Relationships between Perceived Stress, Depression and Alcohol Use Disorders in University Students during the COVID-19 Pandemic: A Socio-Economic Dimension


Abstract
:1. Introduction
2. Theoretical Background
2.1. Perceived Stress
2.2. Depression
2.3. Alcohol Use Disorders
3. Materials and Methods
3.1. Research Objective
3.2. Research Sample and Data Collection Process
3.3. Research Instruments and Variables
3.4. Statistical Analysis
4. Results
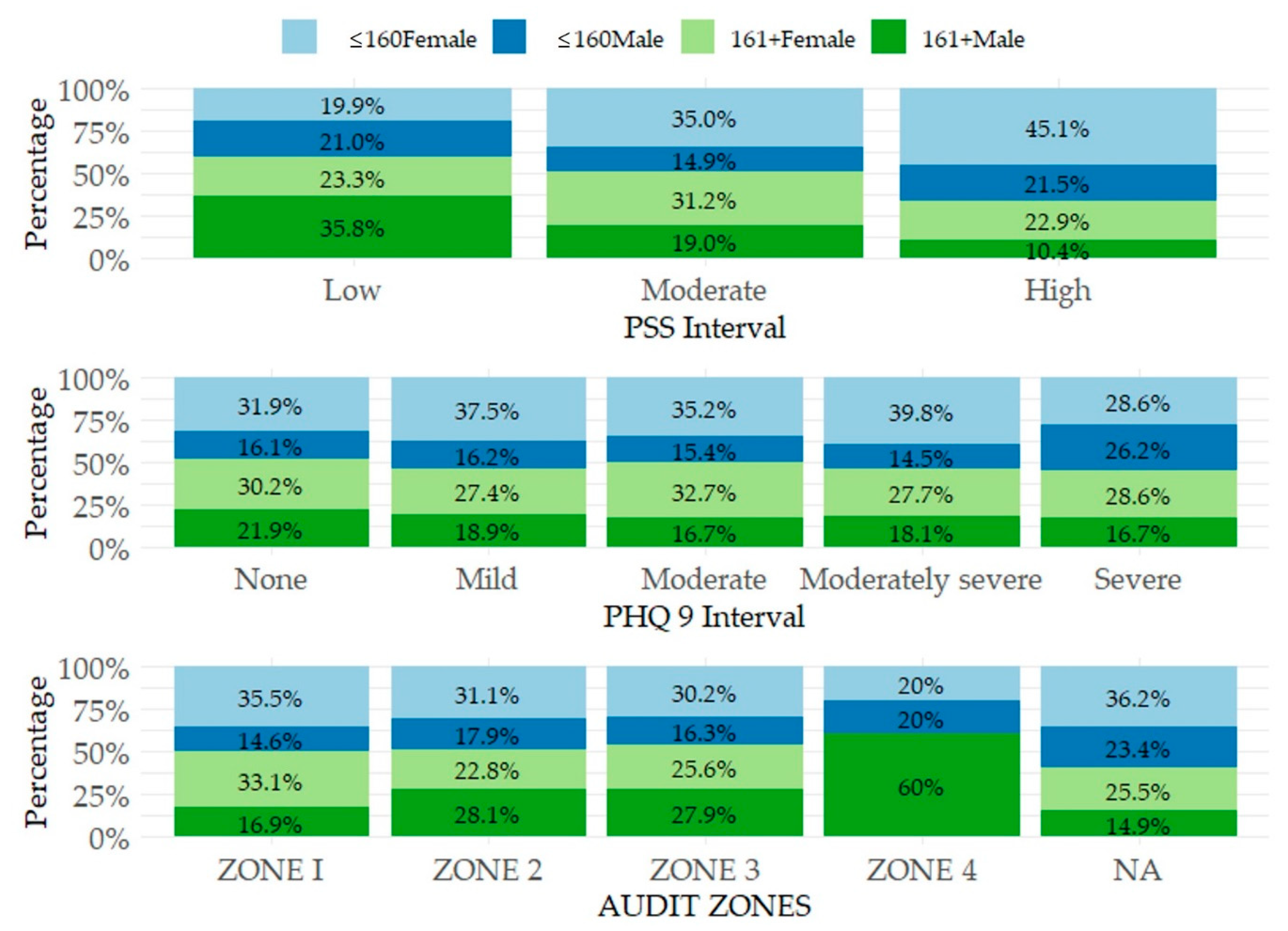
4.1. Descriptive Part
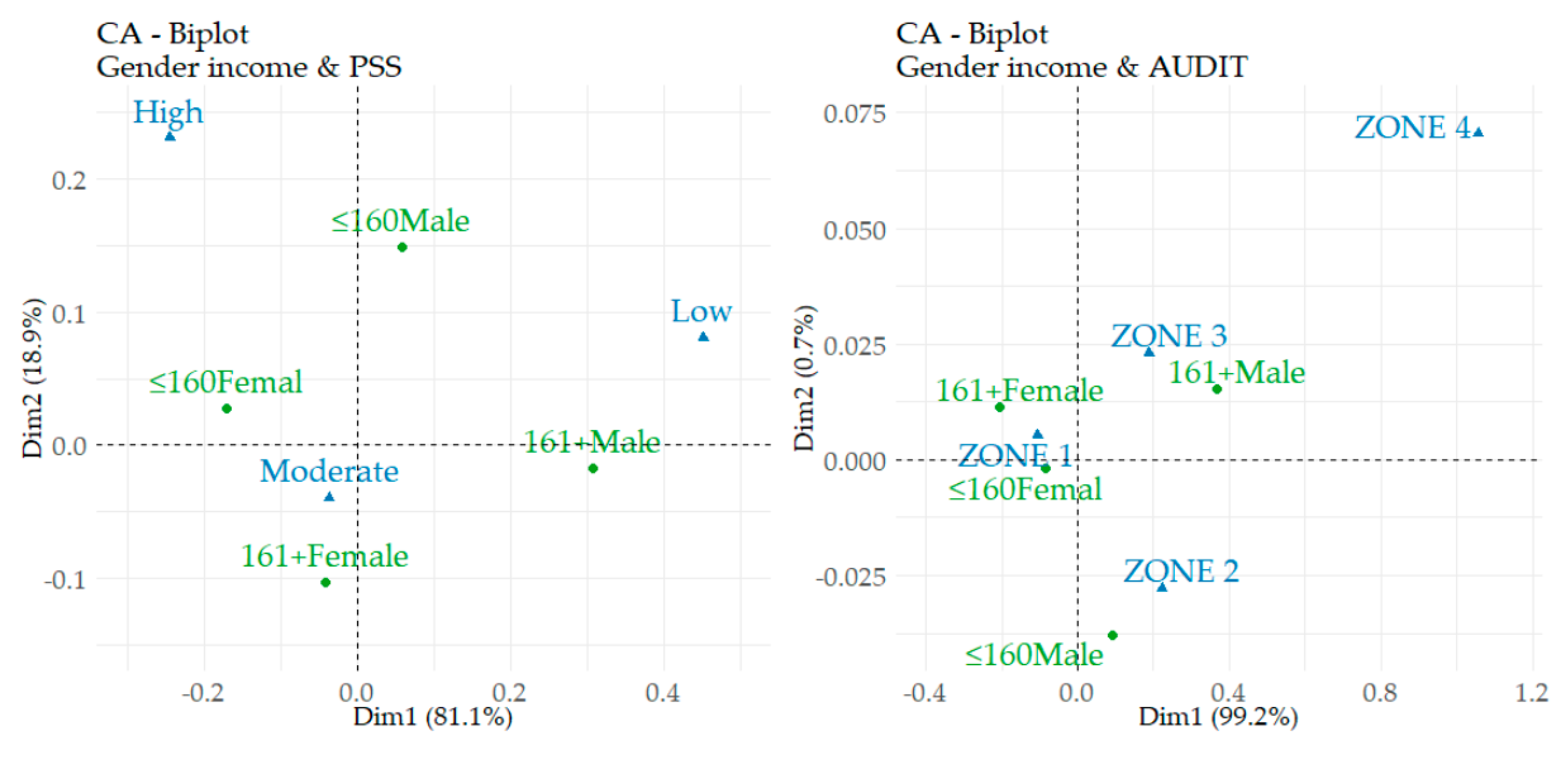
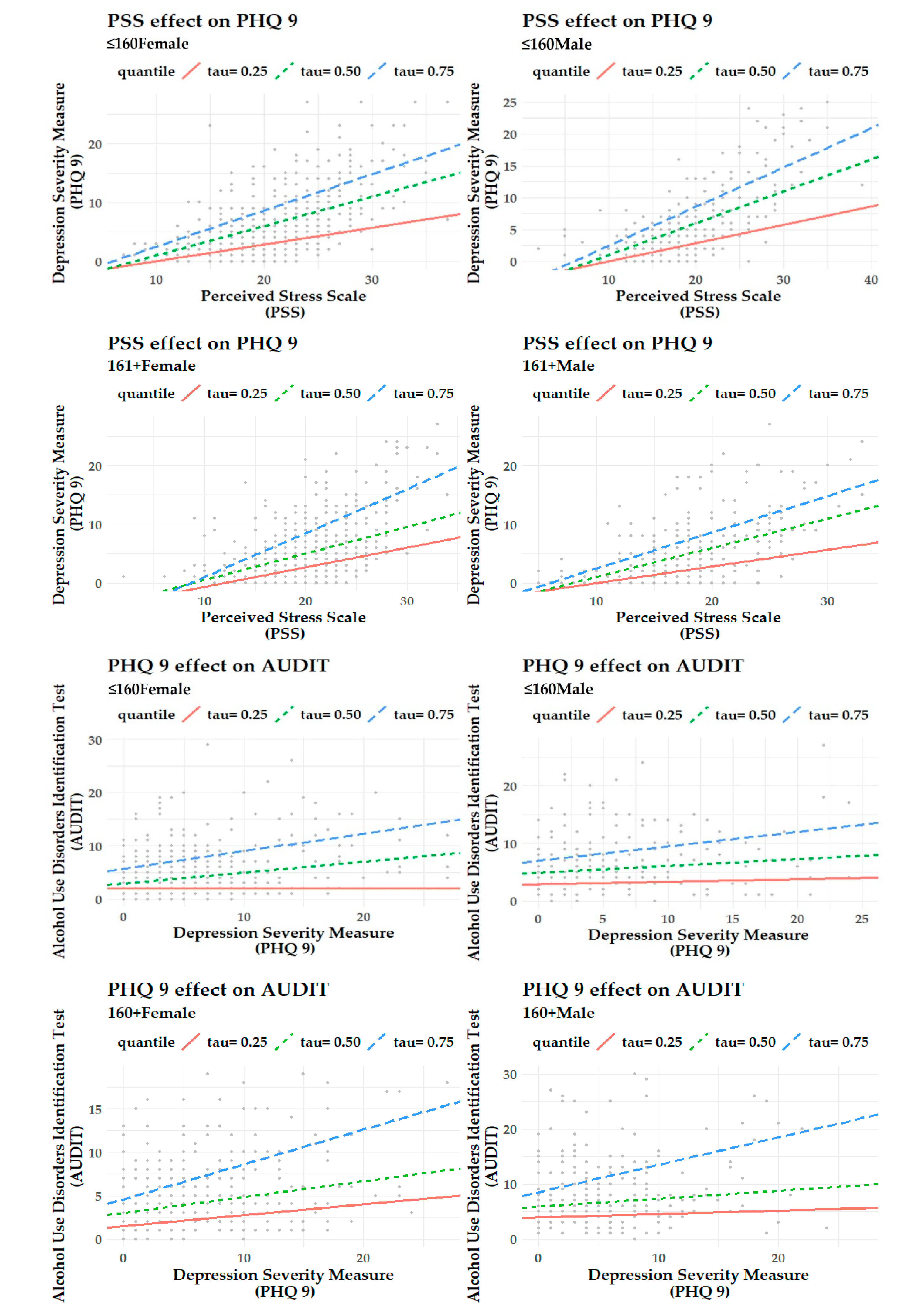
4.2. Relational Part
5. Discussion
5.1. Prevalence and Levels of Stress, Depression, and Alcohol Use Disorders of Slovak Students in an International Comparison
5.2. Effects within the Analysed Mental and Behavioural Disorders
5.3. Practical Implications and Interventions
6. Conclusions
6.1. Limitations of the Study
6.2. Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Blanco, C.; Okuda, M.; Wright, C.; Hasin, D.S.; Grant, B.F.; Liu, S.M.; Olfson, M. Mental health of college students and their non-college-attending peers results from the national epidemiologic study on alcohol and related conditions. Arch. Gen. Psychiatry 2008, 65, 1429–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Furr, S.R.; Westefeld, J.S.; McConnell, G.N.; Jenkins, J.M. Suicide and depression among college students: A decade later. Prof. Psychol. Res. Pr. 2001, 32, 97–100. [Google Scholar] [CrossRef]
- Robotham, D.; Julian, C. Stress and the higher education student: A critical review of the literature. J. Furth. High. Educ. 2006, 30, 107–117. [Google Scholar] [CrossRef]
- Saleh, D.; Camart, N.; Romo, L. Predictors of stress in college students. Front. Psychol. 2017, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.K.; Kelly, S.J.; Adams, C.E.; Glazebrook, C. A systematic review of studies of depression prevalence in university students. J. Psychiatr. Res. 2013, 47, 391–400. [Google Scholar] [CrossRef]
- El Ansari, W.; Stock, C.; Mills, C. Is alcohol consumption associated with poor academic achievement in university students? Int. J. Prev. Med. 2013, 4, 1175–1188. [Google Scholar]
- Rogowska, A.M. Problematic use of psychoactive substances in undergraduates: A comparison of four patterns of substance use. J. Subst. Use 2016, 21, 304–308. [Google Scholar] [CrossRef]
- Dawson, D.A.; Grant, B.F.; Stinson, F.S.; Chou, P.S. Another look at heavy episodic drinking and alcohol use disorders among college and noncollege youth. J. Stud. Alcohol 2004, 65, 477–488. [Google Scholar] [CrossRef]
- Chavan, B.S.; Das, S.; Garg, R.; Puri, S.; Banavaram, A.B.A. Disability and socio-economic impact of mental disorders in the state of Punjab, India: Findings from national mental health survey, 2015–2016. Int. J. Soc. Psychiatry 2018, 64, 589–596. [Google Scholar] [CrossRef]
- Dewa, C.S.; McDaid, D. Investing in the mental health of the labor force: Epidemiological and economic impact of mental health disabilities in the workplace. In Work Accommodation and Retention in Mental Health; Schultz, I.Z., Rogers, E.S., Eds.; Springer: New York, NY, USA, 2011; pp. 33–51. [Google Scholar] [CrossRef]
- Goetzel, R.Z.; Long, S.R.; Ozminkowski, R.J.; Hawkins, K.; Wang, S.H.; Lynch, W. Health, absence, disability, and presenteeism cost estimates of certain physical and mental health conditions affecting US employers. J. Occup. Environ. Med. 2004, 46, 398–412. [Google Scholar] [CrossRef] [PubMed]
- Mark, T.L.; Levit, K.R.; Buck, J.A.; Coffey, R.M.; Vandivort-Warren, R. Mental health treatment expenditure trends, 1986–2003. Psychiatr. Serv. 2007, 58, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, P.; Yim, R.; Ohinmaa, A.; Eng, K.; Dewa, C.S.; Bland, R.; Block, R.; Slomp, M. Expenditures on mental health and addictions for Canadian provinces in 2003 and 2004. Can. J. Psychiatry 2008, 53, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Broulikova, H.M.; Dlouhy, M.; Winkler, P. Expenditures on mental health care in the Czech Republic in 2015. Psychiatr. Q. 2020, 91, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Chadimova, K.; Mlcoch, T.; Dolejsi, D.; Hajickova, B.; Mazalova, M.; Lamblova, K.; Dolezal, T. The economic burden of alcohol consumption in the Czech Republic. Value Health 2019, 22, S686. [Google Scholar] [CrossRef]
