Breastfeeding in Hospitals: Factors Influencing Maternal Choice in Italy

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Horta, B.L.; Victora, C.G.; World Health Organization. Short-Term Effects of Breastfeeding: A Systematic Review on the Benefits of Breastfeeding on Diarrhoea and Pneumonia Mortality; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Bernardo, H.; Cesar, V.; World Health Organization. Long-Term Effects of Breastfeeding: A Systematic Review; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Miksic, S.; Uglesic, B.; Jakab, J.; Holik, D.; Milostic Srb, A.; Degmecic, D. Positive Effect of Breastfeeding on Child Development, Anxiety, and Postpartum Depression. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef] [Green Version]
- Del Ciampo, L.A.; Del Ciampo, I.R.L. Breastfeeding and the Benefits of Lactation for Women’s Health. Rev. Bras. Ginecol. Obstet. 2018, 40, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loof-Johanson, M.; Brudin, L.; Sundquist, M.; Rudebeck, C.E. Breastfeeding Associated with Reduced Mortality in Women with Breast Cancer. Breastfeed. Med. 2016, 11, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.J.; Na, R.; Johnatty, S.E.; Wise, L.A.; Adami, H.O.; Brinton, L.A.; Chen, C.; Cook, L.S.; Dal Maso, L.; De Vivo, I.; et al. Breastfeeding and Endometrial Cancer Risk: An Analysis from the Epidemiology of Endometrial Cancer Consortium. Obstet. Gynecol. 2017, 129, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Li, D.P.; Du, C.; Zhang, Z.M.; Li, G.X.; Yu, Z.F.; Wang, X.; Li, P.F.; Cheng, C.; Liu, Y.P.; Zhao, Y.S. Breastfeeding and ovarian cancer risk: A systematic review and meta-analysis of 40 epidemiological studies. Asian Pac. J. Cancer Prev. 2014, 15, 4829–4837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellia, A.; Vitale, S.G.; Lagana, A.S.; Cannone, F.; Houvenaeghel, G.; Rua, S.; Ladaique, A.; Jauffret, C.; Ettore, G.; Lambaudie, E. Feasibility and surgical outcomes of conventional and robot-assisted laparoscopy for early-stage ovarian cancer: A retrospective, multicenter analysis. Arch. Gynecol. Obstet. 2016, 294, 615–622. [Google Scholar] [CrossRef]
- Cignini, P.; Vitale, S.G.; Lagana, A.S.; Biondi, A.; La Rosa, V.L.; Cutillo, G. Preoperative work-up for definition of lymph node risk involvement in early stage endometrial cancer: 5-year follow-up. Updates Surg. 2017, 69, 75–82. [Google Scholar] [CrossRef]
- Bernardi, S.; Londero, A.P.; Bertozzi, S.; Driul, L.; Marchesoni, D.; Petri, R. Breast-feeding and benign breast disease. J. Obstet. Gynaecol. 2012, 32, 58–61. [Google Scholar] [CrossRef] [Green Version]
- Magro, G.; Angelico, G.; Spadola, S.; Ragusa, R.; Righi, A.; Orviero, E. Fibroma of the breast: A rare tumour in the spectrum of the benign spindle cell tumours of the mammary stroma. Pol. J. Pathol. 2018, 69, 189–194. [Google Scholar] [CrossRef]
- Joham, A.E.; Nanayakkara, N.; Ranasinha, S.; Zoungas, S.; Boyle, J.; Harrison, C.L.; Forder, P.; Loxton, D.; Vanky, E.; Teede, H.J. Obesity, polycystic ovary syndrome and breastfeeding: An observational study. Acta Obstet. Gynecol. Scand. 2016, 95, 458–466. [Google Scholar] [CrossRef]
- Lagana, A.S.; Rossetti, P.; Sapia, F.; Chiofalo, B.; Buscema, M.; Valenti, G.; Rapisarda, A.M.C.; Vitale, S.G. Evidence-Based and Patient-Oriented Inositol Treatment in Polycystic Ovary Syndrome: Changing the Perspective of the Disease. Int. J. Endocrinol. Metab. 2017, 15, e43695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Munoz, E.; Sathyapalan, T.; Rossetti, P.; Shah, M.; Long, M.; Buscema, M.; Valenti, G.; La Rosa, V.L.; Cianci, S.; Vitale, S.G. Polycystic Ovary Syndrome: Implication for Drug Metabolism on Assisted Reproductive Techniques-A Literature Review. Adv. Ther. 2018, 35, 1805–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C.L.; Teede, H.J.; Joham, A.E.; Moran, L.J. Breastfeeding and obesity in PCOS. Expert Rev. Endocrinol. Metab. 2016, 11, 449–454. [Google Scholar] [CrossRef]
