Intracervical Foley Catheter Plus Intravaginal Misoprostol vs Intravaginal Misoprostol Alone for Cervical Ripening: A Meta-Analysis

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction
2.4. Selection of Outcomes
2.5. Statistical Analysis
3. Results
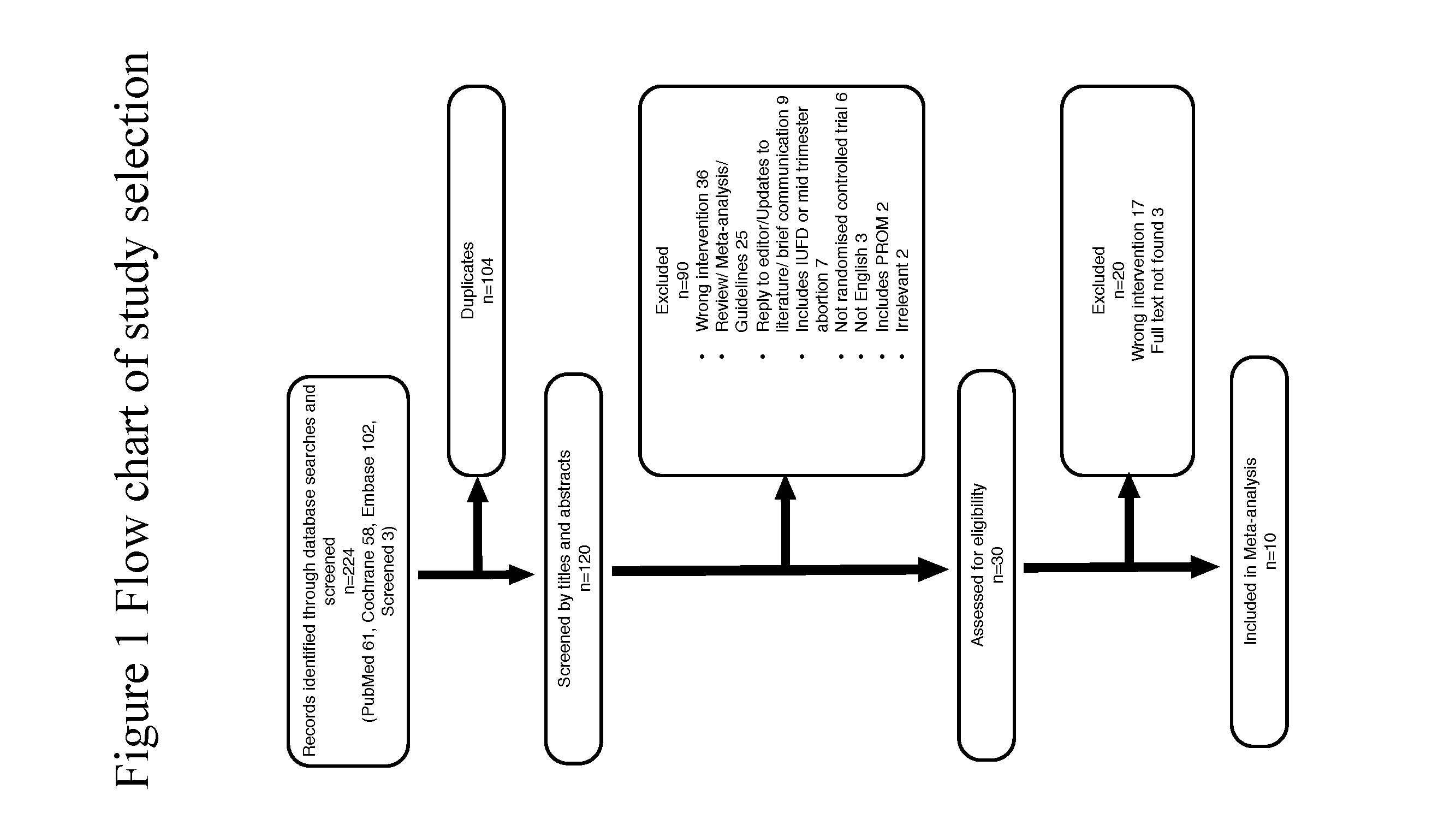
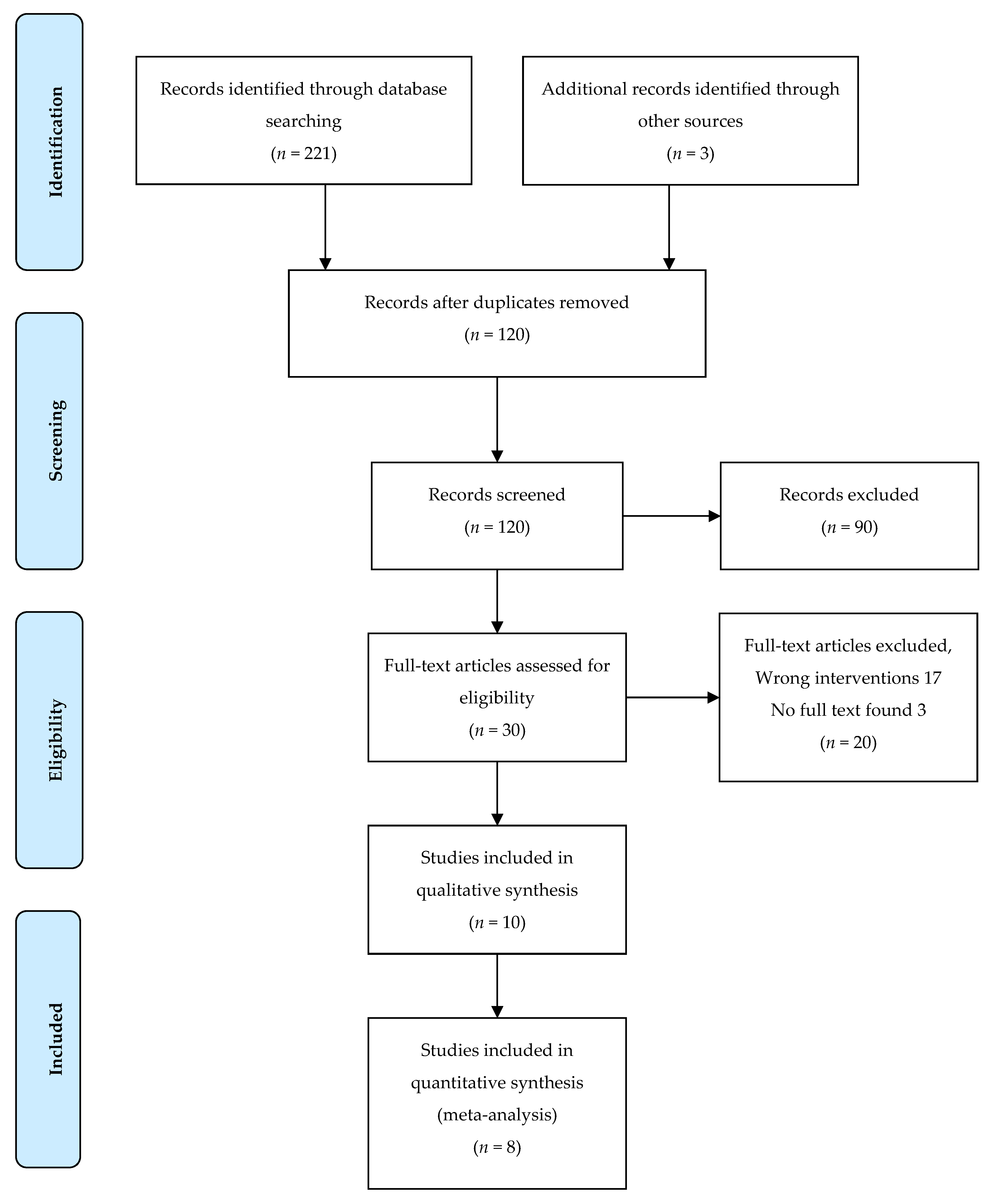
3.1. Study Selection, Quality Assessment, and Study Characteristics
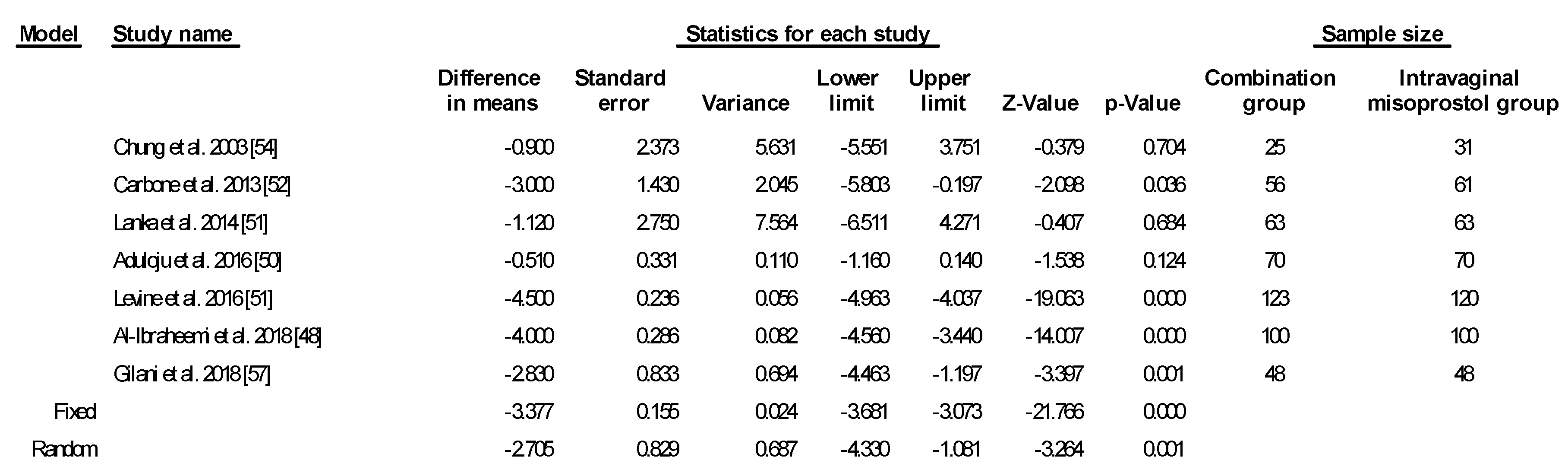
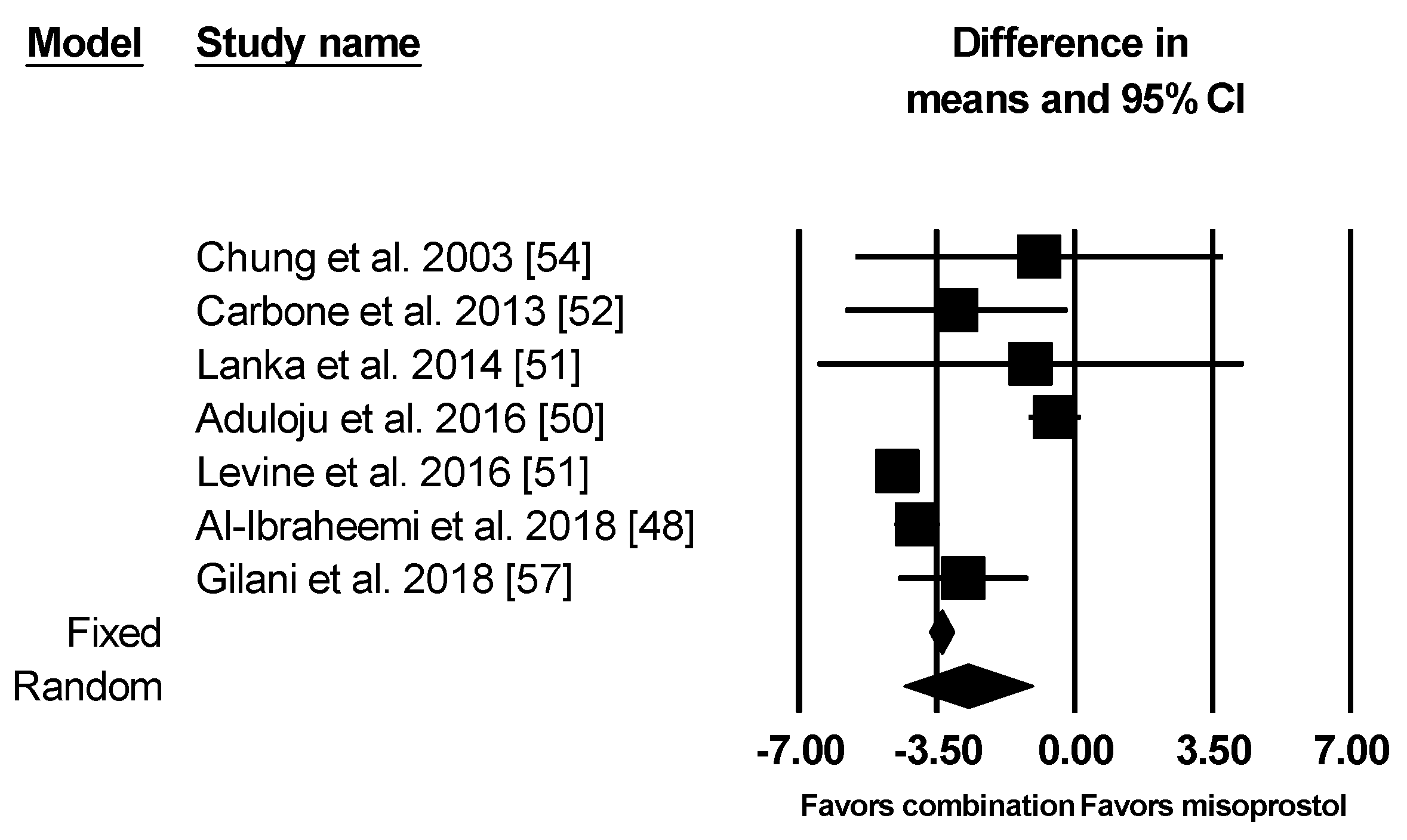
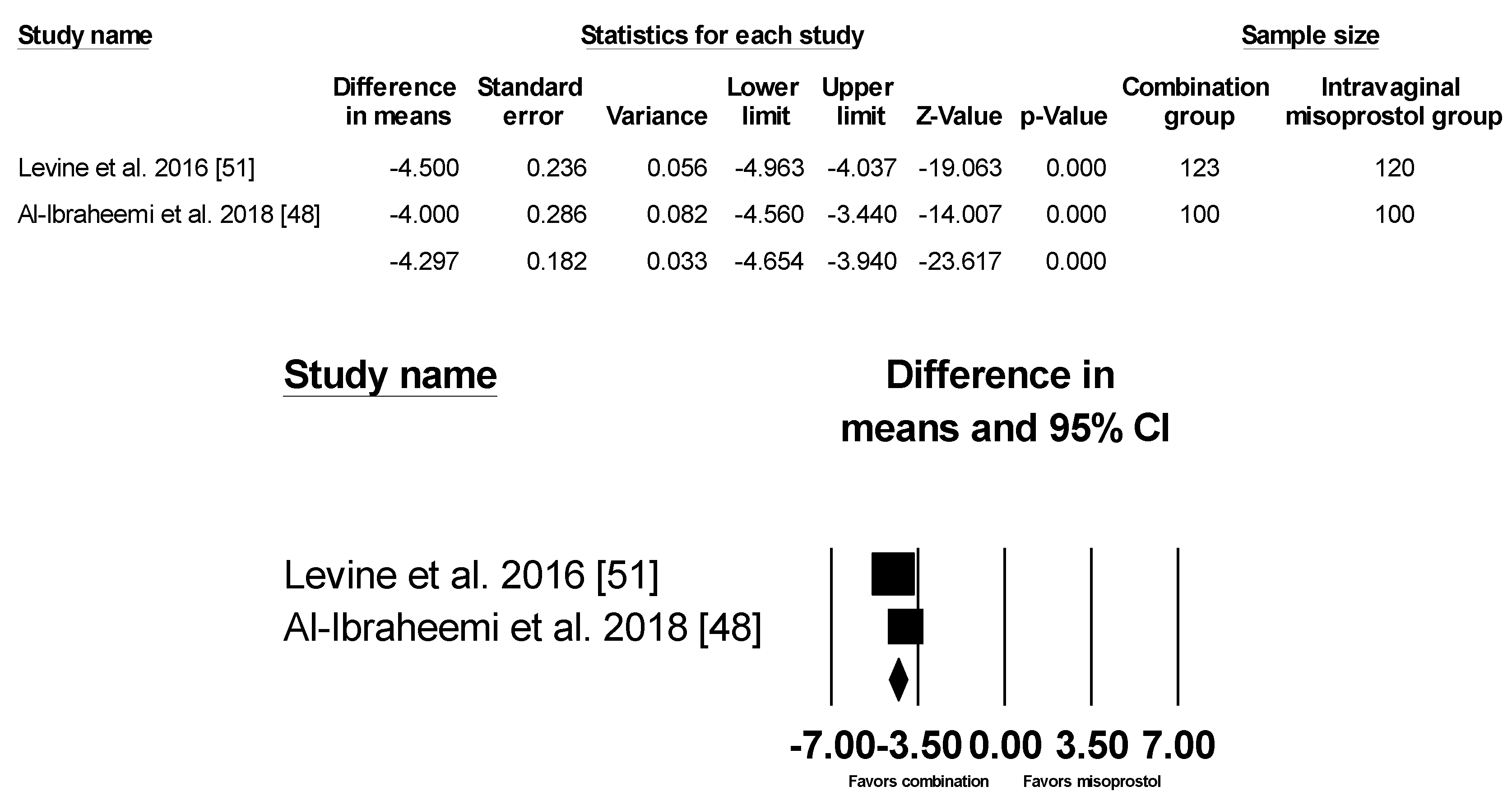
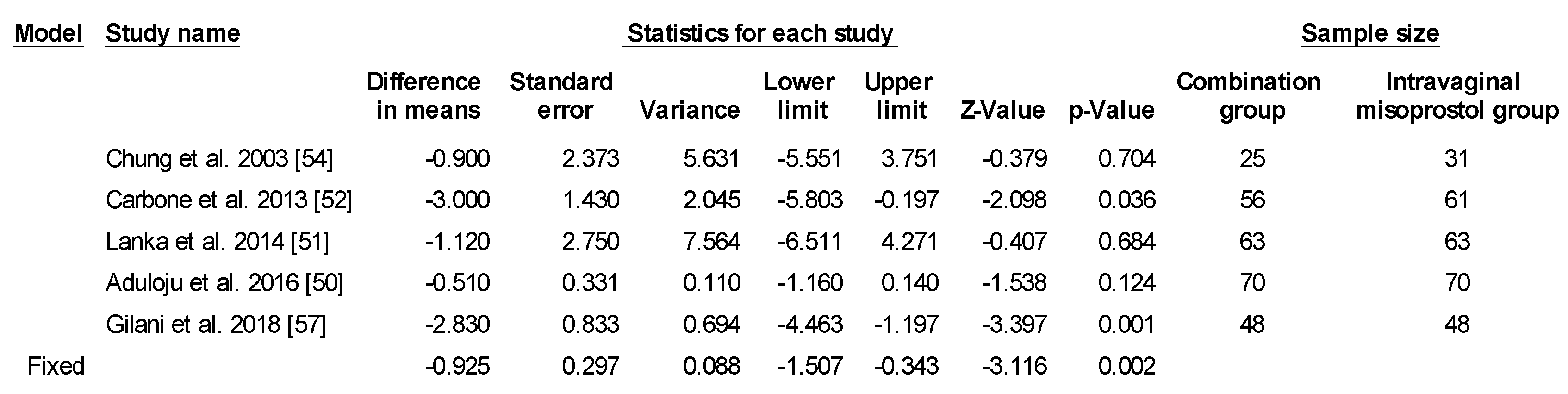
3.2. Time to Delivery
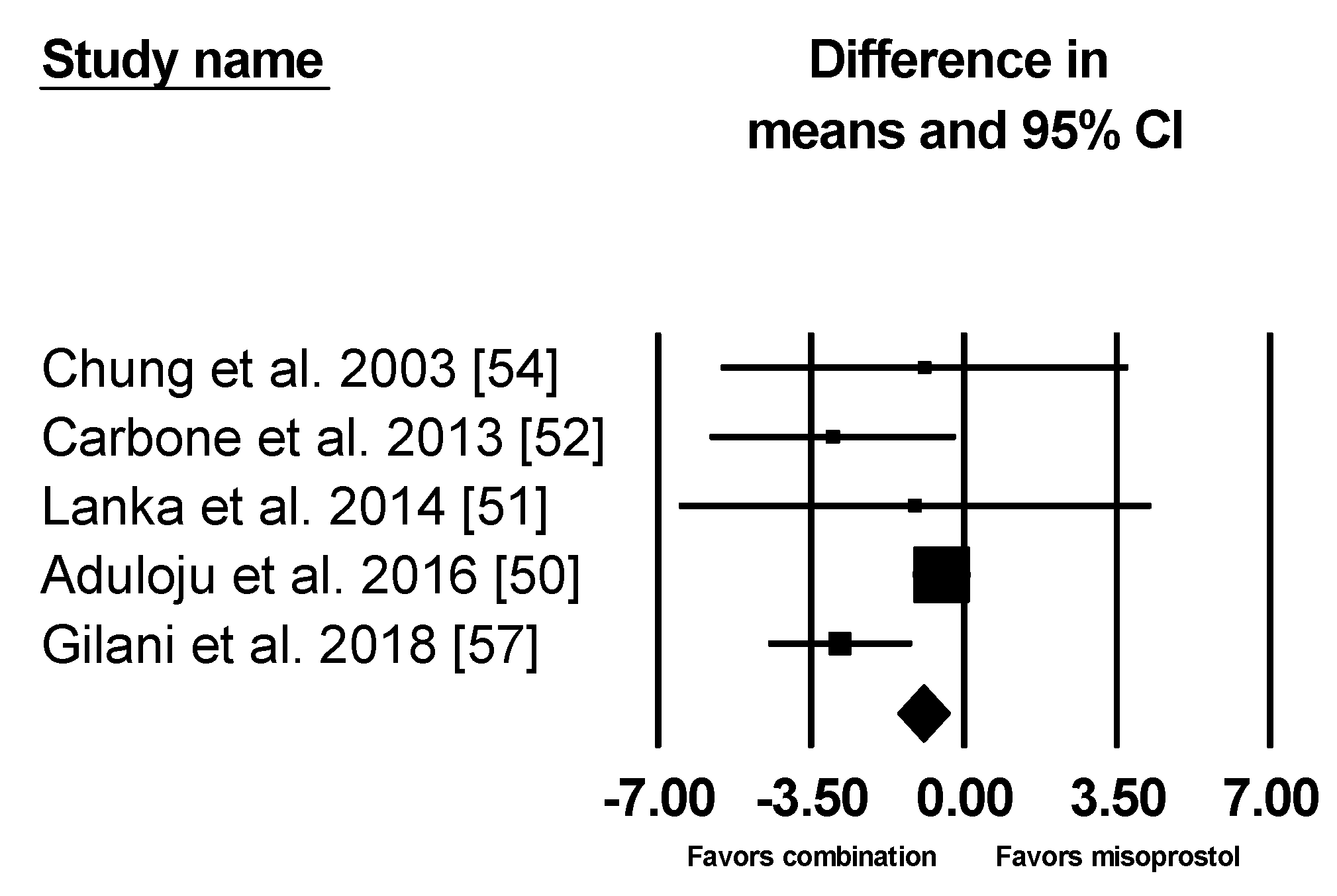
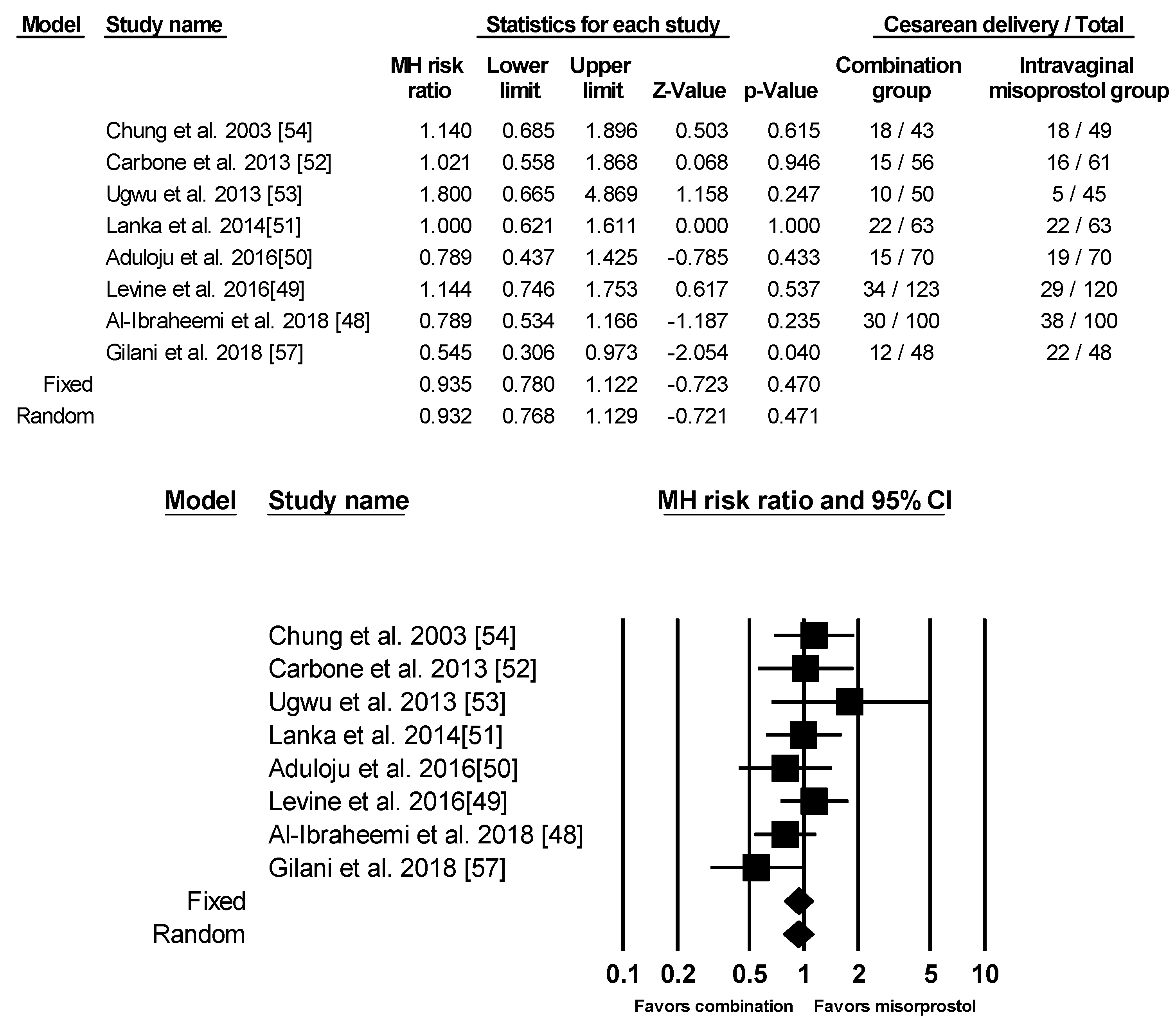
3.3. Cesarean Delivery
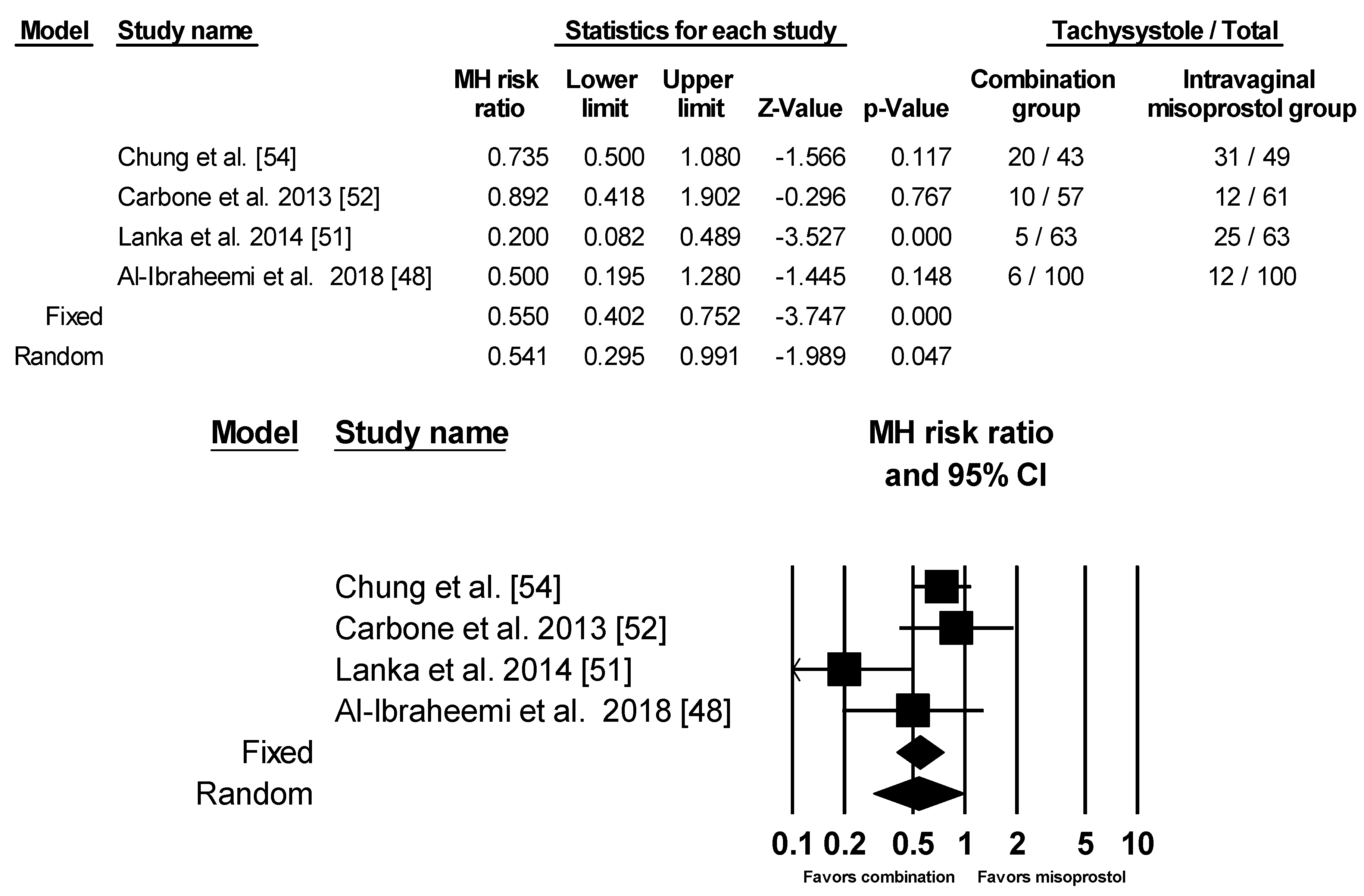
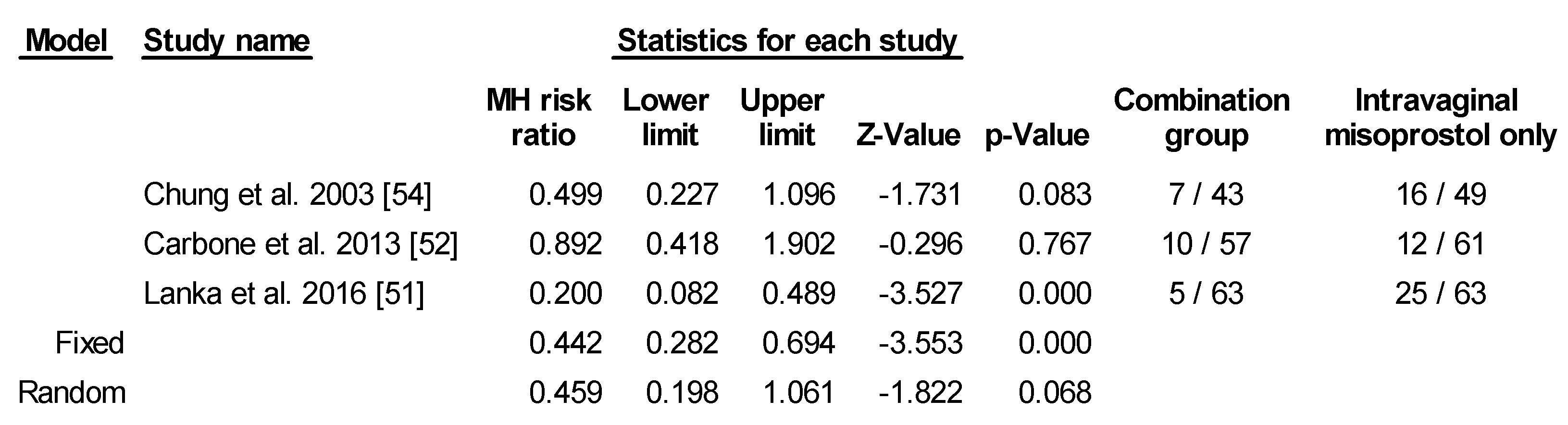
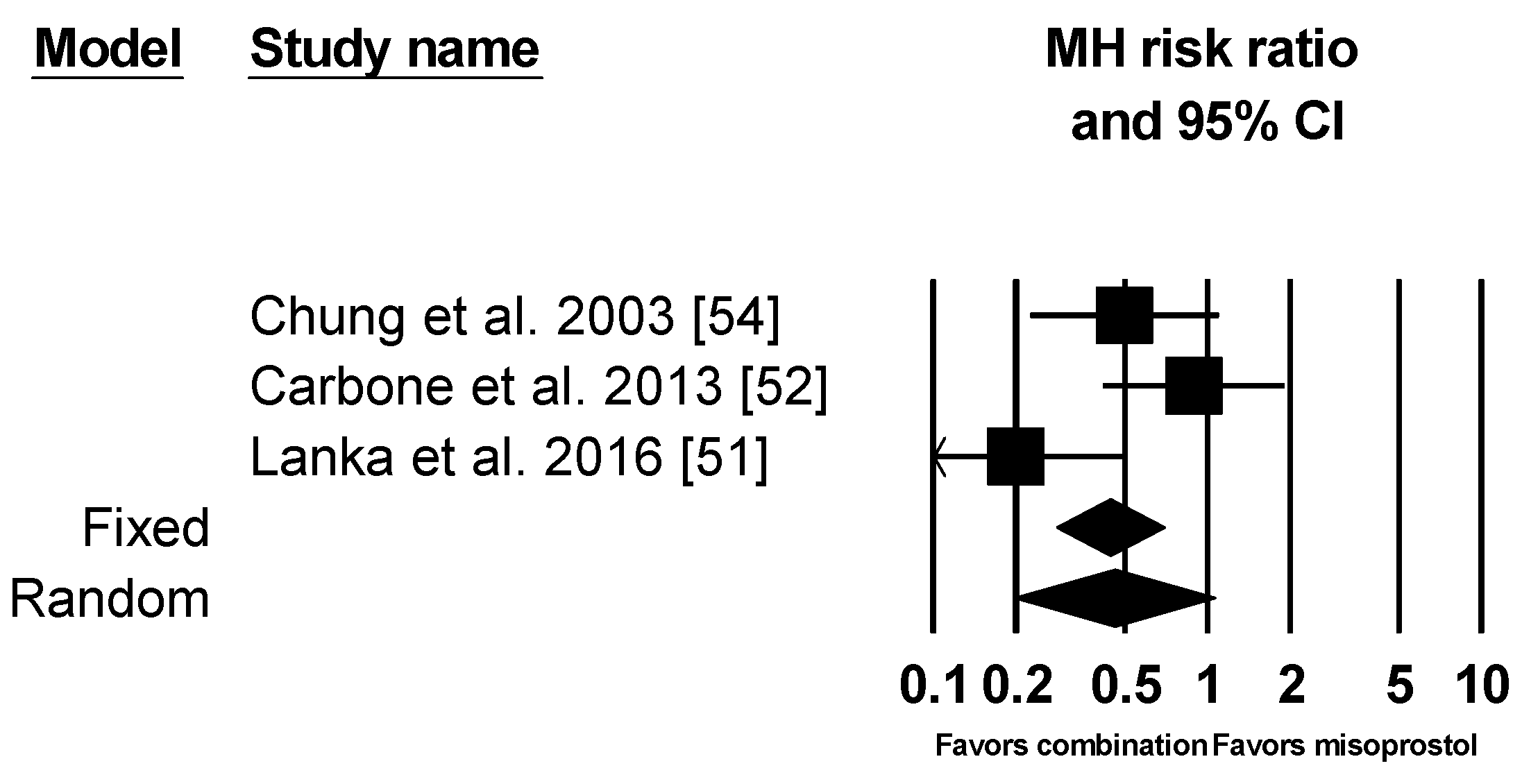
3.4. Uterine Tachysystole with and without Fetal Heart Rate Changes
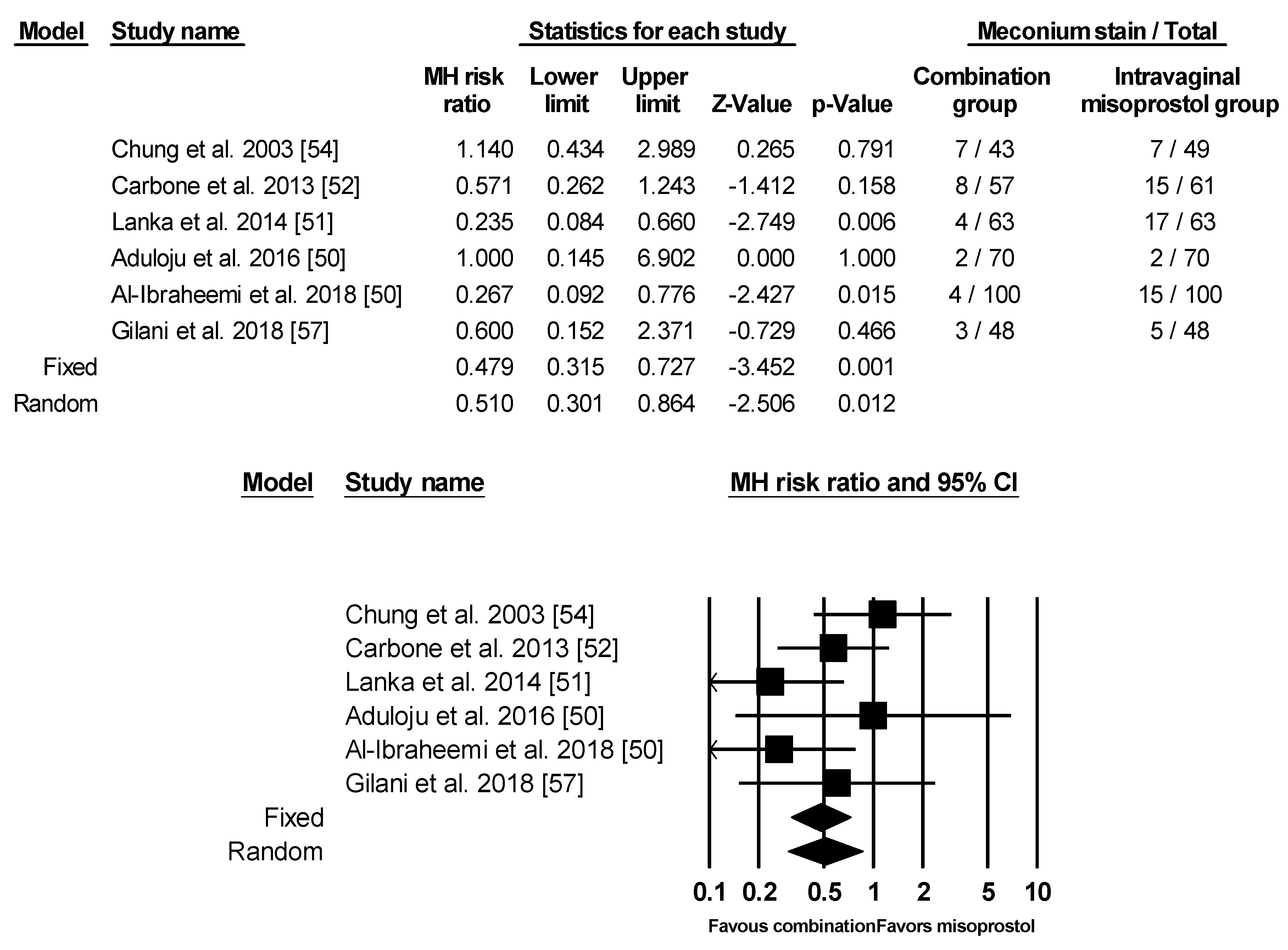
3.5. Meconium Stain
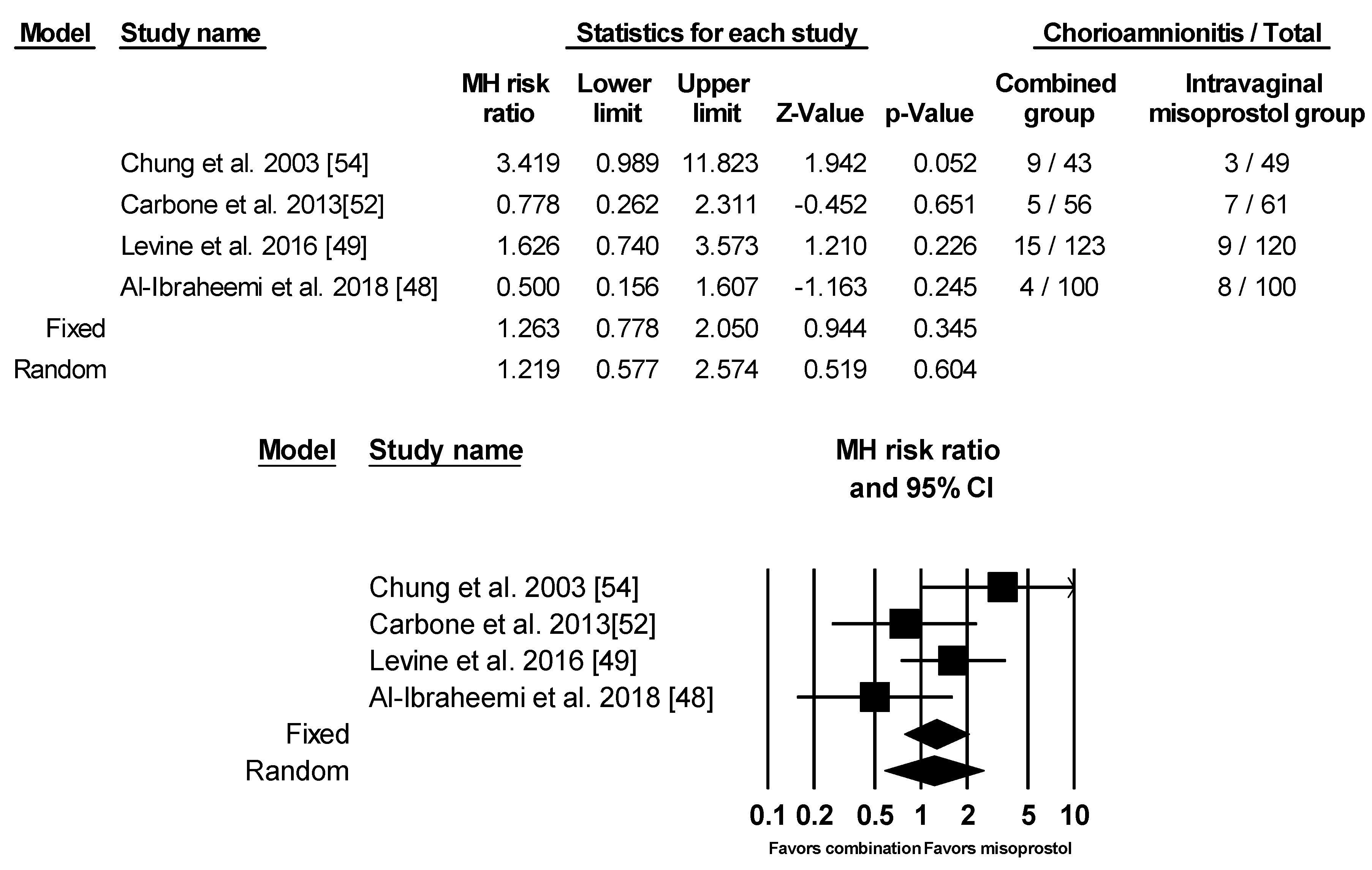
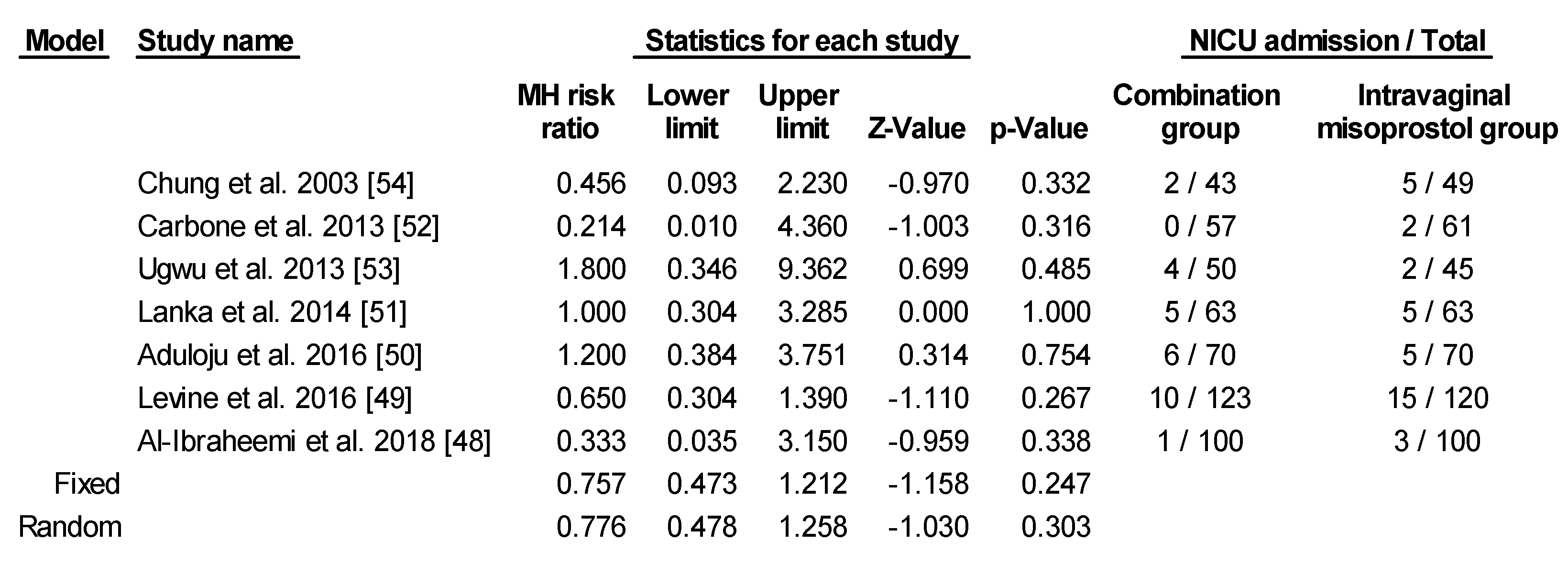
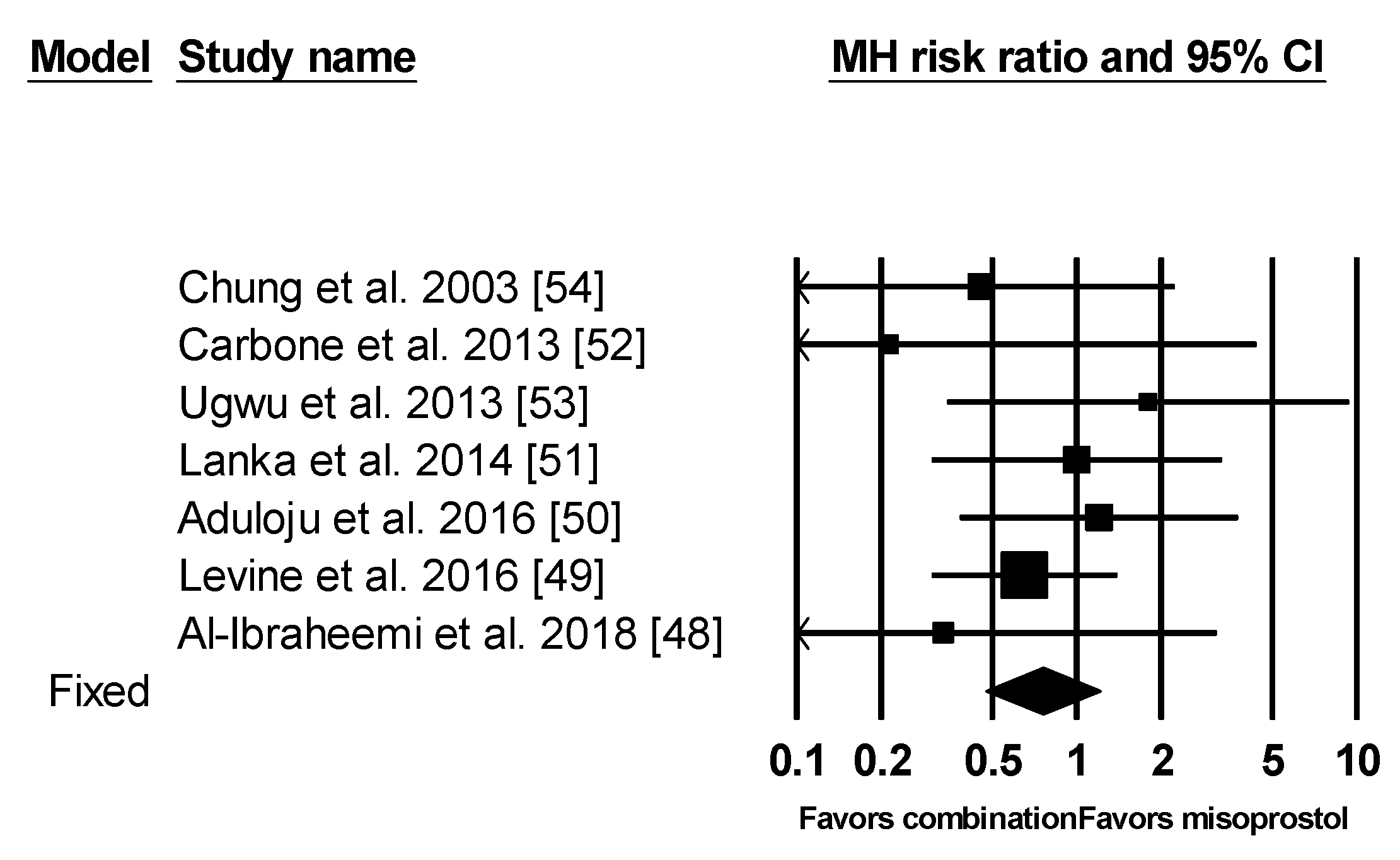
3.6. Other Outcomes
3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- de Vaan, M.D.; Ten Eikelder, M.L.; Jozwiak, M.; Palmer, K.R.; Davies-Tuck, M.; Bloemenkamp, K.W.; Mol, B.W.J.; Boulvain, M. Mechanical methods for induction of labour. Cochrane Database Syst. Rev. 2019, 10, CD001233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huisman, C.M.A.; Ten Eikelder, M.L.G.; Mast, K.; Oude Rengerink, K.; Jozwiak, M.; van Dunné, F.; Duvekot, J.J.; van Eyck, J.; Gaugler-Senden, I.; de Groot, C.J.M.; et al. PROBAAT-S project group. Balloon catheter for induction of labor in women with one previous cesarean and an unfavorable cervix. Acta. Obstet. Gynecol. Scand. 2019, 98, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ten Eikelder, M.L.G.; van Baaren, G.J.; Oude Rengerink, K.; Jozwiak, M.; de Leeuw, J.W.; Kleiverda, G.; Evers, I.; de Boer, K.; Brons, J.; Bloemenkamp, K.W.M.; et al. Comparing induction of labour with oral misoprostol or Foley catheter at term: Cost-effectiveness analysis of a randomised controlled multi-centre non-inferiority trial. BJOG 2018, 125, 375–383. [Google Scholar] [CrossRef]
- Atia, H.; Ellaithy, M.; Altraigey, A.; Kolkailah, M.; Alserehi, A.; Ashfaq, S. Mechanical induction of labor and ecbolic-less vaginal birth after cesarean section: A cohort study. Taiwan J. Obstet. Gynecol. 2018, 57, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, A.; Mahmoud, A.A.; Ellaithy, M.I.; Abees, S.H. Pre-induction cervical ripening using two different dinoprostone vaginal preparations: A randomized clinical trial of tablets and slow release retrievable insert. Taiwan J. Obstet. Gynecol. 2018, 57, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Mundle, S.; Bracken, H.; Khedikar, V.; Mulik, J.; Faragher, B.; Easterling, T.; Leigh, S.; Granby, P.; Haycox, A.; Turner, M.A.; et al. Foley catheterisation versus oral misoprostol for induction of labour in hypertensive women in India (INFORM): A multicentre, open-label, randomised controlled trial. Lancet 2017, 390, 669–680. [Google Scholar] [CrossRef] [Green Version]
