
Occupational Paraquat and Glyphosate Exposure May Decline Renal Functions among Rural Farming Communities in Sri Lanka

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
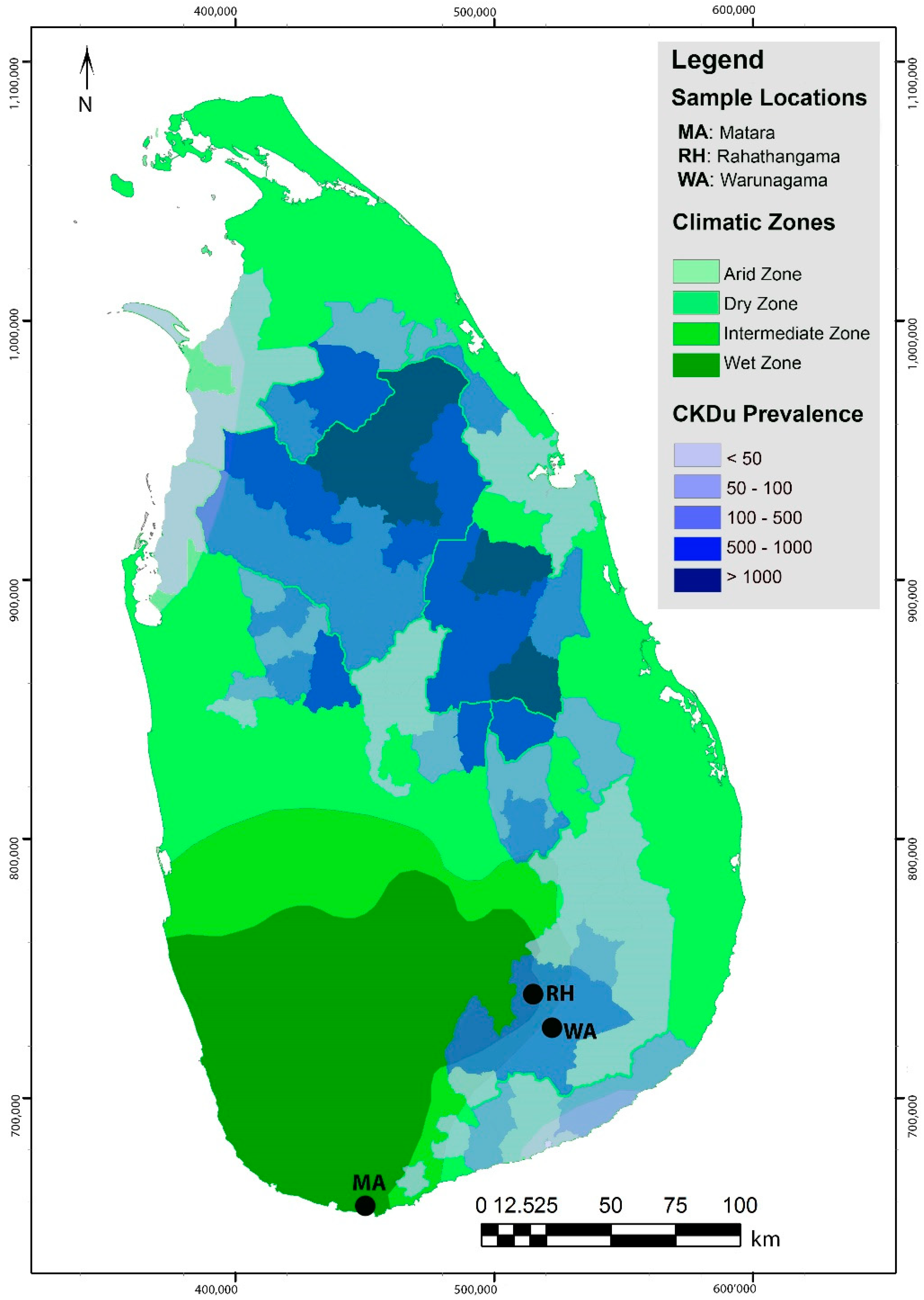
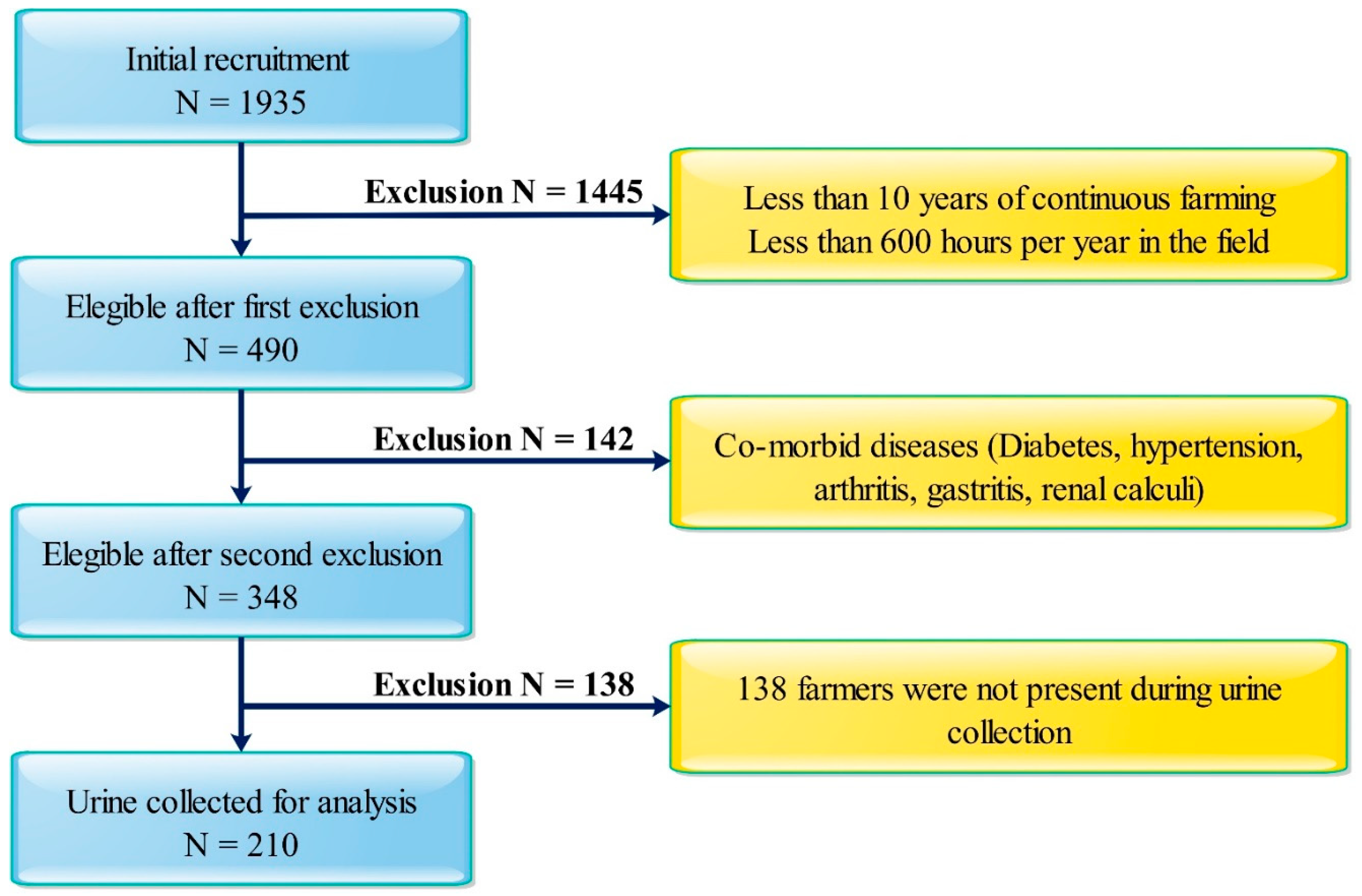
2.1. Study Locations and Populations
2.2. Sample Collection
2.3. Determination of SCr, UCr and eGFR
2.4. Determination of Urinary Microalbumin
2.5. Determination of Urinary Glyphosate and Paraquat
2.6. Measurement of Renal Injury Biomarkers
2.7. Statistical Analysis
2.8. Ethics Statement
3. Results
3.1. Exposure Assessment of Urinary Glyphosate and Paraquat
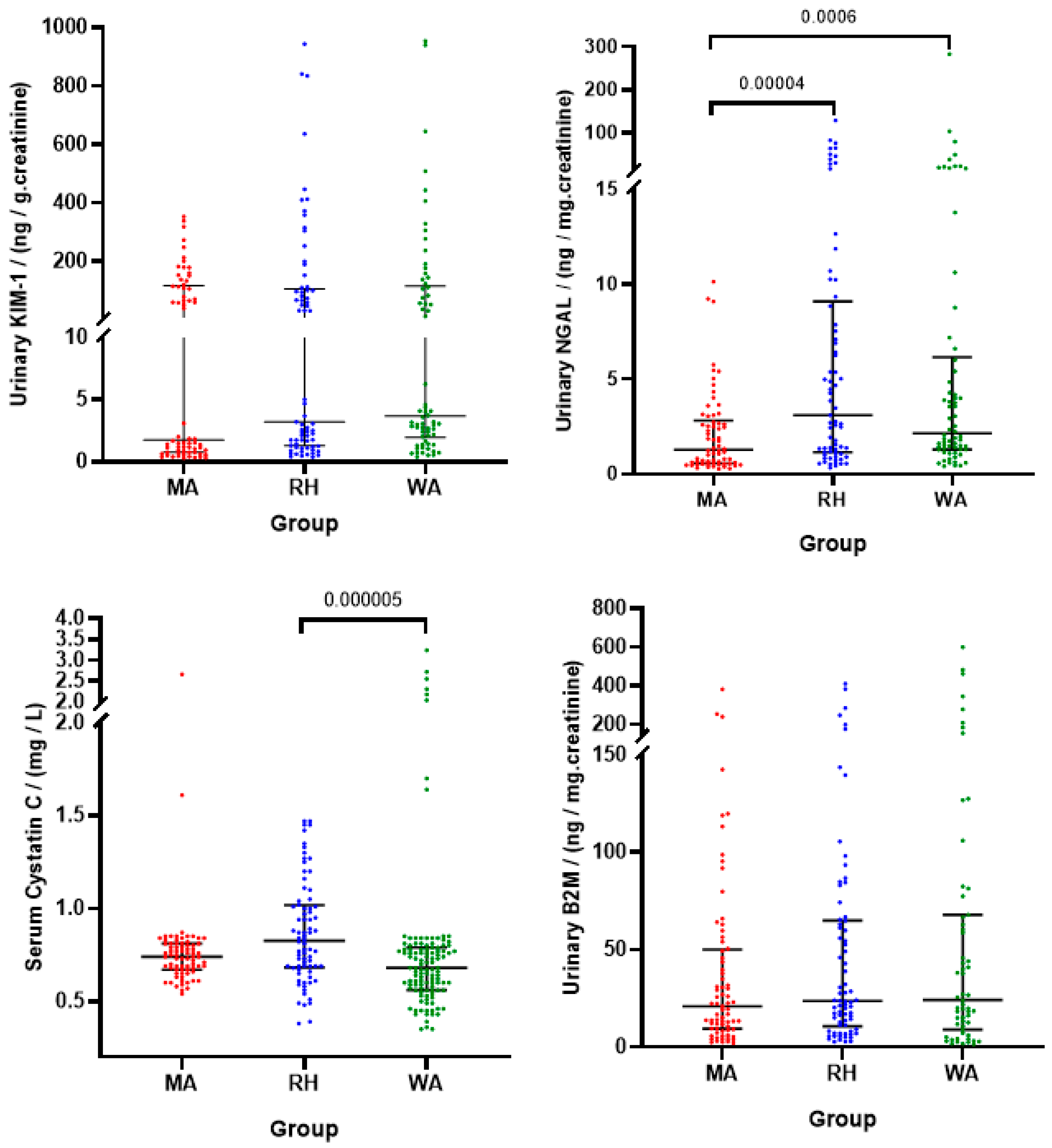
3.2. Assessment of Renal Biomarkers
3.3. Assessment of Kidney Injury Using Urinary Biomarkers
3.4. Association between Herbicide Exposure and Kidney Functions
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CKDu | Chronic Kidney Disease of unknown etiology |
| KIM-1 | Kidney Injury Molecule-1 |
| SCr | Serum Creatinine |
| eGFR | Estimated Glomerular Filtration Rate |
| ACR | Albumin Creatinine Ratio |
| NGAL | Neutrophil Gelatinase-Associated Lipocalin |
| CINAC | Chronic Interstitial Nephritis in Agricultural Communities |
| MEN | Meso American Nephropathy |
| CKD-EPI | CKD-epidemiology collaboration equation |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| HPLC | High-Performance Liquid Chromatography |
References
- Gianessi, L.P. The increasing importance of herbicides in worldwide crop production. Pest Manag. Sci. 2013, 69, 1099–1105. [Google Scholar] [CrossRef]
- Palis, F.G. Research to Impact: Case Studies for Natural Resource Management for Irrigated Rice in Asia; IRRI: Metro Manila, Philippines, 2010. [Google Scholar]
- Zobiole, L.H.S.; de Oliveira, R.S.; Huber, D.M.; Constantin, J.; de Castro, C.; de Oliveira, F.A.; de Oliveira, A. Glyphosate reduces shoot concentrations of mineral nutrients in glyphosate-resistant soybeans. Plant Soil 2010, 328, 57–69. [Google Scholar] [CrossRef]
- Solomon, K.R. Estimated exposure to glyphosate in humans via environmental, occupational, and dietary pathways: An updated review of the scientific literature. Pest Manag. Sci. 2020, 76, 2878–2885. [Google Scholar] [CrossRef]
- Gasnier, C.; Dumont, C.; Benachour, N.; Clair, E.; Chagnon, M.-C.; Séralini, G.-E. Glyphosate-based herbicides are toxic and endocrine disruptors in human cell lines. Toxicology 2009, 262, 184–191. [Google Scholar] [CrossRef]
- Kroncke, A.P.; Willard, M.; Huckabee, H. Assessment of Autism Spectrum Disorder: Critical Issues in Clinical, Forensic and School Settings; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Peper, E. Food for thought: Are Herbicides a Factor for the Increase in Allergies and Autism? Neuroregulation 2015, 2, 162–167. [Google Scholar] [CrossRef] [Green Version]
- Seneff, S.; Samsel, A. Glyphosate, pathways to modern diseases III: Manganese, neurological diseases, and associated pathologies. Surg. Neurol. Int. 2015, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.-T. A review on environmental exposure and health risks of herbicide paraquat. Toxicol. Environ. Chem. 2013, 95, 197–206. [Google Scholar] [CrossRef]
- Hoffer, E.; Taitelman, U. Exposure to Paraquat Through Skin Absorption: Clinical and Laboratory Observations of Accidental Splashing on Healthy Skin of Agricultural Workers. Hum. Toxicol. 1989, 8, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.K. Paraquat: A Review of Worker Exposure in Normal Usage*. Occup. Med. 1980, 30, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Park, E.-K.; Stoecklin-Marois, M.; Koivunen, M.E.; Gee, S.J.; Hammock, B.D.; Beckett, L.A.; Schenker, M.B. Occupational paraquat exposure of agricultural workers in large Costa Rican farms. Int. Arch. Occup. Environ. Health 2009, 82, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Mamane, A.; Baldi, I.; Tessier, J.-F.; Raherison, C.; Bouvier, G. Occupational exposure to pesticides and respiratory health. Eur. Respir. Rev. 2015, 24, 306–319. [Google Scholar] [CrossRef] [Green Version]
- Saravu, K.; Sekhar, S.; Pai, A.; Barkur, A.S.; Rajesh, V.; Earla, J.R. Paraquat—A deadly poison: Report of a case and review. Indian J. Crit. Care Med. 2013, 17, 182–184. [Google Scholar] [CrossRef]
