Interrelationship among Obstructive Sleep Apnea, Renal Function and Survival: A Cohort Study

 ,
,
Abstract
:1. Introduction
2. Methods and Patients
2.1. Study Design and Setting
2.2. Patients and Samples
2.3. Sample Size
2.4. Statistical Analysis
3. Results
3.1. Polysomnographic Data
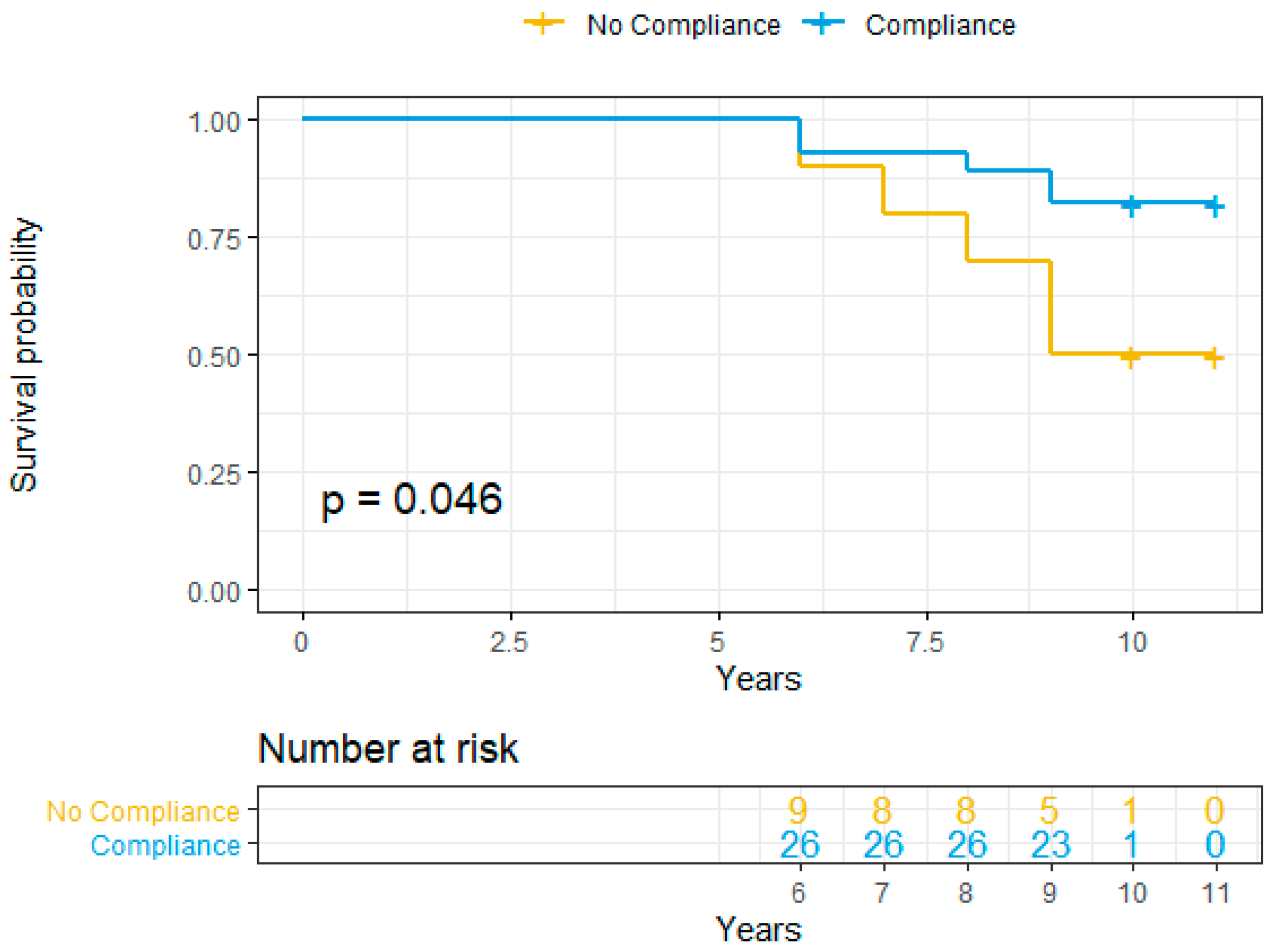
3.2. Compliance to Positive Air Pressure Treatment
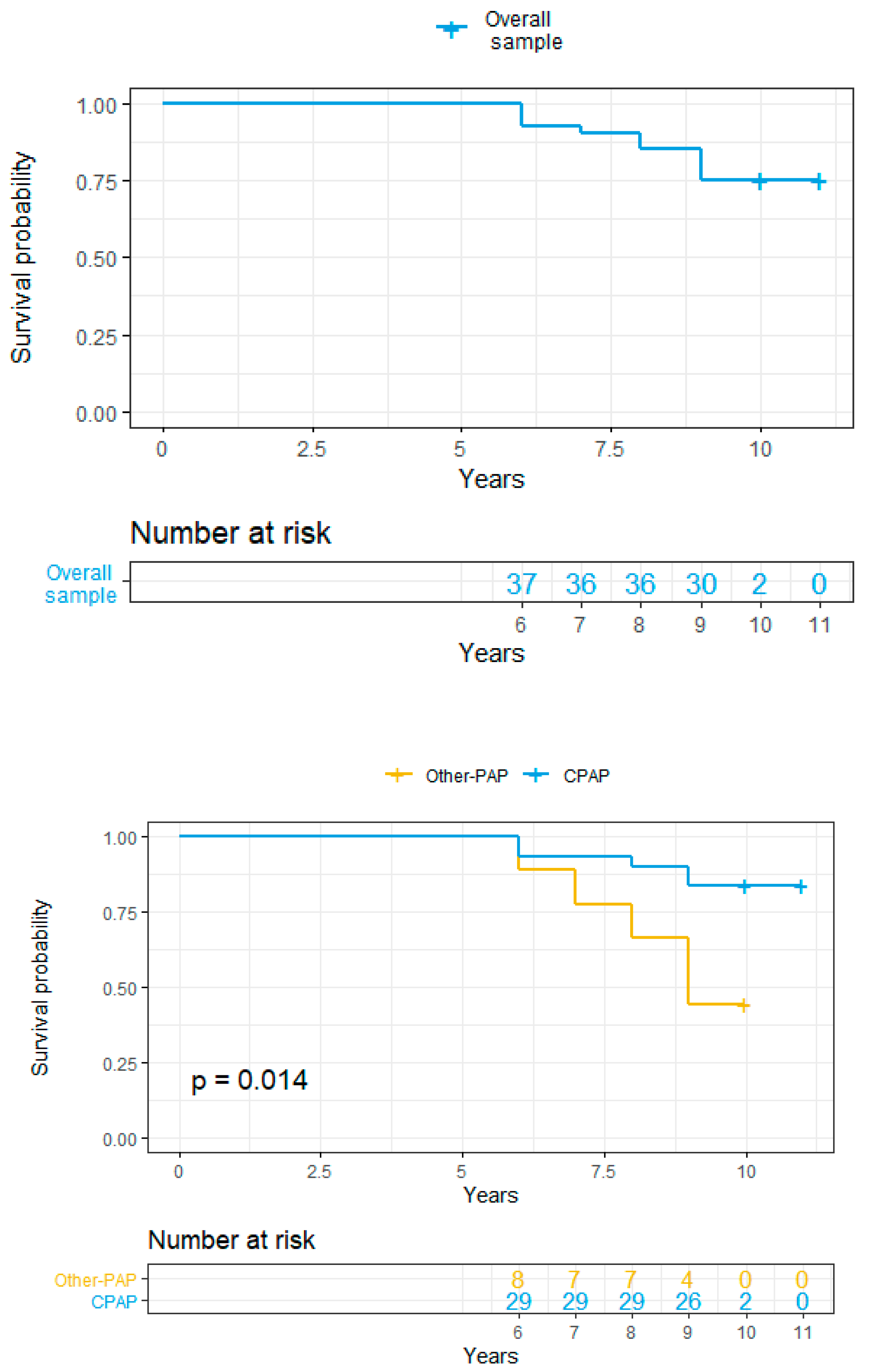
3.3. 10 Years Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Eckardt, K.-U.; Coresh, J.; Devuyst, O.; Johnson, R.J.; Köttgen, A.; Levey, A.S.; Levin, A. Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 2013, 382, 158–169. [Google Scholar] [CrossRef] [Green Version]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.N.; Gilbertson, D.T.; Murray, T.; Collins, A.J. Long Interdialytic Interval and Mortality among Patients Receiving Hemodialysis. N. Engl. J. Med. 2011, 365, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Zoccali, C.; Ikizler, T.A. Obesity in CKD—What Should Nephrologists Know? J. Am. Soc. Nephrol. 2013, 24, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Nicholl, D.D.M.; Ahmed, S.B.; Loewen, A.H.S.; Hemmelgarn, B.R.; Sola, D.Y.; Beecroft, J.M.; Turin, T.C.; Hanly, P.J. Declining Kidney Function Increases the Prevalence of Sleep Apnea and Nocturnal Hypoxia. Chest 2012, 141, 1422–1430. [Google Scholar] [CrossRef] [Green Version]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of obstructive sleep apnea: A population health perspective. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef]
- Eckert, D.J.; Malhotra, A.; Jordan, A.S. Mechanisms of Apnea. Prog. Cardiovasc. Dis. 2009, 51, 313–323. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Hung, S.-Y.; Wang, H.-K.; Lin, C.-W.; Wang, H.-H.; Chen, S.-W.; Chang, M.-Y.; Ho, L.-C.; Chen, Y.-T.; Liou, H.-H.; et al. Sleep Apnea and the Risk of Chronic Kidney Disease: A Nationwide Population-Based Cohort Study. Sleep 2015, 38, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Voulgaris, A.; Marrone, O.; Bonsignore, M.R.; Steiropoulos, P. Chronic kidney disease in patients with obstructive sleep apnea. A narrative review. Sleep Med. Rev. 2019, 47, 74–89. [Google Scholar] [CrossRef]
