Gender Differences in Oesophageal Squamous Cell Carcinoma in a South African Tertiary Hospital

Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, Y. Epidemiology of esophageal cancer. World J. Gastroenterol. 2013, 19, 5598–5606. [Google Scholar] [CrossRef]
- He, L.; Jin-Hu, F.; You-Lin, Q.; Liang, H.; Fan, J.; Qiao, Y. Epidemiology, etiology, and prevention of esophageal squamous cell carcinoma in China. Cancer Biol. Med. 2017, 14, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abnet, C.C.; Arnold, M.; Wei, W. Epidemiology of Esophageal Squamous Cell Carcinoma. Gastroenterology 2018, 154, 360–373. [Google Scholar] [CrossRef] [PubMed]
- Bagnardi, V.; Blangiardo, M.; La Vecchia, C.; Corrao, G. A meta-analysis of alcohol drinking and cancer risk. Br. J. Cancer 2001, 85, 1700–1705. [Google Scholar] [CrossRef] [PubMed]
- Islami, F.; Fedirko, V.; Tramacere, I.; Bagnardi, V.; Jenab, M.; Scotti, L.; Rota, M.; Corrao, G.; Garavello, W.; Schüz, J.; et al. Alcohol drinking and esophageal squamous cell carcinoma with focus on light-drinkers and never-smokers: A systematic review and meta-analysis. Int. J. Cancer 2011, 129, 2473–2484. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, S.; Miyamoto, S.; Kikuchi, O.; Goto, T.; Amanuma, Y.; Muto, M. Recent Advances From Basic and Clinical Studies of Esophageal Squamous Cell Carcinoma. Gastroenterology 2015, 149, 1700–1715. [Google Scholar] [CrossRef] [Green Version]
- Mao, W.; Zheng, W.-H.; Ling, Z.-Q. Epidemiologic risk factors for esophageal cancer development. Asian Pac. J. Cancer Prev. 2011, 12, 2461–2466. [Google Scholar]
- Yang, C.S.; Chen, X.; Tu, S. Etiology and Prevention of Esophageal Cancer. Gastrointest. Tumors 2016, 3, 3–16. [Google Scholar] [CrossRef]
- Prabhu, A.; Obi, K.O.; Rubenstein, J.H. The Synergistic Effects of Alcohol and Tobacco Consumption on the Risk of Esophageal Squamous Cell Carcinoma: A Meta-Analysis. Am. J. Gastroenterol. 2014, 109, 822–827. [Google Scholar] [CrossRef]
- McCormack, V.; Menya, D.; Munishi, M.; Dzamalala, C.; Gasmelseed, N.; Roux, M.L.; Assefa, M.; Osano, O.; Watts, M.J.; Mwasamwaja, A.; et al. Informing etiologic research priorities for squamous cell esophageal cancer in Africa: A review of setting-specific exposures to known and putative risk factors. Int. J. Cancer 2016, 140, 259–271. [Google Scholar] [CrossRef] [Green Version]
- Murphy, G.; McCormack, V.; Abedi-Ardekani, B.; Arnold, M.; Camargo, M.C.; Dar, N.A.; Dawsey, S.M.; Etemadi, A.; Fitzgerald, R.C.; Fleischer, D.E.; et al. International cancer seminars: A focus on esophageal squamous cell carcinoma. Ann. Oncol. 2017, 28, 2086–2093. [Google Scholar] [CrossRef] [PubMed]