- McKeag, D.; Maini, R.; Taylor, H.R. The ocular surface toxicity of paraquat. Br. J. Ophthalmol. 2002, 86, 350–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J. Paraquat Poisoning by Skin Absorption: A Review. Hum. Toxicol. 1988, 7, 15–19. [Google Scholar] [CrossRef]
- Tungsanga, K.; Chusilp, S.; Israsena, S.; Sitprija, V. Paraquat poisoning: Evidence of systemic toxicity after dermal exposure. Postgrad. Med. J. 1983, 59, 338–339. [Google Scholar] [CrossRef]
- Zhou, Y.; Vaidya, V.S.; Brown, R.P.; Zhang, J.; Rosenzweig, B.A.; Thompson, K.L.; Miller, T.J.; Bonventre, J.V.; Goering, P.L. Comparison of Kidney Injury Molecule-1 and Other Nephrotoxicity Biomarkers in Urine and Kidney Following Acute Exposure to Gentamicin, Mercury, and Chromium. Toxicol. Sci. 2007, 101, 159–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suntres, E.Z. Role of antioxidants in paraquat toxicity. Toxicology 2002, 180, 65–77. [Google Scholar] [CrossRef]
- Jayasumana, C.; Orantes, C.; Herrera, R.; Almaguer, M.; Lopez, L.; Silva, L.C.; Ordunez, P.; Siribaddana, S.; Gunatilake, S.; de Broe, M.E. Chronic interstitial nephritis in agricultural communities: A worldwide epidemic with social, occupational and environmental determinants. Nephrol. Dial. Transplant. 2017, 32, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Athuraliya, N.T.C.; Abeysekera, T.D.J.; Amerasinghe, P.H.; Kumarasiri, R.; Bandara, P.; Karunaratne, U.; Milton, A.H.; Jones, A.L. Uncertain etiologies of proteinuric-chronic kidney disease in rural Sri Lanka. Kidney Int. 2011, 80, 1212–1221. [Google Scholar] [CrossRef] [Green Version]
- Wanigasuriya, K. Update on uncertain etiology of chronic kidney disease in Sri Lanka’s north-central dry zone. MEDICC Rev. 2014, 16, 61–65. [Google Scholar] [PubMed]
- Gifford, F.J.; Gifford, R.M.; Eddleston, M.; Dhaun, N. Endemic Nephropathy Around the World. Kidney Int. Rep. 2017, 2, 282–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, C.; Aragón, A.; González, M.; López, I.; Jakobsson, K.; Elinder, C.-G.; Lundberg, I.; Wesseling, C. Decreased Kidney Function of Unknown Cause in Nicaragua: A Community-Based Survey. Am. J. Kidney Dis. 2010, 55, 485–496. [Google Scholar] [CrossRef] [Green Version]
- Lunyera, J.; Mohottige, D.; von Isenburg, M.; Jeuland, M.; Patel, U.D.; Stanifer, J.W. CKD of Uncertain Etiology: A Systematic Review. Clin. J. Am. Soc. Nephrol. 2016, 11, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Babich, R.; Ulrich, J.C.; Ekanayake, E.D.V.; Massarsky, A.; de Silva, P.M.C.; Manage, P.M.; Jackson, B.P.; Ferguson, P.L.; di Giulio, R.T.; Drummond, I.A.; et al. Kidney developmental effects of metal-herbicide mixtures: Implications for chronic kidney disease of unknown etiology. Environ. Int. 2020, 144, 106019. [Google Scholar] [CrossRef]
- Jayasumana, C.; Gunatilake, S.; Siribaddana, S. Simultaneous exposure to multiple heavy metals and glyphosate may contribute to Sri Lankan agricultural nephropathy. BMC Nephrol. 2015, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; González-Quiroz, M.; Weiss, I.; Glaser, J.; Vindell, J.J.; Stockfelt, L.; Roncal, C.; et al. Heat stress, dehydration, and kidney function in sugarcane cutters in El Salvador—A cross-shift study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2015, 142, 746–755. [Google Scholar] [CrossRef] [Green Version]
- Roncaljimenez, A.C.; García-Trabanino, R.; Barregard, L.; Lanaspa, M.A.; Wesseling, C.; Harra, T.; Aragón, A.; Grases, F.; Jarquin, E.R.; González, M.A.; et al. Heat Stress Nephropathy From Exercise-Induced Uric Acid Crystalluria: A Perspective on Mesoamerican Nephropathy. Am. J. Kidney Dis. 2016, 67, 20–30. [Google Scholar] [CrossRef]
- Jimenez, C.A.R.; Ishimoto, T.; Lanaspa, M.A.; Rivard, C.J.; Nakagawa, T.; Ejaz, A.A.; Cicerchi, C.; Inaba, S.; Le, M.; Miyazaki, M.; et al. Fructokinase activity mediates dehydration-induced renal injury. Kidney Int. 2014, 86, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Santos, U.P.; Zanetta, D.M.T.; Terra-Filho, M.; Burdmann, E.A. Burnt sugarcane harvesting is associated with acute renal dysfunction. Kidney Int. 2015, 87, 792–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, X.; Lu, J.; Wang, Z. Associated Risk Factors for Chronic Kidney Disease of Unknown Etiologies in 241 Patients. Int. J. Artif. Organs 2015, 38, 184–191. [Google Scholar] [CrossRef]
