Effectiveness of Virtual Reality Systems to Improve the Activities of Daily Life in Older People

 ,
, 
 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search
2.2. Review, Selection and Data Extraction
2.3. Summary Measures and Statistical Analysis
2.4. Assessment of Level of Evidence of the Set of Studies
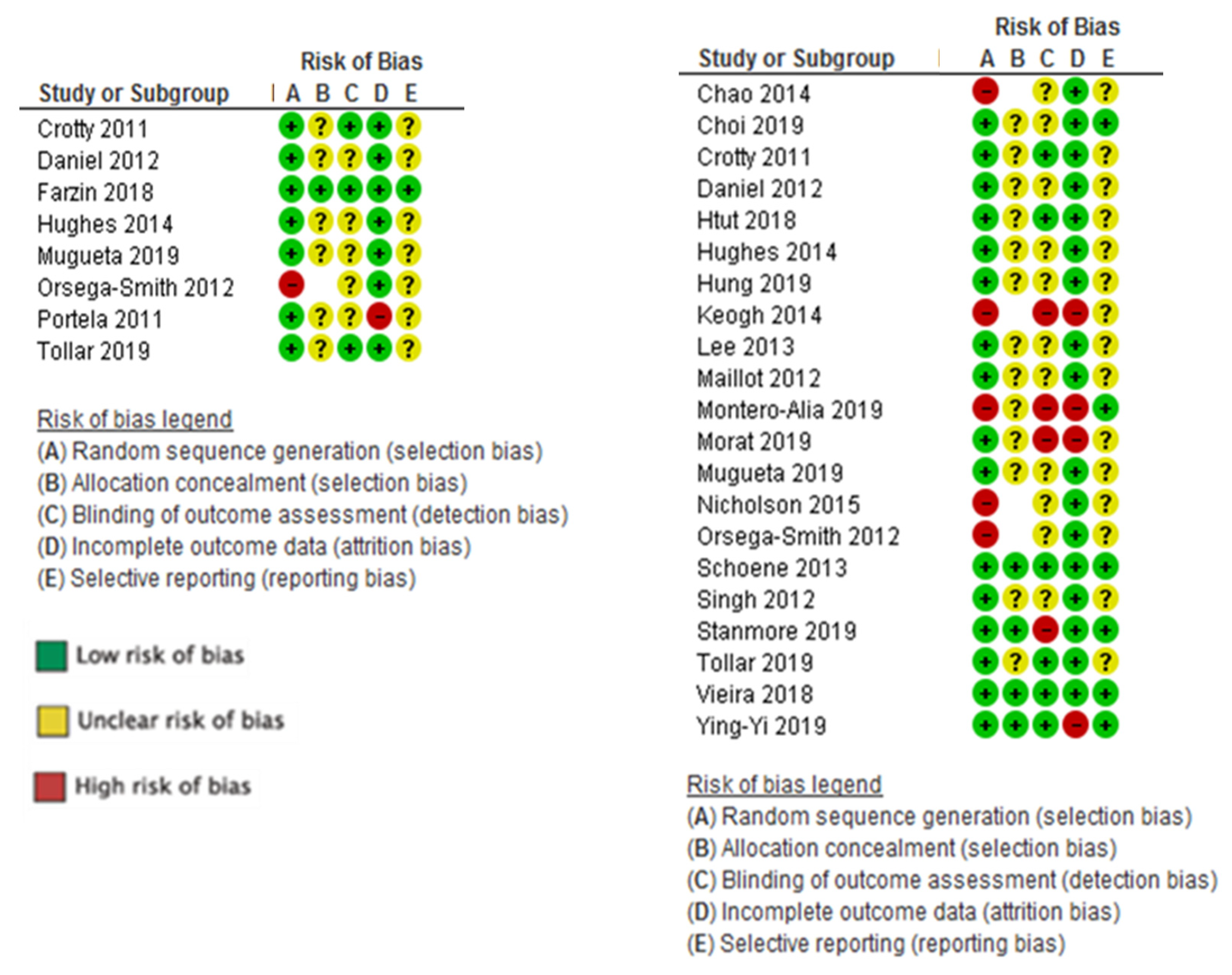
2.5. Risk of Bias Assessment in Individual Studies
- a low risk of bias were those in which all items were assigned a low risk of bias;
- an unclear risk of bias were studies in which one or more items were found to be at an unclear risk of bias; and
- a high risk of bias were studies in which one or more items were found to be at a high risk of bias.
2.6. Heterogeneity
2.7. Publication Bias
3. Results
3.1. Characteristics of Included Studies
3.2. Intervention with VRS
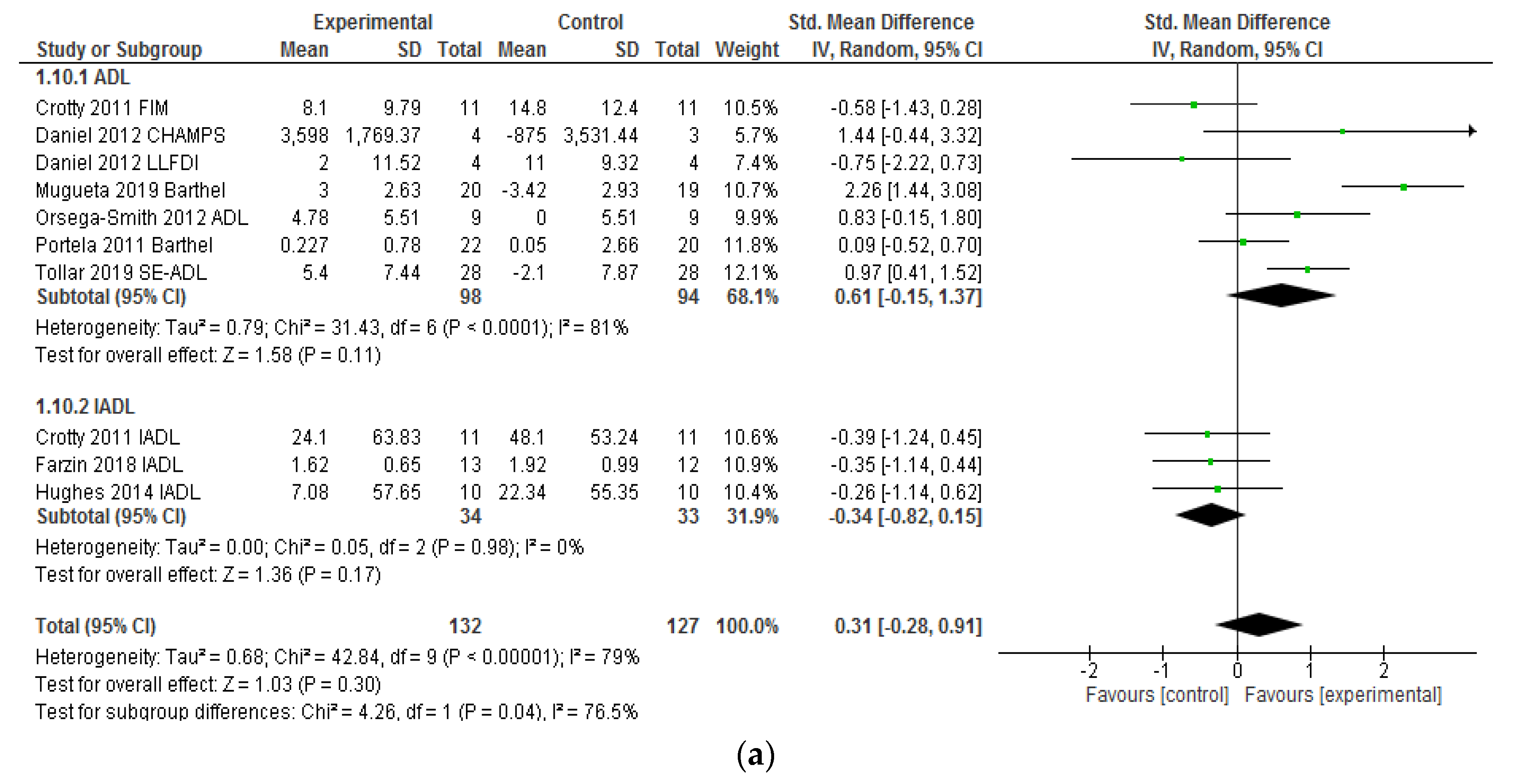
3.3. Effectiveness of VRSs on Activities of Daily Living
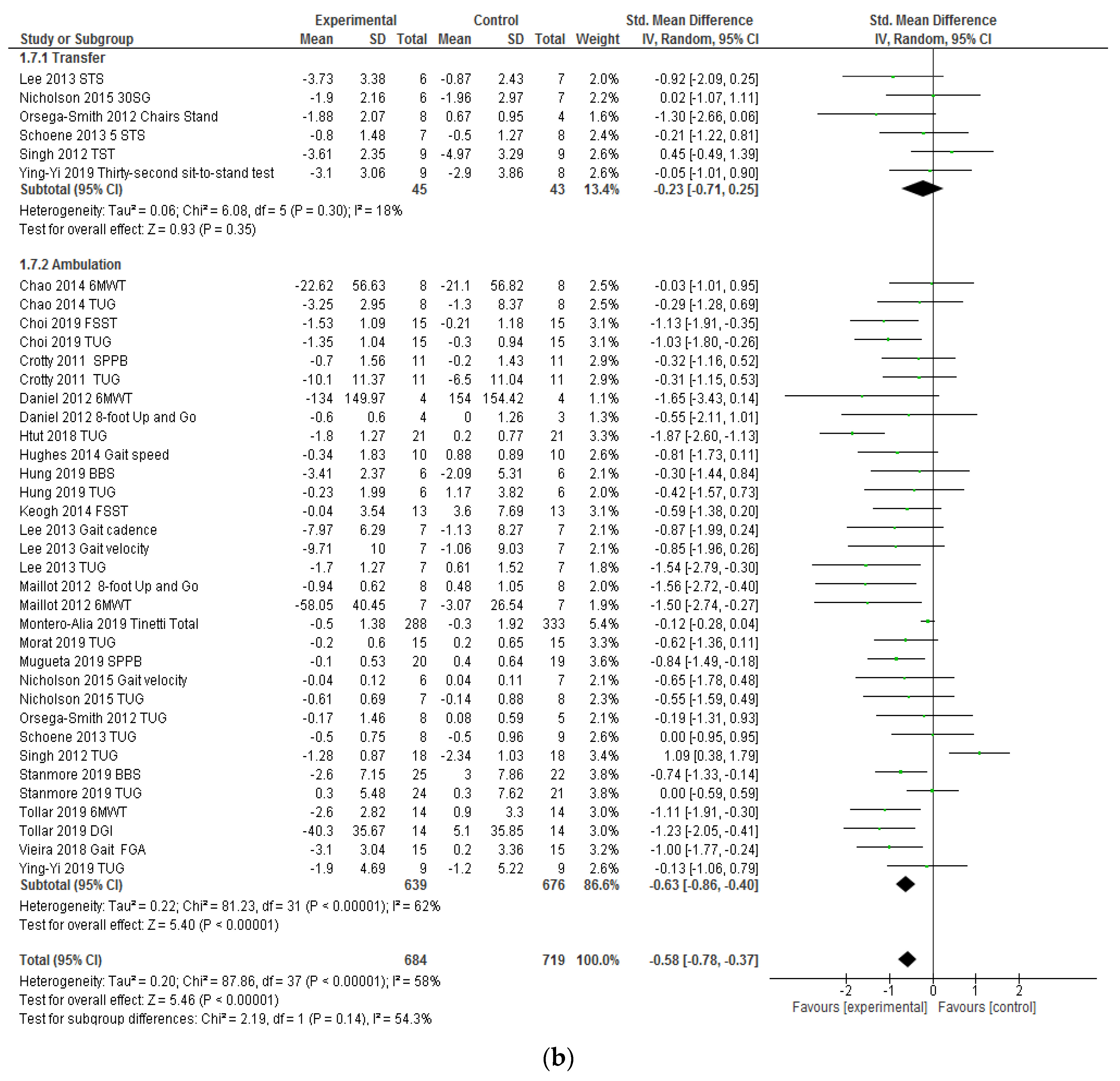
3.4. Effectiveness of VRSs on Functional Ambulation and Transfers
3.5. Risk of Bias of the Individual Studies
3.6. Heterogeneity
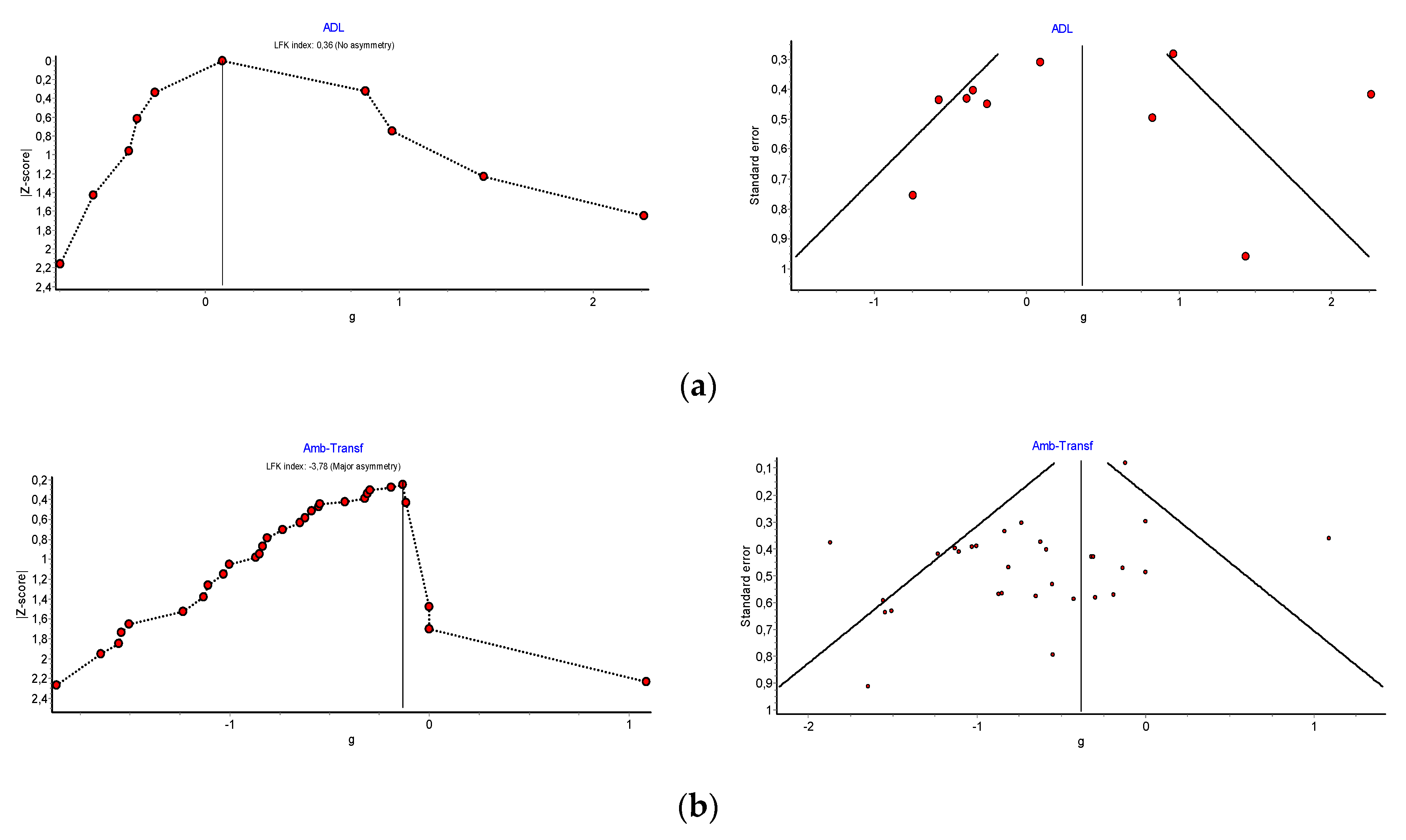
3.7. Publication Bias
3.8. GRADE Quality of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Key Search Terms |
|---|---|
| Population | Aging, elderly, geriatr *, gerontology, late life, older adults, oldest, seniors, old age. |
| Intervention: VRT | (“Wii *” OR “gaming technology” OR “active videogame” OR nintendo OR “video game*” OR exergam* OR Wii OR kinect OR Xbox OR “Play Station” OR “Xavi Sports”) OR (“virtual reality” OR virtual-reality tecnhology OR “Virtual navigation” OR “Virtual environment” OR “Simulated reality” OR “virtual rehabilitation” OR vr-based OR “virtually simulated” OR “use-computer interface”) |
| Outcome | Activities of daily living, daily living activities, daily self-care activities, adl, daily life activity *, functional Independence, physical functional performance, transfer, bathing, grooming, eating, feeding, functional mobility, walking, walking capacity, ambulation, gait, mobility, showering, toilet hygiene, toileting, personal hygiene, self-care, self-feeding, |
| Study and trial designs | clinical trial, controlled clinical trial, double blind, evidence-based, evidence synthesis, feasibility study, health technology assessment, intervention, longitudinal, multicenter study, pilot, random allocation, randomized controlled trials, standard of care, treatment outcome, validation study |
Appendix B
| Characteristics of Included Studies (N = 23) | |||||||||||
| Author | Evidence Level Design | Participants | Intervention | Follow-ups | Result | ||||||
| n | Age (yrs) Mean (SD) Range | Sex | Inclusion Criteria | Placement | Experimental Group | Control Group | Outcome Measures | Results | |||
| Chao 2014 [48] | Level II | n = 32 EC = 16 CC = 16 | 85 (79–91) | 67 % Female | >65 years; independent walking; able to read and speak English; able to follow instructions | Assisted living Buffalo (EEUU) | SAHA + Nintendo Wii Fit 4 weeks 2 times/week | Health educational session | BBS; TUG SMWT; GDS FES; SF8 | No follow-up | The experimental group improved gait speed, reduced depressive symptoms and increased confidence in activities of daily living. The control group did not show improvement in any result. |
| Choi 2019 [58] | Level I RCT | n = 57 EC = 28 CC = 29 | 69–85 | 84% Female | >65 years; < 26 MCA; able to communicate | Welfare center, Korea | VPK Exercise 6 weeks 2 times/week | Home exercise program: flexion, curl-ups, sideways leg lifts, prone leg lifts and supine leg lifts. | BBS; FSST; TUG; OLST; MCA; ACT | No follow-up | VPK improves physical and cognitive functions. VKP exercise induces significant increases in postural control and muscular strength. |
| Crotty 2011 [38] | Level I RCT | n = 44 EC = 22 CC = 22 | 84 (80–88) | 79% Female | >65 years; <150 kilos; independent walking; MEC: 21–30; good level of vision | Acute care hospital, Australia | Nintendo Wii 2 weeks 5 times/week | Strength, balance, aerobic exercises | TUG; BBS; SPPB; FIM; AIDL | 4 weeks after intervention | Wii is feasible for providing treatment to elderly patients. It can improve mobility and balance in comparison with traditional approaches. |
| Daniel 2012 [33] | Level I RCT | n = 23 EC = 16 CC = 7 | 76 (55–86) | 57% Female | >65 years; 1–2 of the characteristics of frailty | Senior centers and residential living centers Texas, US | Nintendo Wii Fit 15 weeks 3 times/week | Traditional senior fitness program | Senior fitness test; body weight; BES, CHAMPS; LLFDI SF-36. | No follow-up | Both groups improved scores in ABC and CHAMPS scales. The experimental group increased caloric expenditure. |