- Little, S.E. Elective induction of labor: What is the impact? Obstet. Gynecol. Clin. N. Am. 2017, 44, 601–614. [Google Scholar] [CrossRef]
- Vogel, J.P.; Osoti, A.O.; Kelly, A.J.; Livio, S.; Norman, J.E.; Alfirevic, Z. Pharmacological and mechanical interventions for labour induction in outpatient settings. Cochrane Database Syst. Rev. 2017, 9, CD007701. [Google Scholar] [CrossRef] [Green Version]
- Magro-Malosso, E.R.; Saccone, G.; Chen, M.; Navathe, R.; Di Tommaso, M.; Berghella, V. Induction of labour for suspected macrosomia at term in non-diabetic women: A systematic review and meta-analysis of randomized controlled trials. BJOG 2017, 124, 414–421. [Google Scholar] [CrossRef]
- Ten Eikelder, M.L.; Oude Rengerink, K.; Jozwiak, M.; de Leeuw, J.W.; de Graaf, I.M.; van Pampus, M.G.; Holswilder, M.; Oudijk, M.A.; van Baaren, G.J.; Pernet, P.J.; et al. Induction of labour at term with oral misoprostol versus a Foley catheter (PROBAAT-II): A multicentre randomised controlled non-inferiority trial. Lancet 2016, 387, 1619–1628. [Google Scholar] [CrossRef]
- Connolly, K.A.; Kohari, K.S.; Rekawek, P.; Smilen, B.S.; Miller, M.R.; Moshier, E.; Factor, S.H.; Stone, J.L.; Bianco, A.T. A randomized trial of Foley balloon induction of labor trial in nulliparas (FIAT-N). Am. J. Obstet. Gynecol. 2016, 215, 392.e1-6. [Google Scholar] [CrossRef] [PubMed]
- Boulvain, M.; Irion, O.; Dowswell, T.; Thornton, J.G. Induction of labour at or near term for suspected fetal macrosomia. Cochrane Database Syst. Rev. 2016, 5, CD000938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Xue, J.; Peprah, M.K.; Wen, S.W.; Walker, M.; Gao, Y.; Tang, Y. A systematic review and network meta-analysis comparing the use of Foley catheters, misoprostol, and dinoprostone for cervical ripening in the induction of labour. BJOG 2016, 123, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Kondrad, E.; Liegl, S. Labor induction at term. Am. Fam. Physician 2016, 93, 266–268. [Google Scholar]
- Ten Eikelder, M.L.; Mast, K.; van der Velden, A.; Bloemenkamp, K.W.; Mol, B.W. Induction of labor using a Foley catheter or misoprostol: A systematic review and meta-analysis. Obstet. Gynecol. Surv. 2016, 71, 620–630. [Google Scholar] [CrossRef]
- Chen, W.; Xue, J.; Gaudet, L.; Walker, M.; Wen, S.W. Meta-analysis of Foley catheter plus misoprostol versus misoprostol alone for cervical ripening. Int. J. Gynaecol. Obstet. 2015, 129, 193–198. [Google Scholar] [CrossRef]
