards, P.J.; Marks, J. Perceptions of HIV/AIDS policies and treatment programmes by Western Cape construction firms. Constr. Manag. Econ. 2010, 28, 997–1006. [Google Scholar] [CrossRef]
- Blake, H.; Hussain, B.; Hand, J.; Rowlands, D.; Juma, A.; Evans, C. Employee perceptions of a workplace HIV testing intervention. Int. J. Workplace Health Manag. 2018, 11, 333–348. [Google Scholar] [CrossRef]
- Sorensen, G.; Landsbergis, P.; Hammer, L.; Amick, B.C., III; Linnan, L.; Yancey, A.; Welch, L.S.; Goetzel, R.Z.; Flannery, K.M.; Pratt, C.; et al. Preventing chronic disease in the workplace: A workshop report and recommendations. Am. J. Public Health 2011, 101, S196–S207. [Google Scholar] [CrossRef] [PubMed]
- Kouvonen, A.; Kivimäki, M.; Virtanen, M.; Pentti, J.; Vahtera, J. Work stress, smoking status, and smoking intensity: An observational study of 46,190 employees. J. Epidemiol. Community Health 2005, 59, 63–69. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health Policies and Programmes in the Workplace; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- The Chartered Institute of Building. Inclusivity: The Changing Role of Women in the Construction Workforce. Berkshire, UK. Available online: https://www.ciob.org/sites/default/files/CIOB%20research%20-%20The%20Changing%20Role%20of%20Women%20in%20the%20Construction%20Workforce.pdf (accessed on 27 March 2021).
- Boal, W.L.; Li, J.; Dong, X.S.; Sussell, A. Health Risk Behavior Profile of Construction Workers, 32 States, 2013–2016. J. Occup. Environ. Med. 2020, 62, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Ompad, D.C.; Gershon, R.R.; Sandh, S.; Acosta, P.; Palamar, J.J. Construction trade and extraction workers: A population at high risk for drug use in the United States, 2005–2014. Drug Alcohol Depend. 2019, 205, 107640. [Google Scholar] [CrossRef]
- Kassa, M.; Tesfaye, E.; Alamrew, Z. Risky Sexual Behaviour among Big Construction Enterprise Workers; Bahir Dar City, Amhara Regional State, Northwest Ethiopia. Int. J. Clin. Med. 2013, 2013, 296–303. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, M.; Heikkilä, K.; Jokela, M.; Ferrie, J.E.; Batty, G.D.; Vahtera, J.; Kivimäki, M. Long working hours and coronary heart disease: A systematic review and meta-analysis. Am. J. Epidemiol. 2012, 176, 586–596. [Google Scholar] [CrossRef] [Green Version]
- Kivimäki, M.; Jokela, M.; Nyberg, S.T.; Singh-Manoux, A.; Fransson, E.I.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 2015, 386, 1739–1746. [Google Scholar] [CrossRef] [Green Version]
- Kremers, S.P.J.; de Bruijn, G.-J.; Visscher, T.L.S.; van Mechelen, W.; de Vries, N.K.; Brug, J. Environmental influences on energy balance-related behaviors: A dual-process view. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Stergiou-Kita, M.; Mansfield, E.; Bezo, R.; Colantonio, A.; Garritano, E.; Lafrance, M.; Lewko, J.; Mantis, S.; Moody, J.; Power, N.; et al. Danger zone: Men, masculinity and occupational health and safety in high risk occupations. Saf. Sci. 2015, 80, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groeneveld, I.F.; Proper, K.I.; van der Beek, A.J.; Hildebrandt, V.H.; van Mechelen, W. Short and long term effects of a lifestyle intervention for construction workers at risk for cardiovascular disease: A randomized controlled trial. BMC Public Health 2011, 11, 836. [Google Scholar] [CrossRef] [Green Version]
- Bradshaw, C.; Atkinson, S.; Doody, O. Employing a Qualitative Description Approach in Health Care Research. Glob. Qual. Nurs. Res. 2017, 4, 2333393617742282. [Google Scholar] [CrossRef] [Green Version]