| Farzin 2018 [39] | Level I ECA | N = 25 | 55 (51–59) | 68% Female | >55 years; absence of a) history of neurological impairments, b) psychiatric disorders, c) learning disabilities, d) cerebrovascular disease | Older Adult University Program Kuala Lumpur, Malaysia | Virtual Week Board Game 6 weeks 1 time/week | Usual routine activities | GAS; IADL; PRMQ; PMT | 4 and 12 weeks after the intervention | VWB training improved performance and activities of daily living and reduce depression and anxiety levels. |
| Htut [51] | Level I RCT | n = 84 EC:VR = 21 EC:BE = 21 EC:PE = 21 CC = 21 | 75 (70–80) | 37% female | 65–85 years MEC > 23 BI = 100 | Residential aged-care Yangon, Myanmar | Xbox Kinect Cognitive Stimulation Balance exercise 8 weeks 3 times/week | Without intervention | TUG; 5 TST FES; MoCA BBS | No follow-up | VR group improved both physical and cognition performance, while BE was effective in enhancing cognition. VR and BE may help fall concern in older persons. |
| Hughes 2014 [40] | Level II | n = 20 EC = 10 CC = 10 | 77.4 (72–83) | 70% Female | MYHAT Cognitive Classification | Community-dwelling adults Pittsburgh, US | Nintendo Wii Sports 24 weeks 1 time/week | Without intervention | CAMCI; CRSQ AIVD GAIT: 6 m | No follow-up | The experimental group improved in overall cognition, perceived cognitive ability and gait speed. |
| Hung 2019 [42] | Level I RCT | n = 24 EC = 12 CC = 12 | 68 (66–72) | 57% female | >60 years; medical diagnoses of diabetes; independently ambulatory; MEC > 24 | Community-dwelling adults Taipei, China | Xavi Sport VR 6 weeks 3 times/week | Without intervention | TUG; BBS UST; MFES | 6 weeks after the intervention | VR showed positive effects on functional balance. BBS, UTS and TUG test scores significantly improved after intervention. |
| Keogh 2014 [49] | Level II Quasi-experimental | n = 34 EC = 19 CC = 15 | 83 (75–91) | 55% Female | >65 years; walk 10 min without aid; cognitive capacity to understand instructions | Residential aged-care Gold Coast, Australia | Nintendo Wii Sports 8 weeks | Usual routine activities | FSST RAPA WhOQOL-BREF semistructured group Interview | No follow-up | The intervention group showed a statistically significant improvement in strength in upper limbs, levels of physical and psychological activity and quality of life after participating in virtual reality programs with Wii. |
| Lee 2013 | Level I RCT | n = 64 EC = 32 CC = 32 | 74 (69–79) | 71% Female | >65 years; diagnosis of type 2 DM; able to communicate | Community-dwelling adults Seoul, Korea | Sony PlayStation and EyeToy 10 weeks 2 times/week | Health education on diabetes management | BBS TUG STS Gait Rite FES | No follow-up | VR can be used to prevent falls and improve the quality of walking. |
| Maillot 2012 [7] | Level I RCT | n = 32 EC = 16 CC = 16 | 71 (65–78) | 84% Female | Recommendation to Canadian Health Network. Never play video games and living a sedentary lifestyle | Community-dwelling adults Paris, France | Nintendo Wii Sports 14 weeks | Without intervention | MAQ; GDS MMSE, SFT, TNT, ST, MRT, SST | No follow-up | Improvement in the VRTI group in cognitive and physical tests. There were no differences in visuospatial function. |
| Montero 2019 [43] | Level II Quasi-random | n = 977 EC:508 EE:469 | 75 (72–78) | 59% female | <70 years; able to walk independently (with or without walking aids) | Community-dwelling adults Cataluña, Spain | Exergame Wii Fit with Wii Balance Board | Usual routine activities | Tinetti Test Short FES-I UST | 9 weeks after intervention | Found no effect of balance training usie on balance or falls. A reduced fear of falling was found at 3 months, but no longer at 1 year. The authors think this may be a chance finding. |
| Morat 2019 [46] | n = 45 VOL = 15 VOL + US = 15 Cc = 15 | 69 (64–74) | 62% female | <60 years; healthy | Community-dwelling adults Cologne, Germany | Dvidat, Senso Dvidat Senso+ Postoromed 8 weeks 3 times/week | Without intervention | TUG, Y-balance test, motor dual-task | No follow-up | Exergames under stable and unstable conditions are a feasible training tool with high adherence rates to improve functional balance and calf strength. Exergames, especially under unstable conditions, improve factors that are relevant for fall prevention, such as balance, functional mobility and strength. | |
| Mugueta 2019 [34] | Level I RCT | n = 40 EC = 20 CC = 20 | 84 (77–91) | 60% female | >65 years; >90 MBI; <10 SPPB; no physical exercise | Elderly day centers Bilbao, Spain | Exergame FRED, Kinect 6 weeks 3 times/week | Without intervention | BI; SPPB EuroQol | No follow-up | FRED Exergame reduced frailty risk: 14.7% less than control group No difference in EuroQol or BI. |