- McMaster, K.; Sanchez-Ramos, L.; Kaunitz, A.M. Evaluation of a Transcervical Foley catheter as a source of infection: A systematic review and meta-analysis. Obstet. Gynecol. 2015, 126, 539–551. [Google Scholar] [CrossRef]
- Greenberg, V.; Khalifeh, A. Intracervical Foley balloon catheter for cervical ripening and labor induction: A review. Semin. Perinatol. 2015, 39, 441–443. [Google Scholar] [CrossRef] [Green Version]
- Alfirevic, Z.; Aflaifel, N.; Weeks, A. Oral misoprostol for induction of labour. Cochrane Database Syst. Rev. 2014, 6, CD001338. [Google Scholar] [CrossRef]
- Jozwiak, M.; Oude Rengerink, K.; Ten Eikelder, M.L.; van Pampus, M.G.; Dijksterhuis, M.G.; de Graaf, I.M.; van der Post, J.A.; van der Salm, P.; Scheepers, H.C.; Schuitemaker, N.; et al. Foley catheter or prostaglandin E2 inserts for induction of labour at term: An open-label randomized controlled trial (PROBAAT-P trial) and systematic review of literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 170, 137–145. [Google Scholar] [CrossRef]
- Jozwiak, M.; Oude Rengerink, K.; Benthem, M.; van Beek, E.; Dijksterhuis, M.G.; de Graaf, I.M.; van Huizen, M.E.; Oudijk, M.A.; Papatsonis, D.N.; Perquin, D.A.; et al. Foley catheter versus vaginal prostaglandin E2 gel for induction of labour at term (PROBAAT trial): An open-label, randomised controlled trial. Lancet 2011, 378, 2095–2103. [Google Scholar] [CrossRef] [Green Version]
- Alfirevic, Z.; Kelly, A.J.; Dowswell, T. Intravenous oxytocin alone for cervical ripening and induction of labour. Cochrane Database Syst. Rev. 2009, 4, CD003246. [Google Scholar] [CrossRef] [PubMed]
- Boulvain, M.; Stan, C.; Irion, O. Membrane sweeping for induction of labour. Cochrane Database Syst. Rev. 2001, 2, CD000451. [Google Scholar]
- WHO Guidelines Approved by the Guidelines Review Committee. WHO Recommendations: Induction of Labour at or beyond Term; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Friedman, E.A.; Niswander, K.R.; Bayonet-Rivera, N.P.; Sachtleben, M.R. Relation of prelabor evaluation to inducibility and the course of labor. Obstet. Gynecol. 1966, 28, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Shirley, M. Dinoprostone vaginal insert: A review in cervical ripening. Drugs 2018, 78, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- West, H.M.; Jozwiak, M.; Dodd, J.M. Methods of term labour induction for women with a previous caesarean section. Cochrane Database Syst. Rev. 2017, 6, CD009792. [Google Scholar] [CrossRef]
- Ghosh, A.; Lattey, K.R.; Kelly, A.J. Nitric oxide donors for cervical ripening and induction of labour. Cochrane Database Syst. Rev. 2016, 12, CD006901. [Google Scholar] [CrossRef]