- Aguilar Cordero, M.J.; Madrid Banos, N.; Baena Garcia, L.; Mur Villar, N.; Guisado Barrilao, R.; Sanchez Lopez, A.M. Breastfeeding as a method to prevent cardiovascular diseases in the mother and the child. Nutr. Hosp. 2015, 31, 1936–1946. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wang, J.; Zhou, W.; Yin, H.; Wang, M. Breastfeeding and Risk of Rheumatoid Arthritis: A Systematic Review and Metaanalysis. J. Rheumatol. 2015, 42, 1563–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, M.; Berzuini, C.; Knapp, L.A. Maternal breastfeeding history and Alzheimer’s disease risk. J. Alzheimer’s Dis. JAD 2013, 37, 809–821. [Google Scholar] [CrossRef] [PubMed]
- Langer-Gould, A.; Smith, J.B.; Hellwig, K.; Gonzales, E.; Haraszti, S.; Koebnick, C.; Xiang, A. Breastfeeding, ovulatory years, and risk of multiple sclerosis. Neurology 2017, 89, 563–569. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Breastfeeding. Available online: https://www.who.int/health-topics/breastfeeding#tab=tab_1 (accessed on 9 April 2020).
- Bagci Bosi, A.T.; Eriksen, K.G.; Sobko, T.; Wijnhoven, T.M.; Breda, J. Breastfeeding practices and policies in WHO European Region Member States. Public Health Nutr. 2016, 19, 753–764. [Google Scholar] [CrossRef] [Green Version]
- Bizon, A.; Giugliani, C.; Castro de Avilla Lago, J.; de Senna, A.F.K.; Martins, A.C.M.; de Jezus Castro, S.M.; Giugliani, E.R.J. Combined pro-breastfeeding practices are advantageous in facilities providing maternity and newborn services. Matern. Child Nutr. 2019, 15, e12822. [Google Scholar] [CrossRef] [Green Version]
- Ikonen, R.; Paavilainen, E.; Kaunonen, M. Preterm Infants’ Mothers’ Experiences With Milk Expression and Breastfeeding: An Integrative Review. Adv. Neonatal Care 2015, 15, 394–406. [Google Scholar] [CrossRef]
- Vitale, S.G.; Marilli, I.; Rapisarda, A.M.; Rossetti, D.; Belluomo, G.; Iapichino, V.; Stancanelli, F.; Cianci, A. Cellular and biochemical mechanisms, risk factors and management of preterm birth: State of the art. Minerva Ginecol. 2014, 66, 589–595. [Google Scholar] [PubMed]
- Wouk, K.; Stuebe, A.M.; Meltzer-Brody, S. Postpartum Mental Health and Breastfeeding Practices: An Analysis Using the 2010-2011 Pregnancy Risk Assessment Monitoring System. Matern. Child Health J. 2017, 21, 636–647. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Lagana, A.S.; Muscatello, M.R.; La Rosa, V.L.; Curro, V.; Pandolfo, G.; Zoccali, R.A.; Bruno, A. Psychopharmacotherapy in Pregnancy and Breastfeeding. Obstet. Gynecol. Surv. 2016, 71, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Pratt, B.A.; Longo, J.; Gordon, S.C.; Jones, N.A. Perceptions of Breastfeeding for Women with Perinatal Depression: A Descriptive Phenomenological Study. Issues Ment. Health Nurs. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Canicali Primo, C.; de Oliveira Nunes, B.; de Fatima Almeida Lima, E.; Marabotti Costa Leite, F.; Barros de Pontes, M.; Gomes Brandao, M.A. Which factors influence women in the decision to breastfeed? Investig. Educ. Enferm. 2016, 34, 198–217. [Google Scholar] [CrossRef] [Green Version]
- Italian Ministry of Health Tavolo Tecnico Operativo Interdisciplinare per la Promozione Dell’allattamento al seno (TAS). Available online: http://www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=3894&area=nutrizione&menu=allattamento (accessed on 9 May 2020).