| Nicholson 2015 [50] | Level II Two groups, nonrandomized studies | n = 43 EC = 21 CC = 22 | 74 (69–79) | 76% Female | >65 years; not involved in balance exercises for the last 3 months; independent walking; adequate visual capacity; without progressive or terminal illness, acute illness or unstable chronic illness | Community-dwelling adults. Sunshine Coast, Australia | Nintendo Wii Fit 6 weeks 3 times/week without supervision | Without intervention | TUG; FES STS; PACES; FR | No follow-up | The experimental group improved in all variables but only left lateral reach showed statistical significance. |
| Orsega-Smith 2012 [35] | Level I RCT | n = 30 EC = 20 CC = 9 | 71 (66–83) | 92% Female | >63 years | Community-dwelling Older Adults | Nintendo Wii Fit: balance and yoga 4 weeks 8 weeks | Without intervention | ABC/FES; ADL BBS; TUG; CS | No follow-up | The experimental group improved transfers, balance and ADLs. The control group did not show any changes. |
| Portela [36] | Level I RCT | n = 65 EC = 23 CC = 42 | 79 (78–80) | 61% Female | >65 years; good level of vision and hearing; stand for 2 min without upper limb support | Community-dwelling Older Adults | Nintendo Wii 12 weeks 1 time/week | Traditional senior fitness program | BI; BBS; MMSE SF36 | No follow-up | The supervised use of Wii had an impact on physical improvement. The unsupervised use of Wii had a positive impact on vitality and mental health. |
| Schoene 2013 [47] | Level I RCT | n = 37 EC = 15 CC = 17 | 77.5 (73–82) | - | Walking independently 20 m; independent for ADLs | Independent-living units Sydney, Australia | Exergame DDR Stepmania 8 weeks 2 times/week | Usual routine activities | CSRT RT/CRST MT; 5STS; TUG TRIAL MAKING FES; PPA; AST | No follow-up | VR is safe and can be applied at home. It improves physical and cognitive parameters for fall prevention. |
| Singh 2013 [44] | Level I RCT | n = 38 EC = 16 CC = 16 | 62.5 (58–69) | 100% Female | >65 years; independent walking | Senior citizens’ club Kuala Lumpur, Malaysia | Wii Balance Board 6 weeks | Traditional senior fitness balance program | OPI; TST; TUG | No follow-up | VR improves agility, balance and functional mobility. There was no significant difference between groups. |
| Stanmore 2019 [45] | Level I RCT | n = 106 EC = 56 CC = 50 | 78 (58–96) | 78 % Female | >55 years; mental capacity; able to speak English; able to watch television from 2 m distance; able to use VR | Assisted living facilities Manchester and Glasgow, UK | Exergame FAME OTAGO 12 weeks | Physical exercise | BBS; FES TUG; GDS | No follow-up | VR exergame improved balance, pain and fear of falling and are a cost-effective fall prevention strategy in assisted living facilities. |
| Tollar 2019 [37] | Level I RCT | n = 83 EC-CYC = 27 EC-EXE = 28 CC = 28 | 69.6 (66–72) | 53% Female | >60 years; >24 MMSE; >40 BDI; mobility difficulty | Hospital Somogy, Hungary | Xbox or bicycle ergometer 5 weeks 5 times/week | Usual routine activities | 6MWT; SE-ADL; DGI; MAP; SF-36; WOMAC | No follow-up | Xbox and cycling improved general health-related QoL and walking capacity. Xbox improved the SE-ADL (7.3%) |
| Gomes 2019 [41] | Level I RCT | n = 30 EC = 15 CC = 15 | 84 (78–90) | 93% female | >60 years; able to walk independently; normal or corrected visual acuity; good hearing; no previous experience with VR | Sao Paulo Brazil Hospital | Nintendo Wii Fit 7 weeks 2 times/week | Advice regarding the importance of physical activity | FGA; MoCA; FES | 4 weeks after intervention | VR Wii-Fit was feasible, acceptable and safe for frail older adults and improved their postural control and gait. There were no effects on cognition, mood or fear of falling. |
| Liao 2019 [52] | Level I ECA | n = 52 EC = 27 Cc = 25 | 81 (73–89) | >65 and <95 years; the presence of at least one of the 5 frailty characteristics defined by Fried | Daycare centers Taiwan | Kinect: Tano, LongGood 12 weeks 3 times/week | Combined exercise: Resistance, aerobic and balance | IPAQ: IMC; TUG; grip strength; FES | No follow-up | Kinect-based exergaming is at least as beneficial as combined exercise in the prefrail and frail elderly. | |
| ABC: Activity-specific Balance Confidence; ACT: Arm Curl Test; ADL: Activities of Daily Living; AIDL: Activity Instrumental Daily Living; AST: Alternate Step Test; BBS: Balance Berg Scale; BE: Brain Exercise; BI: Barthel Index; BDI: Beck Depression Inventory; CAMCI: Computer Assessment of Mild Cognitive Impairment; CHAMPS: Community Healthy Activities Model Program for Seniors questionnaire CSRQ: Cognitive Self-Report Questionnaire; CRST-RT: Choice Stepping Reaction Time; CS: Chair Stand; FES: Falls Efficacy Scale; DGI: Dynamic Gait Index: FGA: Functional Gait Assessment; FIM: Functional Independence Measure; FPA: Foot Placement Accuracy; FR: Functional Reach; FSST: Four Square Step Test; GAS: Geriatric Anxiety Scale; GDS: Geriatric Depression Scale; IADL: Instrumental Activities of Daily Living scale; Level I: randomized