Is Post-Reprocessing Microbiological Surveillance of Duodenoscopes Effective in Reducing the Potential Risk in Transmitting Pathogens?

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Procedure
2.3. Modality of Sampling and Microbiological Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Associazione Nazionale Operatori Tecnologie Endoscopiche (ANOTE). Linee Guida Pulizia e Disinfezione in Endoscopia. 2011. Available online: https://www.anoteanigea.it/linee-guida-public/linee-guida-pulizia-e-disinfezione-in-endoscopia-update-2011/ (accessed on 2 December 2019).
- The Lancet Gastroenterology Hepatology. Scoping the problem: Endoscopy-associated infections. Lancet Gastroenterol. Hepatol. 2018, 3, 445. [Google Scholar] [CrossRef]
- Cristina, M.L.; Valeriani, F.; Casini, B.; Agodi, A.; D’Errico, M.M.; Gianfranceschi, G.; Laganà, P.; Liguori, G.; Liguori, R.; Mucci, N.; et al. Procedures in endoscope reprocessing and monitoring: An Italian survey. Ann. Ig. 2018, 30, 45–63. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.J. Managing and preventing exposure events from inappropriately reprocessed endoscopes. Infect. Control Hosp. Epidemiol. 2012, 33, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Valeriani, F.; Agodi, A.; Casini, B.; Cristina, M.L.; D’Errico, M.M.; Gianfranceschi, G.; Liguori, G.; Liguori, R.; Mucci, N.; Mura, I.; et al. Potential testing of reprocessing procedures by real-time polymerase chain reaction: A multicenter study of colonoscopy devices. Am. J. Infect. Control 2018, 46, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristina, M.L.; Spagnolo, A.M.; Orlando, P.; Perdelli, F. The role of the environment in the spread of emerging pathogens in at-risk hospital wards. Rev. Med. Microbiol. 2013, 24, 104–112. [Google Scholar] [CrossRef]
- ASGE Quality Assurance in Endoscopy Committee; Calderwood, A.H.; Day, L.W.; Muthusamy, V.R.; Collins, J.; Hambrick, R.D., 3rd; Brock, A.S.; Guda, N.M.; Buscaglia, J.M.; Petersen, B.T.; et al. ASGE guideline for infection control during GI endoscopy. Gastrointest. Endosc. 2018, 87, 1167–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, L.; Hunter, J.C.; Arwady, M.A.; Tsai, V.; Stein, L.; Gribogiannis, M.; Frias, M.; Guh, A.Y.; Laufer, A.S.; Black, S.; et al. New Delhi Metallo-β-Lactamase Producing Carbapenem-Resistant Escherichia coli Associated with Exposure to Duodenoscopes. JAMA 2014, 312, 1447–1455. [Google Scholar] [CrossRef] [Green Version]
- CDC. Interim Protocol for Healthcare Facilities Regarding Surveillance for Bacterial Contamination of Duodenoscopes after Reprocessing; CDC: Atlanta, GA, USA, 2015.
- Muscarella, L.F. Risk of transmission of carbapenem-resistant Enterobacteriaceae and related “superbugs” during gastrointestinal endoscopy. World J. Gastrointest. Endosc. 2014, 6, 457–474. [Google Scholar] [CrossRef]
- Rahman, M.R.; Perisetti, A.; Coman, R.; Bansal, P.; Chhabra, R.; Goyal, H. Duodenoscope-Associated Infections: Update on an Emerging Problem. Dig. Dis. Sci. 2019, 64, 1409–1418. [Google Scholar] [CrossRef]
- CDC. Interim Sampling Method for the Duodenoscope—Distal End and Instrument Channel; CDC: Atlanta, GA, USA, 2015.
- CDC. Interim Culture Method for the Duodenoscope—Distal End and Instrument Channel; CDC: Atlanta, GA, USA, 2015.
- CDC. Duodenoscope Surveillance Sampling & Culturing. Reducing the Risks of Infection. 2018. Available online: https://www.fda.gov/media/111081/download (accessed on 2 December 2019).