- Laramee, P.; Kusel, J.; Leonard, S.; Aubin, H.J.; Francois, C.; Daeppen, J.B. The economic burden of alcohol dependence in Europe. Alcohol Alcohol. 2013, 48, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Manthey, J.; Laramee, P.; Parrott, S.; Rehm, J. Economic burden associated with alcohol dependence in a German primary care sample: A bottom-up study. BMC Public Health 2016, 16, 906. [Google Scholar] [CrossRef] [Green Version]
- Baumberg, B. The global economic burden of alcohol: A review and some suggestions. Drug Alcohol Rev. 2006, 25, 537–551. [Google Scholar] [CrossRef]
- Weycker, D.; Erder, H.; Edelsberg, J.; Holder, H.; Oster, G. Economic burden of alcoholism and alcohol abuse in a us managed-care setting. Value Health 2007, 10, A80. [Google Scholar] [CrossRef]
- Rehm, J.; Mathers, C.; Popova, S.; Thavorncharoensap, M.; Teerawattananon, Y.; Patra, J. Alcohol and Global Health 1 Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009, 373, 2223–2233. [Google Scholar] [CrossRef]
- Lyszczarz, B. Production losses associated with alcohol-attributable mortality in the European Union. Int. J. Environ. Res. Public Health 2019, 16, 3536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohao, F. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, P. Stress and health related quality of life of Nepalese students studying in South Korea: A cross sectional study. Health Qual. Life Outcomes 2012, 10, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, X.; Alenzi, E.O.; Dwibedi, N. Impact of perceived stress, perceived social support, and personality on the perceived health status among West Virginia University students. Value Health 2016, 19, A191. [Google Scholar] [CrossRef]
- Casuso-Holgado, M.J.; Moreno-Morales, N.; Labajos-Manzanares, M.T.; Montero-Bancalero, F.J. The association between perceived health symptoms and academic stress in Spanish higher education students. Eur. J. Educ. Psychol. 2019, 12, 109–123. [Google Scholar] [CrossRef]
- Gorter, R.; Freeman, R.; Hammen, S.; Murtomaa, H.; Blinkhorn, A.; Humphris, G. Psychological stress and health in undergraduate dental students: Fifth year outcomes compared with first year baseline results from five European dental schools. Eur. J. Dent. Educ. 2008, 12, 61–68. [Google Scholar] [CrossRef]
- Mikolajczyk, R.T.; El Ansari, W.; Maxwell, A.E. Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 2009, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Calderon, R.; Pupanead, S.; Prachakul, W.; Kim, G. Happiness, perceived stress, psychological well-being, and health behaviors of Thai university students: Preliminary results from a multinational study on well-being. J. Am. Coll. Health 2019. [Google Scholar] [CrossRef]
- Choi, J. Impact of stress levels on eating behaviors among college students. Nutrients 2020, 12, 1241. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Orucu, M.C.; Demir, A. Psychometric evaluation of perceived stress scale for Turkish university students. Stress Health 2009, 25, 103–109. [Google Scholar] [CrossRef]
- Roberti, J.W.; Harrington, L.N.; Storch, E.A. Further psychometric support for the 10-item version of the perceived stress scale. J. Coll. Couns. 2006, 9, 135–147. [Google Scholar] [CrossRef]
- Lee, E.H.; Chung, B.Y.; Suh, C.H.; Jung, J.Y. Korean versions of the Perceived Stress Scale (PSS-14, 10 and 4): Psychometric evaluation in patients with chronic disease. Scand. J. Caring Sci. 2015, 29, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.; Bartlett, D.; Andiappan, M.; Cabot, L. Students’ perceived stress and perception of barriers to effective study: Impact on academic performance in examinations. Br. Dent. J. 2015, 219, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Saleh, D.; Camart, N.; Sbeira, F.; Romo, L. Can we learn to manage stress? A randomized controlled trial carried out on university students. PLoS ONE 2018, 13, e0200997. [Google Scholar] [CrossRef] [Green Version]
