Association between Uranium Exposure and Thyroid Health: A National Health and Nutrition Examination Survey Analysis and Ecological Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. NHANES Analysis
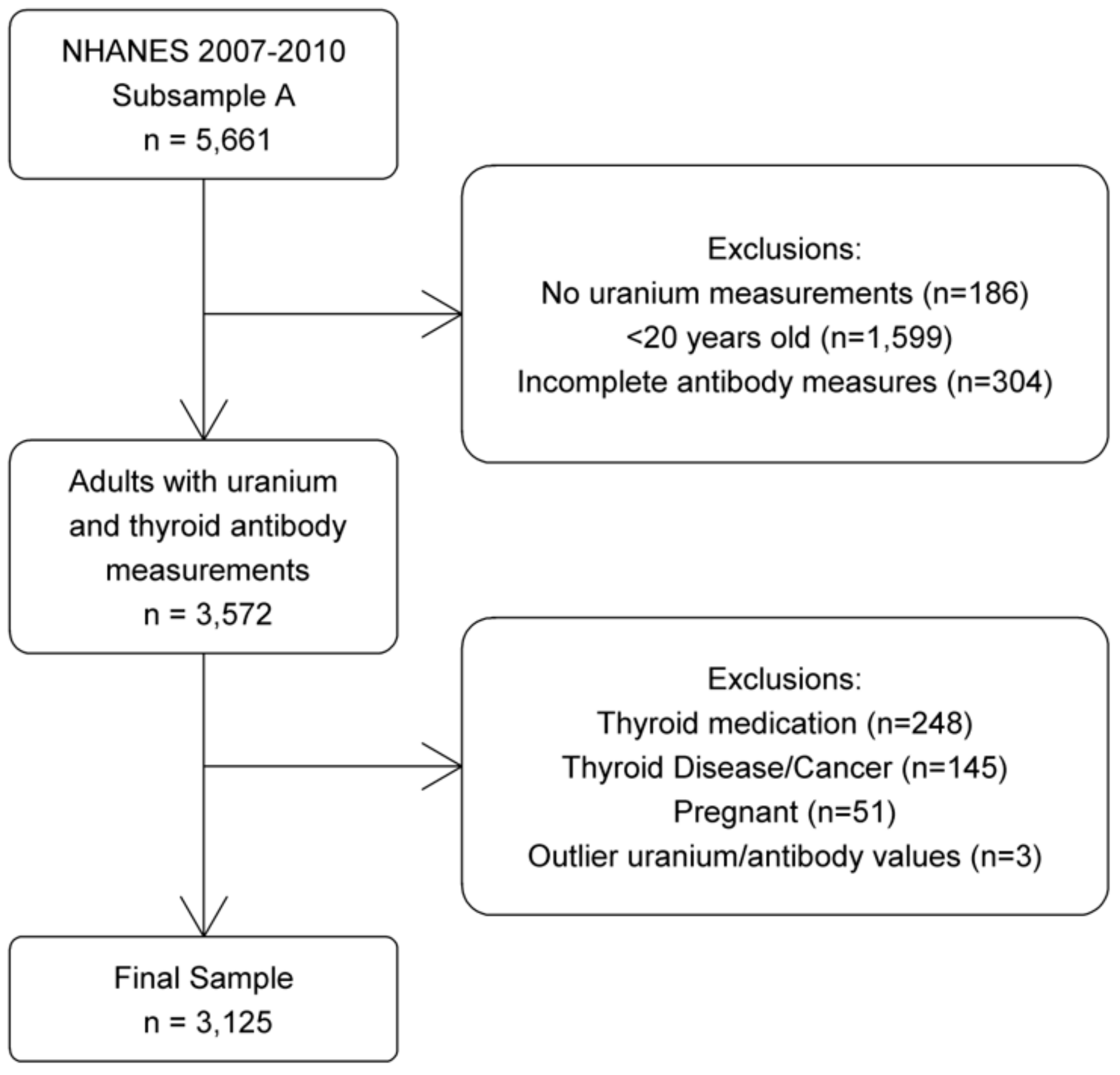
2.1.1. Data Source and Study Population
2.1.2. Outcomes and Covariates
2.1.3. Statistical Analysis
2.2. Ecological Study
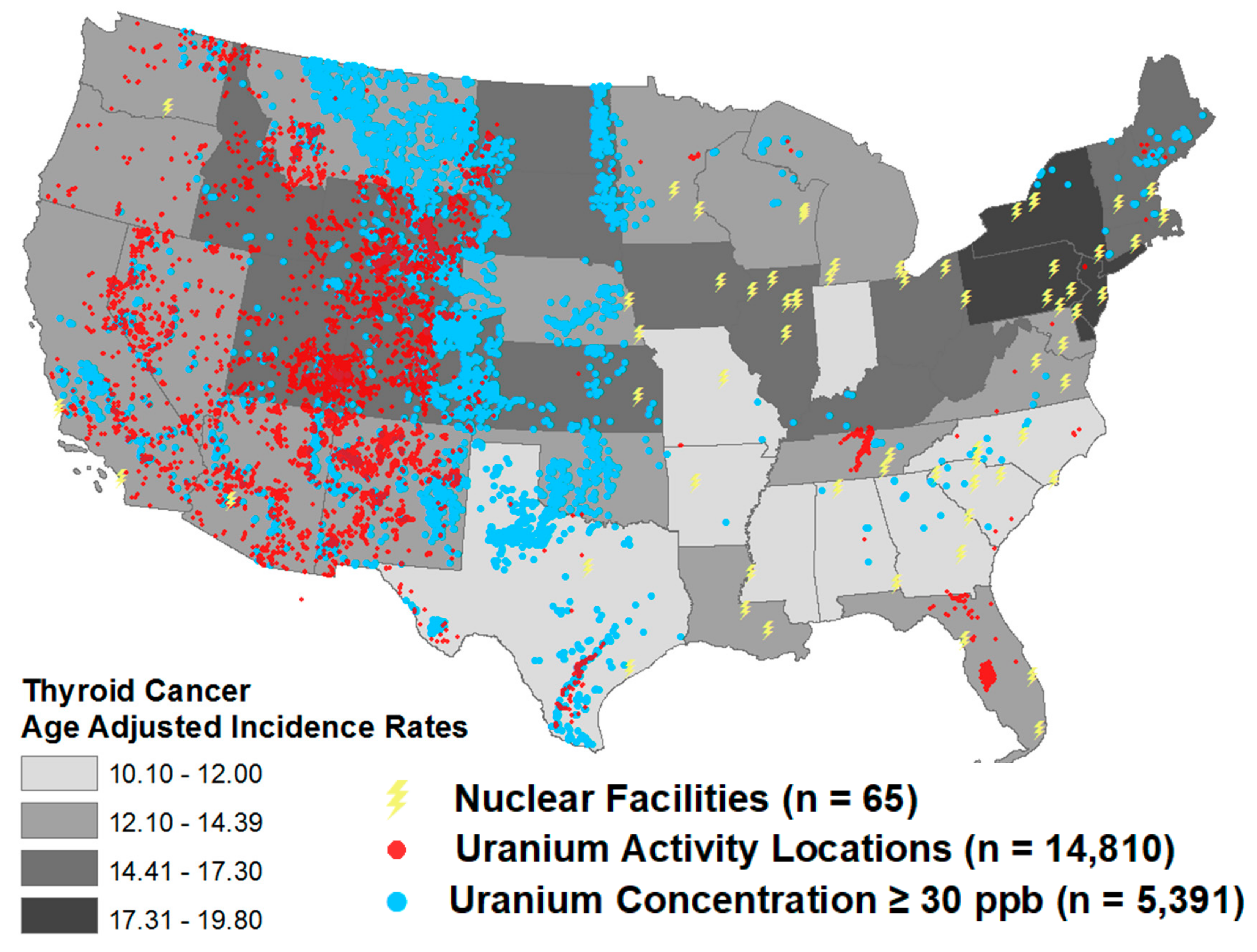
2.2.1. Thyroid Cancer Incidence
2.2.2. Uranium Measurements
2.2.3. Statistical Analysis
3. Results
3.1. NHANES Analysis
3.2. Ecological Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Albi, E.; Cataldi, S.; Lazzarini, A.; Codini, M.; Beccari, T.; Ambesi-Impiombato, F.S.; Curcio, F. Radiation and Thyroid Cancer. Int. J. Mol. Sci. 2017, 18, 911. [Google Scholar] [CrossRef] [PubMed]
- Nagataki, S.; Hirayu, H.; Izumi, M.; Inoue, S.; Okajima, S.; Shimaoka, K. High prevalence of thyroid nodule in area of radioactive fallout. Lancet 1989, 2, 385–386. [Google Scholar] [CrossRef]
- Kazakov, V.S.; Demidchik, E.P.; Astakhova, L.N. Thyroid cancer after Chernobyl. Nature 1992, 359, 21. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Yamashita, S.; Masyakin, V.B.; Panasyuk, G.D.; Nagataki, S. 15 years after Chernobyl: New evidence of thyroid cancer. Lancet 2001, 358, 1965–1966. [Google Scholar] [CrossRef]
- Takahashi, T.; Schoemaker, M.J.; Trott, K.R.; Simon, S.L.; Fujimori, K.; Nakashima, N.; Fukao, A.; Saito, H. The relationship of thyroid cancer with radiation exposure from nuclear weapon testing in the Marshall Islands. J. Epidemiol. 2003, 13, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Imaizumi, M.; Usa, T.; Tominaga, T.; Neriishi, K.; Akahoshi, M.; Nakashima, E.; Ashizawa, K.; Hida, A.; Soda, M.; Fujiwara, S.; et al. Radiation dose-response relationships for thyroid nodules and autoimmune thyroid diseases in Hiroshima and Nagasaki atomic bomb survivors 55–58 years after radiation exposure. JAMA 2006, 295, 1011–1022. [Google Scholar] [CrossRef] [Green Version]