- American Society for Gastrointestinal Endoscopy. Multi-society guideline for reprocessing flexible gastrointestinal endoscopes. Gastrointest. Endosc. 2003, 58, 1–8. [Google Scholar] [CrossRef]
- Alvarado, C.J.; Reichelderfer, M. APIC guideline for infection prevention and control in flexible endoscopy. Association for Professionals in Infection Control. Am. J. Infect. Control 2000, 28, 138–155. [Google Scholar] [CrossRef] [PubMed]
- Beilenhoff, U.; Neumann, C.S.; Biering, H.; Blum, R.; Schmidt, V.; Rey, J.F. ESGE/ESGENA guideline for process validation and routine testing for reprocessing endoscopes in washer-disinfectors, according to the European Standard prEN ISO 15883 parts 1, 4 and 5. Endoscopy 2007, 39, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Systchenko, R.; Marchetti, B.; Canard, J.N.; Palazzo, L.; Ponchon, T.; Rey, J.F.; Sautereau, D.; French Society of Digestive Endoscopy. Guidelines of the French Society of Digestive Endoscopy: Recommendations for setting up cleaning and disinfection procedures in gastrointestinal endoscopy. Endoscopy 2000, 32, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care. Health Technical Memorandum 01–06: Decontamination of Flexible Endoscopes: Part E—Testing Methods; Department of Health and Social Care: London, UK, 2016.
- ARS Toscana. Il Reprocessing in Endoscopia Digestiva: Criticità e Strumenti per la Sicurezza del Percorso. Available online: https://www.ars.toscana.it/files/pubblicazioni/Volumi/2013/doc_ars_70_2013_ok.pdf (accessed on 2 December 2019).
- McCafferty, C.E.; Aghajani, M.J.; Abi-Hanna, D.; Gosbell, I.B.; Jensen, S.O. An update on gastrointestinal endoscopy-associated infections and their contributing factors. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaker, A.M.; Kim, S.; Sedarat, A.; Watson, R.R.; Muthusamy, V.R. Inspection of endoscope instrument channels after reprocessing using a prototype borescope. Gastrointest. Endosc. 2018, 88, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Rauwers, A.W.; Voor, A.F.; Buijs, J.G.; De Groot, W.; Hansen, B.E.; Bruno, M.J.; Vos, M.C. High prevalence rate of digestive tract bacteria in duodenoscopes: A nationwide study. Gut 2018, 67, 1637–1645. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, M.M.; de Oliveira, A.C. Analysis of the air/water channels of gastrointestinal endoscopies as a risk factor for the transmission of microorganisms among patients. Am. J. Infect. Control 2012, 40, 913–916. [Google Scholar] [CrossRef]