controlled trials; Level II: two groups, nonrandomized studies (e.g., cohort, case–control); MAQ: Modifiable Activity Questionnaire; MBI: Modified Barthel Index; MCA: Montreal Cognitive Assessment; MEC: Mini-Examen Cognoscitivo; DM: Diabetes Mellitus; MAP: Mean Arterial Pressure; MCA: Montreal Cognitive Assessment; MFES: Modified Falls Efficacy Scale; MMSE = Mini Mental State Examination; MoCA: Montreal Cognitive Assessment; MRT: Matrix Reasoning Test; MT: Movement Time; OLST: One-Leg Stance Test; OPI: Overall Performance Index; PPA: Physiological Profile Assessment score; PACES: Physical Activity Enjoyment Scale; PE: Physical Exercise; PMT: Prospective Memory Tasks; PRMQ: Prospective Retrospective Memory Questionnaire; RAPA: Rapid Assessment Physical Activity scale; RCT: Randomized Clinical Trial; SFT: Senior Fitness Test; SF8: Short Form 8; SF36: Short Form 36; ST: Stroop Test; SE-ADL: Schwab–England Activities of Daily Living scale; SF-36: Short Form 36 Health Survey; SMWT: Six-Minute Walk Test; SPPB: Shot Physical Performance Battery; SST: Spatial Span Test TMT: Trail Making Test; TST: Ten Step Test; TUG: Timed Up and Go; UST: Unipedal Stance Test; VR: Virtual Reality; WHOQL-BREF: World Health Organization Quality of Life; WOMAC: McMaster Universities Osteoarthritis Index; VPK: Virtual Kayak Paddling; 5STS = Five Times Sit-to-Stand; 6MWT: 6-min Walk Test. | |||||||||||
Appendix C
| Author | Virtual Reality Type | Videogame Console and Technical Assistance | Exergame |
|---|---|---|---|
| Chao, 2014 [48] | Active Video Game | Nintendo Wii + Balance Board Walker was placed around the balance board | Wii Fit: Jogging; LungE; Penguin slide Table tilt; Chair; Deep breathing |
| Choi, 2019 [58] | Specific Virtual Reality | Virtual kayak paddling + a projected video | Kayaking |
| Crotty, 2011 [38] | Active Video Game | Nintendo Wii + Balance Board Chair around the balance board | Wii Fit |
| Daniel, 2012 [33] | Active Video Game | Nintendo Wii + weighty vest | Wii Sport, tennis, boxing, boling |
| Farzin, 2019 [39] | Specific Virtual Reality | Virtual Week (VW) Board Game | VW includes 8 to 10 PM tasks (four regular, four irregular and two stop clock tasks) which allow for exercising almost all types of everyday PM tasks (e.g., self-care, medication adherence, keeping social appointments) |
| Htut, 2018 [51] | Active Video Game | X-Box 360 + Kinect | Light Raise, Virtual Smash Stack ’em Up, One Ball Roll, Pin Push, Super Saber, Target Kick, Play Paddle Panic, Body Bally, Bamp Bash |
| Hughes, 2014 [40] | Active Video Game | Nintendo Wii | Wii Sports: bowling, golf, tennis, and baseball Wii Play: Wii Resort Boom Blox |
| Hung, 2019 [42] | Active Video Game | Xavi Sport + stepping mat | Set-up, stepping exercise, hamster game, drumming game |
| Keogh, 2014 [49] | Active Video Game | Nintendo Wii | Wii Sports: bowling, golf, tennis, baseball, boxing |
| Lee, 2013 [59] | Active Video Game | Play Station + EyeToy | Wishi Washi: window washing, Keep Ups, Bowling, Bubble Pop, Boot Camp, Kung Foo |
| Maillot, 2012 [7] | Active Video Game | Nintendo Wii | Wii Fit Wii Sport: tennis |
| Montero, 2019 [43] | Active Video Game | Nintendo Wii | Not specified |
| Morat, 2019 [46] | Specific Virtual Reality | Dividat Senso Swing and Posturomed | Targets, Divided, Simon, Flexi, Snake, Tetris, Habitats, Birds, Hexagon |
| Mugueta, 2019 [34] | Specific Virtual Reality | FRED + Kinect | FRED entails several scenarios, with each one representing one or more steps in a simplified process to enable txakoli to be produced |
| Nicholson, 2015 [50] | Active Video Game | Nintendo Wii + Balance Board | Soccer heading, penguin slide, ski slalom, ski jump, table tilt, snowball fight, perfect 10, and tightrope walking |
| Orsega Smith, 2012 [35] | Active Video Game | Nintendo Wii + Balance Board | Wii Fit: Balance Games: Penguin Slide,’ ‘Table Tilt,’ ‘Ski Slalom,’ ‘Balance Bubble’, Hula Hood, Snowboard Slalom; Wii Fit: Yoga: deep breathing, half-moon, palm tree |
| Portela [36] | Active Video Game | Nintendo Wii | Wii Sport |
| Schoene, 2013 [47] | Active Video Game: Stepmania | Television + step pad + computer unit | Open-source modified DDR game Stepmania: pressure sensitive panels which represent stepping direction and additional cognitive load (“bomb” for dodge) |
| Singh, 2013 [44] | Active Video Game | Nintendo Wii+ Balance Board | Ski Slalom, Table Tilt, Penguin Slide, Soccer Heading, Tight Rope Walk, Perfect 10, Tilt City |
