
Community Pharmacy Practice in Italy during the COVID-19 (SARS-CoV-2) Pandemic: Regulatory Changes and a Cross-Sectional Analysis of Seroprevalence

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Regulatory Research
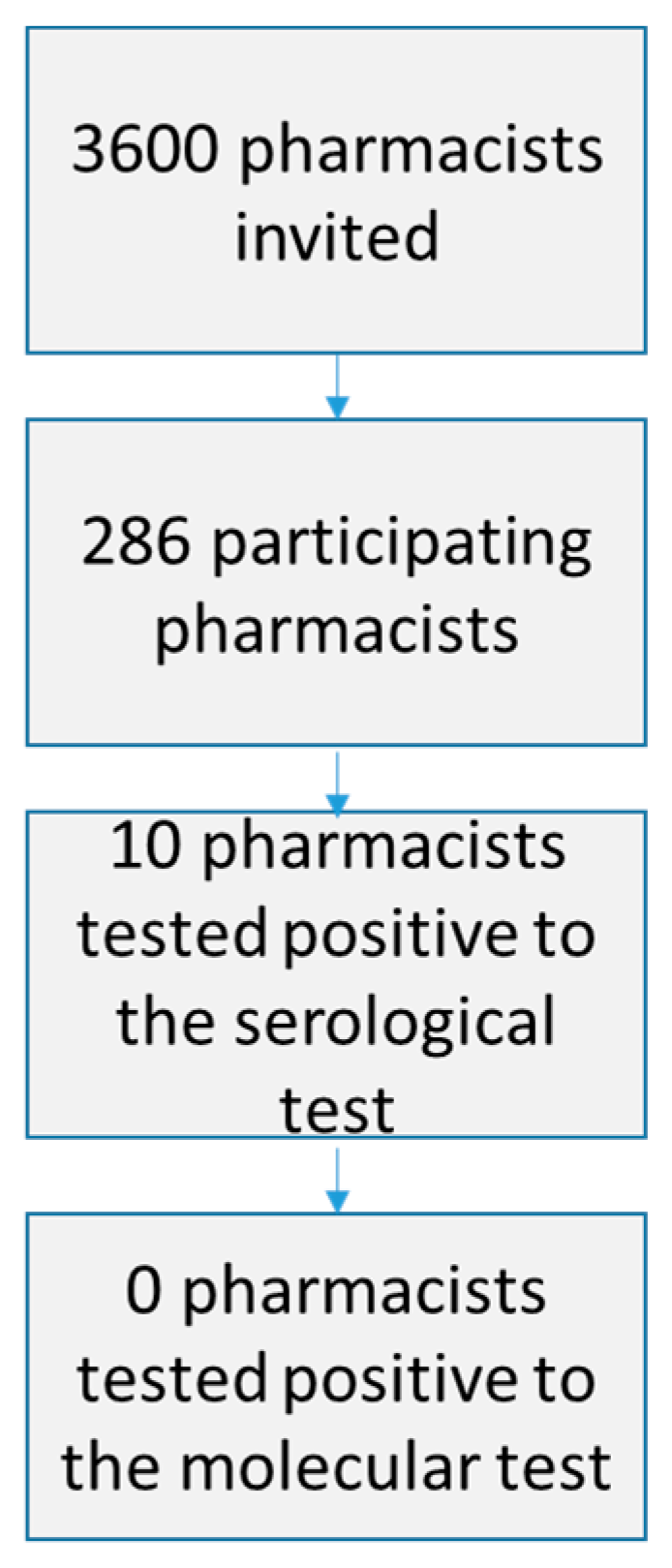
2.2. Seroprevalence Investigation
3. Results
3.1. Anti-COVID-19 Preventative Measures Applied in Pharmacies in the Piedmont Region
3.2. Seroprevalence Investigation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Submission Declaration
References
- Hasan, S.S.; Kow, C.S.; Razi Zaidi, S.T. Social distancing and the use of PPE by community pharmacy personnel: Does evidence support these measures? Res. Social Adm. Pharm. 2021, 17, 456–459. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Website. Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 1 December 2020).
- Italian Government Website. Available online: http://www.governo.it/it/articolo/comunicato-stampa-del-consiglio-dei-ministri-n-27/13937 (accessed on 1 December 2020).
- Italian Ministry of Health Website. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4084 (accessed on 1 December 2020).
- Pharmaceutical Group of the European Union (PGEU) Website. Available online: https://www.pgeu.eu/wp-content/uploads/2020/03/PR-Community-Pharmacists-in-the-frontline-in-the-fight-against-coronavirus.pdf (accessed on 1 December 2020).
- Italian Government Website. Available online: http://opendatadpc.maps.arcgis.com/apps/opsdashboard/index.html#/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 1 December 2020).