- Somdyala, N.I.; Bradshaw, D.; Gelderblom, W.C.; Parkin, D.M. Cancer incidence in a rural population of South Africa, 1998–2002. Int. J. Cancer 2010, 127, 2420–2429. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, T.; Wakefield, J.; Hanisch, R.; Bray, F.; Schuz, J.; Joy, E.J.M.; Watts, M.J.; McCormack, V. Africa’s Oesophageal Cancer Corridor: Geographic Variations in Incidence Correlate with Certain Micronutrient Deficiencies. PLoS ONE 2015, 10, e0140107. [Google Scholar] [CrossRef] [Green Version]
- Thrift, A.P. The epidemic of oesophageal carcinoma: Where are we now? Cancer Epidemiol. 2016, 41, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, R.I.; Gaede, B.; Aldous, C. Description of an internal medicine outreach consultant appointment in Western KwaZulu-Natal, South Africa, 2007 to mid-2014. South Afr. Med. J. 2015, 105, 353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics South Africa. Census 2011. Provincial profile: KwaZulu-Natal. Available online: www.statssa.gov.za (accessed on 15 March 2020).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO Obesity Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Mellow, M.H. Endoscopic Laser Therapy for Malignancies Affecting the Esophagus and Gastroesophageal Junction. Arch. Intern. Med. 1985, 145, 1443–1446. [Google Scholar] [CrossRef]
- Azam, F.; Latif, M.F.; Farooq, A.; Tirmazy, S.H.; Alshahrani, S.; Bashir, S.; Bukhari, N. Performance Status Assessment by Using ECOG (Eastern Cooperative Oncology Group) Score for Cancer Patients by Oncology Healthcare Professionals. Case Rep. Oncol. 2019, 12, 728–736. [Google Scholar] [CrossRef]
- Mohan, H. Textbook of Pathology, 6th ed.; Jaypee Brothers Medical Publishing: New Delhi, India, 2015. [Google Scholar]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, N.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Kachala, R. Systematic review: Epidemiology of Oesophageal Cancer in SubSaharan Africa. Malawi Med. J. 2010, 22, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Kamangar, F.; Chow, W.-H.; Abnet, C.C.; Dawsey, S.M. Environmental Causes of Esophageal Cancer. Gastroenterol. Clin. North Am. 2009, 38, 27–57. [Google Scholar] [CrossRef] [Green Version]