| Stanmore, 2019 [45] | Specific Virtual Reality | MIRA Exergames + Kinect | Side Taps: Atlantis, Catch, Izzy the Bee, Move, Follow; Jugger, Firefly, Catch, Follow, Move; Sit to Stand: Powerhouse Bid, Atlantis, Izzy the Bee; Squats: Izzy the Bee, Atlantis, Catch, Move, Follow; Hip Frontal Flexion: Animals, Atlantis, Airplane, Catch, Follow, Colour Clouds, Move, Piano; Elbow Flexion: Grab, Catch, Follow, Atlantis, Izzy the Bee, Move, Firefly, Piano, Jugger; Full Body Turn: Animals, Catch, Firefly, Colour Clouds, Follow, Jugger, Basketball, Move; General–Shoulder: Atlantis, Catch, Firefly, Follow, Izzy the Bee, Jugger, Move; Hip Abduction: Atlantis, Catch, Izzy the Bee, Move, Follow, Fireflies, Jugger, Seasons; Knee Flexion: Grab, Catch, Follow, Atlantis, Izzy the Bee, Move, Firefly, Jugger; Shoulder Abduction: Atlantis, Follow, Catch, Izzy the Bee, Move, Firefly, Jugger, Follow, Memory scape |
| Tollar, 2019 [37] | Specific Virtual Reality | Exer Program designed to improve postural control, gait mobility, gait stability, turning and balance + Kinect | Space Pop trains spatial orientation through target reaching with arms, legs and whole body and Just Dance prompts users to generate and combine movement sequences |
| Gomes, 2018 [41] | Active Video Game | Nintendo + Balance Board | Wii Fit Plus: Table Tilt, Rhythm, Parade, Obstacle Course, Single Leg Extension, Tilt City, Basic Step, Penguin Heading Soccer, Basic Run, Torso Twist |
| Liao, 2019 [52] | Active Video Game | Tano and LongGood software packages + Kinect | Tai-chi exercise, resistance and aerobic exercises, balance game |
Appendix D
| Evidence Profile: SRV vs. Control on Functional Capacity: ADL | Evidence Profile: SRV vs. Control on Functional Mobility | ||||
|---|---|---|---|---|---|
| N° of studies: 8 (10 comparisons) Type of studies: RCT Intervention: Virtual Reality Systems on ADL Control: TPE, ADL, programs of health education or non-intervention N° of patients: 212 | N° of studies: 22 (38 comparisons) Type of studies: RCT Intervention: Virtual Reality Systems Control: physical exercise, programs of health education or non-intervention N° of patients: 1097 | ||||
| GRADE Factor | Importance | Explanations | GRADE Factor | Importance | Explanations |
| Limitations in study design or execution (risk of bias) | Moderate ↓1 level | Downgrading for risk of bias was not considered because most information is from studies at moderate risk of bias Moderate risk of bias Rate down one level | Limitations in study design or execution (risk of bias) | Moderate ↓1 level | Downgrading for risk of bias was not considered because most information is from studies at moderate risk of bias. Moderate risk of bias Rate down one level |
| Inconsistency results | Serious ↓1 level | Downgrading for inconsistency was considered because I2 = 79%. | Inconsistency results | No serious inconsistency | Downgrading for inconsistency was not considered because I2 = 58% |
| Indirectness evidence | No serious indirectness | In none of the studies were there substantial differences between the population, intervention or outcomes measured in the studies and those established in the systematic review. | Indirectness evidence | No serious indirectness | In none of the studies were there substantial differences between the population, intervention or outcomes measured in the studies and those established in the systematic review. |
| Imprecision | Moderated ↓1 level | The OIS was calculated, the resulting OIS being 276 participants with MDS = 0.3. The number of patients included in the meta-analysis is 212, moderately lower to the OIS. Downgrading for imprecision was considered. | Imprecision | No serious imprecision | The OIS was calculated, the resulting OIS being 276 participants with MDS = 0.3. The number of patients included in the meta-analysis is 1097, far superior to OIS. Downgrading for imprecision was not considered. |
| Publication bias | Not serious | Downgrading for publication bias was not considered because the DOI plot shows no asymmetry with LFK = 0.36. | Publication bias | Serious ↓1 level | Downgrading for publication bias was considered because the DOI plot shows marked asymmetry with LFK = 3.3 (major asymmetry). |
| Magnitude of effect | Moderated ↓1 level | SMD = │0.31 │ Upgrading for large magnitude of effect was not considered. | Magnitude of effect | Not serious | SMD =│0.58│ Upgrading for large magnitude of effect was not considered. |
| Dose-response gradient | Not considered. | Dose–response gradient | Not considered. | ||
| No plausible confounders | Not considered because studies in this meta-analysis are not observational. | No plausible confounders | Not considered because studies in this meta-analysis are not observational. | ||
| Quality rating | Very low quality: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different (GRADE Working Group grades of evidence) | Quality rating | Moderate–low quality: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different (GRADE Working Group grades of evidence) | ||
References
