
Family Physicians’ Standpoint and Mental Health Assessment in the Light of COVID-19 Pandemic—A Nationwide Survey Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey
2.3. Mental Health Assessment
2.4. Knowledge, Attitudes and Practices Assessment
2.5. Statistical Analysis
3. Results
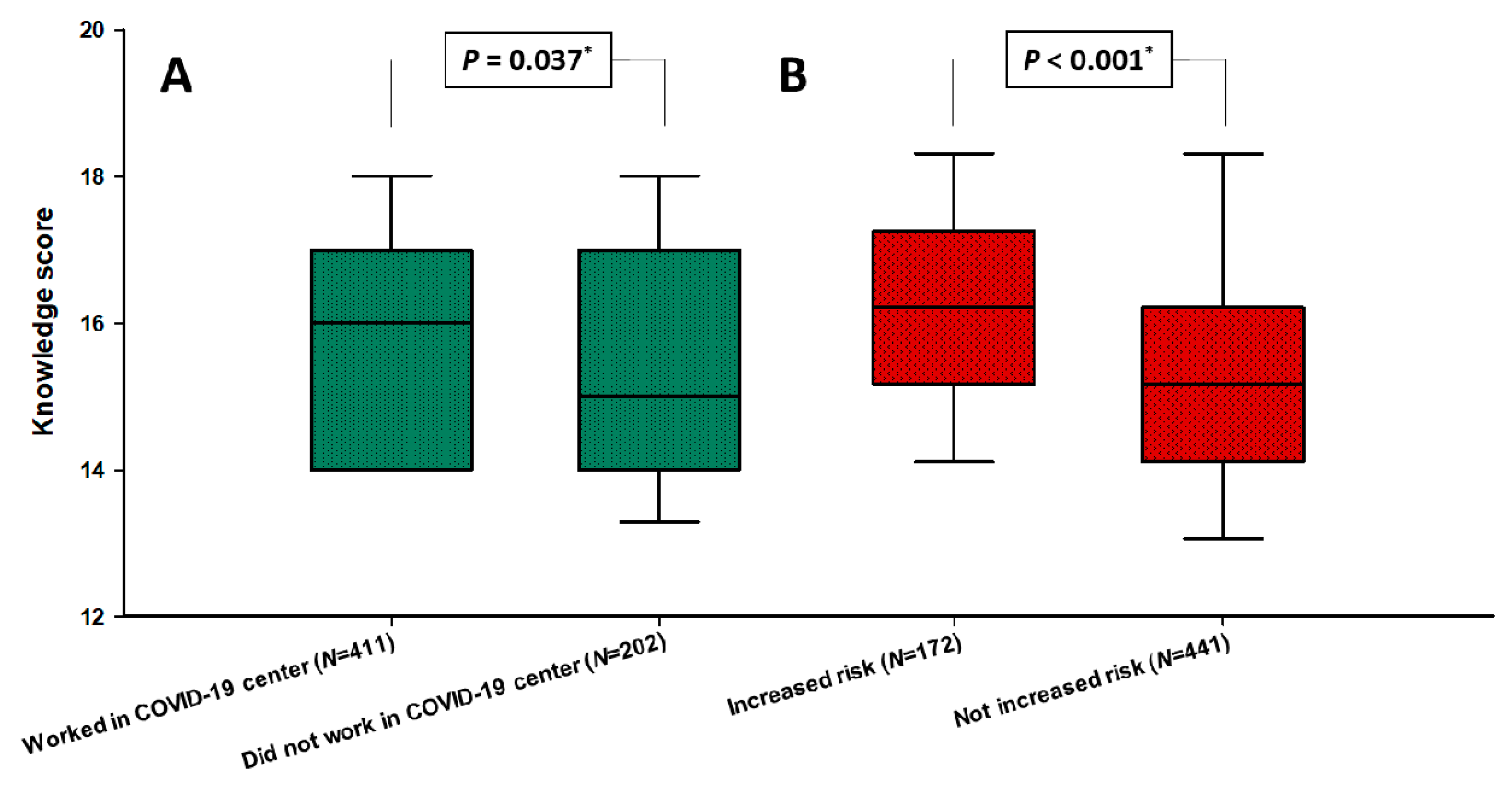
3.1. Baseline Information and COVID-19 Knowledge Characteristics
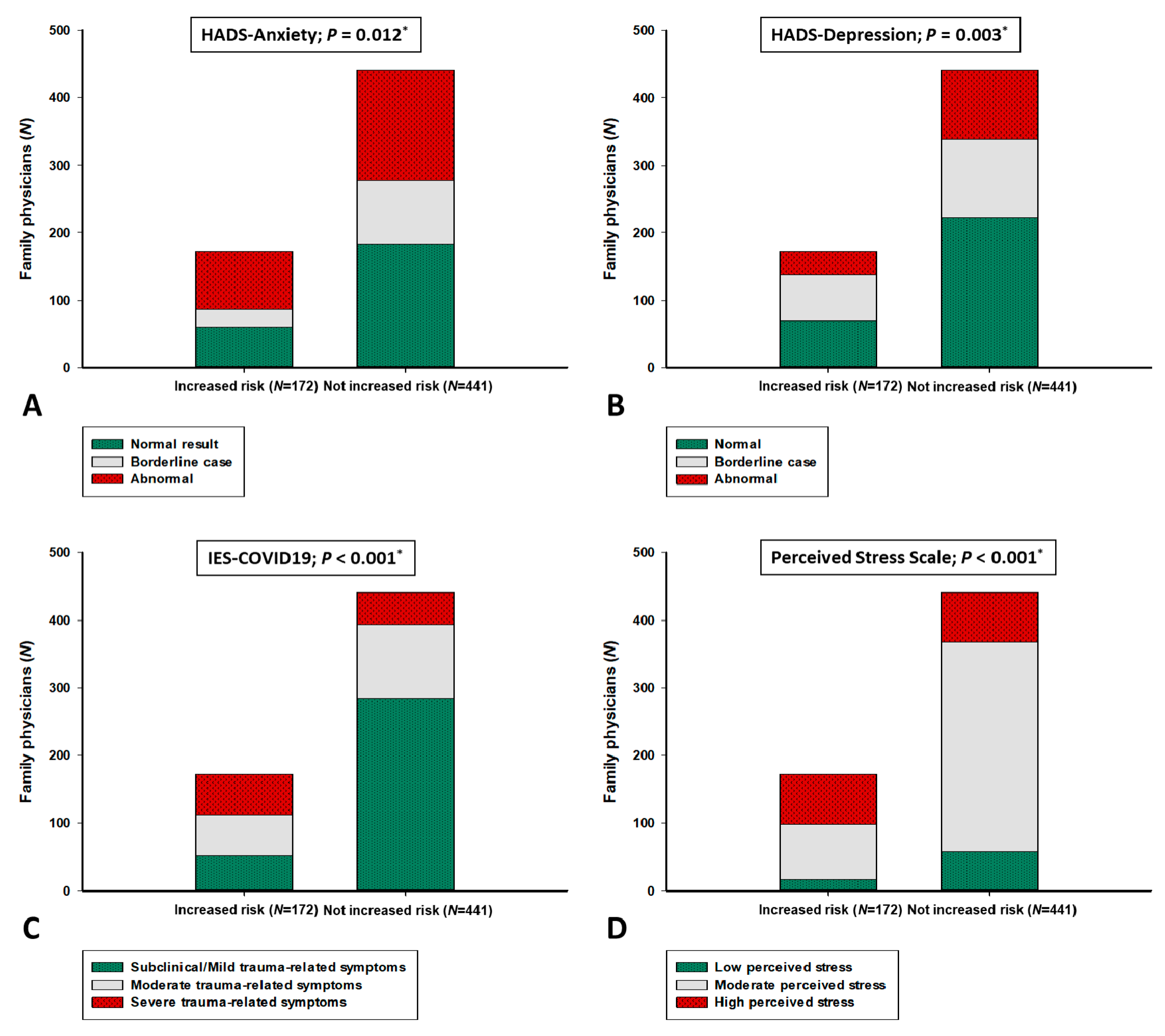
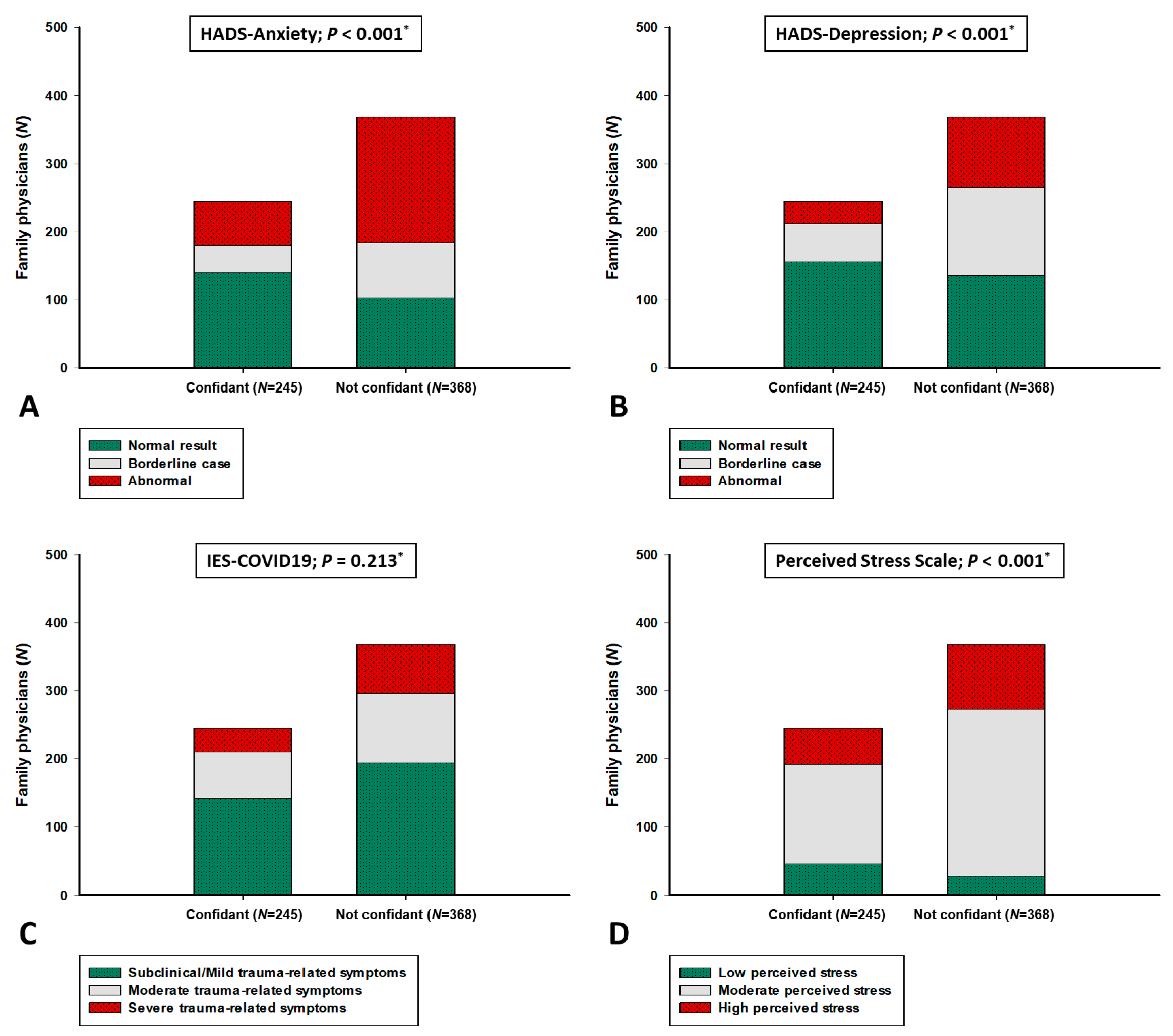
3.2. Mental Health Characteristics and Associations with Other Parameters
3.3. Attitudes and Practices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 29 December 2020).
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 20 January 2021).
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 20 January 2021).