- Shore, R.E.; Hildreth, N.; Dvoretsky, P.; Andresen, E.; Moseson, M.; Pasternack, B. Thyroid cancer among persons given X-ray treatment in infancy for an enlarged thymus gland. Am. J. Epidemiol. 1993, 137, 1068–1080. [Google Scholar] [CrossRef]
- Schneider, A.B.; Ron, E.; Lubin, J.; Stovall, M.; Gierlowski, T.C. Dose-response relationships for radiation-induced thyroid cancer and thyroid nodules: Evidence for the prolonged effects of radiation on the thyroid. J. Clin. Endocrinol. Metab. 1993, 77, 362–369. [Google Scholar]
- Shore, R.E.; Hildreth, N.; Dvoretsky, P.; Pasternack, B.; Andresen, E. Benign thyroid adenomas among persons X-irradiated in infancy for enlarged thymus glands. Radiat. Res. 1993, 134, 217–223. [Google Scholar] [CrossRef]
- Ron, E.; Lubin, J.H.; Shore, R.E.; Mabuchi, K.; Modan, B.; Pottern, L.M.; Schneider, A.B.; Tucker, M.A.; Boice, J.D., Jr. Thyroid cancer after exposure to external radiation: A pooled analysis of seven studies. Radiat. Res. 1995, 141, 259–277. [Google Scholar] [CrossRef]
- Taylor, D.M.; Taylor, S.K. Environmental uranium and human health. Rev. Environ. Health 1997, 12, 147–157. [Google Scholar] [CrossRef] [PubMed]
- UNSCEAR 2016 Report; Sources, Effects and Risks of Ionizing Radiation. Available online: https://www.unscear.org/unscear/en/publications/2016.html (accessed on 3 January 2020).
- Keith, S.; Faroon, O.; Roney, N.; Scinicariello, F.; Wilbur, S.; Ingerman, L.; Llados, F.; Plewak, D.; Wohlers, D.; Diamond, G. Toxicological Profile for Uranium; ATSDR: Atlanta, GA, USA, 2013. [Google Scholar]
- Nolan, J.; Weber, K.A. Natural uranium contamination in major US aquifers linked to nitrate. Environ. Sci. Technol. Lett. 2015, 2, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Jurgens, B.C.; Fram, M.S.; Belitz, K.; Burow, K.R.; Landon, M.K. Effects of groundwater development on uranium: Central Valley, California, USA. Ground Water 2010, 48, 913–928. [Google Scholar] [CrossRef] [Green Version]