- Dandara, C.; Robertson, B.; Dzobo, K.; Moodley, L.; Parker, M.I. Patient and tumour characteristics as prognostic markers for oesophageal cancer: A retrospective analysis of a cohort of patients at Groote Schuur Hospital. Eur. J. Cardio Thoracic Surg. 2015, 49, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Loots, E.; Sartorius, B.; Madiba, T.E.; Mulder, C.J.J.; Clarke, D.L. Oesophageal squamous cell cancer in a South African tertiary hospital: A risk factor and presentation analysis. S. Afr. J. Surg. 2017, 55, 42–46. [Google Scholar] [PubMed]
- Feng, X.-S.; Yang, Y.-T.; Gao, S.-G.; Ru, Y.; Wang, G.-P.; Zhou, B.; Wang, Y.-F.; Zhang, P.-F.; Li, P.-Y.; Liu, Y.-X. Prevalence and age, gender and geographical area distribution of esophageal squamous cell carcinomas in North China from 1985 to 2006. Asian Pac. J. Cancer Prev. 2014, 15, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, P.; Chhabra, S. Effect of smoking on body mass index. A community-based study. Natl. J. Community Med. 2011, 2, 325–330. [Google Scholar]
- Micklesfield, L.K.; Kagura, J.; Munthali, R.J.; Crowther, N.J.; Jaff, N.G.; Gradidge, P.J.; Ramsay, M. Demographic, socio-economic and behavioural correlates of BMI in middle-aged black men and women from urban Johannesburg, South Africa. Glob. Health Action 2018, 11. [Google Scholar] [CrossRef] [Green Version]
- Shisana, O.; Labadarios, D.; Rehle, T.; Simbayi, L.; Zuma, K.; Dhansay, A.; Reddy, P.; Parker, W.; Hoosain, E.; Naidoo, P.; et al. South African National Health and Nutrition Examination Survey (SANHANES-1), 2014 ed.; HSRC Press: Cape Town, South Africa, 2014. [Google Scholar]
- Johnson, I.T. Understanding the association between diet and nutrition in upper gastrointestinal cancer. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 1347–1349. [Google Scholar] [CrossRef] [Green Version]
- Lahmann, P.H.; Pandeya, N.; Webb, P.M.; Green, A.; Whiteman, D. Body mass index, long-term weight change, and esophageal squamous cell carcinoma. Cancer 2011, 118, 1901–1909. [Google Scholar] [CrossRef]
- Vellios, N.; Van Walbeek, C. Self-reported alcohol use and binge drinking in South Africa: Evidence from the National Income Dynamics Study, 2014–2015. South Afr. Med, J. 2017, 108, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, U., Jr.; Posner, M.C.; Safatle-Ribeiro, A.V.; Reynolds, J.C. Risk factors for squamous cell carcinoma of the oesophagus. Br. J. Surg. 1996, 83, 1174–1185. [Google Scholar] [CrossRef]
- Freedman, N.D.; Abnet, C.C.; Leitzmann, M.; Mouw, T.; Subar, A.F.; Hollenbeck, A.R.; Schatzkin, A. A Prospective Study of Tobacco, Alcohol, and the Risk of Esophageal and Gastric Cancer Subtypes. Am. J. Epidemiol. 2007, 165, 1424–1433. [Google Scholar] [CrossRef]