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [Green Version]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of Coronavirus disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Rospleszcz, S.; Greiser, K.H.; Dallavalle, M.; Berger, K. The impact of the COVID-19 pandemic on self-reported health. Dtsch. Arztebl. Int. 2020, 117, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- De Filippis, G.; Cavazzana, L.; Gimigliano, A.; Piacenza, M.; Vimercati, S. COVID-19 pandemic: A frontline hospital reorganization to cope with therapeutic and diagnostic emergency. Pharmacol. Res. 2020, 161, 105160. [Google Scholar] [CrossRef] [PubMed]
- Rawaf, S.; Allen, L.N.; Stigler, F.L.; Kringos, D.; Quezada Yamamoto, H.; van Weel, C.; Global Forum on Universal Health Coverage and Primary Health Care. Lessons on the COVID-19 pandemic, for and by primary care professionals worldwide. Eur. J. Gen. Pract. 2020, 26, 129–133. [Google Scholar] [CrossRef]
- Kunin, M.; Engelhard, D.; Piterman, L.; Thomas, S. Response of general practitioners to infectious disease public health crises: An integrative systematic review of the literature. Disaster Med. Public Health Prep. 2013, 7, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, L.S.; Von Pressentin, K.B.; Naidoo, K.; Schaefer, R. The evolving role of family physicians during the coronavirus disease 2019 crisis: An appreciative reflection. Afr. J. Prim. Health Care Fam. Med. 2020, 12, e1–e4. [Google Scholar] [CrossRef]
- Li, D. First in, Last out—The Role of Family Doctors in the Fight Against Novel Coronavirus. Available online: https://www.globalfamilydoctor.com/News/DonaldLiontheCoronavirus.aspx (accessed on 30 December 2020).
- Verhoeven, V.; Tsakitzidis, G.; Philips, H.; Van Royen, P. Impact of the COVID-19 pandemic on the core functions of primary care: Will the cure be worse than the disease? A qualitative interview study in Flemish GPs. BMJ Open 2020, 10, e039674. [Google Scholar] [CrossRef]
- The European Definition of GP/FM. World Organization of Family Doctors, WONCA. Available online: https://www.woncaeurope.org/page/definition-of-general-practice-family-medicine (accessed on 30 December 2020).
- Allen, J.; Gay, B.; Crebolder, H.; Heyrman, J.; Svab, I.; Ram, P. The European definitions of the key features of the discipline of general practice: The role of the GP and core competencies. Br. J. Gen. Pract. 2002, 52, 526–527. [Google Scholar] [PubMed]
- Tarrant, C.; Stokes, T.; Baker, R. Factors associated with patients’ trust in their general practitioner: A cross-sectional survey. Br. J. Gen. Pract. 2003, 53, 798–800. [Google Scholar]
- Schultz, K.; Delva, D.; Kerr, J. Emotional effects of continuity of care on family physicians and the therapeutic relationship. Can. Fam. Physician. 2012, 58, 178–185. [Google Scholar]
- Viehmann, A.; Kersting, C.; Thielmann, A.; Weltermann, B. Prevalence of chronic stress in general practitioners and practice assistants: Personal, practice and regional characteristics. PLoS ONE 2017, 12, e0176658. [Google Scholar] [CrossRef]
- Soler, J.K.; Yaman, H.; Esteva, M.; Dobbs, F.; Asenova, R.S.; Katic, M.; Ozvacic, Z.; Desgranges, J.P.; Moreau, A.; Lionis, C.; et al. Burnout in European family doctors: The EGPRN study. Fam. Pract. 2008, 25, 245–265. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-related mental health effects in the workplace: A narrative review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef] [PubMed]
- Amerio, A.; Bianchi, D.; Santi, F.; Costantini, L.; Odone, A.; Signorelli, C.; Costanza, A.; Serafini, G.; Amore, M.; Aguglia, A. Covid-19 pandemic impact on mental health: A web-based cross-sectional survey on a sample of Italian general practitioners. Acta Biomed. 2020, 91, 83–88. [Google Scholar] [CrossRef]