- Lin, C.-H.; Lurie, R.C.; Lyons, O.D. Sleep Apnea and Chronic Kidney Disease. Chest 2020, 157, 673–685. [Google Scholar] [CrossRef]
- Lin, C.-H.; Perger, E.; Lyons, O.D. Obstructive sleep apnea and chronic kidney disease. Curr. Opin. Pulm. Med. 2018, 24, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottlieb, D.J.; Yenokyan, G.; Newman, A.B.; O’Connor, G.T.; Punjabi, N.M.; Quan, S.F.; Redline, S.; Resnick, H.E.; Tong, E.K.; Diener-West, M.; et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: The sleep heart health study. Circulation 2010, 122, 352–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldi, I.; Azzolina, D.; Berchialla, P.; Gregori, D.; Scotti, L.; Corrao, G. Comorbidity-adjusted relative survival in newly hospitalized heart failure patients: A population-based study. Int. J. Cardiol. 2017, 243, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Loffler, K.A.; Heeley, E.; Freed, R.; Anderson, C.S.; Brockway, B.; Corbett, A.; Chang, C.L.; Douglas, J.A.; Ferrier, K.; Graham, N.; et al. Effect of Obstructive Sleep Apnea Treatment on Renal Function in Patients with Cardiovascular Disease. Am. J. Respir. Crit. Care Med. 2017, 196, 1456–1462. [Google Scholar] [CrossRef]
- Lorenzoni, G.; Azzolina, D.; Lanera, C.; Brianti, G.; Gregori, D.; Vanuzzo, D.; Baldi, I. Time trends in first hospitalization for heart failure in a community-based population. Int. J. Cardiol. 2018, 271, 195–199. [Google Scholar] [CrossRef]
- Shahar, E.; Whitney, C.W.; Redline, S.; Lee, E.T.; Newman, A.B.; Javier Nieto, F.; O’Connor, G.T.; Boland, L.L.; Schwartz, J.E.; Samet, J.M. Sleep-disordered Breathing and Cardiovascular Disease: Cross-sectional Results of the Sleep Heart Health Study. Am. J. Respir. Crit. Care Med. 2001, 163, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Baldi, I.; Gulati, A.; Lorenzoni, G.; Natarajan, K.; Ballali, S.; Kameswaran, M.; Rajeswaran, R.; Gregori, D.; Sethi, G. Public Health Implications of Obstructive Sleep Apnea Burden. Indian J. Pediatr. 2014, 81, 55–62. [Google Scholar] [CrossRef]