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Ferrante di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 6, CD013652. [Google Scholar] [CrossRef] [PubMed]
- PRIMA Lab SA Website. Available online: https://primahometest.com/en/covid-19_serological_test (accessed on 16 February 2021).
- ANSA Website. Available online: https://www.ansa.it/sito/notizie/cronaca/2020/02/21/coronavirus-un-contagiato-in-lombardia_dda62491-4ae1-40af-9cd4-e7dc8402b493.html (accessed on 1 December 2020).
- Italian Government Website. Available online: http://www.governo.it/it/coronavirus. (accessed on 1 December 2020).
- Italian Ministry of Health Website. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/homeNuovoCoronavirus.jsp (accessed on 1 December 2020).
- Italian Civil Protection Website. Available online: http://www.protezionecivile.gov.it/attivita-rischi/rischio-sanitario/emergenze/coronavirus (accessed on 1 December 2020).
- Piedmont Region Website. Available online: https://www.regione.piemonte.it/web/temi/sanita/coronavirus-piemonte-ordinanze-circolari-disposizioni-attuative (accessed on 1 December 2020).
- Pharmacy Owners Association Website. Available online: https://www.federfarma.it/ (accessed on 1 December 2020).
- Bragazzi, N.L.; Mansour, M.; Bonsignore, A.; Ciliberti, R. The Role of Hospital and Community Pharmacists in the Management of COVID-19: Towards an Expanded Definition of the Roles, Responsibilities, and Duties of the Pharmacist. Pharmacy 2020, 8, 140. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency Website. Available online: https://www.ema.europa.eu/en/news/covid-19-reminder-risk-serious-side-effects-chloroquine-hydroxychloroquine (accessed on 1 December 2020).
- Diao, B.; Wen, K.; Zhang, J.; Chen, J.; Han, C.; Chen, Y.; Wang, S.; Deng, G.; Zhou, H.; Wu, Y. Accuracy of a nucleocapsid protein antigen rapid test in the diagnosis of SARS-CoV-2 infection. Clin. Microbiol. Infect. 2020, 27, 289.e1–289.e4. [Google Scholar] [CrossRef] [PubMed]
- Strömer, A.; Rose, R.; Schäfer, M.; Schön, F.; Vollersen, A.; Lorentz, T.; Fickenscher, H.; Krumbholz, A. Performance of a Point-of-Care Test for the Rapid Detection of SARS-CoV-2 Antigen. Microorganisms 2020, 9, 58. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, T.J.; Kang, Y.; Bridges, C.B.; Talbert, T.; Vagi, S.J.; Lamont, B.; Graitcer, S.B. Integrating pharmacies into public health program planning for pandemic influenza vaccine response. Vaccine 2016, 34, 5643–5648. [Google Scholar] [CrossRef] [Green Version]
- Australian Government Department of Health Website. Available online: https://www.health.gov.au/sites/default/files/documents/2021/02/covid-19-vaccination-community-pharmacy-covid-19-vaccine-rollout-from-phase-2a.pdf (accessed on 16 February 2021).
- Centers for Disease Control and Prevention (CDC) Website. Available online: https://www.cdc.gov/vaccines/covid-19/retail-pharmacy-program/index.html (accessed on 16 February 2021).
- General Pharmaceutical Council Website. Available online: https://www.pharmacyregulation.org/standards/guidance/qa-coronavirus/covid-19-vaccination-programme (accessed on 16 February 2021).
- Amato, M.; Werba, J.P.; Frigerio, B.; Coggi, D.; Sansaro, D.; Ravani, A.; Ferrante, P.; Veglia, F.; Tremoli, E.; Baldassarre, D. Relationship between Influenza Vaccination Coverage Rate and COVID-19 Outbreak: An Italian Ecological Study. Vaccines 2020, 8, 535. [Google Scholar] [CrossRef] [PubMed]
- Bach, A.T.; Goad, J.A. The role of community pharmacy-based vaccination in the USA: Current practice and future directions. Integr. Pharm. Res. Pract. 2015, 4, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isenor, J.E.; Edwards, N.T.; Alia, T.A.; Slayter, K.L.; MacDougall, D.M.; McNeil, S.A.; Bowles, S.K. Impact of pharmacists as immunizers on vaccination rates: A systematic review and meta-analysi. Vaccine 2016, 34, 5708–5723. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.Q.; Yang, L.; Zhou, P.X.; Li, H.B.; Liu, F.; Zhao, R.S. Recommendations and guidance for providing pharmaceutical care services during COVID-19 pandemic: A China perspective. Res. Social Adm. Pharm. 2021, 17, 1819–1824. [Google Scholar] [CrossRef] [PubMed]