- Monterrosa-Castro, A.; Redondo-Mendoza, V.; Mercado-Lara, M. Psychosocial factors associated with symptoms of generalized anxiety disorder in general practitioners during the COVID-19 pandemic. J. Investig. Med. 2020, 68, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Danhieux, K.; Buffel, V.; Pairon, A.; Benkheil, A.; Remmen, R.; Wouters, E.; van Olmen, J. The impact of COVID-19 on chronic care according to providers: A qualitative study among primary care practices in Belgium. BMC Fam. Pract. 2020, 21, 255. [Google Scholar] [CrossRef]
- Lin, S.; Sattler, A.; Smith, M. Retooling primary care in the COVID-19 era. Mayo Clin. Proc. 2020, 95, 1831–1834. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pokrajac-Bulian, A.; Kukic, M.; Basic-Markovic, N. Quality of life as a mediator in the association between body mass index and negative emotionality in overweight and obese non-clinical sample. Eat. Weight. Disord. 2015, 20, 473–481. [Google Scholar] [CrossRef]
- Galic, M.; Mustapic, L.; Simunic, A.; Sic, L.; Cipolletta, S. COVID-19 related knowledge and mental health: Case of Croatia. Front. Psychol. 2020, 11, 567368. [Google Scholar] [CrossRef]
- Vanaken, L.; Scheveneels, S.; Belmans, E.; Hermans, D. Validation of the impact of event scale with modifications for COVID-19 (IES-COVID19). Front. Psychiatry 2020, 11, 738. [Google Scholar] [CrossRef]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of event scale: A measure of subjective stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Sterling, M. The impact of event scale (IES). Aust. J. Physiother. 2008, 54, 78. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Nielsen, M.G.; Ørnbøl, E.; Vestergaard, M.; Bech, P.; Larsen, F.B.; Lasgaard, M.; Christensen, K.S. The construct validity of the perceived stress scale. J. Psychosom. Res. 2016, 84, 22–30. [Google Scholar] [CrossRef]
- Hudek-Knezevic, J.; Kardum, I.; Lesic, R. Effects of perceived stress and coping strategies on physical symptoms. Drus. Istraz. Zagreb 1999, 8, 543–561. [Google Scholar]
- Nakic, S.; Tadinac, M.; Herman, R. The role of perceived stress and coping styles in development of prenatal anxiety. Klin. Psihol. 2009, 2, 7–21. [Google Scholar]
- Wahed, A.W.Y.; Hefzy, E.M.; Ahmed, M.I.; Hamed, N.S. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J. Community Health 2020, 45, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.L.; Luo, W.; Li, H.M.; Zhang, Q.Q.; Liu, X.G.; Li, W.T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef]
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dardas, L.A.; Khalaf, I.; Nabolsi, M.; Nassar, O.; Halasa, S. Developing an understanding of adolescents’ knowledge, attitudes, and practices toward COVID-19. J. Sch. Nurs. 2020, 36, 430–441. [Google Scholar] [CrossRef]
- Parikh, P.A.; Shah, B.V.; Phatak, A.G.; Vadnerkar, A.C.; Uttekar, S.; Thacker, N.; Nimbalkar, S.M. COVID-19 Pandemic: Knowledge and perceptions of the public and healthcare professionals. Cureus 2020, 12, e8144. [Google Scholar] [CrossRef]
- Hussain, I.; Majeed, A.; Imran, I.; Ullah, M.; Hashmi, F.K.; Saeed, H.; Chaudhry, M.O.; Rasool, M.F. Knowledge, attitude, and practices toward COVID-19 in primary healthcare providers: A cross-sectional study from three tertiary care hospitals of Peshawar, Pakistan. J. Community Health 2020, 1–9. [Google Scholar] [CrossRef]
- Alzoubi, H.; Alnawaiseh, N.; Al-Mnayyis, A.; Abu-Lubad, M.; Aqel, A.; Al-Shagahin, H. COVID-19—Knowledge, attitude and practice among medical and non-medical university students in Jordan. J. Pure Appl. Microbiol. 2020, 14, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Rabbani, U.; Al Saigul, A.M. Knowledge, attitude and practices of health care workers about corona virus disease 2019 in Saudi Arabia. J. Epidemiol. Glob. Health 2020. [Google Scholar] [CrossRef]
- Raudenská, J.; Steinerová, V.; Javůrková, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best. Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef]
- COVID-19 Country Overviews. Available online: https://covid19-country-overviews.ecdc.europa.eu/ (accessed on 28 December 2020).