- Yang, H.-Y.; Hung, C.-C.; Liu, S.-H.; Guo, Y.-G.; Chen, Y.-C.; Ko, Y.-C.; Huang, C.-T.; Chou, L.-F.; Tian, Y.-C.; Chang, M.-Y.; et al. Overlooked Risk for Chronic Kidney Disease after Leptospiral Infection: A Population-Based Survey and Epidemiological Cohort Evidence. PLoS Negl. Trop. Dis. 2015, 9, e0004105. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, S.; Senevirathna, S.T.M.L.D.; Parahitiyawa, N.B.; Abeysekera, T.; Chandrajith, R.; Ratnatunga, N.; Hitomi, T.; Kobayashi, H.; Harada, K.H.; Koizumi, A. Whole-exome sequencing reveals genetic variants associated with chronic kidney disease characterized by tubulointerstitial damages in North Central Region, Sri Lanka. Environ. Health Prev. Med. 2015, 20, 354–359. [Google Scholar] [CrossRef]
- Correa-Rotter, R.; Wesseling, C.; Johnson, R.J. CKD of Unknown Origin in Central America: The Case for a Mesoamerican Nephropathy. Am. J. Kidney Dis. 2014, 63, 506–520. [Google Scholar] [CrossRef] [PubMed]
- Nerbass, F.B.; Pecoits-Filho, R.; Clark, W.F.; Sontrop, J.M.; McIntyre, C.W.; Moist, L. Occupational Heat Stress and Kidney Health: From Farms to Factories. Kidney Int. Rep. 2017, 2, 998–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaser, J.; Lemery, J.; Rajagopalan, B.; Diaz, H.F.; García-Trabanino, R.; Taduri, G.; Madero, M.; Amarasinghe, M.; Abraham, G.; Anutrakulchai, S.; et al. Climate Change and the Emergent Epidemic of CKD from Heat Stress in Rural Communities: The Case for Heat Stress Nephropathy. Clin. J. Am. Soc. Nephrol. 2016, 11, 1472–1483. [Google Scholar] [CrossRef] [Green Version]
- Wesseling, C.; Aragón, A.; González, M.; Weiss, I.; Glaser, J.; Bobadilla, N.A.; Roncal-Jiménez, C.; Correa-Rotter, R.; Johnson, R.J.; Barregard, L. Kidney function in sugarcane cutters in Nicaragua—A longitudinal study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2016, 147, 125–132. [Google Scholar] [CrossRef]
- Herath, C.; Jayasumana, C.; de Silva, P.M.C.; de Silva, P.C.; Siribaddana, S.; de Broe, M.E. Kidney Diseases in Agricultural Communities: A Case Against Heat-Stress Nephropathy. Kidney Int. Rep. 2018, 3, 271–280. [Google Scholar] [CrossRef]
- Jayasumana, C.; Paranagama, P.; Agampodi, S.B.; Wijewardane, C.; Gunatilake, S.; Siribaddana, S. Drinking well water and occupational exposure to Herbicides is associated with chronic kidney disease, in Padavi-Sripura, Sri Lanka. Environ. Health 2015, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jayatilake, N.; Mendis, S.; Maheepala, P.; Mehta, F.R. Chronic kidney disease of uncertain aetiology: Prevalence and causative factors in a developing country. BMC Nephrol. 2013, 14, 180. [Google Scholar] [CrossRef] [Green Version]
- Wasung, M.E.; Chawla, L.S.; Madero, M. Biomarkers of renal function, which and when? Clin. Chim. Acta 2015, 438, 350–357. [Google Scholar] [CrossRef]
- Waikar, S.S.; Betensky, R.A.; Bonventre, J.V. Creatinine as the gold standard for kidney injury biomarker studies? Nephrol. Dial. Transplant. 2009, 24, 3263–3265. [Google Scholar] [CrossRef] [Green Version]
- Bosch, J.P.; Saccaggi, A.; Lauer, A.; Ronco, C.; Belledonne, M.; Glabman, S. Renal functional reserve in humans. Am. J. Med. 1983, 75, 943–950. [Google Scholar] [CrossRef]
- Ichimura, T.; Bonventre, J.V.; Bailly, V.; Wei, H.; Hession, C.A.; Cate, R.L.; Sanicola, M. Kidney Injury Molecule-1 (KIM-1), a Putative Epithelial Cell Adhesion Molecule Containing a Novel Immunoglobulin Domain, Is Up-regulated in Renal Cells after Injury. J. Biol. Chem. 1998, 273, 4135–4142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, J.; Ma, Q.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of Neutrophil Gelatinase-Associated Lipocalin as a Novel Early Urinary Biomarker for Ischemic Renal Injury. J. Am. Soc. Nephrol. 2003, 14, 2534–2543. [Google Scholar] [CrossRef] [Green Version]