- Makhubela, M. Assessing psychological stress in South African university students: Measurement validity of the perceived stress scale (PSS-10) in diverse populations. Curr. Psychol. 2020. [Google Scholar] [CrossRef]
- Ráczová, B.; Hricová, M.; Lovašová, S. Verification of psychometric properties of the Slovak version of the PSS-10 survey (Perceived Stress Scale) on a sample of assisting professionals. Cesk. Psychol. 2018, 62, 552–564. [Google Scholar]
- Orosova, O.; Benka, J.; Sebena, R.; Gajdosova, B. Optimism, perceived stress and problematic internet use among Slovak university students. In Psychology Applications & Developments; Pracana, C., Ed.; Portuguese Association of Psychoanalysis and Psychoanalytic Psychotherapy, inScience Press: Lisboa, Portugal, 2014; pp. 306–315. [Google Scholar]
- Huang, Y.; Shrey, G.; Sansgiry, S.S. Characteristics of students with high perceived stress with advanced pharmacy practice experiences. Res. Social Admin. Pharm. 2019, 15, e38–e39. [Google Scholar] [CrossRef]
- Drachev, S.N.; Stangvaltaite-Mouhat, L.; Bolstad, N.L.; Johnsen, J.A.K.; Yushmanova, T.N.; Trovik, T.A. Perceived stress and associated factors in Russian medical and dental students: A cross-sectional study in North-West Russia. Int. J. Environ. Res. Public Health 2020, 17, 5390. [Google Scholar] [CrossRef]
- Machul, M.; Bieniak, M.; Chaldas-Majdanska, J.; Bak, J.; Chrzan-Rodak, A.; Mazurek, P.; Pawlowski, P.; Makuch-Kusmierz, D.; Obuchowska, A.; Bartoszek, A.; et al. Lifestyle practices, satisfaction with life and the level of perceived stress of Polish and foreign medical students studying in Poland. Int. J. Environ. Res. Public Health 2020, 17, 4445. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Grochans, E.; Kaducakova, H.; Mikla, M.; Jozwik, M. Analysis of the relationship between stress intensity and coping strategy and the quality of life of nursing students in Poland, Spain and Slovakia. Int. J. Environ. Res. Public Health 2020, 17, 4536. [Google Scholar] [CrossRef] [PubMed]
- Seedhom, A.E.; Kamel, E.G.; Mohammed, E.S.; Raouf, N.R. Predictors of perceived stress among medical and nonmedical college students, Minia, Egypt. Int. J. Prev. Med. 2019, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Olfert, M.D.; Barr, M.L.; Charlier, C.C.; Greene, G.W.; Zhou, W.; Colby, S.E. Sex differences in lifestyle behaviors among US college freshmen. Int. J. Environ. Res. Public Health 2019, 16, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavallo, P.; Carpinelli, L.; Savarese, G. Perceived stress and bruxism in university students. BMC Res. Notes 2016, 9, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denovan, A.; Dagnall, N.; Dhingra, K.; Grogan, S. Evaluating the Perceived Stress Scale among UK university students: Implications for stress measurement and management. Stud. High. Educ. 2019, 44, 120–133. [Google Scholar] [CrossRef]
- Tavolacci, M.P.; Ladner, J.; Grigioni, S.; Richard, L.; Villet, H.; Dechelotte, P. Prevalence and association of perceived stress, substance use and behavioral addictions: A cross-sectional study among university students in France, 2009–2011. BMC Public Health 2013, 13, 724. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, M.; Joneborg, N.; Runeson, B. Stress and depression among medical students: A cross-sectional study. Med. Educ. 2005, 39, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Mosimah, C.I.; Sizemore, G.; Goyat, R.; Dwibedi, N. Impact of mindful self-care and perceived stress on the health related quality of life among young-adult students in West Virginia. J. Hum. Behav. Soc. Environ. 2019, 29, 26–36. [Google Scholar] [CrossRef]
- Cohen, S.; Janicki-Deverts, D. Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 2009. J. Appl. Soc. Psychol. 2012, 42, 1320–1334. [Google Scholar] [CrossRef]
- Klein, E.M.; Brahler, E.; Dreier, M.; Reinecke, L.; Muller, K.W.; Schmutzer, G.; Wolfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale—Psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef] [Green Version]