- Malandrino, P.; Russo, M.; Ronchi, A.; Minoia, C.; Cataldo, D.; Regalbuto, C.; Giordano, C.; Attard, M.; Squatrito, S.; Trimarchi, F.; et al. Increased thyroid cancer incidence in a basaltic volcanic area is associated with non-anthropogenic pollution and biocontamination. Endocrine 2016, 53, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Ting, B.G.; Paschal, D.C.; Jarrett, J.M.; Pirkle, J.L.; Jackson, R.J.; Sampson, E.J.; Miller, D.T.; Caudill, S.P. Uranium and thorium in urine of United States residents: Reference range concentrations. Environ. Res. 1999, 81, 45–51. [Google Scholar] [CrossRef]
- Pellegriti, G.; De Vathaire, F.; Scollo, C.; Attard, M.; Giordano, C.; Arena, S.; Dardanoni, G.; Frasca, F.; Malandrino, P.; Vermiglio, F.; et al. Papillary thyroid cancer incidence in the volcanic area of Sicily. J. Natl. Cancer Inst. 2009, 101, 1575–1583. [Google Scholar] [CrossRef]
- Kung, T.M.; Ng, W.L.; Gibson, J.B. Volcanoes and carcinoma of the thyroid: A possible association. Arch. Environ. Health 1981, 36, 265–267. [Google Scholar] [CrossRef]
- Malenchenko, A.F.; Barkun, N.A.; Guseva, G.F. Effect of uranium on the induction and course of experimental autoimmune orchitis and thyroiditis. J. Hyg. Epidemiol. Microbiol. Immunol. 1978, 22, 268–277. [Google Scholar]
- Banning, A.; Benfer, M. Drinking Water Uranium and Potential Health Effects in the German Federal State of Bavaria. Int. J. Environ. Res. Public Health 2017, 14, 927. [Google Scholar] [CrossRef]
- Rapoport, B.; McLachlan, S.M. Reflections on Thyroid Autoimmunity: A Personal Overview from the Past into the Future. Horm. Metab. Res. 2018, 50, 840–852. [Google Scholar] [CrossRef] [Green Version]