- Amanullah, S.; Shankar, R.R. The impact of COVID-19 on physician burnout globally: A review. Healthcare 2020, 8, 421. [Google Scholar] [CrossRef]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Jalnapurkar, I.; Allen, M.; Pigott, A.T. Sex differences in anxiety disorders: A review. J. Psychiatry Depress. Anxiety 2018, 4, 12. [Google Scholar] [CrossRef]
- Yu, S. Uncovering the hidden impacts of inequality on mental health: A global study. Transl. Psychiatry 2018, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Nørøxe, K.B.; Pedersen, A.F.; Bro, F.; Vedsted, P. Mental well-being and job satisfaction among general practitioners: A nationwide cross-sectional survey in Denmark. BMC Fam. Pract. 2018, 19, 130. [Google Scholar] [CrossRef] [PubMed]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442. [Google Scholar] [CrossRef]
- Gokdemir, O.; Pak, H.; Bakola, M.; Bhattacharya, S.; Hoedebecke, K.; Jelastopulu, E. Family physicians’ knowledge about and attitudes towards COVID-19—A Cross-sectional multicentric study. Infect. Chemother. 2020, 52, 539–549. [Google Scholar] [CrossRef]
- Puspitasari, I.M.; Yusuf, L.; Sinuraya, R.K.; Abdulah, R.; Koyama, H. Knowledge, attitude, and practice during the COVID-19 pandemic: A review. J. Multidiscip. Healthc. 2020, 13, 727–733. [Google Scholar] [CrossRef]
- Nejasmic, D.; Vrdoljak, D.; Lang, B.V.; Borovac, J.A.; Marusic, A. Awareness, attitudes, barriers, and knowledge about evidence-based medicine among family physicians in Croatia: A cross-sectional study. BMC Fam. Pract. 2020, 21, 88. [Google Scholar] [CrossRef]
- Tysiąc-Miśta, M.; Dziedzic, A. The attitudes and professional approaches of dental practitioners during the COVID-19 outbreak in Poland: A cross-sectional survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Simms, A.; Fear, N.T.; Greenberg, N. The impact of having inadequate safety equipment on mental health. Occup. Med. 2020, 70, 278–281. [Google Scholar] [CrossRef] [PubMed]
- The Impact of the COVID-19 Pandemic on Noncommunicable Disease Resources and Services: Results of a Rapid Assessment. Available online: https://www.who.int/teams/noncommunicable-diseases/covid-19 (accessed on 15 January 2021).
- Chopra, S.; Ranjan, P.; Singh, V.; Kumar, S.; Arora, M.; Hasan, M.S.; Kasiraj, R.; Kaur, D.; Vikram, N.K.; Malhotra, A.; et al. Impact of COVID-19 on lifestyle-related behaviours—A cross-sectional audit of responses from nine hundred and ninety-five participants from India. Diabetes Metab. Syndr. 2020, 14, 2021–2030. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Monaco, A.; Kivipelto, M.; Onder, G.; Maggi, S.; Michel, J.P.; Prieto, R.; Sykara, G.; Donde, S. The potential long-term impact of the COVID-19 outbreak on patients with non-communicable diseases in Europe: Consequences for healthy ageing. Ageing Clin. Exp. Res. 2020, 32, 1189–1194. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Female Physicians (N = 491) | Male Physicians (N = 122) | Total Population (N = 613) | p * |
|---|---|---|---|---|
| Age (years) | 44.0 (35.0–55.0) | 43.0 (36.0–55.0) | 44.0 (35.0–55.0) | 0.279 |