- Wingfield Digby, J.; Mathioudakis, A.; Heartshorne, R.; Mohammad, M.; Tewkesbury, D.; Needham, M. CPAP appears to protect kidney function of patients with OSA. In Proceedings of the Sleep and Control of Breathing, European Respiratory Society, Lausanne, Switzerland, 1 September 2017; p. OA3210. [Google Scholar]
- Koga, S.; Ikeda, S.; Yasunaga, T.; Nakata, T.; Maemura, K. Effects of nasal continuous positive airway pressure on the glomerular filtration rate in patients with obstructive sleep apnea syndrome. Intern. Med. 2013, 52, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Marrone, O.; Battaglia, S.; Steiropoulos, P.; Basoglu, O.K.; Kvamme, J.A.; Ryan, S.; Pepin, J.-L.; Verbraecken, J.; Grote, L.; Hedner, J.; et al. Chronic kidney disease in European patients with obstructive sleep apnea: The ESADA cohort study. J. Sleep Res. 2016, 25, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Takata, Y.; Usui, Y.; Shiina, K.; Asano, K.; Hashimura, Y.; Saruhara, H.; Nishihata, Y.; Tomiyama, H.; Yamashina, A. Severe obstructive sleep apnea increases cystatin C in clinically latent renal dysfunction. Respir. Med. 2011, 105, 643–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.B.; Ronksley, P.E.; Hemmelgarn, B.R.; Tsai, W.H.; Manns, B.J.; Tonelli, M.; Klarenbach, S.W.; Chin, R.; Clement, F.M.; Hanly, P.J. Nocturnal Hypoxia and Loss of Kidney Function. PLoS ONE 2011, 6, e19029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakaguchi, Y.; Hatta, T.; Hayashi, T.; Shoji, T.; Suzuki, A.; Tomida, K.; Okada, N.; Rakugi, H.; Isaka, Y.; Tsubakihara, Y. Association of nocturnal hypoxemia with progression of CKD. Clin. J. Am. Soc. Nephrol. 2013, 8, 1502–1507. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, G.; Fillafer, G.; Matterer, H.; Skrabal, F.; Kotanko, P. Prevalence of chronic kidney disease in patients with suspected sleep apnoea. Nephrol. Dial. Transplant. 2010, 25, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Canales, M.T.; Lui, L.-Y.; Taylor, B.C.; Ishani, A.; Mehra, R.; Stone, K.L.; Redline, S.; Ensrud, K.E.; for the Osteoporotic Fractures in Men (MrOS) Study Group. Renal function and sleep-disordered breathing in older men. Nephrol. Dial. Transplant. 2008, 23, 3908–3914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, E.C. Obstructive sleep apnea and the kidney. J. Am. Soc. Nephrol. 1993, 4, 1111–1121. [Google Scholar]