- Pandeya, N.; Olsen, C.; Whiteman, D. Sex differences in the proportion of esophageal squamous cell carcinoma cases attributable to tobacco smoking and alcohol consumption. Cancer Epidemiol. 2013, 37, 579–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Stefani, E.; Victora, C.G.; Castelletto, R.; Castellsagué, X.; Muñoz, N.; Rolón, P.A.; Quintana, M.J. Independent and joint effects of tobacco smoking and alcohol drinking on the risk of esophageal cancer in men and women. Int. J. Cancer 1999, 82, 657–664. [Google Scholar] [CrossRef]
- Anantharaman, D.; Marron, M.; Lagiou, P.; Samoli, E.; Ahrens, W.; Pohlabeln, H.; Slamova, A.; Schejbalova, M.; Merletti, F.; Richiardi, L.; et al. Population attributable risk of tobacco and alcohol for upper aerodigestive tract cancer. Oral Oncol. 2011, 47, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Gallus, S.; Bosetti, C.; Franceschi, S.; Levi, F.; Simonato, L.; Negri, E.; La Vecchia, C. Oesophageal cancer in women: Tobacco, alcohol, nutritional and hormonal factors. Br. J. Cancer 2001, 85, 341–345. [Google Scholar] [CrossRef]
- Mahboubi, E.; Kmet, J.; Cook, P.J.; Day, N.E.; Ghadirian, P.; Salmasizadeh, S. Oesophageal Cancer Studies in the Caspian Littoral of Iran: The Caspian Cancer Registry. Br. J. Cancer 1973, 28, 197–214. [Google Scholar] [CrossRef]
- Tran, G.D.; Sun, X.-D.; Abnet, C.C.; Fan, J.-H.; Dawsey, S.M.; Dong, Z.-W.; Mark, S.D.; Qiao, Y.; Taylor, P.R. Prospective study of risk factors for esophageal and gastric cancers in the Linxian general population trial cohort in China. Int. J. Cancer 2004, 113, 456–463. [Google Scholar] [CrossRef]
- Roshandel, G.; Semnani, S.; Malekzadeh, R.; Dawsey, S.M. Polycyclic aromatic hydrocarbons and esophageal squamous cell carcinoma. Arch. Iran. Med. 2012, 15, 713–722. [Google Scholar]
- Abedi-Ardekani, B.; Kamangar, F.; Hewitt, S.M.; Hainaut, P.; Sotoudeh, M.; Abnet, C.C.; Taylor, P.R.; Boffetta, P.; Malekzadeh, R.; Dawsey, S.M. Polycyclic aromatic hydrocarbon exposure in oesophageal tissue and risk of oesophageal squamous cell carcinoma in north-eastern Iran. Gut 2010, 59, 1178–1183. [Google Scholar] [CrossRef]
- Gustavsson, P.; Jakobsson, R.; Johansson, H.; Lewin, F.; Norell, S.; Rutkvist, L.E. Occupational exposures and squamous cell carcinoma of the oral cavity, pharynx, larynx, and oesophagus: A case-control study in Sweden. Occup. Environ. Med. 1998, 55, 393–400. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All | Male | Female | p Value | ||||