- Nauta, F.L.; Boertien, W.E.; Bakker, S.J.; van Goor, H.; van Oeveren, W.; de Jong, P.E.; Bilo, H.; Gansevoort, R.T. Glomerular and Tubular Damage Markers Are Elevated in Patients With Diabetes. Diabetes Care 2011, 34, 975–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, W.K.; Bailly, V.; Abichandani, R.; Thadhani, R.; Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): A novel biomarker for human renal proximal tubule injury. Kidney Int. 2002, 62, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidya, V.S.; Niewczas, M.A.; Ficociello, L.H.; Johnson, A.C.; Collings, F.B.; Warram, J.H.; Krolewski, A.S.; Bonventre, J.V. Regression of microalbuminuria in type 1 diabetes is associated with lower levels of urinary tubular injury biomarkers, kidney injury molecule-1, and N-acetyl-β-D-glucosaminidase. Kidney Int. 2011, 79, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Supavekin, S.; Zhang, W.; Kucherlapati, R.; Kaskel, F.J.; Moore, L.C.; Devarajan, P. Differential gene expression following early renal ischemia/reperfusion. Kidney Int. 2003, 63, 1714–1724. [Google Scholar] [CrossRef] [Green Version]
- Yuen, P.S.T.; Jo, S.-K.; Holly, M.K.; Hu, X.; Star, R.A. Ischemic and nephrotoxic acute renal failure are distinguished by their broad transcriptomic responses. Physiol. Genom. 2006, 25, 375–386. [Google Scholar] [CrossRef] [Green Version]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.-H.; Roumelioti, M.-E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering Beta-2 Microglobulin As a Biomarker across the Spectrum of Kidney Diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickolas, T.L.; O’Rourke, M.J.; Yang, J.; Sise, M.E.; Canetta, P.A.; Barasch, N.; Buchen, C.; Khan, F.; Mori, K.; Giglio, J.; et al. Sensitivity and Specificity of a Single Emergency Department Measurement of Urinary Neutrophil Gelatinase-Associated Lipocalin for Diagnosing Acute Kidney Injury. Ann. Intern. Med. 2008, 148, 810–819. [Google Scholar] [CrossRef]
- De Silva, P.M.C.S.; Abdul, K.S.M.; Eakanayake, E.M.D.V.; Jayasinghe, S.S.; Jayasumana, C.; Asanthi, H.B.; Perera, H.S.D.; Chaminda, G.G.T.; Chandana, E.P.S.; Siribaddana, S.H. Urinary Biomarkers KIM-1 and NGAL for Detection of Chronic Kidney Disease of Uncertain Etiology (CKDu) among Agricultural Communities in Sri Lanka. PLoS Neglected Trop. Dis. 2016, 10, e0004979. [Google Scholar] [CrossRef]
- Gunasekara, T.; de Silva, P.M.C.; Herath, C.; Siribaddana, S.; Siribaddana, N.; Jayasumana, C.; Jayasinghe, S.; Cardenas-Gonzalez, M.; Jayasundara, N. The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review. Int. J. Environ. Res. Public Health 2020, 17, 9522. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Acquavella, J.F.; Alexander, B.H.; Mandel, J.S.; Gustin, C.; Baker, B.; Chapman, P.; Bleeke, M. Glyphosate biomonitoring for farmers and their families: Results from the Farm Family Exposure Study. Environ. Health Perspect. 2004, 112, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Bolognesi, C.; Carrasquilla, G.; Volpi, S.; Solomon, K.R.; Marshall, E.J.P. Biomonitoring of Genotoxic Risk in Agricultural Workers from Five Colombian Regions: Association to Occupational Exposure to Glyphosate. J. Toxicol. Environ. Health Part A 2009, 72, 986–997. [Google Scholar] [CrossRef] [PubMed]
- Cha, E.S.; Lee, Y.K.; Moon, E.K.; Kim, Y.B.; Lee, Y.-J.; Jeong, W.C.; Cho, E.Y.; Lee, I.J.; Hur, J.; Ha, M.; et al. Paraquat application and respiratory health effects among South Korean farmers. Occup. Environ. Med. 2012, 69, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Kongtip, P.; Nankongnab, N.; Phupancharoensuk, R.; Palarach, C.; Sujirarat, D.; Sangprasert, S.; Sermsuk, M.; Sawattrakool, N.; Woskie, S.R. Glyphosate and Paraquat in Maternal and Fetal Serums in Thai Women. J. Agromed. 2017, 22, 282–289. [Google Scholar] [CrossRef]
- Mariager, T.P.; Madsen, P.V.; Ebbehøj, N.E.; Schmidt, B.; Juhl, A. Severe adverse effects related to dermal exposure to a glyphosate-surfactant herbicide. Clin. Toxicol. 2013, 51, 111–113. [Google Scholar] [CrossRef]
- Curwin, B.D.; Hein, M.J.; Sanderson, W.T.; Striley, C.; Heederik, D.; Kromhout, H.; Reynolds, S.J.; Alavanja, M.C. Urinary Pesticide Concentrations Among Children, Mothers and Fathers Living in Farm and Non-Farm Households in Iowa. Ann. Occup. Hyg. 2006, 51, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Schledorn, M.K.P. Detection of Glyphosate Residues in Animals and Humans. J. Environ. Anal. Toxicol. 2014, 4, 4. [Google Scholar] [CrossRef]