- Sticchi, C.; Alberti, M.; Artioli, S.; Assensi, M.; Baldelli, I.; Battistini, A.; Boni, S.; Cassola, G.; Castagnola, E.; Cattaneo, M.; et al. Regional point prevalence study of healthcare-associated infections and antimicrobial use in acute care hospitals in Liguria, Italy. J. Hosp. Infect. 2018, 99, 8–16. [Google Scholar] [CrossRef]
- Cristina, M.L.; Alicino, C.; Sartini, M.; Faccio, V.; Spagnolo, A.M.; Bono, V.D.; Cassola, G.; De Mite, A.M.; Crisalli, M.P.; Ottria, G.; et al. Epidemiology, management, and outcome of carbapenem-resistant Klebsiella pneumoniae bloodstream infections in hospitals within the same endemic metropolitan area. J. Infect. Public Health 2018, 11, 171–177. [Google Scholar] [CrossRef]
- Cristina, M.L.; Sartini, M.; Ottria, G.; Schinca, E.; Cenderello, N.; Crisalli, M.P.; Fabbri, P.; Lo Pinto, G.; Usiglio, D.; Spagnolo, A.M. Epidemiology and biomolecular characterization of carbapenem-resistant Klebsiella pneumoniae in an Italian hospital. J. Prev. Med. Hyg. 2016, 57, E149–E156. [Google Scholar]
- Spagnolo, A.M.; Orlando, P.; Panatto, D.; Perdelli, F.; Cristina, M.L. An overview of carbapenem-resistant Klebsiella pneumoniae: Epidemiology and control measures. Rev. Med. Microbiol. 2014, 25, 7–14. [Google Scholar] [CrossRef]
- Cristina, M.L.; Spagnolo, A.M.; Cenderello, N.; Fabbri, P.; Sartini, M.; Ottria, G.; Orlando, P. Multidrug-resistant Acinetobacter baumannii outbreak: An investigation of the possible routes of transmission. Public Health 2013, 127, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Cristina, M.L.; Spagnolo, A.M.; Ottria, G.; Sartini, M.; Orlando, P.; Perdelli, F.; Galliera Hospital Group. Spread of multidrug carbapenem-resistant Acinetobacter baumannii in different wards of an Italian hospital. Am. J. Infect. Control 2011, 39, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, A.M.; Orlando, P.; Panatto, D.; Amicizia, D.; Perdelli, F.; Cristina, M.L. Staphylococcus aureus with reduced susceptibility to vancomycin in healthcare settings. J. Prev. Med. Hyg. 2014, 55, 137–144. [Google Scholar] [PubMed]
- Perdelli, F.; Dallera, M.; Cristina, M.L.; Sartini, M.; Ottria, G.; Spagnolo, A.M.; Orlando, P. A new microbiological problem in intensive care units: Environmental contamination by MRSA with reduced susceptibility to glycopeptides. Int. J. Hyg. Environ. Health 2008, 211, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Gastmeier, P.; Vonberg, R.P. Klebsiella spp. in endoscopy-associated infections: We may only be seeing the tip of the iceberg. Infection 2014, 42, 15–21. [Google Scholar] [CrossRef]