|---|---|---|---|---|---|---|---|
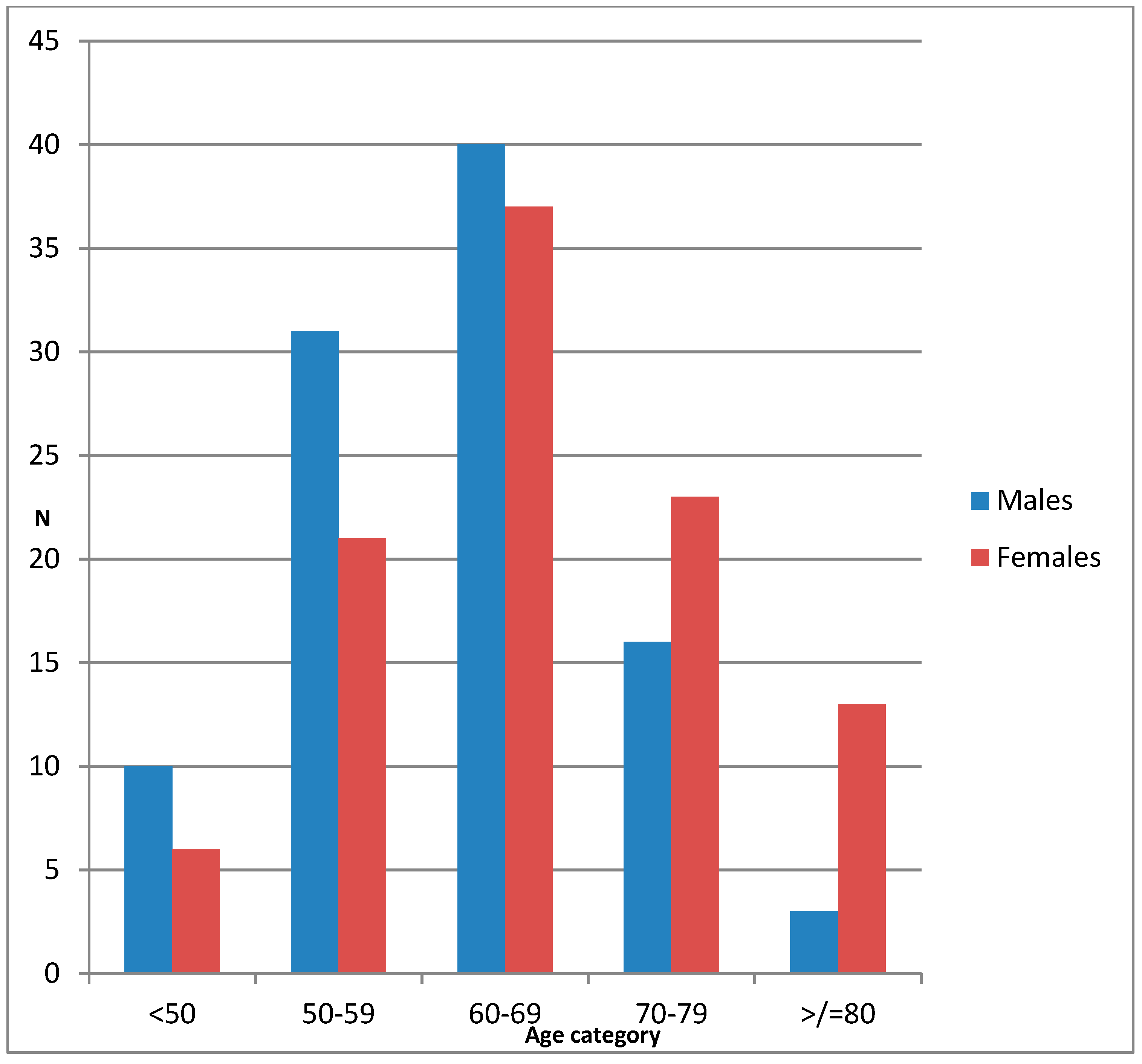
| Number of Subjects | 363 | 209 | 154 | ||||
| Mean | SD | Mean | SD | Mean | SD | ||
| Age (years) | 63 | 61.4 | ±9.6 | 66 | ±11.6 | <0.0001 | |
| Dysphagia grade | 2.2 | 2.2 | ±0.98 | 2.3 | ±0.86 | 0.71 | |
| Dysphagia duration (months) | 4.5 | 4.4 | ±2.6 | 4.6 | ±2.4 | 0.65 | |
| ECOG Score 1 | 1.75 | 1.7 | ±0.89 | 1.8 | ±0.83 | 0.32 | |
| BMI 2 | 19.9 | 18.4 | ±3.83 | 21.6 | ±5.84 | <0.001 | |
| No | % | No | % | No | % | ||
| Patients from urban area | 104 | 28.8 | 59 | 28.4 | 45 | 29.4 | 0.91 |
| Patients with weight loss | 286 | 78.5 | 164 | 78 | 122 | 79 | 0.86 |
| Patients with additional symptoms | 75 | 21 | 30 | 14 | 45 | 29 | 0.005 |
| All | Males | Female | p Value | |
|---|---|---|---|---|
| Smoking history (%) | 160 (48.3) | 148 (79) | 12 (8) | <0.0001 |
| Mean pack years (SD) | 15.99 | 16.59 (12.89) | 5.14 (3.23) | 0.021 |
| Alcohol history (%) | 156 (47.3) | 142 (76) | 14 (10) | <0.0001 |
| Traditional beer (%) | 129 (39.6) | 118 (63) | 11 (8) | <0.0001 |
| All | Males | Females | p Value | |
|---|---|---|---|---|
| Tumor location (%) | ||||
| Proximal | 64 (19) | 40 (20) | 24 (17) | 0.95 |
| Middle | 167 (49) | 84 (42) | 83 (59) | |
| Distal | 111 (32) | 77 (38) | 34 (24) | |
| Tumor histology | ||||
| Well-differentiated | 22 (8) | 9 (5) | 13 (11) | 0.8 |
| Moderately- differentiated | 233 (81) | 147 (85) | 86 (75) | |
| Poorly-differentiated | 32 (11) | 17 (10) | 15 (14) | |
| Mean tumor length (cm) | 6.6 | 6.8 | 6.4 | 0.31 |
| Patients receiving palliative management (%) | 351 (97) | 201 (97) | 150 (98) | 0.53 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferndale, L.; Aldous, C.; Hift, R.; Thomson, S. Gender Differences in Oesophageal Squamous Cell Carcinoma in a South African Tertiary Hospital. Int. J. Environ. Res. Public Health 2020, 17, 7086. https://doi.org/10.3390/ijerph17197086
Ferndale L, Aldous C, Hift R, Thomson S. Gender Differences in Oesophageal Squamous Cell Carcinoma in a South African Tertiary Hospital. International Journal of Environmental Research and Public Health. 2020; 17(19):7086. https://doi.org/10.3390/ijerph17197086
Chicago/Turabian StyleFerndale, Lucien, Colleen Aldous, Richard Hift, and Sandie Thomson. 2020. "Gender Differences in Oesophageal Squamous Cell Carcinoma in a South African Tertiary Hospital" International Journal of Environmental Research and Public Health 17, no. 19: 7086. https://doi.org/10.3390/ijerph17197086