- Ruisoto, P.; Lopez-Guerra, V.M.; Paladines, M.B.; Vaca, S.L.; Cacho, R. Psychometric properties of the three versions of the Perceived Stress Scale in Ecuador. Physiol. Behav. 2020, 224, 113045. [Google Scholar] [CrossRef]
- Miron, J.; Casteras, D.P.; Gil, M.V.; Ventura, G.N.; Alvarez, N.C.; Goldberg, X. Perceived stress, anxiety and depression among undergraduate students. Eur. Neuropsychopharmacol. 2019, 29, S589. [Google Scholar] [CrossRef]
- Iorga, M.; Dondas, C.; Zugun-Eloae, C. Depressed as freshmen, stressed as seniors: The relationship between depression, perceived stress and academic results among medical students. Behav. Sci. 2018, 8, 70. [Google Scholar] [CrossRef] [Green Version]
- Kaya, C. Factors impacting depression severity among Turkish college students. Curr. Psychol. 2020. [Google Scholar] [CrossRef]
- Zajenkowska, A.; Jasielska, D.; Melonowska, J. Stress and sensitivity to frustration predicting depression among young adults in Poland and Korea—Psychological and philosophical explanations. Curr. Psychol. 2019, 38, 769–774. [Google Scholar] [CrossRef] [Green Version]
- Hou, X.L.; Wang, H.Z.; Hu, T.Q.; Gentile, D.A.; Gaskin, J.; Wang, J.L. The relationship between perceived stress and problematic social networking site use among Chinese college students. J. Behav. Addict. 2019, 8, 306–317. [Google Scholar] [CrossRef]
- Kessler, R.C.; Bromet, E.J. The epidemiology of depression across cultures. Annu. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Arusha, A.R.; Biswas, R.K. Prevalence of stress, anxiety and depression due to examination in Bangladeshi youths: A pilot study. Child. Youth Serv. Rev. 2020, 116, 105254. [Google Scholar] [CrossRef]
- Li, W.; Yin, J.; Cai, X.; Cheng, X.; Wang, Y. Association between sleep duration and quality and depressive symptoms among university students: A cross-sectional study. PLoS ONE 2020, 15, e0238811. [Google Scholar] [CrossRef]
- Beiter, R.; Nash, R.; McCrady, M.; Rhoades, D.; Linscomb, M.; Clarahan, M.; Sammut, S. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J. Affect. Disord. 2015, 173, 90–96. [Google Scholar] [CrossRef]
- Sarokhani, D.; Delpisheh, A.; Veisani, Y.; Sarokhani, M.T.; Manesh, R.E.; Sayehmiri, K. Prevalence of depression among university students: A systematic review and meta-analysis study. Depress. Res. Treat. 2013, 2013, 373857. [Google Scholar] [CrossRef]
- Ludwig, A.B.; Burton, W.; Weingarten, J.; Milan, F.; Myers, D.C.; Kligler, B. Depression and stress amongst undergraduate medical students. BMC Med. Educ. 2015, 15, 141. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The Patient Health Questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Garlow, S.J.; Rosenberg, J.; Moore, J.D.; Haas, A.P.; Koestner, B.; Hendin, H.; Nemeroff, C.B. Depression, desperation, and suicidal ideation in college students: Results from the American foundation for suicide prevention college screening project at Emory university. Depress. Anxiety 2008, 25, 482–488. [Google Scholar] [CrossRef]
- Miranda, C.A.C.; Scoppetta, O. Factorial structure of the Patient Health Questionnaire-9 as a depression screening instrument for university students in Cartagena, Colombia. Psychiatry Res. 2018, 269, 425–429. [Google Scholar] [CrossRef]
- Alsubaie, M.M.; Stain, H.J.; Webster, L.A.D.; Wadman, R. The role of sources of social support on depression and quality of life for university students. Int. J. Adolesc. Youth 2019, 24, 484–496. [Google Scholar] [CrossRef] [Green Version]
- Grant, F.; Guille, C.; Sen, S. Well-Being and the risk of depression under stress. PLoS ONE 2013, 8, e67395. [Google Scholar] [CrossRef]
- Honney, K.; Buszewicz, M.; Coppola, W.; Griffin, M. Comparison of levels of depression in medical and non-medical students. Clin. Teach. 2010, 7, 180–184. [Google Scholar] [CrossRef]
- Lipson, S.K.; Zhou, S.; Wagner, B.; Beck, K.; Eisenberg, D. Major differences: Variations in undergraduate and graduate student mental health and treatment utilization across academic disciplines. J. Coll. Stud. Psychother. 2016, 30, 23–41. [Google Scholar] [CrossRef]