- Thorne, S.; Kirkham, S.R.; MacDonald-Emes, J. Interpretive description: A noncategorical qualitative alternative for developing nursing knowledge. Res. Nurs. Health 1997, 20, 169–177. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Blake, H.; Somerset, S.; Whittingham, K.; Middleton, M.; Yildrim, M.; Evans, C. WHIRL Study: Workplace Health Interprofessional Learning in the Construction Industry. Int. J. Environ. Res. Public Health 2020, 17, 6815. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Somerset, S.; Evans, C. Development and Fidelity Testing of the Test@Work Digital Toolkit for Employers on Workplace Health Checks and Opt-In HIV Testing. Int. J. Environ. Res. Public Health 2020, 17, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Blake, H.; Lloyd, S. The price is right: Making workplace wellness financially sustainable. Int. J. Workplace Health Manag. 2010, 3, 58–69. [Google Scholar] [CrossRef]
- Seaton, C.L.; Bottorff, J.L.; Caperchione, C.M.; Johnson, S.T.; Oliffe, J.L. The Association Between Men’s Heath Behaviors and Interest in Workplace Health Promotion. Workplace Health Saf. 2020, 68, 226–235. [Google Scholar] [CrossRef]
- Wang, Y.; Hunt, K.; Nazareth, I.; Freemantle, N.; Petersen, I. Do men consult less than women? An analysis of routinely collected UK general practice data. BMJ Open 2013, 3, e003320. [Google Scholar] [CrossRef] [Green Version]
- Verdonk, P.; Seesing, H.; de Rijk, A. Doing masculinity, not doing health? A qualitative study among Dutch male employees about health beliefs and workplace physical activity. BMC Public Health 2010, 10, 712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosu, M.B.; Oliffe, J.L.; Kelly, M.T. Nurse Practitioners and Men’s Primary Health Care. Am. J. Men’s Health 2017, 11, 1501–1511. [Google Scholar] [CrossRef] [Green Version]
- Ishimaru, T.; Wada, K.; Smith, D.R. HIV testing and attitudes among the working-age population of Japan: Annual health checkups may offer an effective way forwards. Ind. Health 2016, 54, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Terry, G.; Braun, V. Short but Often Sweet: The Surprising Potential of Qualitative Survey Methods. In Collecting Qualitative Data: A Practical Guide to Textual, Media and Virtual Techniques; Gray, D., Clarke, V., Braun, V., Eds.; Cambridge University Press: Cambridge, UK, 2017; pp. 13–14. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Interview Participants † N = 426 (100%) | |||
|---|---|---|---|
| Men N = 348 (81.7 %) | Women N = 78 (18.3 %) | Total N = 426 (100%) | |
| Age category (years) 17–30 31–40 41–50 51–60 61–70 | 90 (25.9) 98 (28.2) 86 (24.7) 55 (15.8) 19 (5.5) | 16 (20.5) 23 (29.5) 18 (23.1) 18 (23.1) 3 (3.8) | 106 (24.9) 121 (28.4) 104 (24.4) 73 (17.1) 22 (5.2) |
| English as first language Yes No Not stated | 326 (93.7) 19 (5.5) 3 (0.9) | 71 (91.0) 7 (9.0) - | 397 (93.2) 26 (6.1) 3 (0.7) |
| Ethnicity British Irish Any other white background White and black Caribbean Any other mixed background Indian Pakistani Bangladeshi Caribbean African Other Ethnic groups Chinese Not stated | 296 (85.1) 6 (1.7) 11 (3.2) 3 (0.9) 1 (0.3) - 18 (5.2) 2 (0.6) 2 (0.6) 6 (1.7) 1 (0.3) - 2 (0.6) | 56 (71.8) - 6 (7.7) 1 (1.3) 1 (1.3) 1 (1.3) 5 (6.4) - - 5 (6.4) 1 (0.3) 1 (0.3) 1 (0.3) | 352 (82.6) 6 (1.4) 17 (4.0) 4 (0.9) 2 (1.5) 1 (0.2) 23 (5.4) 2 (0.5) 2 (0.5) 11 (2.6) 2 (0.5) 1 (0.2) 3 (0.7) |
| Sexual orientation Heterosexual Homosexual Other Not stated | 337 (96.8) 2 (0.6) 2 (0.6) 7 (2.0) | 78 (100.0) - - - | 415 (97.4) 2 (0.5) 2 (0.5) 7 (1.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somerset, S.; Evans, C.; Blake, H. Accessing Voluntary HIV Testing in the Construction Industry: A Qualitative Analysis of Employee Interviews from the Test@Work Study. Int. J. Environ. Res. Public Health 2021, 18, 4184. https://doi.org/10.3390/ijerph18084184
Somerset S, Evans C, Blake H. Accessing Voluntary HIV Testing in the Construction Industry: A Qualitative Analysis of Employee Interviews from the Test@Work Study. International Journal of Environmental Research and Public Health. 2021; 18(8):4184. https://doi.org/10.3390/ijerph18084184
Chicago/Turabian StyleSomerset, Sarah, Catrin Evans, and Holly Blake. 2021. "Accessing Voluntary HIV Testing in the Construction Industry: A Qualitative Analysis of Employee Interviews from the Test@Work Study" International Journal of Environmental Research and Public Health 18, no. 8: 4184. https://doi.org/10.3390/ijerph18084184