- Niemann, L.; Sieke, C.; Pfeil, R.; Solecki, R. A critical review of glyphosate findings in human urine samples and comparison with the exposure of operators and consumers. J. Consum. Prot. Food Saf. 2015, 10, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Baharuddin, M.R.B.; Sahid, I.B.; Noor, M.A.B.M.; Sulaiman, N.; Othman, F. Pesticide risk assessment: A study on inhalation and dermal exposure to 2,4-D and paraquat among Malaysian paddy farmers. J. Environ. Sci. Health Part B 2011, 46, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Joode, B.N.V.W.D.; de Graaf, I.A.M.; Wesseling, C.; Kromhout, H. Paraquat Exposure of Knapsack Spray Operators on Banana Plantations in Costa Rica. Int. J. Occup. Environ. Health 1996, 2, 294–304. [Google Scholar] [CrossRef]
- Huang, Y.; He, Q. Inhibition of c-Src protects paraquat induced microvascular endothelial injury by modulating caveolin-1 phosphorylation and caveolae mediated transcellular permeability. Environ. Toxicol. Pharmacol. 2017, 52, 62–68. [Google Scholar] [CrossRef]
- Weng, C.-H.; Hu, C.-C.; Lin, J.-L.; Lin-Tan, D.-T.; Huang, W.-H.; Hsu, C.-W.; Yen, T.-H. Sequential Organ Failure Assessment Score Can Predict Mortality in Patients with Paraquat Intoxication. PLoS ONE 2012, 7, e51743. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.-B.; He, J.-L.; Lu, Y.-Q. The significance of urine N-acetyl-beta-D-glucosaminidase in kidney injury with patients acute paraquat poisoning. Zhonghua Laodong Weisheng Zhiyebing Zazhi = Chin. J. Ind. Hyg. Occup. Dis. 2013, 31, 223–224. [Google Scholar]
- Mohamed, F.; Buckley, N.A.; Jayamanne, S.; Pickering, J.W.; Peake, P.; Palangasinghe, C.; Wijerathna, T.; Ratnayake, I.; Shihana, F.; Endre, Z.H. Kidney damage biomarkers detect acute kidney injury but only functional markers predict mortality after paraquat ingestion. Toxicol. Lett. 2015, 237, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, F.; Buckley, N.A.; Pickering, J.W.; Wunnapuk, K.; Dissanayake, S.; Chathuranga, U.; Gawarammana, I.; Jayamanne, S.; Endre, Z.H. Nephrotoxicity-induced proteinuria increases biomarker diagnostic thresholds in acute kidney injury. BMC Nephrol. 2017, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Orantes, C.M.; Herrera, R.; Almaguer, M.; Brizuela, E.G.; Núñez, L.; Alvarado, N.P.; Fuentes, E.J.; Bayarre, H.D.; Amaya, J.C.; Calero, D.J.; et al. Epidemiology of chronic kidney disease in adults of Salvadoran agricultural communities. MEDICC Rev. 2014, 16, 23–30. [Google Scholar]
- Laws, R.L.; Brooks, D.R.; Amador, J.J.; Weiner, D.E.; Kaufman, J.S.; Ramírez-Rubio, O.; Riefkohl, A.; Scammell, M.K.; López-Pilarte, D.; Sánchez, J.M.; et al. Changes in kidney function among Nicaraguan sugarcane workers. Int. J. Occup. Environ. Health 2015, 21, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Charlton, J.R.; Portilla, D.; Okusa, M.D. A basic science view of acute kidney injury biomarkers. Nephrol. Dial. Transplant. 2014, 29, 1301–1311. [Google Scholar] [CrossRef] [Green Version]
- Wunnapuk, K.; Liu, X.; Peake, P.; Gobe, G.; Endre, Z.; Grice, J.E.; Roberts, M.S.; Buckley, N.A. Renal biomarkers predict nephrotoxicity after paraquat. Toxicol. Lett. 2013, 222, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.Y.; Lee, M.J.; Seo, J.S.; Choi, D.; Park, J.B. Plasma neutrophil gelatinase-associated lipocalin as a predictive biomarker for the detection of acute kidney injury in adult poisoning. Clin. Toxicol. 2016, 54, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Gil, H.-W.; Yang, J.-O.; Lee, E.-Y.; Hong, S.-Y. Clinical implication of urinary neutrophil gelatinase-associated lipocalin and kidney injury molecule-1 in patients with acute paraquat intoxication. Clin. Toxicol. 2009, 47, 870–875. [Google Scholar] [CrossRef]
- Roberts, D.M.; Wilks, M.F.; Roberts, M.S.; Swaminathan, R.; Mohamed, F.; Dawson, A.H.; Buckley, N.A. Changes in the concentrations of creatinine, cystatin C and NGAL in patients with acute paraquat self-poisoning. Toxicol. Lett. 2011, 202, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, S.; Caplin, B.; Gonzalez-Quiroz, M.; Schensul, S.L.; Bhalla, V.; Parada, X.; Nanayakkara, N.; Fire, A.; Levin, A.; Friedman, D.J.; et al. Epidemiology, molecular, and genetic methodologies to evaluate causes of CKDu around the world: Report of the Working Group from the ISN International Consortium of Collaborators on CKDu. Kidney Int. 2019, 96, 1254–1260. [Google Scholar] [CrossRef]