- Irani, R.A.; Foster, S. Overview of the mechanisms of induction of labor. Semin. Perinatol. 2015, 39, 426–429. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Gulmezoglu, A.M.; Pileggi, C. Vaginal misoprostol for cervical ripening and induction of labour. Cochrane Database Syst. Rev. 2010, 10, CD000941. [Google Scholar] [CrossRef]
- Embrey, M.P.; Mollison, B.G. The unfavourable cervix and induction of labour using a cervical balloon. J. Obstet. Gynaecol. Br. Commonw. 1967, 74, 44–48. [Google Scholar] [CrossRef]
- Leiberman, J.R.; Piura, B.; Chaim, W.; Cohen, A. The cervical balloon method for induction of labor. Acta. Obstet. Gynecol. Scand. 1977, 56, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Kashanian, M.; Akbarian, A.R.; Fekrat, M. Cervical ripening and induction of labor with intravaginal misoprostol and Foley catheter cervical traction. Int. J. Gynaecol. Obstet. 2006, 92, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.S.; Saltzman, D.H.; Roman, A.S.; Klauser, C.K.; Moshier, E.; Rebarber, A. Intravaginal misoprostol versus Foley catheter for labour induction: A meta-analysis. BJOG 2011, 118, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A. Balloon dilators for labor induction: A historical review. J. Med. Ethics Hist. Med. 2013, 6, 10. [Google Scholar]
- Sandberg, E.M.; Schepers, E.M.; Sitter, R.L.V.; Huisman, C.M.A.; Wijngaarden, W.J.V. Foley catheter for induction of labour filled with 30mL or 60mL: A randomized controlled trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 211, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Patabendige, M.; Jayawardane, A. Foley catheter for cervical priming in induction of labour at University Obstetrics Unit, Colombo, Sri Lanka: A clinical audit with a patient satisfaction survey. BMC Res. Notes 2017, 10, 155. [Google Scholar] [CrossRef] [Green Version]
- Battarbee, A.N.; Palatnik, A.; Peress, D.A.; Grobman, W.A. The association between cervical exam after ripening with foley balloon catheter and outcomes of nulliparous labor induction. Am. J. Perinatol. 2018, 35, 1001–1005. [Google Scholar]
- Leigh, S.; Granby, P.; Haycox, A.; Mundle, S.; Bracken, H.; Khedikar, V.; Mulik, J.; Faragher, B.; Easterling, T.; Turner, M.A.; et al. Foley catheter vs. oral misoprostol to induce labour among hypertensive women in India: A cost-consequence analysis alongside a clinical trial. BJOG 2018, 125, 1734–1742. [Google Scholar] [CrossRef]
- Ten Eikelder, M.L.; Neervoort, F.; Oude Rengerink, K.; van Baaren, G.J.; Jozwiak, M.; de Leeuw, J.W.; de Graaf, I.; van Pampus, M.G.; Franssen, M.; Oudijk, M.; et al. Induction of labour with a Foley catheter or oral misoprostol at term: The PROBAAT-II study, a multicentre randomised controlled trial. BMC Pregnancy Childbirth. 2013, 13, 67. [Google Scholar]