| Work experience (years) | 13.0 (6.2–25.7) | 14.5 (7.0–27.0) | 13.0 (7.0–26.0) | 0.630 |
| Increased personal risk of COVID-19 | 138 (28.1) | 34 (27.9) | 172 (28.1) | 0.958 |
| Work experience in COVID-19 center | 326 (66.4) | 85 (69.7) | 411 (67.0) | 0.491 |
| Occupation | ||||
| Family physician | 415 (84.5) | 114 (93.4) | 529 (86.3) | 0.010 |
| Family medicine resident | 76 (15.5) | 8 (6.6) | 84 (13.7) | |
| Practice localization | ||||
| Urban area | 338 (68.8) | 78 (63.9) | 416 (67.9) | 0.299 |
| Rural area/islands | 153 (31.2) | 44 (36.1) | 197 (32.1) | |
| Main source of COVID-19 information | ||||
| Online medical databases | 65 (13.2) | 20 (16.4) | 85 (13.9) | 0.647 |
| Colleagues health professionals | 73 (14.9) | 18 (14.8) | 91 (14.8) | |
| WHO/CIPH recommendations | 304 (61.9) | 69 (56.6) | 373 (60.0) | |
| News (online, television) | 29 (5.9) | 7 (5.7) | 36 (5.9) | |
| Other | 20 (4.1) | 8 (6.6) | 28 (4.6) | |
| Confident in personal COVID-19 knowledge | 192 (39.1) | 53 (43.4) | 245 (40.0) | 0.382 |
| Knowledge test score | 16.0 (14.2–17.0) | 15.0 (14.0–17.0) | 16.0 (14.0–17.0) | 0.115 |
| Parameter | Female Physicians (N = 491) | Male Physicians (N = 122) | Total Population (N = 613) | p * |
|---|---|---|---|---|
| Mental health questionnaires scores | ||||
| Perceived Stress Scale | 21.0 (16.0–27.0) | 16.0 (12.0–19.0) | 20.0 (16.0–26.0) | <0.001 |
| Impact on Event Scale-COVID19 | 26.0 (15.0–39.0) | 15.0 (4.0–23.0) | 24.0 (14.0–36.2) | <0.001 |
| HADS-Anxiety | 10.0 (6.0–13.0) | 8.0 (4.0–12.0) | 9.0 (5.0–12.0) | 0.001 |
| HADS-Depression | 8.0 (4.0–10.0) | 6.5 (3.0–10.0) | 8.0 (4.0–10.0) | 0.005 |
| Mental health questionnaires categories | ||||
| Perceived Stress Scale | ||||
| Low perceived stress | 40 (8.1) | 35 (28.7) | 75 (12.2) | <0.001 |
| Moderate perceived stress | 315 (64.2) | 75 (61.5) | 390 (63.6) | |
| High perceived stress | 136 (27.7) | 12 (9.8) | 148 (24.1) | |
| Impact on Event Scale-COVID19 | ||||
| Subclinical/Mild PTSD symptoms | 241 (49.1) | 95 (77.9) | 336 (54.8) | <0.001 |
| Moderate PTSD symptoms | 153 (31.2) | 17 (13.9) | 170 (27.7) | |
| Severe PTSD symptoms | 97 (19.8) | 10 (8.2) | 107 (17.5) | |
| HADS-Anxiety subscale | ||||
| Normal result | 185 (37.7) | 58 (47.5) | 243 (39.6) | 0.047 |
| Borderline case | 94 (19.1) | 26 (21.3) | 120 (19.6) | |
| Abnormal | 212 (43.2) | 38 (31.1) | 250 (40.8) | |
| HADS-Depression subscale | ||||
| Normal | 223 (45.4) | 69 (56.6) | 292 (47.6) | 0.009 |
| Borderline case | 147 (29.9) | 38 (31.1) | 185 (30.2) | |
| Abnormal | 121 (24.6) | 15 (12.3) | 136 (22.2) | |
| Parameter | PSS r (p *) | HADS-A r (p *) | HADS-D r (p *) | IES-COVID19 r (p *) |
|---|---|---|---|---|
| Age (years) | 0.106 (0.009) | −0.011 (0.776) | 0.111 (0.006) | 0.195 (<0.001) |
| Work experience (years) | 0.110 (0.006) | 0.024 (0.554) | 0.128 (0.001) | 0.212 (<0.001) |
| Patients in care (N) † | 0.128 (0.002) | 0.119 (0.003) | 0.135 (0.001) | 0.050 (0.237) |
| Knowledge score | −0.064 (0.114) | −0.131 (0.001) | −0.048 (0.239) | 0.045 (0.267) |