- Aumeran, C.; Poincloux, L.; Souweine, B.; Robin, F.; Laurichesse, H.; Baud, O.; Bommelaer, G.; Traoré, O. Multidrug-resistant Klebsiella pneumoniae outbreak after endoscopic retrograde cholangiopancreatography. Endoscopy 2010, 42, 895–899. [Google Scholar] [CrossRef]
- Bajolet, O.; Ciocan, D.; Vallet, C.; de Champs, C.; Vernet-Garnier, V.; Guillard, T.; Brasme, L.; Thiefin, G.; Cadiot, G.; Bureau-Chalot, F. Gastroscopy-associated transmission of extended-spectrum beta-lactamase-producing Pseudomonas aeruginosa. J. Hosp. Infect. 2013, 83, 341–343. [Google Scholar] [CrossRef]
- Chiu, K.W.; Lu, L.S.; Chiou, S.S. High-level disinfection of gastrointestinal endoscope reprocessing. World J. Exp. Med. 2015, 5, 33–39. [Google Scholar] [CrossRef]
- Orlando, P.; Cristina, M.L.; Dallera, M.; Ottria, G.; Vitale, A.; Badolati, G. Surface disinfection: Evaluation of the efficacy of a nebulization system spraying hydrogen peroxide. J. Prev. Med. Hyg. 2008, 49, 116–119. [Google Scholar]



{kind=link}
{kind=link}
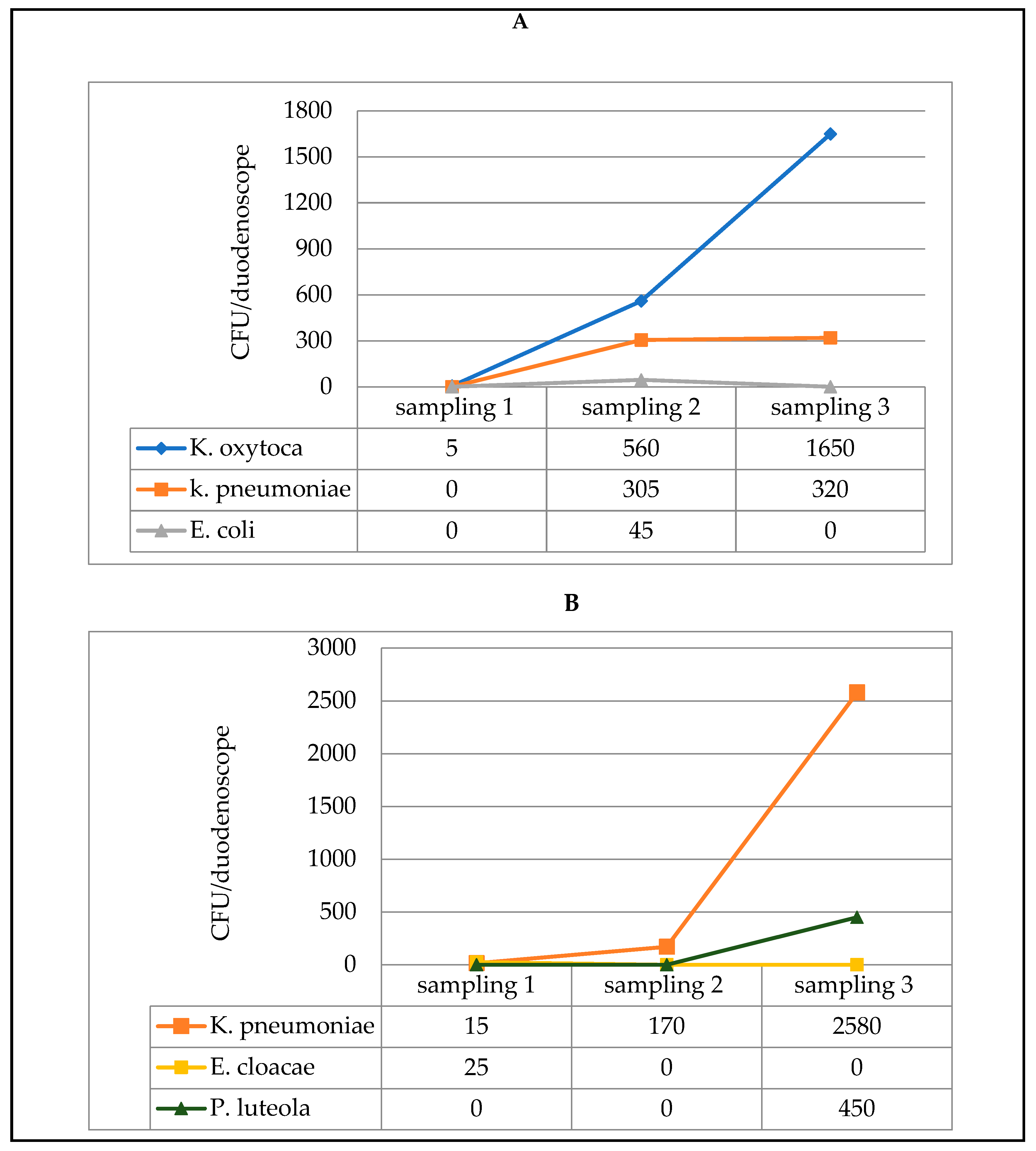
| Distal End | Instrument Channel | |
|---|---|---|
| Micro-Organism | Min-Max CFU/Duodenoscope (% Positivity) | Min-Max CFU/Duodenoscope (% Positivity) |
| P. aeruginosa | 10–2500 (41.67) | 15–2500 (41.67) |
| K. pneumoniae | 120–650 (41.67) | 15–2580 (50.00) |
| K. oxytoca | 5–1650 (25.00) | - |
| Enterobacter spp | - | 25–50 (16.67) |
| S. maltophilia | 20–25 (16.67) | 20–120 (16.67) |
| A. baumannii | 2600 (16.67) | 360–2600 (16.67) |
| E. coli | 45 (8.33) | - |
| C. freundii | 125 (8.33) | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristina, M.L.; Sartini, M.; Schinca, E.; Ottria, G.; Dupont, C.; Bova, P.; Coccia, G.; Casini, B.; Spagnolo, A.M. Is Post-Reprocessing Microbiological Surveillance of Duodenoscopes Effective in Reducing the Potential Risk in Transmitting Pathogens? Int. J. Environ. Res. Public Health 2020, 17, 140. https://doi.org/10.3390/ijerph17010140
Cristina ML, Sartini M, Schinca E, Ottria G, Dupont C, Bova P, Coccia G, Casini B, Spagnolo AM. Is Post-Reprocessing Microbiological Surveillance of Duodenoscopes Effective in Reducing the Potential Risk in Transmitting Pathogens? International Journal of Environmental Research and Public Health. 2020; 17(1):140. https://doi.org/10.3390/ijerph17010140
Chicago/Turabian StyleCristina, Maria Luisa, Marina Sartini, Elisa Schinca, Gianluca Ottria, Chiara Dupont, Palmira Bova, Gianni Coccia, Beatrice Casini, and Anna Maria Spagnolo. 2020. "Is Post-Reprocessing Microbiological Surveillance of Duodenoscopes Effective in Reducing the Potential Risk in Transmitting Pathogens?" International Journal of Environmental Research and Public Health 17, no. 1: 140. https://doi.org/10.3390/ijerph17010140