- el-Refaey, H.; Calder, L.; Wheatley, D.N.; Templeton, A. Cervical priming with prostaglandin E1 analogues, misoprostol and gemeprost. Lancet 1994, 343, 1207–1209. [Google Scholar] [CrossRef]
- McLaughlin, J.; Devoe, L.D. Current status of prostaglandins for cervical ripening. J. Reprod. Med. 2017, 62, 221–228. [Google Scholar] [PubMed]
- Ho, P.C. Development of medical termination of pregnancy: A review. BJOG 2017, 124, 1942–1947. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.; Kapp, N.; Dragoman, M.; de Souza, J.P. WHO recommendations for misoprostol use for obstetric and gynecologic indications. Int. J. Gynaecol. Obstet. 2013, 121, 186–189. [Google Scholar] [CrossRef]
- Tang, O.S.; Gemzell-Danielsson, K.; Ho, P.C. Misoprostol: Pharmacokinetic profiles, effects on the uterus and side-effects. Int. J. Gynaecol. Obstet. 2007, 99, S160–CS167. [Google Scholar] [CrossRef]
- Goldberg, A.B.; Greenberg, M.B.; Darney, P.D. Misoprostol and pregnancy. N. Engl. J. Med. 2001, 344, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.J.; Gülmezoglu, A.M.; Alfirevic, Z. Misoprostol for induction of labour: A systematic review. Br. J. Obstet. Gynaecol. 1999, 106, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Al-Ibraheemi, Z.; Brustman, L.; Bimson, B.E.; Porat, N.; Rosenn, B. Misoprostol with Foley bulb compared with misoprostol alone for cervical Ripening: A randomized controlled trial. Obstet. Gynecol. 2018, 131, 23–29. [Google Scholar] [CrossRef]
- Levine, L.D.; Downes, K.L.; Elovitz, M.A.; Parry, S.; Sammel, M.D.; Srinivas, S.K. Mechanical and pharmacologic methods of labor induction: A randomized controlled trial. Obstet. Gynecol. 2016, 128, 1357–1364. [Google Scholar] [CrossRef]
- Aduloju, O.P.; Akintayo, A.A.; Adanikin, A.I.; Ade-Ojo, I.P. Combined Foley’s catheter with vaginal misoprostol for pre-induction cervical ripening: A randomised controlled trial. Aust. N. Z. J. Obstet. Gynaecol. 2016, 56, 578–584. [Google Scholar] [CrossRef]
- Lanka, S.; Surapaneni, T.; Nirmalan, P.K. Concurrent use of Foley catheter and misoprostol for induction of labor: A randomized clinical trial of efficacy and safety. J. Obstet. Gynaecol. Res. 2014, 40, 1527–1533. [Google Scholar] [CrossRef]
- Carbone, J.F.; Tuuli, M.G.; Fogertey, P.J.; Roehl, K.A.; Macones, G.A. Combination of Foley bulb and vaginal misoprostol compared with vaginal misoprostol alone for cervical ripening and labor induction: A randomized controlled trial. Obstet. Gynecol. 2013, 121, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Ugwu, E.O.; Onah, H.E.; Obi, S.N.; Dim, C.C.; Okezie, O.A.; Chigbu, C.O.; Okoro, O.S. Effect of the Foley catheter and synchronous low dose misoprostol administration on cervical ripening: A randomised controlled trial. J. Obstet. Gynaecol. 2013, 33, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Huang, W.H.; Rumney, P.J.; Garite, T.J.; Nageotte, M.P. A prospective randomized controlled trial that compared misoprostol, Foley catheter, and combination misoprostol-Foley catheter for labor induction. Am. J. Obstet. Gynecol. 2003, 189, 1031–1035. [Google Scholar] [CrossRef] [Green Version]