- Iseki, K.; Tohyama, K.; Matsumoto, T.; Nakamura, H. High Prevalence of Chronic Kidney Disease among Patients with Sleep Related Breathing Disorder (SRBD). Hypertens. Res. 2008, 31, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Hanly, P.J.; Ahmed, S.B. Sleep Apnea and the Kidney. Chest 2014, 146, 1114–1122. [Google Scholar] [CrossRef]
- Kinebuchi, S.; Kazama, J.J.; Satoh, M.; Sakai, K.; Nakayama, H.; Yoshizawa, H.; Narita, I.; Suzuki, E.; Gejyo, F. Short-term use of continuous positive airway pressure ameliorates glomerular hyperfiltration in patients with obstructive sleep apnoea syndrome. Clin. Sci. 2004, 107, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Faulx, M.D.; Storfer-Isser, A.; Kirchner, H.L.; Jenny, N.S.; Tracy, R.P.; Redline, S. Obstructive sleep apnea is associated with increased urinary albumin excretion. Sleep 2007, 30, 923–929. [Google Scholar] [CrossRef] [Green Version]
- Drager, L.F.; McEvoy, R.D.; Barbe, F.; Lorenzi-Filho, G.; Redline, S. INCOSACT Initiative (International Collaboration of Sleep Apnea Cardiovascular Trialists) Sleep Apnea and Cardiovascular Disease: Lessons from Recent Trials and Need for Team Science. Circulation 2017, 136, 1840–1850. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, revised ed.; Routledge: New York, NY, USA, 1977. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Bull, S.B. Regression models for multiple outcomes in large epidemiologic studies. Stat. Med. 1998, 17, 2179–2197. [Google Scholar] [CrossRef]
- Pipper, C.B.; Ritz, C.; Bisgaard, H. A versatile method for confirmatory evaluation of the effects of a covariate in multiple models: Evaluation of Effects of a Covariate in Multiple Models. J. R. Stat. Soc. Ser. C (Appl. Stat.) 2012, 61, 315–326. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Ristl, R. Mmmgee: Simultaneous Inference for Multiple Linear Contrasts in GEE Models; R CRAN: Vienna, Austria, 2018. [Google Scholar]
- Carey, V.J.; Lumley, T.; Ripley, B.D. Gee: Generalized Estimation Equation Solver. R Package Version 2012, 4, 13–18. Available online: http://CRAN.R-project.org/package=gee (accessed on 5 February 2020).