- Mateus Solarte, J.C.; Cabrera Arana, G.A. Factors associated with exclusive breastfeeding practice in a cohort of women from Cali, Colombia. Colomb. Med. (CaliColomb.) 2019, 50, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Garbarino, F.; Morniroli, D.; Ghirardi, B.; Garavaglia, E.; Bracco, B.; Gianni, M.L.; Roggero, P.; Mosca, F. Prevalence and duration of breastfeeding during the first six months of life: Factors affecting an early cessation. Pediatr. Med. Chir. 2013, 35, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Ayton, J.E.; Tesch, L.; Hansen, E. Women’s experiences of ceasing to breastfeed: Australian qualitative study. BMJ Open 2019, 9, e026234. [Google Scholar] [CrossRef] [Green Version]
- Isik, Y.; Dag, Z.O.; Tulmac, O.B.; Pek, E. Early postpartum lactation effects of cesarean and vaginal birth. Ginekol. Pol. 2016, 87, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Mitha, A.; Piedvache, A.; Khoshnood, B.; Fresson, J.; Glorieux, I.; Roue, J.M.; Blondel, B.; Durox, M.; Burguet, A.; Ancel, P.Y.; et al. The impact of neonatal unit policies on breast milk feeding at discharge of moderate preterm infants: The EPIPAGE-2 cohort study. Matern. Child Nutr. 2019, 15, e12875. [Google Scholar] [CrossRef] [Green Version]
- Barrera, C.M.; Nelson, J.M.; Boundy, E.O.; Perrine, C.G. Trends in rooming-in practices among hospitals in the United States, 2007–2015. Birth 2018, 45, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Mc Loughlin, G. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Int. J. Nurs. Pract. 2019, 25, e12731. [Google Scholar] [CrossRef] [PubMed]