- Hajduk, M.; Heretik, A.; Vaseckova, B.; Forgacova, L.; Pecenak, J. Prevalence and correlations of depression and anxiety among Slovak college students. Bratisl. Lek. Listy—Bratisl. Med. J. 2019, 120, 695–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahas, A.R.M.F.; Elkalmi, R.M.; Al-Shami, A.M.; Elsayed, T.M. Prevalence of depression among health sciences students: Findings from a public university in Malaysia. J. Pharm. Bioallied Sci. 2019, 11, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Xu, J.; Rief, W. Are comparisons of mental disorders between Chinese and German students possible? An examination of measurement invariance for the PHQ-15, PHQ-9 and GAD-7. BMC Psychiatry 2020, 20, 480. [Google Scholar] [CrossRef] [PubMed]
- Milic, J.; Skrlec, I.; Vranjes, I.M.; Podgornjak, M.; Heffer, M. High levels of depression and anxiety among Croatian medical and nursing students and the correlation between subjective happiness and personality traits. Int. Rev. Psychiatry 2019, 31, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.; Lee, Y.; Han, C.; Pae, C.U.; Yoon, H.K.; Patkar, A.A.; Steffens, D.C.; Kim, Y.K. Usefulness of the Patient Health Questionnaire-9 for Korean medical students. Acad. Psychiatry 2014, 38, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Ngasa, S.N.; Sama, C.B.; Dzekem, B.S.; Nforchu, K.N.; Tindong, M.; Aroke, D.; Dimala, C.A. Prevalence and factors associated with depression among medical students in Cameroon: A cross-sectional study. BMC Psychiatry 2017, 17, 216. [Google Scholar] [CrossRef] [Green Version]
- Lafay, N.; Manzanera, C.; Papet, N.; Marcelli, D.; Senon, J.L. Depression states during post-adolescence. Results of a study in 1521 students of Poitiers University. Ann. Med. Psychol. 2003, 161, 147–151. [Google Scholar] [CrossRef]
- Sebena, R.; El Ansari, W.; Stock, C.; Orosova, O.; Mikolajczyk, R. Are perceived stress, depressive symptoms and religiosity associated with alcohol consumption? A survey of freshmen university students across five European countries. Subst. Abuse Treat. Prev. Policy 2012, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Kawaida, K.; Yoshimoto, H.; Goto, R.; Saito, G.; Ogai, Y.; Morita, N.; Saito, T.; Takahashi, S. Reasons for drinking among college students in Japan: A cross sectional study. Tohoku J. Exp. Med. 2018, 246, 183–189. [Google Scholar] [CrossRef] [Green Version]
- White, A.; Hingson, R. The burden of alcohol use: Excessive alcohol consumption and related consequences among college students. Alcohol Res. 2013, 35, 201–218. [Google Scholar] [PubMed]
- Dos Reis, T.G.; de Oliveira, L.C.M. Alcohol consumption among students of a Brazilian public university and consequences associated with this consumption. Biosci. J. 2017, 33, 1371–1380. [Google Scholar] [CrossRef] [Green Version]
- Boden, J.M.; Fergusson, D.M. Alcohol and depression. Addiction 2011, 106, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Boschloo, L.; Vogelzangs, N.; van den Brink, W.; Smit, J.H.; Veltman, D.J.; Beekman, A.T.F.; Penninx, B.W.J.H. Alcohol use disorders and the course of depressive and anxiety disorders. Br. J. Psychiatry 2012, 200, 476–484. [Google Scholar] [CrossRef] [Green Version]
- Stock, C.; Mikolajczyk, R.; Bloomfield, K.; Maxwell, A.E.; Ozcebe, H.; Petkeviciene, J.; Naydenova, V.; Marin-Fernandez, B.; El-Ansari, W.; Kramer, A. Alcohol consumption and attitudes towards banning alcohol sales on campus among European university students. Public Health 2009, 123, 122–129. [Google Scholar] [CrossRef]
- Dos Santos, D.T.; Nazario, F.P.; Freitas, R.A.; Henriques, V.M.; de Paiva, I.S. Alcohol abuse and dependence among Brazilian medical students: Association to sociodemographic variables, anxiety and depression. J. Subst. Use 2019, 24, 285–292. [Google Scholar] [CrossRef]
- Ndegwa, S.; Munene, A.; Oladipo, R. Factors influencing alcohol use among university students in a Kenyan university. Afr. J. Clin. Psychol. 2017, 1, 135–153. [Google Scholar]