- Cogni, G.; Chiovato, L. An overview of the pathogenesis of thyroid autoimmunity. Hormones (Athens) 2013, 12, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Lim, D.J.; Baek, K.H.; Lee, J.M.; Kim, M.K.; Kwon, H.S.; Song, K.H.; Kang, M.I.; Cha, B.Y.; Lee, K.W.; et al. Thyroglobulin antibody is associated with increased cancer risk in thyroid nodules. Thyroid 2010, 20, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Zhou, Q.; Xu, Y.; Yuan, S.L.; Liu, Q.A. Positive thyroid antibodies and risk of thyroid cancer: A systematic review and meta-analysis. Mol. Clin. Oncol. 2019, 11, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Yorita Christensen, K.L. Metals in blood and urine, and thyroid function among adults in the United States 2007–2008. Int. J. Hyg. Environ. Health 2013, 216, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Turyk, M.E.; Anderson, H.A.; Persky, V.W. Relationships of thyroid hormones with polychlorinated biphenyls, dioxins, furans, and DDE in adults. Environ. Health Perspect. 2007, 115, 1197–1203. [Google Scholar] [CrossRef] [Green Version]
- National Health and Nutrition Examination Survey. Available online: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx (accessed on 17 December 2019).
- United States Cancer Statistics (USCS). Available online: https://www.cdc.gov/cancer/uscs/dataviz/index.htm (accessed on 17 December 2019).
- EPA. Radiation Protection. Available online: https://www.epa.gov/radiation/uranium-mines-and-mills-location-database-0 (accessed on 17 December 2019).
- National Uranium Resource Evaluation (NURE) Hydrogeochemical and Stream Sediment Reconnaissance Data. Available online: https://mrdata.usgs.gov/metadata/nurehssr.html (accessed on 17 December 2019).
- Water Quality Association. Uranium Fact Sheet. Available online: https://www.wqa.org/Portals/0/Technical/Technical%20Fact%20Sheets/2014_Uranium.pdf (accessed on 17 December 2019).