- Jaafar, S.H.; Ho, J.J.; Lee, K.S. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Cochrane Database Syst. Rev. 2016, Cd006641. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.A.; Ho, J.J.; Lee, Z.H. The effect of rooming-in on duration of breastfeeding: A systematic review of randomised and non-randomised prospective controlled studies. PLoS ONE 2019, 14, e0215869. [Google Scholar] [CrossRef] [Green Version]
- McRae, M.J. Exclusive Breastfeeding, 24-Hour Rooming-In, and the Importance of Women’s Informed Choices. Nurs. Womens Health 2019, 23, 309–315. [Google Scholar] [CrossRef]
- Artieta-Pinedo, I.; Paz-Pascual, C.; Grandes, G.; Bacigalupe, A.; Payo, J.; Montoya, I. Antenatal education and breastfeeding in a cohort of primiparas. J. Adv. Nurs. 2013, 69, 1607–1617. [Google Scholar] [CrossRef]
- Mahesh, P.K.B.; Gunathunga, M.W.; Arnold, S.M.; Jayasinghe, C.; Pathirana, S.; Makarim, M.F.; Manawadu, P.M.; Senanayake, S.J. Effectiveness of targeting fathers for breastfeeding promotion: Systematic review and meta-analysis. BMC Public Health 2018, 18, 1140. [Google Scholar] [CrossRef]
- Alberdi, G.; O’Sullivan, E.J.; Scully, H.; Kelly, N.; Kincaid, R.; Murtagh, R.; Murray, S.; McGuinness, D.; Clive, A.; Brosnan, M.; et al. A feasibility study of a multidimensional breastfeeding-support intervention in Ireland. Midwifery 2018, 58, 86–92. [Google Scholar] [CrossRef]
- Ladomenou, F.; Moschandreas, J.; Kafatos, A.; Tselentis, Y.; Galanakis, E. Protective effect of exclusive breastfeeding against infections during infancy: A prospective study. Arch. Dis. Child 2010, 95, 1004–1008. [Google Scholar] [CrossRef]
- Ardic, C.; Yavuz, E. Effect of breastfeeding on common pediatric infections: A 5-year prospective cohort study. Arch. Argent Pediatr. 2018, 116, 126–132. [Google Scholar] [CrossRef]