- Rust, O.A.; Greybush, M.; Atlas, R.O.; Jones, K.J.; Balducci, J. Preinduction cervical ripening. A randomized trial of intravaginal misoprostol alone vs. a combination of transcervical Foley balloon and intravaginal misoprostol. J. Reprod. Med. 2001, 46, 899–904. [Google Scholar]
- Ashwini, M.M.; Kamatar, S.C.; Mann, D. Randomized control study of foley bulb and vaginal misoprostol compared with vaginal misoprostol alone in Induction of labour. Indian J. Public Health Res. Dev. 2018, 9, 96. [Google Scholar] [CrossRef]
- Gilani, S.; Ai, Q.T.; Hanif, M.; Mazhar, S.B.; Saeed, N. Concurrent use of intracervical foleys catheter plus vaginal misoprostol versus vaginal misoprostol alone for induction of labour. J. Soc. Obstet. Gynaecol. Pak. 2018, 8, 189–193. [Google Scholar]
- Adeniji, A.O.; Olayemi, O.; Odukogbe, A.A. Intravaginal misoprostol versus transcervical Foley catheter in pre-induction cervical ripening. Int. J. Gynaecol. Obstet. 2006, 92, 130–132. [Google Scholar] [CrossRef]
- Adeniji, A.O.; Olayemi, O.; Odukogbe, A.A.; Aimakhu, C.O.; Oladokun, A.; Akindele, F.O.; Adeniji, O.I.; Omigbodun, A.O.; Ilesanmi, A.O. Comparison of changes in pre-induction cervical factors’ scores following ripening with transcervical foley catheter and intravaginal misoprostol. Afr. J. Med. Med. Sci. 2005, 34, 377–382. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGee, T.M.; Gidaszewski, B.; Khajehei, M.; Tse, T.; Gibbs, E. Foley catheter silicone versus latex for term outpatient induction of labour: A randomised trial. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Battarbee, A.N.; Palatnik, A.; Peress, D.A.; Grobman, W.A. Association of early amniotomy after Foley balloon catheter ripening and duration of nulliparous labor induction. Obstet. Gynecol. 2016, 128, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.C.; Lee, W.L.; Wang, P.H. Is it safe to use pharmacological agents for induction of labor? J. Chin. Med. Assoc. 2017, 80, 123–124. [Google Scholar] [CrossRef] [Green Version]
- Kansu-Celik, H.; Gun-Eryılmaz, O.; Dogan, N.U.; Haktankaçmaz, S.; Cinar, M.; Yilmaz, S.S.; Gülerman, C. Prostaglandin E2 induction of labor and cervical ripening for term isolated oligohydramnios in pregnant women with Bishop score ≤ 5. J. Chin. Med. Assoc. 2017, 80, 169–172. [Google Scholar] [CrossRef] [Green Version]
- Cuerva, M.J.; Piñel, C.S.; Caceres, J.; Espinosa, J.A. Labor induction just after external cephalic version with epidural analgesia at term. Taiwan J. Obstet. Gynecol. 2017, 56, 366–367. [Google Scholar] [CrossRef]