- Musiat, P.; Conrod, P.; Treasure, J.; Tylee, A.; Williams, C.; Schmidt, U. Targeted prevention of common mental health disorders in university students: Randomised controlled trial of a transdiagnostic trait-focused web-based intervention. PLoS ONE 2014, 9, e93621. [Google Scholar] [CrossRef] [Green Version]
- Selkie, E.M.; Kota, R.; Chan, Y.F.; Moreno, M. Cyberbullying, depression, and problem alcohol use in female college students: A multisite study. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Talih, F.; Daher, M.; Daou, D.; Ajaltouni, J. Examining burnout, depression, and attitudes regarding drug use among Lebanese medical students during the 4 years of medical school. Acad. Psychiatry 2018, 42, 288–296. [Google Scholar] [CrossRef]
- Said, D.; Kypri, K.; Bowman, J. Risk factors for mental disorder among university students in Australia: Findings from a web-based cross-sectional survey. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Fleming, M.F.; Barry, K.L.; Macdonald, R. The Alcohol-Use Disorders Identification Test (AUDIT) in a college sample. Int. J. Addict. 1991, 26, 1173–1185. [Google Scholar] [CrossRef] [PubMed]
- Kokotailo, P.K.; Egan, J.; Gangnon, R.; Brown, D.; Mundt, M.; Fleming, M. Validity of the alcohol use disorders identification test in college students. Alcohol. Clin. Exp. Res. 2004, 28, 914–920. [Google Scholar] [CrossRef] [PubMed]
- DeMartini, K.S.; Carey, K.B. Optimizing the use of the AUDIT for alcohol screening in college students. Psychol. Assess. 2012, 24, 954–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomas, M.T.C.; Costa, J.A.G.; Motos-Selles, P.; Beitia, M.D.S.; Cadaveira, F. The utility of the Alcohol Use Disorders Identification Test (AUDIT) for the analysis of binge drinking in university students. Psicothema 2017, 29, 229–235. [Google Scholar] [CrossRef]
- Madson, M.B.; Schutts, J.W.; Jordan, H.R.; Villarosa-Hurlocker, M.C.; Whitley, R.B.; Mohn, R.S. Identifying at-risk college student drinkers with the AUDIT-US: A receiver operating characteristic curve analysis. Assessment 2020, 27, 1089–1099. [Google Scholar] [CrossRef]
- Lopez, V.; Paladines, B.; Vaca, S.; Cacho, R.; Fernandez-Montalvo, J.; Ruisoto, P. Psychometric properties and factor structure of an Ecuadorian version of the Alcohol Use Disorders Identification Test (AUDIT) in college students. PLoS ONE 2019, 14, e0219618. [Google Scholar] [CrossRef]
- Caamano-Isorna, F.; Corral, M.; Parada, M.; Cadaveira, F. Factors associated with risky consumption and heavy episodic drinking among Spanish university students. J. Stud. Alcohol Drugs 2008, 69, 308–312. [Google Scholar] [CrossRef]
- Heather, N.; Partington, S.; Partington, E.; Longstaff, F.; Allsop, S.; Jankowski, M.; Wareham, H.; Gibson, A.S. Alcohol use disorders and hazardous drinking among undergraduates at English universities. Alcohol Alcohol. 2011, 46, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Andersson, C.; Johnsson, K.O.; Berglund, M.; Ojehagen, A. Alcohol involvement in Swedish University freshmen related to gender, age, serious relationship and family history of alcohol problems. Alcohol Alcohol. 2007, 42, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Villarosa-Hurlocker, M.C.; Schutts, J.W.; Madson, M.B.; Jordan, H.R.; Whitley, R.B.; Mohn, R.C. Screening for alcohol use disorders in college student drinkers with the AUDIT and the USAUDIT: A receiver operating characteristic curve analysis. Am. J. Drug Alcohol Abuse 2020. [Google Scholar] [CrossRef] [PubMed]
- Wicki, M.; Kuntsche, E.; Gmel, G. Drinking at European universities? A review of students’ alcohol use. Addict. Behav. 2010, 35, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.G.; Premarajan, K.C.; Subitha, L.; Suguna, E.; Vinayagamoorthy, V.K. Prevalence and pattern of alcohol consumption using Alcohol Use Disorders Identification Test (AUDIT) in rural Tamil Nadu, India. J. Clin. Diagn. Res. 2013, 7, 1637–1639. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. 2013. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 14 November 2020).