- Osten, J.R.-V.; Dzul-Caamal, R. Glyphosate Residues in Groundwater, Drinking Water and Urine of Subsistence Farmers from Intensive Agriculture Localities: A Survey in Hopelchén, Campeche, Mexico. Int. J. Environ. Res. Public Health 2017, 14, 595. [Google Scholar] [CrossRef]
- Rubio, F.; Veldhuis, L.J.; Clegg, B.S.; Fleeker, J.R.; Hall, J.C. Comparison of a Direct ELISA and an HPLC Method for Glyphosate Determinations in Water. J. Agric. Food Chem. 2003, 51, 691–696. [Google Scholar] [CrossRef]
- Wanigasuriya, K.; Jayawardene, I.; Amarasiriwardena, C.; Wickremasinghe, R. Novel urinary biomarkers and their association with urinary heavy metals in chronic kidney disease of unknown aetiology in Sri Lanka: A pilot study. Ceylon Med. J. 2017, 62, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Cárdenas-González, M.; Osorio-Yáñez, C.; Gaspar-Ramírez, O.; Pavković, M.; Ochoa-Martínez, A.; López-Ventura, D.; Medeiros, M.; Barbier, O.; Pérez-Maldonado, I.; Sabbisetti, V.; et al. Environmental exposure to arsenic and chromium in children is associated with kidney injury molecule-1. Environ. Res. 2016, 150, 653–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prozialeck, W.C.; Edwards, J.R. Early biomarkers of cadmium exposure and nephrotoxicity. BioMetals 2010, 23, 793–809. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 210) | Matara (n = 75) | Rahathangama (n = 69) | Warunagama (n = 66) | p-Value |
|---|---|---|---|---|---|
| Age (Mean ± SEM) | 44.39 ± 0.93 | 39 ± 1.4 | 48 ± 1.5 | 47 ± 1.5 | <0.0001 |
| Smoking (%) | |||||
| Yes | 30.46 | 25.3 | 21.74 | 45.45 | 0.006 |
| Alcohol consumption (%) | |||||
| Yes | 33.33 | 25.3 | 14.49 | 62.12 | <0.0001 |
| Chewing betel (%) | |||||
| Yes | 44.76 | 16.00 | 60.87 | 60.61 | <0.0001 |
| Drinking water (%)—current | |||||
| Surface water | 40.49 | 4.00 | 75.36 | 4.55 | <0.0001 |
| Drinking water (%)—past | |||||
| Surface water | 62.86 | 9.33 | 92.75 | 92.43 | <0.0001 |
| Intensive Herbicide use (%) | |||||
| Yes | 53.33 | 10.66 | 81.20 | 72.70 | <0.0001 |
| Fertilizer use (%) | |||||
| Yes | 83.44 | 70.66 | 81.20 | 72.70 | 0.352 |
| Mixing herbicides on-site (%) | |||||
| Yes | 54.41 | 50.66 | 62.32 | 50.00 | 0.250 |
| Source of recommendation (%) | |||||
| Agriculture officer | 8.55 | 14.60 | 4.35 | 6.06 | 0.107 |
| Usage at the recommended dose (%) | |||||
| Yes | 21.91 | 20.00 | 28.99 | 16.67 | 0.194 |
| Overuse of herbicides (%) | |||||
| Yes | 54.76 | 44.00 | 55.07 | 66.67 | 0.038 |
| Use of Personal Protective Equipment (PPE) (%) | |||||
| Yes | 29.49 | 30.60 | 39.13 | 18.18 | 0.027 |
| Safe storage of herbicides (%) | |||||
| Yes | 31.89 | 29.30 | 36.23 | 30.30 | 0.616 |
| Correct disposal (%) | |||||
| Yes | 32.84 | 17.30 | 36.23 | 46.97 | <0.000 |
| Variables | Total | Matara (MA) | Rahathangama (RH) | Warunagama (WA) | Kruskal-Wallis & Mann-Whitney U Test |
|---|---|---|---|---|---|
| Glyphosate (µg/g Cr) | |||||
| All (Median) | 198.49 | 177.8 | 224.3 | 224.5 | <0.0001 1 MA vs. RH 0.033 2 MA vs. WA 0.017 2 RH vs. WA 0.710 |
| Range | 0.0–979.98 | 99.5–350.1 | 33.1–827.3 | 0.0–979.9 | |
| IQR | 147.01–286.61 | 147.1–225 | 138.3–327.7 | 147.9–353 | |
| n | 210 | 75 | 69 | 66 | |
| Male (Median) | 175.3 | 175.2 | 147.2 | 200.8 | 0.07 1 MA vs. RH 0.207 MA vs. WA 0.157 RH vs. WA 0.034 2 |
| Range | 33.14–555.4 | 105–287.3 | 33.14–474.5 | 41.74–555.4 | |
| IQR | 138.3–250.8 | 148.5–216.8 | 95.23–238.4 | 146.2–328.0 | |
| n | 124 | 47 | 31 | 46 | |
| Female (Median) | 234.1 | 185.3 | 299.0 | 276.9 | 0.012 1 MA vs. RH 0.002 2 MA vs. WA 0.035 2 RH vs. WA 0.901 |
| Range | 0.0–827.3 | 99.5–350.1 | 83.78–827.3 | 0–980 | |
| IQR | 163.0–343.1 | 137.2–235.9 | 177.9–400.7 | 161.6–494.1 | |
| n | 86 | 28 | 38 | 20 | |
| Paraquat (µg/g Cr) | |||||
| All (median) | 0.31 | 0 | 0.12 | 0.75 | <0.0001 1 MA vs. RH 0.7341 MA vs. WA < 0.0001 2 RH vs. WA 0.0042 2 |
| Range | 0.0–11.42 | 0.0–1.3 | 0.0–2.8 | 0.0–11.4 | |
| IQR | 0.0–0.99 | 0–0.63 | 0–0.92 | 0–2.1 | |
| n | 210 | 75 | 69 | 66 | |
| Male (Median) | 0.645 | 0 | 0.84 | 1.675 | <0.0001 1 MA vs. RH 0.0006 2 MA vs. WA < 0.0001 2 RH vs. WA 0.019 |
| Range | 0.0–11.42 | 0–1.32 | 0–2.63 | 0–11.42 | |
| IQR | 0.0–1.57 | 0–0.63 | 0–1.52. | 0.18–2.73 | |