- Iwarsson, S.; Horstmann, V.; Sonn, U. Assessment of dependence in daily activities combined with a self-rating of difficulty. J. Rehabil. Med. 2009, 41, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y. Characterising Long Term Care Needs among Chinese Older Adults with Cognitive Impairment or ADL Limitations. J. Cross Cult. Gerontol. 2019, 35, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-J.C. Functional Ability in the Changing Demographic Landscape: Evidence and Opportunities for Occupational Therapy. Am. J. Occup. 2018, 72, 7204170010p1–7204170010p5. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J.; Neyens, J.C.L.; van Rossum, E.; Spreeuwenberg, M.D.; de Witte, L.P. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.T.S.; Vieira, L.P.; de Oliveira Barbosa, E.; Oliveira, L.M.; Maillot, P.; Vaghetti, C.A.O.; Giovani Carta, M.; Machado, S.; Gatica-Rojas, V.; Monteiro-Junior, R.S. Virtual Reality-Based Exercise with Exergames as Medicine in Different Contexts: A Short Review. Clin. Pract. Epidemiol. Ment. Health 2019, 15, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Skjæret, N.; Nawaz, A.; Morat, T.; Schoene, D.; Helbostad, J.L.; Vereijken, B. Exercise and rehabilitation delivered through exergames in older adults: An integrative review of technologies, safety and efficacy. Int. J. Med. Inform. 2016, 85, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Belchior, P.; Yam, A.; Thomas, K.R.; Bavelier, D.; Ball, K.K.; Mann, W.C.; Marsiske, M. Computer and Videogame Interventions for Older Adults’ Cognitive and Everyday Functioning. Games Health J. 2019, 8, 129–143. [Google Scholar] [CrossRef]
- Faria, A.L.; Andrade, A.; Soares, L.I.; Badia, S.B. Benefits of virtual reality based cognitive rehabilitation through simulated activities of daily living: A randomized controlled trial with stroke patients. J. Neuroeng. Rehabil. 2016, 13, 96. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Erdt, M.; Chen, L.; Cao, Y.; Lee, S.-Q.; Theng, Y.-L. The Social Effects of Exergames on Older Adults: Systematic Review and Metric Analysis. J. Med. Int. Res. 2018, 20, e10486. [Google Scholar] [CrossRef]
- Levin, M.F. Can virtual reality offer enriched environments for rehabilitation? Expert Rev. Neurother. 2011, 11, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Contreras, K.; Cubillos, R.; Hernández, Ó.; Reveco, C.; Santis, N. Rehabilitación virtual en la intervención de terapia ocupacional. Rev. Chil. Ter. Ocup. 2014, 14, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.D.; Guo, L.; Kang, D.; Xiong, S. Exergame technology and interactive interventions for elderly fall prevention: A systematic literature review. Appl. Ergon. 2017, 65, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Neri, S.G.; Cardoso, J.R.; Cruz, L.; Lima, R.M.; de Oliveira, R.J.; Iversen, M.D.; Carregaro, R.L. Do virtual reality games improve mobility skills and balance measurements in community-dwelling older adults? Systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 1292–1304. [Google Scholar] [CrossRef]
- Bonnechère, B.; Jansen, B.; Omelina, L.; Van Sint Jan, S. The use of commercial video games in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef] [PubMed]
- D’Cunha, N.M.; Nguyen, D.; Naumovski, N.; McKune, A.J.; Kellett, J.; Georgousopoulou, E.N.; Frost, J.; Isbel, S. A Mini-Review of Virtual Reality-Based Interventions to Promote Well-Being for People Living with Dementia and Mild Cognitive Impairment. Gerontology 2019, 65, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- American Occupational Therapy Association. Occupational Therapy practice framework: Domain and Process (3rd Edition). Am. J. Occup. Ther. 2017, 68, S1. [Google Scholar] [CrossRef]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.A.; Haynes, R.B.; Richardson, W.S. Evidence based medicine: What it is and what it isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef] [Green Version]
- Cobos-Carbó, A.; Augustovski, F. Declaración CONSORT 2010: Actualización de la lista de comprobación para informar ensayos clínicos aleatorizados de grupos paralelos. Med. Clín. 2011, 137, 213–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cid-Ruzafa, J.; Damián-Moreno, J. Valoración de la discapacidad física: El indice de Barthel. Rev. Esp. Salud Pública 1997, 71, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martín, P.; Fernández-Mayoralas, G.; Frades-Payo, B.; Rojo-Pérez, F.; Petidier, R.; Rodríguez-Rodríguez, V.; Forjaz, M.J.; Prieto-Flores, M.E.; Pedro Cuesta, J. de Validación de la Escala de Independencia Funcional. Gac. Sanit. 2009, 23, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayers, S.P.; Jette, A.M.; Haley, S.M.; Heeren, T.C.; Guralnik, J.M.; Fielding, R.A. Validation of the Late-Life Function and Disability Instrument. J. Am. Geriatr. Soc. 2004, 52, 1554–1559. [Google Scholar] [CrossRef] [PubMed]