- Walker, K.F.; Thornton, J.G. Delivery at term: When, how, and why. Clin. Perinatol. 2018, 45, 199–211. [Google Scholar] [CrossRef]
- Walker, K.; Thornton, J. Induction of labour at 37 weeks for suspected fetal macrosomia may reduce birth trauma. Evid.-Based Med. 2017, 22, 148. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Rand Process * | Deviations | Miss * | Measure | Selection * | OB * | OB without Selection |
|---|---|---|---|---|---|---|---|
| Chung et al. 2003 [54] | Low | Low | Low | Low | Con. | Con. | Low |
| Kashanian et al. 2006 [33] | High | High | High | Low | Con. | High | High |
| Carbone et al. 2013 [52] | Low | Low | Con. | Low | Con. | Con. | Con. |
| Ugwu et al. 2013 [53] | Low | Low | Con. | Low | Con. | Con. | Con. |
| Lanka et al. 2014 [51] | Low | Low | Low | Low | Con. | Con. | Low |
| Aduloju et al. 2016 [50] | Low | Low | Low | Low | Con. | Con. | Low |
| Levine et al. 2016 [49] | Low | Low | Low | Low | Con. | Con. | Low |
| Al-Ibraheemi et al. 2018 [48] | Low | Low | Low | Low | Con. | Con. | Low |
| Ashwini et al. 2018 [56] | High | High | High | Low | Con. | High | High |
| Gilani et al. 2018 [57] | Con. | Low | Low | Low | Con. | Con. | Con. |
| Study | Inclusion Criteria | IA in F + M | IA in M | Oxytocin Used | AROM | No. | |||
|---|---|---|---|---|---|---|---|---|---|
| PD (gw) | BS | F size (mL) | M Dose and Frequency | Dose and Frequency | F + M | M | |||
| Chung et al. 2003 [54] | >28 | <6 | 16 Fr. 30 mL, traction with tape to inner thigh, max 12 h | 25 μg q3h, until AC, max 6 doses | 25 μg q3h, until AC, max 6 doses | 3 h later at the end of procedure | At cervical dilation > 3 cm | 43 | 49 |
| Kashanian et al. 2006 * [33] | >28 | <5 | 16 Fr. traction with 500 mL NS | 25 μg q3h, max 6 doses | 25 μg q3h, max 6 doses | 12 h after if absence of AC | NA | 100 | 100 |
| Carbone et al. 2013 [52] | >24 | <6 | Size (NA), 60 mL under gentle traction to inner thigh | 25 μg q4h, until BS > 6, max 6 doses | 25 μg q4h, until BS > 6, max 6 doses | 4 h later at the end of procedure | Discretion | 57 | 61 |
| Ugwu et al. 2013 [53] | >37 | <6 | 16 Fr. 30 mL, traction with tape to inner thigh, max 12 h, repeated once if BS < 5 | 25 μg q4h, until BS > 6, max 6 doses | 25 μg q4h, until BS > 6, max 6 doses | 4 h after last M later at the end of procedure or once reaching favorable BS | NA | 50 | 45 |
| Lanka et al. 2014 [51] | >28 | <4 | 16 Fr. 30 mL, traction with tape to inner thigh, max 12 h | 25 μg q4h, until BS > 6, max 8 doses | 25 μg q4h, until BS > 6, max 8 doses | AM | AM before oxytocin was added | 63 | 63 |
| Aduloju et al. 2016 [50] | at term | <6 | 16 Fr. 30 mL, traction with tape to inner thigh, max 12 h, repeated once more if BS < 6 | 25 μg q6h, until BS > 6, max 4 doses | 25 μg q6h, until BS >6, max 4 doses | 6 h after last M later at the end of procedure or once reaching favorable BS | At cervical dilation > 4 cm | 70 | 70 |