- Duijts, L.; Jaddoe, V.W.; Hofman, A.; Moll, H.A. Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy. Pediatrics 2010, 126, e18–e25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragusa, R.; Corsaro, L.S.; Frazzetto, E.; Bertino, E.; Bellia, M.A.; Bertino, G. Hepatitis C Virus Infection in Children and Pregnant Women: An Updated Review of the Literature on Screening and Treatments. Ajp Rep. 2020, 10, e121–e127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zappala, G.; Platania, A.; Paladino, G.; Nicolosi, L.K.; Ragusa, R.; Marranzano, M. Meal habits and metabolic status in Southern Italian adults. Nutr. Healthy Aging 2019, 5, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Rito, A.I.; Buoncristiano, M.; Spinelli, A.; Salanave, B.; Kunesova, M.; Hejgaard, T.; Garcia Solano, M.; Fijalkowska, A.; Sturua, L.; Hyska, J.; et al. Association between Characteristics at Birth, Breastfeeding and Obesity in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative—COSI 2015/2017. Obes. Facts 2019, 12, 226–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Hansen, K. Breastfeeding: A smart investment in people and in economies. Lancet 2016, 387, 416. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Total | Community Hospital (A) | Public, Specialized Hospital (B) | Public, Emergency Hospital (C) | Public, Teaching Hospital (D) | Private Hospital (E) |
|---|---|---|---|---|---|---|
| No. of questionnaires | 3813 | 789 | 1193 | 96 | 1285 | 450 |
| % coverage * | 38 | 70 | 32 | 32 | 23–36 ** | 28 |
| Age (yrs., mean ± std. dev.) | 31.3 ± 5.8 | 29.7 ± 6.0 § | 31.9 ± 5.6 | 31.4 ± 6.1 | 32.1 ± 5.5 | 31.3 ± 5.7 |