- Sum, Z.Z.; Ow, C.J.W. Community pharmacy response to infection control during COVID-19. A cross-sectional survey. Res. Social Adm. Pharm. 2021, 17, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Giua, C.; Paoletti, G.; Minerba, L.; Malipiero, G.; Melone, G.; Heffler, E.; Pistone, A.; Keber, E.; SIFAC Group of Clinical Community Pharmacists (SGCP). Community pharmacist’s professional adaptation amid Covid-19 emergency: A national survey on Italian pharmacists. Int. J. Clin. Pharm. 2021, 1–8. [Google Scholar] [CrossRef]
- Hayden, J.C.; Parkin, R. The challenges of COVID-19 for community pharmacists and opportunities for the future. Ir. J. Psychol. Med. 2020, 37, 198–203. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
Health and hygiene measures
|
| Variable | Response | Pharmacists with Positive Serological Test n (%) | Pharmacists with Negative Serological Test n (%) |
|---|---|---|---|
| Mask (any type) | Yes | 10 (4%) | 274 (96%) |
| No | 0 (0%) | 2 (100%) | |
| p-value = 1.00 | |||
| Face shield and/or safety glasses | Yes | 0 (0%) | 75 (100%) |
| No | 10 (5%) | 201 (95%) | |
| p-value = 0.07 | |||
| Plexiglass protection barrier | Yes | 9 (4%) | 249 (96%) |
| No | 1 (4%) | 27 (96%) | |
| p-value = 1.00 | |||
| Disposable gloves | Yes | 9 (3%) | 253 (97%) |
| No | 1 (4%) | 23 (96%) | |
| p-value = 0.59 | |||
| Hand sanitizer | Yes | 7 (3%) | 257 (97%) |
| No | 3 (14%) | 19 (86%) | |
| p-value = 0.03 | |||
| Decontamination of premises | Yes | 4 (3%) | 112 (97%) |
| No | 6 (4%) | 164 (96%) | |
| p-value = 1.00 | |||
| Regular surface decontamination | Yes | 8 (3%) | 252 (97%) |
| No | 2 (8%) | 24 (92%) | |
| p-value = 0.23 | |||
| Quota restrictions on admissions for customers | Yes | 8 (3%) | 260 (97%) |
| No | 2 (11%) | 16 (89%) | |
| p-value = 0.13 |
| Subjects | Cloth Mask | Surgical Mask | Filtered Mask FFP2 or FFP3 | Face Shield | Safety Glasses | Plexiglass Barrier | Disposable Gloves | Disposable Gown | Hand Sanitizer (Gel or Liquid) | Regular Surface Decontamination | Decontamination of Premises by Certified Cleaners | Quota Restrictions on Admissions for Customers |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | no | yes | yes | no | no | yes | no | no | no | yes | no | yes |
| 2 | yes | yes | no | no | no | yes | yes | no | yes | yes | no | no |
| 3 | no | yes | no | no | no | yes | yes | no | no | yes | yes | yes |
| 4 | no | no | yes | no | no | yes | yes | no | no | yes | yes | yes |
| 5 | no | yes | no | no | no | yes | yes | yes | yes | yes | yes | yes |
| 6 | no | yes | yes | no | no | yes | yes | no | yes | yes | no | yes |
| 7 | no | yes | no | no | no | no | yes | no | yes | no | no | no |
| 8 | yes | no | no | no | no | yes | yes | no | yes | yes | no | yes |
| 9 | no | yes | yes | no | no | yes | yes | no | yes | yes | no | yes |
| 10 | no | yes | no | no | no | yes | yes | no | yes | no | yes | yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baratta, F.; Visentin, G.M.; Ravetto Enri, L.; Parente, M.; Pignata, I.; Venuti, F.; Di Perri, G.; Brusa, P. Community Pharmacy Practice in Italy during the COVID-19 (SARS-CoV-2) Pandemic: Regulatory Changes and a Cross-Sectional Analysis of Seroprevalence. Int. J. Environ. Res. Public Health 2021, 18, 2302. https://doi.org/10.3390/ijerph18052302
Baratta F, Visentin GM, Ravetto Enri L, Parente M, Pignata I, Venuti F, Di Perri G, Brusa P. Community Pharmacy Practice in Italy during the COVID-19 (SARS-CoV-2) Pandemic: Regulatory Changes and a Cross-Sectional Analysis of Seroprevalence. International Journal of Environmental Research and Public Health. 2021; 18(5):2302. https://doi.org/10.3390/ijerph18052302
Chicago/Turabian StyleBaratta, Francesca, Giulio Mario Visentin, Lorenzo Ravetto Enri, Marco Parente, Irene Pignata, Francesco Venuti, Giovanni Di Perri, and Paola Brusa. 2021. "Community Pharmacy Practice in Italy during the COVID-19 (SARS-CoV-2) Pandemic: Regulatory Changes and a Cross-Sectional Analysis of Seroprevalence" International Journal of Environmental Research and Public Health 18, no. 5: 2302. https://doi.org/10.3390/ijerph18052302