| Levine et al. 2016 [49] | >37 | <6 | 18 Fr. 60 mL, traction with tape to inner thigh, max 12 h | 25 μg q3h, max 6 doses | 25 μg q3h, max 6 doses | Started if additional cervical ripening was not indicated or at the end of procedure | Discretion (after cervix > 4 cm) | 123 | 120 |
| Al-Ibraheemi et al. 2018 [48] | >37 | <6 | Size (NA), 60 mL under gentle traction to inner thigh | 25 μg q6h, until BS >6, max 8 doses | 25 μg q6h, until BS >6, max 8 doses | Started if AC after last M | Discretion | 100 | 100 |
| Ashwini et al. 2018 * [56] | >28 | <6 | 16 Fr. 50 mL under gentle traction to inner thigh | 25 μg q4h, until cervix favorable, max 6 doses | 25 μg q4h, until cervix favorable, max 6 doses | NA | NA | 50 | 50 |
| Gilani et al. 2018 [57] | >38 | NA | 16 Fr. 60 mL, traction with tape to inner thigh, max 12 h | 50 μg q6h, until BS > 6, max 3 doses | 50 μg q6h, until BS > 6, max 3 doses | NA | NA | 48 | 48 |
| Outcomes | Studies | Egger’s Test P Value | Trim and Fill, No. of Missing Studies | Calculated RR | Adjusted RR |
|---|---|---|---|---|---|
| Time to delivery | 7 | 0.558 | 4 | Random −2.705 (−4.330 to −1.081) | −4.136 (−5.845 to −2.428) |
| Sample size < 200 | 5 | 0.302 | 0 | N/A | N/A |
| Cesarean Section | 8 | 0.563 | 1 | Fixed 0.930 (0.775 to 1.112) | 0.910 (0.775 to 1.117) |
| Chorioamnionitis | 4 | 0.825 | 0 | NA | NA |
| Uterine tachysystole | 4 | 0.414 | 0 | NA | N/A |
| w/FHR change | 3 | 0.124 | 0 | NA | NA |
| Meconium Stain | 6 | 0.881 | 1 | Fixed 0.512 (0.332 to 0.789) | 0.418 (0.282 to 0.621) |
| NICU | 7 | 0.567 | 0 | NA | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.H.; Huang, B.-S.; Cheng, M.; Yeh, C.-C.; Lin, I.-C.; Horng, H.-C.; Huang, H.-Y.; Lee, W.-L.; Wang, P.-H. Intracervical Foley Catheter Plus Intravaginal Misoprostol vs Intravaginal Misoprostol Alone for Cervical Ripening: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1825. https://doi.org/10.3390/ijerph17061825
Lee HH, Huang B-S, Cheng M, Yeh C-C, Lin I-C, Horng H-C, Huang H-Y, Lee W-L, Wang P-H. Intracervical Foley Catheter Plus Intravaginal Misoprostol vs Intravaginal Misoprostol Alone for Cervical Ripening: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(6):1825. https://doi.org/10.3390/ijerph17061825
Chicago/Turabian StyleLee, Howard Hao, Ben-Shian Huang, Min Cheng, Chang-Ching Yeh, I-Chia Lin, Huann-Cheng Horng, Hsin-Yi Huang, Wen-Ling Lee, and Peng-Hui Wang. 2020. "Intracervical Foley Catheter Plus Intravaginal Misoprostol vs Intravaginal Misoprostol Alone for Cervical Ripening: A Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 6: 1825. https://doi.org/10.3390/ijerph17061825