| n | 124 | 47 | 31 | 46 | |
| Female (Median) | 0.00 | 0.33 | 0 | 0.18 | 0.182 1 MA vs. RH 0.160 MA vs. WA 0.890 RH vs. WA 0.100 |
| Range | 0.0–2.79 | 0–0.65 | 0–2.79 | 0–1.17 | |
| IQR | 0.0–0.42 | 0–0.65 | 0–0.227 | 0–0.4925 | |
| n | 86 | 28 | 38 | 20 | |
| Variables | Total n = 210 | Matara n = 75 | Rahathangama n = 69 | Warunagama n = 66 | Mann-Whitney U Test |
|---|---|---|---|---|---|
| Microalbumin (mg/L); p < 0.0001 1 | |||||
| Median | 10.00 | 6 | 11 | 21 | MA vs. RH <0.0001 2 |
| Range | 2.00–311.0 | 2–311 | 2–162 | 2–157 | MA vs. WA <0.0001 2 |
| IQR | 5.00–25.00 | 4–10 | 7–36.5 | 6–65.5 | RH vs. WA 0.3052 |
| Urinary Creatinine (mg/dL); p < 0.0001 1 | |||||
| Median | 85.40 | 136.8 | 58.9 | 62.15 | MA vs. RH <0.0001 2 |
| Range | 0.78–513.10 | 32–513.1 | 19.9–355.2 | 7.8–337.4 | MA vs. WA <0.0001 2 |
| IQR | 45.65–179.10 | 87.4–259.3 | 40.7–108.1 | 34.6–142 | RH vs. WA 0.636 |
| ACR (mg/g Cr); p < 0.0001 1 | |||||
| Median | 12.00 | 4.3 | 14.9 | 23.7 | MA vs. RH <0.0001 2 |
| Range | 1.10–470.00 | 1.1–237.9 | 5.4–393.1 | 7.1–470 | MA vs. WA <0.0001 2 |
| IQR | 6.57–24.55 | 2.2–6.7 | 10.8–24.0 | 11.5–64.6 | RH vs. WA 0.055 |
| Serum Creatinine (mg/dL); p = 0.003 1 | |||||
| Median | 1.11 | 1.09 | 1.13 | 1.225 | MA vs. RH 0.282 |
| Range | 0.67–6.41 | 0.67–4.07 | 0.67–5.98 | 0.67–6.41 | MA vs. WA <0.0001 2 |
| IQR | 0.96–1.33 | 0.98–1.13 | 0.91–1.6 | 1.01–2.07 | RH vs. WA 0.060 |
| eGFR (mL/min/1.73 m2) p < 0.0001 1 | |||||
| Median | 73.00 | 86 | 65 | 59 | MA vs. RH <0.0001 2 |
| Range | 9.0–123.0 | 15–122 | 11–115 | 9–123 | MA vs. WA <0.0001 2 |
| IQR | 51.0–90.0 | 72–98 | 41–87 | 36–87 | RH vs. WA 0.566 |
| KIM-1 (ng/g Cr); p = 0.156 | |||||
| Median | 3.096 | 1.74 | 3.2 | 3.6 | MA vs. RH 0.1207 |
| IQR | 1.181–112.41 | 0.76–116.9 | 1.29–106.1 | 1.94–115.1 | MA vs. WA 0.0807 |
| Mean (SEM) | 94.56 ± 12.62 | 66.5 ± 11.6 | 114.6 ± 25.5 | 101.6 ± 25.0 | RH vs. WA 0.7165 |
| Range | 0.30–954.0 | 0.3–353.9 | 0.4–944.2 | 0.4–954.3 | |
| NGAL (ng/mg Cr); p < 0.0001 1 | |||||
| Median | 2.05 | 1.28 | 3.09 | 2.14 | MA vs. RH <0.0001 2 |
| IQR | 0.91–5.20 | 0.56–2.81 | 1.15–9.09 | 1.28–6.15 | MA vs. WA 0.0006 2 |
| Mean (SEM) | 8.89 ± 1.83 | 2.1 ± 0.3 | 12.0 ± 2.8 | 12.4 ± 4.7 | RH vs. WA 0.5766 |
| Range | 0.27–283.01 | 0.3–10.1 | 0.3–128.4 | 0.4–283.0 | |
| B2M (ng/mg Cr) p = 0.7403 | |||||
| Median | 22.54 | 21.01 | 23.64 | 24.18 | MA vs. RH 0.852 |
| IQR | 9.49–61.63 | 9.41–50.01 | 10.79–65.03 | 9.13–68.04 | MA vs. WA 0.90 |
| Mean (SEM) | 55.74 ± 6.29 | 42.27 ± 7.32 | 55.06 ± 9.26 | 73.26 ± 16.16 | RH vs. WA 0.90 |
| Range | 1.54–601.14 | 2.11–382.4 | 2.75–411.3 | 1.54–601.4 | |
| Cys C (mg/L); p < 0.0001 1 | |||||
| Median | 0.77 | 0.74 | 0.825 | 0.68 | MA vs. RH 0.094 |
| IQR | 0.69–0.85 | 0.67–0.81 | 0.68–1.02 | 0.56–0.79 | MA vs. WA 0.0504 |
| Mean (SEM) | 0.87 ± 0.03 | 0.77 ± 0.03 | 0.87 ± 0.03 | 0.77 ± 0.04 | RH vs. WA <0.0001 |
| Range | 0.38–3.24 | 0.54–2.66 | 0.38–1.47 | 0.35–3.24 | |
| Variables | Glyphosate (µg/g Cr) | Paraquat (µg/g Cr) | ||
|---|---|---|---|---|
| rs | p | rs | p | |
| Microalbumin (mg/L) | −0.224 | 0.0014 | 0.133 | 0.059 |
| KIM-1 (ng/g Cr) | 0.098 | 0.165 | −0.057 | 0.418 |
| NGAL (ng/mg Cr) | 0.4932 | 0.001 | −0.113 | 0.107 |
| SCr (mg/L) | 0.098 | 0.162 | 0.021 | 0.771 |
| eGFR (mL/min/1.73 m2) | −0.147 | 0.036 | 0.051 | 0.411 |
| B2M (ng/mg Cr) | −0.1438 | 0.0416 | −0.06328 | 0.3721 |
| SCys C (mg/L) | −0.1411 | 0.04567 | 0.1258 | 0.0752 |
| Variable | Total | Matara (MA) | Rahathangama (RH) | Warunagama (WA) | |||||
|---|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | β (95% CI) | p | ||
| SCr | Glyphosate Paraquat Age Gender Location | −0.01 (−0.001 to 0.001) 0.168 (−0.001 to 0.02) 0.21 (0.006 to 0.03) −0.11 (−0.52 to 0.09) 0.239 (0.123 to 0.449) | 0.87 0.02 0.002 0.16 0.01 | 6.2 (−0.003 to 0.003) 0.11 (−0.23 to 0.45) 0.01 (0.001 to 0.02) −0.82 (−0.42 to 0.25) | 0.96 0.52 0.05 0.63 | 7.5 (−0.001 to −0.3) −0.3 (−0.5 to 0.03) 0.000 (−0.02 to 0.02) −0.8 (−1.3 to −0.3) | 0.92 0.07 0.98 0.001 | 0.001 (−0.001 to 0.002) −0.04 (−0.2 to 0.1) 0.02 (−0.006 to 0.04) −0.2 (−1.1 to 0.6) | 0.54 0.62 0.14 0.59 |