| PSS | - | 0.411 (<0.001) | 0.390 (<0.001) | 0.592 (<0.001) |
| HADS-A | 0.411 (<0.001) | - | 0.805 (<0.001) | 0.418 (<0.001) |
| HADS-D | 0.390 (<0.001) | 0.805 (<0.001) | - | 0.382 (<0.001) |
| Variables | Β * | SE † | t-Value | P |
|---|---|---|---|---|
| Model 1—HADS-Anxiety score (F-ratio = 3.11; p = 0.005) | ||||
| Age (years) | −0.03 | 0.02 | −1.37 | 0.169 |
| Increased personal risk of COVID-19 | 1.02 | 0.52 | 1.96 | 0.050 |
| Practice localization (urban vs. rural/island area) | −0.001 | 0.42 | −0.001 | 0.998 |
| Work experience in COVID-19 center | 0.06 | 0.42 | 0.14 | 0.885 |
| Gender (male vs. female) | 1.51 | 0.49 | 3.01 | 0.003 |
| Knowledge score | −0.31 | 0.11 | −2.76 | 0.006 |
| Model 2—HADS-Depression score (F-ratio = 5.18; p < 0.001) | ||||
| Age (years) | 0.03 | 0.02 | 1.43 | 0.152 |
| Increased personal risk of COVID-19 | 0.92 | 0.45 | 2.02 | 0.044 |
| Practice localization (urban vs. rural/island area) | 0.41 | 0.37 | 1.09 | 0.275 |
| Work experience in COVID-19 center | 1.24 | 0.37 | 3.36 | <0.001 |
| Gender (male vs. female) | 1.16 | 0.43 | 2.67 | 0.007 |
| Knowledge score | −0.07 | 0.09 | −0.78 | 0.435 |
| Model 3—IES-COVID19 score (F-ratio = 22.2; p < 0.001) | ||||
| Age (years) | 0.11 | 0.06 | 1.88 | 0.060 |
| Increased personal risk of COVID-19 | 9.39 | 1.55 | 6.06 | <0.001 |
| Practice localization (urban vs. rural/island area) | 2.21 | 1.26 | 1.74 | 0.081 |
| Work experience in COVID-19 center | 1.22 | 1.25 | 0.97 | 0.329 |
| Gender (male vs. female) | 11.6 | 1.47 | 7.84 | <0.001 |
| Knowledge score | −0.37 | 0.32 | −1.15 | 0.250 |
| Model 4—Perceived Stress Scale score (F-ratio = 23.2; p < 0.001) | ||||
| Age (years) | −0.001 | 0.03 | −0.28 | 0.775 |
| Increased personal risk of COVID-19 | 4.05 | 0.69 | 5.82 | <0.001 |
| Practice localization (urban vs. rural/island area) | −0.09 | 0.56 | −0.15 | 0.897 |
| Work experience in COVID-19 center | 1.77 | 0.57 | 3.13 | 0.002 |
| Gender (male vs. female) | 6.21 | 0.66 | 9.34 | <0.001 |
| Knowledge score | −0.33 | 0.15 | −2.27 | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilovic, T.; Bozic, J.; Vilovic, M.; Rusic, D.; Zuzic Furlan, S.; Rada, M.; Tomicic, M. Family Physicians’ Standpoint and Mental Health Assessment in the Light of COVID-19 Pandemic—A Nationwide Survey Study. Int. J. Environ. Res. Public Health 2021, 18, 2093. https://doi.org/10.3390/ijerph18042093
Vilovic T, Bozic J, Vilovic M, Rusic D, Zuzic Furlan S, Rada M, Tomicic M. Family Physicians’ Standpoint and Mental Health Assessment in the Light of COVID-19 Pandemic—A Nationwide Survey Study. International Journal of Environmental Research and Public Health. 2021; 18(4):2093. https://doi.org/10.3390/ijerph18042093
Chicago/Turabian StyleVilovic, Tina, Josko Bozic, Marino Vilovic, Doris Rusic, Sanja Zuzic Furlan, Marko Rada, and Marion Tomicic. 2021. "Family Physicians’ Standpoint and Mental Health Assessment in the Light of COVID-19 Pandemic—A Nationwide Survey Study" International Journal of Environmental Research and Public Health 18, no. 4: 2093. https://doi.org/10.3390/ijerph18042093