- Grani, G.; Calvanese, A.; Carbotta, G.; D’Alessandri, M.; Nesca, A.; Bianchini, M.; Del Sordo, M.; Vitale, M.; Fumarola, A. Thyroid autoimmunity and risk of malignancy in thyroid nodules submitted to fine-needle aspiration cytology. Head Neck 2015, 37, 260–264. [Google Scholar] [CrossRef]
- Vasileiadis, I.; Boutzios, G.; Charitoudis, G.; Koukoulioti, E.; Karatzas, T. Thyroglobulin antibodies could be a potential predictive marker for papillary thyroid carcinoma. Ann. Surg. Oncol. 2014, 21, 2725–2732. [Google Scholar] [CrossRef]
- Anke, M.; Seeber, O.; Müller, R.; Schäfer, U.; Zerull, J. Uranium transfer in the food chain from soil to plants, animals and man. Chem. Erde 2009, 69, 75–90. [Google Scholar] [CrossRef]
- Neves, M.; Abreu, M.; Figueiredo, V. Uranium in vegetable foodstuffs: Should residents near the Cunha Baixa uranium mine site (Central Northern Portugal) be concerned? Environ. Geochem. Health 2012, 34, 181–189. [Google Scholar] [CrossRef]
- Levin, R.J.; De Simone, N.F.; Slotkin, J.F.; Henson, B.L. Incidence of thyroid cancer surrounding three mile island nuclear facility: The 30-year follow-up. Laryngoscope 2013, 123, 2064–2071. [Google Scholar] [CrossRef]
- Bann, D.V.; Goyal, N.; Camacho, F.; Goldenberg, D. Increasing incidence of thyroid cancer in the Commonwealth of Pennsylvania. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 1149–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, J.J. Geographic variation in US thyroid cancer incidence and a cluster near nuclear reactors in New Jersey, New York, and Pennsylvania. Int. J. Health Serv. 2009, 39, 643–661. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Bang, Y.; Lee, W.J. Living near nuclear power plants and thyroid cancer risk: A systematic review and meta-analysis. Environ. Int. 2016, 87, 42–48. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | ||
|---|---|---|
| Demographics | ||
| Mean (SE) | ||
| Age (years) | 45.7 (0.5) | |
| Body Mass Index (kg/m2) | 28.4 (0.1) | |
| Gender | n (%) | |
| Male | 1691 (53.8) | |
| Female | 1434 (46.2) | |
| Race/Ethnicity | ||
| Non-Hispanic White | 1443 (68.5) | |
| Non-Hispanic Black | 611 (11.3) | |
| Hispanic/Other | 1071 (20.2) | |
| Thyroid Antibodies | ||
| TgAb | ||
| <4.0 IU/mL | 2942 (93.8) | |
| ≥4.0 IU/mL | 183 (6.2) | |
| Anti-TPO | ||
| <9.0 IU/mL | 2839 (89.9) | |
| ≥9.0 IU/mL | 286 (10.1) | |
| Median (IQR) | ||
| TgAb (IU/mL) | 0.60 (0.60–0.60) | |
| Anti-TPO (IU/mL) | 0.62 (0.31–1.54) | |
| Uranium | Median (IQR) | % below LOD |
| Urinary Uranium (ug/g creatinine) * | 0.006 (0.003–0.011) | 9.1% |
| Model | Ln TgAb (IU/mL) | Ln Anti-TPO (IU/mL) | ||
|---|---|---|---|---|
| Βadj * (95% CI) | p-Value | Βadj * (95% CI) | p-Value | |
| Continuous | ||||
| Ln Uranium (ug/g creatinine) | 0.035 (−0.006; 0.077) | 0.0947 | 0.035 (−0.060; 0.130) | 0.4569 |
| Quartile (ug/g creatinine) | ||||
| <0.0034 | Ref | 0.0105 | Ref | 0.7552 |
| 0.0034–0.0061 | 0.110 (0.021; 0.198) | 0.117 (−0.110; 0.343) | ||
| 0.0062–0.0112 | 0.114 (0.010; 0.218) | 0.031 (−0.236; 0.298) | ||
| ≥0.0113 | 0.077 (−0.017;0.171) | 0.046 (−0.188;0.281) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Gerwen, M.; Alpert, N.; Lieberman-Cribbin, W.; Cooke, P.; Ziadkhanpour, K.; Liu, B.; Genden, E. Association between Uranium Exposure and Thyroid Health: A National Health and Nutrition Examination Survey Analysis and Ecological Study. Int. J. Environ. Res. Public Health 2020, 17, 712. https://doi.org/10.3390/ijerph17030712
van Gerwen M, Alpert N, Lieberman-Cribbin W, Cooke P, Ziadkhanpour K, Liu B, Genden E. Association between Uranium Exposure and Thyroid Health: A National Health and Nutrition Examination Survey Analysis and Ecological Study. International Journal of Environmental Research and Public Health. 2020; 17(3):712. https://doi.org/10.3390/ijerph17030712
Chicago/Turabian Stylevan Gerwen, Maaike, Naomi Alpert, Wil Lieberman-Cribbin, Peter Cooke, Kimia Ziadkhanpour, Bian Liu, and Eric Genden. 2020. "Association between Uranium Exposure and Thyroid Health: A National Health and Nutrition Examination Survey Analysis and Ecological Study" International Journal of Environmental Research and Public Health 17, no. 3: 712. https://doi.org/10.3390/ijerph17030712