- International Society of Addiction Journal Editors. The Farmington Consensus. 2017. Available online: http://www.isaje.net/farmington-consensus.html (accessed on 14 November 2020).
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health. The Claremont Symposium on Applied Social Psychology; Spacapan, S., Oskamp, S., Eds.; Sage Publications: Newbury Park, CA, USA, 1988; pp. 31–67. [Google Scholar]
- Babor, T.F.; Robaina, K. The Alcohol Use Disorders Identification Test (AUDIT): A review of graded severity algorithms and national adaptations. Int. J. Alcohol Drug Res. 2016, 5, 17–24. [Google Scholar] [CrossRef]
- Zhang, N.; Henderson, C.N.R. Predicting stress and test anxiety among 1st-year chiropractic students. J. Chiropr. Educ. 2019, 33, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Mu, W.; Zhu, D.; Wang, Y.; Li, F.; Ye, L.; Wang, K.; Zhou, M. Three-wave longitudinal survey on the relationship between neuroticism and depressive symptoms of first-year college students: Addictive use of social media as a moderated mediator. Int. J. Environ. Res. Public Health 2020, 17, 6074. [Google Scholar] [CrossRef]
- Seidel, E.J.; Mohlman, J.; Basch, C.H.; Fera, J.; Cosgrove, A.; Ethan, D. Communicating mental health support to college students during COVID-19: An exploration of website messaging. J. Community Health 2020. [Google Scholar] [CrossRef]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef]
- Eisenberg, D.; Golberstein, E.; Gollust, S.E. Help-seeking and access to mental health care in a university student population. Med. Care 2007, 45, 594–601. [Google Scholar] [CrossRef]
- Mental Health Financing in Six Eastern European Countries. Available online: https://www.researchgate.net/publication/288689289_Mental_health_financing_in_Six_Eastern_European_Countries (accessed on 27 November 2020).
- Dlouhy, M. Mental health policy in Eastern Europe: A comparative analysis of seven mental health systems. BMC Health Serv. Res. 2014, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Dragašek, J.; Nawka, A. Mental healthcare in the Slovak Republic: Current situation and future challenges. Int. Psychiatry 2010, 7, 88–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDaid, D.; Knapp, M.; Raja, S. Barriers in the mind: Promoting an economic case for mental health in low- and middle-income countries. World Psychiatry 2008, 7, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarikhani, Y.; Bastani, P.; Rafiee, M.; Kavosi, Z.; Ravangard, R. Key barriers to the provision and utilization of mental health services in low-and middle-income countries: A scope study. Community Ment. Health J. 2020. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency | Percent |
|---|---|---|
| Degree of study: | ||
| 1st degree | 1053 | 69.1 |
| 2nd degree | 379 | 24.9 |
| Combined 1st and 2nd | 35 | 2.3 |
| 3rd degree | 56 | 3.7 |
| Year of study: | ||
| 1st | 555 | 36.4 |
| 2nd | 475 | 31.2 |
| 3rd | 265 | 17.4 |
| 4th | 94 | 6.2 |
| 5th | 124 | 8.1 |
| 6th | 10 | 0.7 |
| Form of study: | ||
| Full-time | 1417 | 93.0 |
| Part-time | 106 | 7.0 |
| Descriptive Characteristics | PSS | PHQ 9 | AUDIT | |
|---|---|---|---|---|
| All | Mean | 5.95 | 5.73 | 6.01 |
| 95% CI | 5.77–6.12 | 5.45–6.01 | 5.76–6.27 | |
| Median | 6 | 4 | 5 | |
| Std. Deviation | 3.33 | 5.22 | 4.83 | |
| Female | Mean | 6.98 | 5.76 | 5.15 |
| 95% CI | 6.77–7.19 | 5.42–6.09 | 4.87–5.42 | |
| Median | 7 | 4 | 4 | |
| Std. Deviation | 3.24 | 5.12 | 4.15 | |
| Male | Mean | 4.11 | 5.68 | 7.54 |
| 95% CI | 3.88–4.34 | 5.21–6.16 | 7.05–8.02 | |
| Median | 4 | 4 | 6 | |
| Std. Deviation | 2.62 | 5.39 | 5.53 | |
| ≤160 | Mean | 6.13 | 5.98 | 5.76 |
| 95% CI | 5.88–6.38 | 5.58–6.37 | 5.41–6.11 | |
| Median | 6 | 5 | 4.5 | |
| Std. Deviation | 3.29 | 5.28 | 4.61 | |
| 161+ | Mean | 5.76 | 5.49 | 6.26 |
| 95% CI | 5.51–6.01 | 5.11–5.87 | 5.88–6.63 | |