- Graf, C. The Lawton Instrumental Activities of Daily Living (IADL) Scale. 2. Med. Surg. Nurses 2008, 108, 59. [Google Scholar]
- Wrisley, D.M.; Marchetti, G.F.; Kuharsky, D.K.; Whitney, S.L. Reliability, internal consistency, and validity of data obtained with the functional gait assessment. Phys. Ther. 2004, 84, 906–918. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Dite, W.; Temple, V.A. A clinical test of stepping and change of direction to identify multiple falling older adults. Arch. Phys. Med. Rehabil. 2002, 83, 1566–1571. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Bohannon, R.W. Daily sit-to-stands performed by adults: A systematic review. J. Phys. Sci. 2015, 27, 939–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Daniel, K. Wii-hab for pre-frail older adults. Rehabil. Nurs. 2012, 37, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Mugueta-Aguinaga, I.; Garcia-Zapirain, B. FRED: Exergame to Prevent Dependence and Functional Deterioration Associated with Ageing. A Pilot Three-Week Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2017, 14, 1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orsega-Smith, E.; Davis, J.; Slavish, K.; Gimbutas, L. Wii Fit Balance Intervention in Community-Dwelling Older Adults. Games Health J. 2012, 1, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Portela, F.R.; Correia, R.J.C.; Fonseca, J.A.; Andrade, J.M. Wiitherapy on seniors—Effects on physical and metal domains. In Proceedings of the 2011 IEEE 1st International Conference on Serious Games and Applications for Health (SeGAH), Braga, Portugal, 16–18 November 2011; pp. 1–5. [Google Scholar]
- Tollár, J.; Nagy, F.; Moizs, M.; Tóth, B.E.; Sanders, L.M.J.; Hortobágyi, T. Diverse Exercises Similarly Reduce Older Adults’ Mobility Limitations. Med. Sci. Sports Exerc. 2019, 51, 1809–1816. [Google Scholar] [CrossRef]
- Crotty, M.; Laver, K.; Quinn, S.; Ratcliffe, J.; George, S.; Whitehead, C.; Davies, O. Is use of the Nintendo Wii Fit in physiotherapy as effective as conventional physiotherapy training for hospitalised older adults? In Proceedings of the 2011 International Conference on Virtual Rehabilitation, Zurich, Switzerland, 27–29 June 2011; pp. 1–2. [Google Scholar]
- Farzin, A.; Ibrahim, R.; Madon, Z.; Basri, H. The Efficiency of a Multicomponent Training for Prospective Memory Among Healthy Older Adults: A Single-Blind, Randomized Controlled Within-Participants Cross-Over Trial. Am. J. Phys. Med. Rehabil. 2018, 97, 628–635. [Google Scholar] [CrossRef]
- Hughes, K.J.; Salmon, N.; Galvin, R.; Casey, B.; Clifford, A.M. Interventions to improve adherence to exercise therapy for falls prevention in community-dwelling older adults: Systematic review and meta-analysis. Age Ageing 2019, 48, 185–195. [Google Scholar] [CrossRef]
- Gomes, G.C.V.; Bacha, J.M.R.; do Socorro Simões, M.; Lin, S.M.; Viveiro, L.A.P.; Varise, E.M.; Filho, W.J.; Pompeu, J.E. Feasibility, safety, acceptability, and functional outcomes of playing Nintendo Wii Fit PlusTM for frail elderly: Study protocol for a feasibility trial. Pilot Feasibility Stud. 2017, 3, 41. [Google Scholar] [CrossRef] [Green Version]
- Hung, E.S.-W.; Chen, S.-C.; Chang, F.-C.; Shiao, Y.; Peng, C.-W.; Lai, C.-H. Effects of Interactive Video Game-Based Exercise on Balance in Diabetic Patients with Peripheral Neuropathy: An Open-Level, Crossover Pilot Study. Evid. Based Complement. Altern. Med. 2019, 2019, 4540709. [Google Scholar] [CrossRef] [Green Version]
- Montero-Alía, P.; Miralles-Basseda, R.; López-Jiménez, T.; Muñoz-Ortiz, L.; Jiménez-González, M.; Prat-Rovira, J.; Albarrán-Sánchez, J.L.; Manresa-Domínguez, J.M.; Andreu-Concha, C.M.; Rodríguez-Pérez, M.C.; et al. Controlled trial of balance training using a video game console in community-dwelling older adults. Age Ageing 2019, 48, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.K.A.; Rajaratnam, B.S.; Palaniswamy, V.; Raman, V.P.; Bong, P.S.; Pearson, H. Effects of balance-focused interactive games compared to therapeutic balance classes for older women. Climacteric 2012, 16, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Stanmore, E.K.; Mavroeidi, A.; de Jong, L.D.; Skelton, D.A.; Sutton, C.J.; Benedetto, V.; Munford, L.A.; Meekes, W.; Bell, V.; Todd, C. The effectiveness and cost-effectiveness of strength and balance Exergames to reduce falls risk for people aged 55 years and older in UK assisted living facilities: A multi-centre, cluster randomised controlled trial. BMC Med. 2019, 17, 49. [Google Scholar] [CrossRef] [PubMed]
- Morat, M.; Bakker, J.; Hammes, V.; Morat, T.; Giannouli, E.; Zijlstra, W.; Donath, L. Effects of stepping exergames under stable versus unstable conditions on balance and strength in healthy community-dwelling older adults: A three-armed randomized controlled trial. Exp. Gerontol. 2019, 127, 110719. [Google Scholar] [CrossRef] [PubMed]