| eGFR | Glyphosate Paraquat Age Gender Location | −0.01 (0.05 to 0.01) −0.14 (−5.5 to 0.17) −0.16 (−0.65 to −0.05) −0.12 (−16.4 to 1.87) −0.3.4 (−15.44 to −6.03) | 0.21 0.07 0.02 0.12 <0.001 | 0.01 (−0.09 to 0.09) −1.92 (−12.9 to 9.1) −1.09 (−1.5 to −0.7) −2.46 (−13.5 to 8.4) | 0.98 0.73 <0.001 0.65 | −0.02 (−0.07 to 0.02) 7.7 (−1.3 to 16.7) −0.5 (−1.02 to −0.05) 9.7 (−5.6 to 25) | 0.26 0.09 0.03 0.21 | −0.02 (−6.06 to 0.02) 2.0 (−1.5 to 5.6) −0.9 (−1.4 to −0.3) −27.4 (−39.2 to −3.6) | 0.42 0.25 0.002 0.02 |
| KIM−1 | Glyphosate Paraquat Age Gender Location | −0.04 (−0.23 to 0.14) 0.05 (−12.61 to 23.85) 0.11 (−0.48 to 3.37) −0.01 (−62.78 to 54.02) 0.08 (−13.15 to 48.24) | 0.65 0.54 0.14 0.88 0.261 | −0.32 (−0.7 to 0.09) −8.26 (−59.5 to 43) −3.14 (−5.05 to −1.23) −72.04 (−122.8 to −21.3) | 0.12 0.75 0.002 0.006 | 0.03 (−0.3 to 0.4) −33.5 (−106.9 to 39.9) 2.4 (−1.6 to 6.4) 46.5 (−78.9 to 171.8) | 0.86 0.36 0.23 0.46 | 0.05 (−0.24 to 0.34) −10.0 (−35.7 to 15.7) 0.01 (−3.9 to 3.9) −154.3 (−283.9 to −24.8) | 0.74 0.44 0.99 0.02 |
| NGAL | Glyphosate Paraquat Age Gender Location | 0.09 (−0.01 to 0.04) −0.008 (−2.76 to 2.48) −0.02 (−0.32 to 0.24) 0.12 (−1.97 to 14.82) 0.16 (0.73 to 9.54) | 0.23 0.92 0.78 0.13 0.023 | 0.02 (0.01 to 0.03) −1.14 (−2.3 to 0.01) 0.03 (−0.01 to 0.07) −0.25 (−1.4 to 0.9) | <0.001 0.05 0.19 0.67 | 0.06 (0.03 to 0.1) −0.3 (−7.8 to 7.2) −0.3 (−0.7 to 0.1) −5.6 (−18.4 to 7.2) | 0.001 0.94 0.17 0.39 | 0.1 (0.07 to 0.2) −3.3 (−7.4 to 0.8) −0.4 (−0.9 to 0.3) −2.2 (−22.7 to 18.3) | <0.001 0.11 0.27 0.83 |
| ACR | Glyphosate Paraquat Age Gender Location | −0.06 (−0.00 to 0.05) 0.17 (1.35 to 17.14) 0.24 (0.57 to 2.24) 0.003 (−24.73 to 25.86) 0.261 (12.45 to 39.11) | 0.39 0.02 0.001 0.97 <0.001 | 0.03 (−0.1 to 0.17) 9.21 (−8.1 to 26.6) 0.50 (−0.14 to 1.15) −2.89 (−20.0 to 14.3) | 0.64 0.29 0.12 0.74 | −0.02 (−0.2 to 0.1) −30.6 (−61.3 to 0.1) −0.5 (−2.2 to 1.2) −54.6 (−1.7 to −2.1) | 0.79 0.05 0.54 0.04 | 0.02 (−0.1 to 0.2) 1.7 (−10.5 to 13.9) 1.6 (−0.3 to 3.4) −4.6 (−66.3 to 56.9) | 0.82 0.78 0.1 0.88 |
| B2M | Glyphosate Paraquat Age Gender Location | −0.03 (−0.17 to 0.12) 0.02 (−12.33 to 16.22) 0.07 (−0.75 to 2.27) −0.09 (−70.9 to 20.56) −0.013 (−24.00 to 21.88) | 0.75 0.79 0.32 0.28 0.854 | −0.07 (−1.22 to 0.69) −0.11 (−187.55 to 74.28) −0.10 (−5.95 to 2.77) −0.14 (−175.43 to 53.08) | 0.58 0.39 0.47 0.29 | −0.02 (−0.15 to 0.13) −0.22 (−50.98 to 4.74) 0.08 (−1.00 to 2.03) −0.24 (−85.68 to 9.48) | 0.89 0.10 0.50 0.12 | −0.09 (−0.22 to 0.11) 0.23 (−2.43 to 27.02) 0.33 (0.87 to 5.38) 0.07 (−56.89 to 91.64) | 0.53 0.1 0.007 0.64 |
| Cys C | Glyphosate Paraquat Age Gender Location | −0.001 (0.00 to 0.00) 0.09 (0.02 to 0.06) 0.19 (0.001 to 0.01) −0.07 (−0.18 to 0.07) 0.165 (0.013 to 0.144) | 0.99 0.25 0.009 0.35 0.019 | −0.04 (−0.001 to 0.001) −0.09 (−0.24 to 0.11) −0.13 (−0.009 to 0.003) −0.19 (−0.26 to 0.05) | 0.76 0.49 0.35 0.17 | 0.04 (0.00 to 0.001) −0.24 (−0.19 to 0.01) 0.03 (−0.01 to 0.01) −0.36 (−0.37 to 0.04) | 0.78 0.07 0.80 0.01 | −0.67 (−0.001 to 0.001) 0.16 (−0.03 to 0.10) 0.34 (0.004 to 0.03) 0.04 (−0.29 to 0.39) | 0.66 0.27 0.006 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul, K.S.M.; De Silva, P.M.C.S.; Ekanayake, E.M.D.V.; Thakshila, W.A.K.G.; Gunarathna, S.D.; Gunasekara, T.D.K.S.C.; Jayasinghe, S.S.; Asanthi, H.B.; Chandana, E.P.S.; Chaminda, G.G.T.; et al. Occupational Paraquat and Glyphosate Exposure May Decline Renal Functions among Rural Farming Communities in Sri Lanka. Int. J. Environ. Res. Public Health 2021, 18, 3278. https://doi.org/10.3390/ijerph18063278
Abdul KSM, De Silva PMCS, Ekanayake EMDV, Thakshila WAKG, Gunarathna SD, Gunasekara TDKSC, Jayasinghe SS, Asanthi HB, Chandana EPS, Chaminda GGT, et al. Occupational Paraquat and Glyphosate Exposure May Decline Renal Functions among Rural Farming Communities in Sri Lanka. International Journal of Environmental Research and Public Health. 2021; 18(6):3278. https://doi.org/10.3390/ijerph18063278
Chicago/Turabian StyleAbdul, K.S.M., P. Mangala C.S. De Silva, E.M.D.V. Ekanayake, W.A.K.G. Thakshila, S.D. Gunarathna, T.D.K.S.C. Gunasekara, S.S. Jayasinghe, H.B. Asanthi, E.P.S. Chandana, G.G.T. Chaminda, and et al. 2021. "Occupational Paraquat and Glyphosate Exposure May Decline Renal Functions among Rural Farming Communities in Sri Lanka" International Journal of Environmental Research and Public Health 18, no. 6: 3278. https://doi.org/10.3390/ijerph18063278