| Age range (years, min–max) | 15–58 | 16–52 | 15–50 | 21–58 | 17–48 | 15–44 |
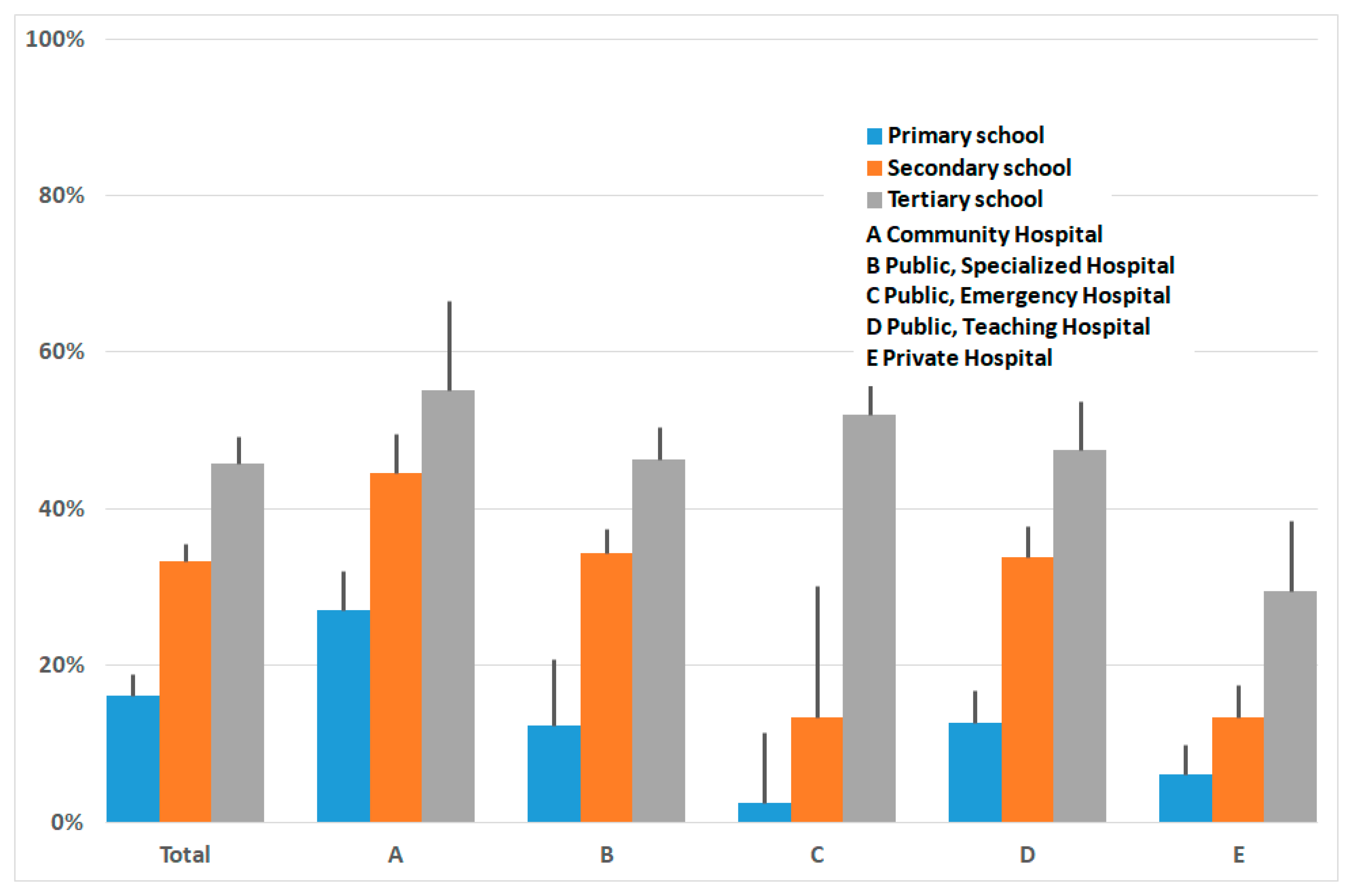
| Education level | ||||||
| primary % | 15 | 34 | 4 | 6 | 15 | 14 |
| secondary % | 53 | 53 | 56 | 22 | 53 | 46 |
| tertiary % | 31 | 13 | 40 | 72 | 32 | 40 |
| Caesarean Section % | 39 | 29 | 37 | 49 | 39 | 61 |
| Primiparae % | 48 | 43 | 52 | 57 | 48 | 41 |
| Rooming-in % | 91 | 66 | 96 | 81 | 99 | 100 |
| Birth preparation courses % | 31 | 38 | 36 | 19 | 29 | 14 |
| Received information on breastfeeding in hospital % | 89 | 93 | 99 | 90 | 79 | 86 |
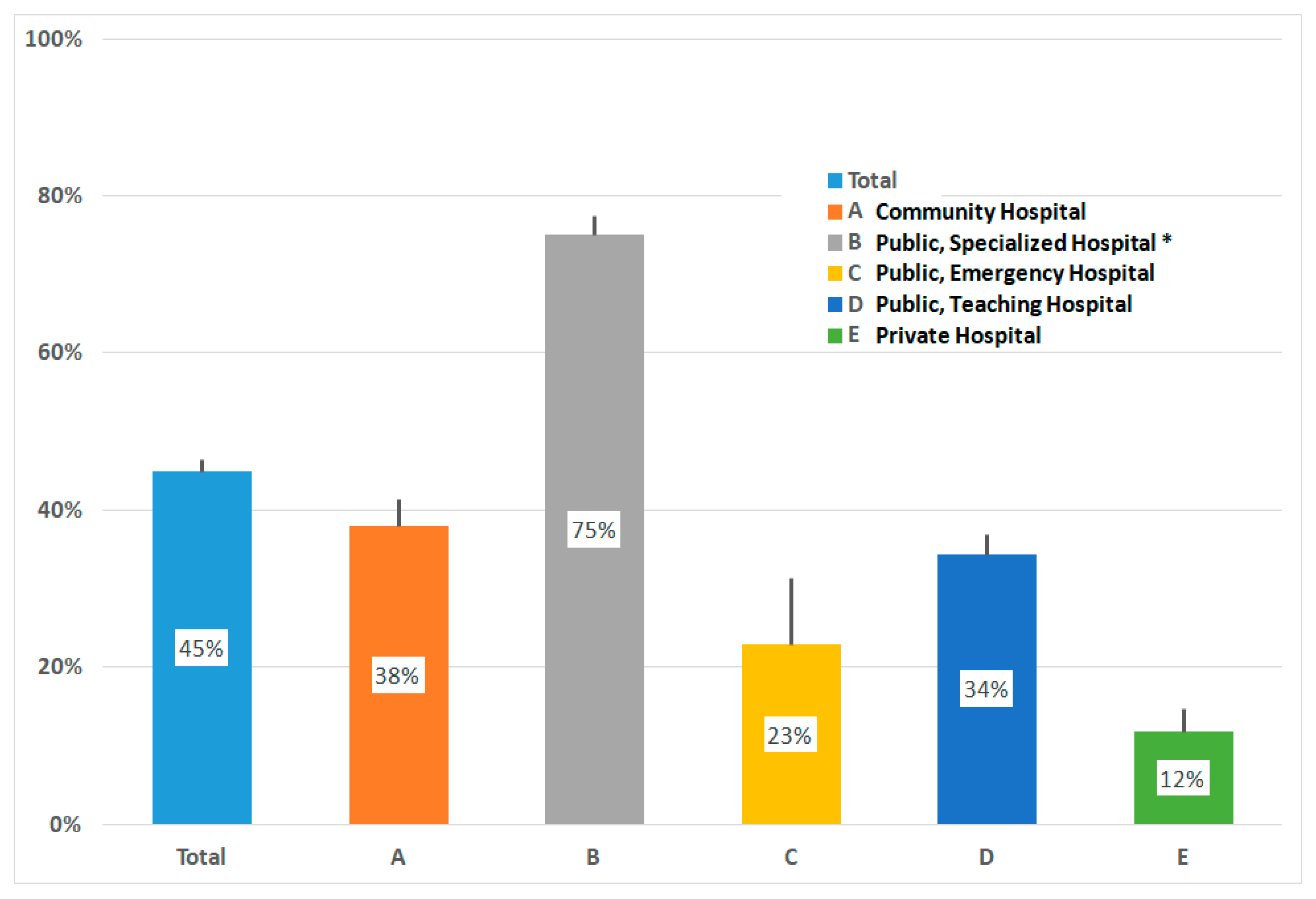
| Exclusive Breastfeeding % | 45 | 38 | 75 §§ | 23 | 34 | 12 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ragusa, R.; Giorgianni, G.; Marranzano, M.; Cacciola, S.; La Rosa, V.L.; Giarratana, A.; Altadonna, V.; Guardabasso, V. Breastfeeding in Hospitals: Factors Influencing Maternal Choice in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3575. https://doi.org/10.3390/ijerph17103575
Ragusa R, Giorgianni G, Marranzano M, Cacciola S, La Rosa VL, Giarratana A, Altadonna V, Guardabasso V. Breastfeeding in Hospitals: Factors Influencing Maternal Choice in Italy. International Journal of Environmental Research and Public Health. 2020; 17(10):3575. https://doi.org/10.3390/ijerph17103575
Chicago/Turabian StyleRagusa, Rosalia, Gabriele Giorgianni, Marina Marranzano, Salvatore Cacciola, Valentina Lucia La Rosa, Alessandra Giarratana, Valentina Altadonna, and Vincenzo Guardabasso. 2020. "Breastfeeding in Hospitals: Factors Influencing Maternal Choice in Italy" International Journal of Environmental Research and Public Health 17, no. 10: 3575. https://doi.org/10.3390/ijerph17103575