- Schoene, D.; Lord, S.R.; Delbaere, K.; Severino, C.; Davies, T.A.; Smith, S.T. A Randomized Controlled Pilot Study of Home-Based Step Training in Older People Using Videogame Technology. PLoS ONE 2013, 8, e57734. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.-Y.; Scherer, Y.K.; Montgomery, C.A.; Wu, Y.-W.; Lucke, K.T. Physical and psychosocial effects of Wii Fit exergames use in assisted living residents: A pilot study. Clin. Nurs. Res. 2015, 24, 589–603. [Google Scholar] [CrossRef]
- Keogh, J.W.L.; Power, N.; Wooller, L.; Lucas, P.; Whatman, C. Physical and psychosocial function in residential aged-care elders: Effect of Nintendo Wii Sports games. J. Aging Phys. Act. 2014, 22, 235–244. [Google Scholar] [CrossRef]
- Nicholson, V.P.; McKean, M.; Lowe, J.; Fawcett, C.; Burkett, B. Six weeks of unsupervised Nintendo Wii Fit gaming is effective at improving balance in independent older adults. J. Aging Phys. Act. 2015, 23, 153–158. [Google Scholar] [CrossRef]
- Htut, T.Z.C.; Hiengkaew, V.; Jalayondeja, C.; Vongsirinavarat, M. Effects of physical, virtual reality-based, and brain exercise on physical, cognition, and preference in older persons: A randomized controlled trial. Eur. Rev. Aging Phys. Act. 2018, 15, 1–12. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Chen, I.-H.; Lin, Y.-J.; Chen, Y.; Hsu, W.-C. Effects of Virtual Reality-Based Physical and Cognitive Training on Executive Function and Dual-Task Gait Performance in Older Adults With Mild Cognitive Impairment: A Randomized Control Trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef] [Green Version]
- Pacheco, T.B.F.; de Medeiros, C.S.P.; de Oliveira, V.H.B.; Vieira, E.R.; de Cavalcanti, F.A.C. Effectiveness of exergames for improving mobility and balance in older adults: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 163. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Maranesi, E.; Riccardi, G.R.; Donna, V.D.; Pelliccioni, P.; Luzi, R.; Lattanzio, F.; Pelliccioni, G. Non-Immersive Virtual Reality for Rehabilitation of the Older People: A Systematic Review into Efficacy and Effectiveness. J. Clin. Med. 2019, 8, 1882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomioka, K.; Kurumatani, N.; Saeki, K. The differential effects of type and frequency of social participation on IADL declines of older people. PLoS ONE 2018, 13, e0207426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, E.G.; Kearney, P.J. Occupational Therapy Interventions to Improve Performance of Instrumental Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review. Am. J. Occup. 2018, 72, 7204190050p1–7204190050p9. [Google Scholar] [CrossRef] [PubMed]
- Orellano, E.; Colón, W.I.; Arbesman, M. Effect of occupation- and activity-based interventions on instrumental activities of daily living performance among community-dwelling older adults: A systematic review. Am. J. Occup. 2012, 66, 292–300. [Google Scholar] [CrossRef] [Green Version]
- The Effects of Virtual Kayak Paddling Exercise on Postural Balance, Muscle Performance, and Cognitive Function in Older Adults with Mild Cognitive-PubMed-NCBI. Available online: https://www.ncbi.nlm.nih.gov/pubmed/?term=The+Effects+of+Virtual+Kayak+Paddling+Exercise+on+Postural+Balance%2C+Muscle+Performance%2C+and+Cognitive+Function+in+Older+Adults+with+Mild+Cognitive+Impairment%3A+A+Randomized+Controlled+Trial (accessed on 27 December 2019).
- Lee, S.; Shin, S. Effectiveness of virtual reality using video gaming technology in elderly adults with diabetes mellitus. Diabetes Technol. Ther. 2013, 15, 489–496. [Google Scholar] [CrossRef]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corregidor-Sánchez, A.-I.; Segura-Fragoso, A.; Criado-Álvarez, J.-J.; Rodríguez-Hernández, M.; Mohedano-Moriano, A.; Polonio-López, B. Effectiveness of Virtual Reality Systems to Improve the Activities of Daily Life in Older People. Int. J. Environ. Res. Public Health 2020, 17, 6283. https://doi.org/10.3390/ijerph17176283
Corregidor-Sánchez A-I, Segura-Fragoso A, Criado-Álvarez J-J, Rodríguez-Hernández M, Mohedano-Moriano A, Polonio-López B. Effectiveness of Virtual Reality Systems to Improve the Activities of Daily Life in Older People. International Journal of Environmental Research and Public Health. 2020; 17(17):6283. https://doi.org/10.3390/ijerph17176283
Chicago/Turabian StyleCorregidor-Sánchez, Ana-Isabel, Antonio Segura-Fragoso, Juan-José Criado-Álvarez, Marta Rodríguez-Hernández, Alicia Mohedano-Moriano, and Begoña Polonio-López. 2020. "Effectiveness of Virtual Reality Systems to Improve the Activities of Daily Life in Older People" International Journal of Environmental Research and Public Health 17, no. 17: 6283. https://doi.org/10.3390/ijerph17176283