| Median | 5 | 4 | 5 | |
| Std. Deviation | 3.36 | 5.14 | 5.03 | |
| AUDIT | PHQ 9 | ||||||
|---|---|---|---|---|---|---|---|
| None | Mild | Moderate | Moderately Severe | Severe | |||
| PSS | Low | M | 5.54 | 6.06 | 9.00 | - | - |
| Med | 5.00 | 6.00 | 9.50 | - | - | ||
| Moderate | M | 5.20 | 6.23 | 6.54 | 9.30 | 11.67 | |
| Med | 4.00 | 5.50 | 5.00 | 8.00 | 6.00 | ||
| High | M | 7.00 | 6.71 | 6.88 | 7.63 | 9.35 | |
| Med | 6.50 | 5.00 | 5.00 | 6.00 | 6.50 | ||
| Between Variable: | Statistic | PSS (p-Value) | PHQ 9 (p-Value) | AUDIT (p-Value) |
|---|---|---|---|---|
| Gender | W | 212,825.0 (<0.001) | 255,215.5 (0.115) | 157,865.5 (<0.001) |
| Income | W | 250,860.5 (<0.001) | 265,993.5 (0.007) | 225,313.5 (0.077) |
| Gender-Income | Χ2 | 62.01 (<0.001) | 9.00 (0.029) | 85.58 (<0.001) |
| Relation | Dimension | Eigenvalue | Variance% | χ2 (Sig) |
|---|---|---|---|---|
| Gender-income & PSS | Dim.1 | 0.0302 | 81.12 | 56.78 (<0.001) |
| Dim.2 | 0.0070 | 18.88 | ||
| Gender-income & PHQ 9 | Dim.1 | 0.0041 | 55.62 | 11.10 (0.5205) |
| Dim.2 | 0.0022 | 29.89 | ||
| Dim.3 | 0.0011 | 14.49 | ||
| Gender-income & AUDIT | Dim.1 | 4.43 × 10−2 | 99.25 | 61.75 (<0.001) |
| Dim.2 | 3.13 × 10−4 | 0.70 | ||
| Dim.3 | 2.32 × 10−5 | 0.05 |
| λ | Coef. | ≤160 Female | ≤160 Male | 161+ Female | 161+ Male |
|---|---|---|---|---|---|
| PSS -> PHQ 9 | |||||
| 0.25 | Intercept (sig.) | −4.77 (<0.001) | −4.83 (<0.001) | −4.00 (<0.001) | −2.86 (0.009) |
| Predictor–PSS (Sig) | 0.38 (<0.001) | 0.42 (<0.001) | 0.33 (<0.001) | 0.29 (<0.001) | |
| 0.5 | Intercept (sig.) | −5.00 (<0.001) | −4.91 (<0.001) | −4.09 (0.002) | −4.00 (<0.001) |
| Predictor–PSS (Sig) | 0.50 (<0.001) | 0.55 (<0.001) | 0.45 (<0.001) | 0.50 (<0.001) | |
| 0.75 | Intercept (sig.) | −5.33 (<0.001) | −6.14 (<0.001) | −6.50 (<0.001) | −3.69 (<0.001) |
| Predictor–PSS (Sig) | 0.67 (<0.001) | 0.76 (<0.001) | 0.75 (<0.001) | 0.62 (<0.001) | |
| PHQ 9 -> AUDIT | |||||
| 0.25 | Intercept (sig.) | 2.00 (<0.001) | 2.91 (<0.001) | 1.50(<0.001) | 3.88 (<0.001) |
| Predictor–PHQ 9 (Sig) | 0.00 (1.000) | 0.05 (0.574) | 0.13 (0.004) | 0.06 (0.444) | |
| 0.5 | Intercept (sig.) | 3.00 (<0.001) | 4.88 (<0.001) | 3.00 (<0.001) | 5.86 (<0.001) |
| Predictor–PHQ 9 (Sig) | 0.20 (0.002) | 0.12 (0.234) | 0.18 (0.002) | 0.14 (0.201) | |
| 0.75 | Intercept (sig.) | 5.67 (<0.001) | 7.00 (<0.001) | 4.60 (<0.001) | 8.50 (<0.001) |
| Predictor–PHQ 9 (Sig) | 0.33 (<0.001) | 0.25 (0.021) | 0.40 (<0.001) | 0.50 (<0.001) | |
| Gender Income | Coefficient | PSS & PHQ 9 | PHQ 9 & AUDIT |
|---|---|---|---|
| All | Coef (sig) | 0.557 (<0.001) | 0.186 (<0.001) |
| ≤160 Female | Coef (sig) | 0.573 (<0.001) | 0.198 (<0.001) |
| ≤160 Male | Coef (sig) | 0.636 (<0.001) | 0.141 (0.039) |
| 161+ Female | Coef (sig) | 0.484 (<0.001) | 0.281 (<0.001) |
| 161+ Male | Coef (sig) | 0.569 (<0.001) | 0.145 (0.014) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavurova, B.; Ivankova, V.; Rigelsky, M. Relationships between Perceived Stress, Depression and Alcohol Use Disorders in University Students during the COVID-19 Pandemic: A Socio-Economic Dimension. Int. J. Environ. Res. Public Health 2020, 17, 8853. https://doi.org/10.3390/ijerph17238853
Gavurova B, Ivankova V, Rigelsky M. Relationships between Perceived Stress, Depression and Alcohol Use Disorders in University Students during the COVID-19 Pandemic: A Socio-Economic Dimension. International Journal of Environmental Research and Public Health. 2020; 17(23):8853. https://doi.org/10.3390/ijerph17238853
Chicago/Turabian StyleGavurova, Beata, Viera Ivankova, and Martin Rigelsky. 2020. "Relationships between Perceived Stress, Depression and Alcohol Use Disorders in University Students during the COVID-19 Pandemic: A Socio-Economic Dimension" International Journal of Environmental Research and Public Health 17, no. 23: 8853. https://doi.org/10.3390/ijerph17238853