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous inference in general parametric models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [Green Version]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Harrell, F.E.J. Rms: Regression Modeling Strategies, R package version 4.1-3; R CRAN: Vienna, Austria, 2014. [Google Scholar]
- Marrone, O.; Cibella, F.; Pépin, J.-L.; Grote, L.; Verbraecken, J.; Saaresranta, T.; Kvamme, J.A.; Basoglu, O.K.; Lombardi, C.; McNicholas, W.T.; et al. Fixed But Not Autoadjusting Positive Airway Pressure Attenuates the Time-dependent Decline in Glomerular Filtration Rate in Patients With OSA. Chest 2018, 154, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Jennum, P.; Tønnesen, P.; Ibsen, R.; Kjellberg, J. All-cause mortality from obstructive sleep apnea in male and female patients with and without continuous positive airway pressure treatment: A registry study with 10 years of follow-up. NSS 2015, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hommos, M.S.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes in Human Kidneys with Healthy Aging. J. Am. Soc. Nephrol. 2017, 28, 2838–2844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksen, B.O.; Stefansson, V.T.N.; Jenssen, T.G.; Mathisen, U.D.; Schei, J.; Solbu, M.D.; Wilsgaard, T.; Melsom, T. Blood pressure and age-related GFR decline in the general population. BMC Nephrol. 2017, 18, 77. [Google Scholar] [CrossRef] [Green Version]
- van Varik, B.J.; Vossen, L.M.; Rennenberg, R.J.; Stoffers, H.E.; Kessels, A.G.; de Leeuw, P.W.; Kroon, A.A. Arterial stiffness and decline of renal function in a primary care population. Hypertens. Res. 2017, 40, 73–78. [Google Scholar] [CrossRef]
- Adams, R.J.; Appleton, S.L.; Vakulin, A.; Hanly, P.J.; McDonald, S.P.; Martin, S.A.; Lang, C.J.; Taylor, A.W.; McEvoy, R.D.; Antic, N.A.; et al. Chronic Kidney Disease and Sleep Apnea Association of Kidney Disease with Obstructive Sleep Apnea in a Population Study of Men. Sleep 2017, 40, 1–9. [Google Scholar]
- Barcellos, R.C.D.B.; Matos, J.P.S.D.; Kang, H.C.; Rosa, M.L.G.; Lugon, J.R. Comparison of serum creatinine levels in different color/race categories in a Brazilian population. Cad. Saúde Pública 2015, 31, 1565–1569. [Google Scholar] [CrossRef] [Green Version]
- Ronco, C.; Bellomo, R.; Kellum, J. Understanding renal functional reserve. Intensive Care Med. 2017, 43, 917–920. [Google Scholar] [CrossRef]
- Ronco, C.; Legrand, M.; Goldstein, S.L.; Hur, M.; Tran, N.; Howell, E.C.; Cantaluppi, V.; Cruz, D.N.; Damman, K.; Bagshaw, S.M.; et al. Neutrophil gelatinase-associated lipocalin: Ready for routine clinical use? An international perspective. Blood Purif. 2014, 37, 271–285. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Other-PAP | C-PAP | Combined | p-value |
|---|---|---|---|---|
| (n = 9) | (n = 31) | (n = 40) | ||
| Sex: Female | 22% (2) | 19% (6) | 20% (8) | 0.800 |
| Male | 78% (7) | 81% (25) | 80% (32) | |
| Age at Diagnosis | 63 (58, 70) | 60 (50, 67) | 60 (54, 68) | 0.300 |
| BMI | 33 (31–35) | 33 (30, 36) | 33 (30, 35) | 0.700 |
| Smoker: No | 22% (2) | 29% (9) | 28% (11) | 0.700 |
| yes | 78% (7) | 71% (22) | 72% (29) | |
| AHI at diagnosis | 36 (28, 36) | 28 (16, 32) | 30 (19, 35) | 0.500 |
| Diabetes: No | 44% (4) | 68% (21) | 62% (25) | 0.200 |
| Yes | 56% (5) | 32% (10) | 38% (15) | |
| CHD: No | 89% (8) | 90% (28) | 90% (36) | 0.900 |
| Yes | 11% (1) | 10% (3) | 10% (4) | |
| CVD: No | 89% (8) | 100% (31) | 98% (39) | 0.060 |
| Yes | 11% (1) | 0% (0) | 2% (1) | |
| COPD No | 78% (7) | 84% (26) | 82% (33) | 0.700 |
| Yes | 22% (2) | 16% (5) | 18% (7) | |
| Asthma: No | 100% (9) | 77% (24) | 82% (33) | 0.100 |
| Yes | 0% (0) | 23% (7) | 18% (7) |
| Variable | Other-PAP | C-PAP | Combined | p-Value |
|---|---|---|---|---|
| (n = 9) | (n = 31) | (n = 40) | ||
| Creatinine delta (after−3 years) | 0.03 (−0.12, 0.13) | 0.08 (0, 0.16) | 0.08 (0, 0.16) | 0.300 |
| Creatinine delta (after−8 Years) | 0.005 (−0.207. 0.225) | 0.015 (−0.108. 0.135) | 0.015 (−0.118, 0.157) | 0.900 |
| eGFR delta (after−3 years) | 22 (22, 22) | −0.5 (−6, 5.8) | 2 (−5, 9) | 0.100 |
| eGFR delta (after−8 Years) | 10 (4, 15) | 4 (−4, 8) | 4 (−4, 8) | 0.500 |
| Panel 1 C-PAP Treatment | |||
|---|---|---|---|
| Variable | Baseline | 3 Years | p-Value |
| (n = 31) | (n = 31) | ||
| Creatinine | 1 (0.9, 1.1) | 0.9 (0.8, 1) | 0.006 |
| eGFR | 88 (73, 97) | 93 (79, 101) | 0.920 |
| Variable | Baseline | 8 Year | p-Value |
| (n = 31) | (n = 31) | ||
| Creatinine | 1 (0.9, 1.1) | 0.9 (0.8, 1.1) | 0.620 |
| eGFR | 88 (73, 97) | 79 (64, 94) | 0.880 |
| Variable | 3 years | 8 Year | p-Value |
| (n = 31) | (n = 31) | ||
| Creatinine | 0.9 (0.8, 1) | 0.9 (0.8, 1.1) | 0.060 |
| eGFR | 93 (79, 101) | 79 (64, 94) | 0.049 |
| Panel 2 Other-PAP Treatment | |||
| Variable | Baseline | 3 Years | p-Value |
| (n = 31) | (n = 31) | ||
| Creatinine | 0.8 (0.8, 0.9) | 0.7 (0.6, 1) | 0.900 |
| eGFR | 76 (74, 77) | 101 (74, 115) | 0.730 |
| Variable | Baseline | 8 Year | p-Value |
| (n = 31) | (n = 31) | ||
| Creatinine | 0.8 (0.8, 0.9) | 0.8 (0.5, 2.0) | 0.910 |
| eGFR | 76 (74, 77) | 100 (78, 108) | 0.700 |
| Variable | 3 years | 8 Year | p-Value |
| (n = 31) | (n = 31) | ||
| Creatinine | 0.7 (0.6, 1.0) | 0.8 (0.5, 2.0) | 0.920 |
| eGFR | 101(74, 115) | 100 (78, 108) | 0.850 |
| Outcome | β-Effect | 95% CI | p-Value | |
|---|---|---|---|---|
| Creatinine | Age | 0.011 | [−0.001; 0.02] | 0.082 |
| BMI | −0.006 | [−0.028; 0.02] | 0.572 | |
| Follow up time – 3 years vs. baseline | −0.044 | [−0.136; 0.05] | 0.349 | |
| 8 year vs. baseline | 0.117 | [−0.102; 0.34] | 0.295 | |
| treatment - other-PAP vs. C-PAP | −0.002 | [−0.576; 0.57] | 0.994 | |
| Sex – Male | 0.257 | [0.034; 0.48] | 0.024 | |
| Active Smoker –Yes | 0.133 | [−0.059; 0.32] | 0.174 | |
| eGFR | Age | −1.155 | [−1.922; −0.39] | 0.003 |
| BMI | 0.141 | [−1.175; 1.46] | 0.834 | |
| Follow up time –3 years vs. baseline | 0.18 | [−8.819; 9.18] | 0.969 | |
| 8 year vs. baseline | −10.61 | [−19.924; −1.29] | 0.026 | |
| treatment - other-PAP vs. C-PAP | 8.972 | [−15.899; 33.84] | 0.480 | |
| Sex –M | 4.002 | [−9.783; 17.79] | 0.569 | |
| Smoke –Yes | −13.34 | [−26.68; 0] | 0.050 | |
| Variable | Other-PAP | C-PAP | Combined | p-Value |
|---|---|---|---|---|
| (n = 9) | (n = 31) | (n = 40) | ||
| AHI (Basal) | 36 (28, 36) | 28 (16, 32) | 30 (19, 35) | 0.500 |
| AHI (3-years) | 0 (0, 0) | 1 (0, 2) | 1 (0, 2) | 0.300 |
| AHI (8-years) | 15 (15, 15) | 2 (2, 3) | 3 (2, 9) | 0.300 |
| ODI (Basal) | 30 (30, 30) | 24 (16, 48) | 26 (16, 44) | 0.600 |
| ODI (3-Years) | 7 (5,8) | 2 (1, 3) | 2 (1, 4) | 0.050 |
| ODI (8-Years) | 19 (19, 19) | 10 (9, 10) | 10 (10, 14) | 0.300 |
| T90 (Basal) | 7 (7, 7) | 12 (4, 38) | 11 (5, 38) | 0.800 |
| T90 (3-Years) | 1.2 (1.1, 1.3) | 1 (0.3, 2) | 1 (0.6, 1.7) | 0.700 |
| T90 (8-Years) | 3 (3, 3) | 4 (3, 6) | 3 (2, 6) | 0.999 |
| Mean Nocturnal Oxygen Saturation (%) (Basal) | 94 (94, 94) | 92 (91, 92) | 92 (92, 92) | 0.100 |
| Mean Nocturnal Oxygen Saturation (%) (3-Years) | 95 (95, 96) | 95 (94, 95) | 95 (94, 95) | 0.300 |
| Mean Nocturnal Oxygen Saturation (%) (8-Years) | 94 (94, 94) | 94 (93, 94) | 94 (94, 94) | 0.700 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pochetti, P.; Azzolina, D.; Ragnoli, B.; Tillio, P.A.; Cantaluppi, V.; Malerba, M. Interrelationship among Obstructive Sleep Apnea, Renal Function and Survival: A Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 4922. https://doi.org/10.3390/ijerph17144922
Pochetti P, Azzolina D, Ragnoli B, Tillio PA, Cantaluppi V, Malerba M. Interrelationship among Obstructive Sleep Apnea, Renal Function and Survival: A Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(14):4922. https://doi.org/10.3390/ijerph17144922
Chicago/Turabian StylePochetti, Patrizia, Danila Azzolina, Beatrice Ragnoli, Paolo Amedeo Tillio, Vincenzo Cantaluppi, and Mario Malerba. 2020. "Interrelationship among Obstructive Sleep Apnea, Renal Function and Survival: A Cohort Study" International Journal of Environmental Research and Public Health 17, no. 14: 4922. https://doi.org/10.3390/ijerph17144922