Trans* Pregnancy and Lactation: A Literature Review from a Nursing Perspective

 ,
,  , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
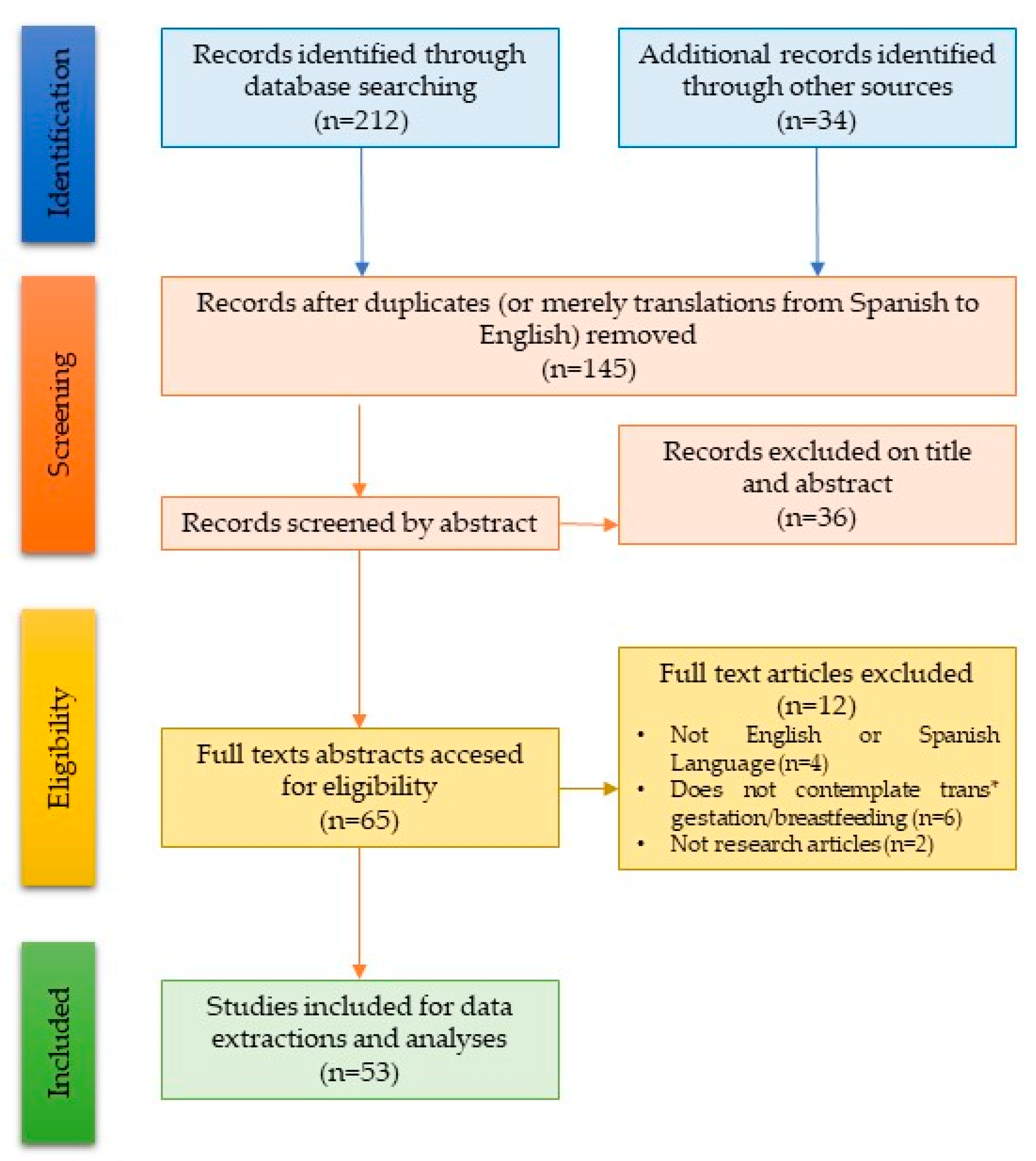
2. Materials and Methods
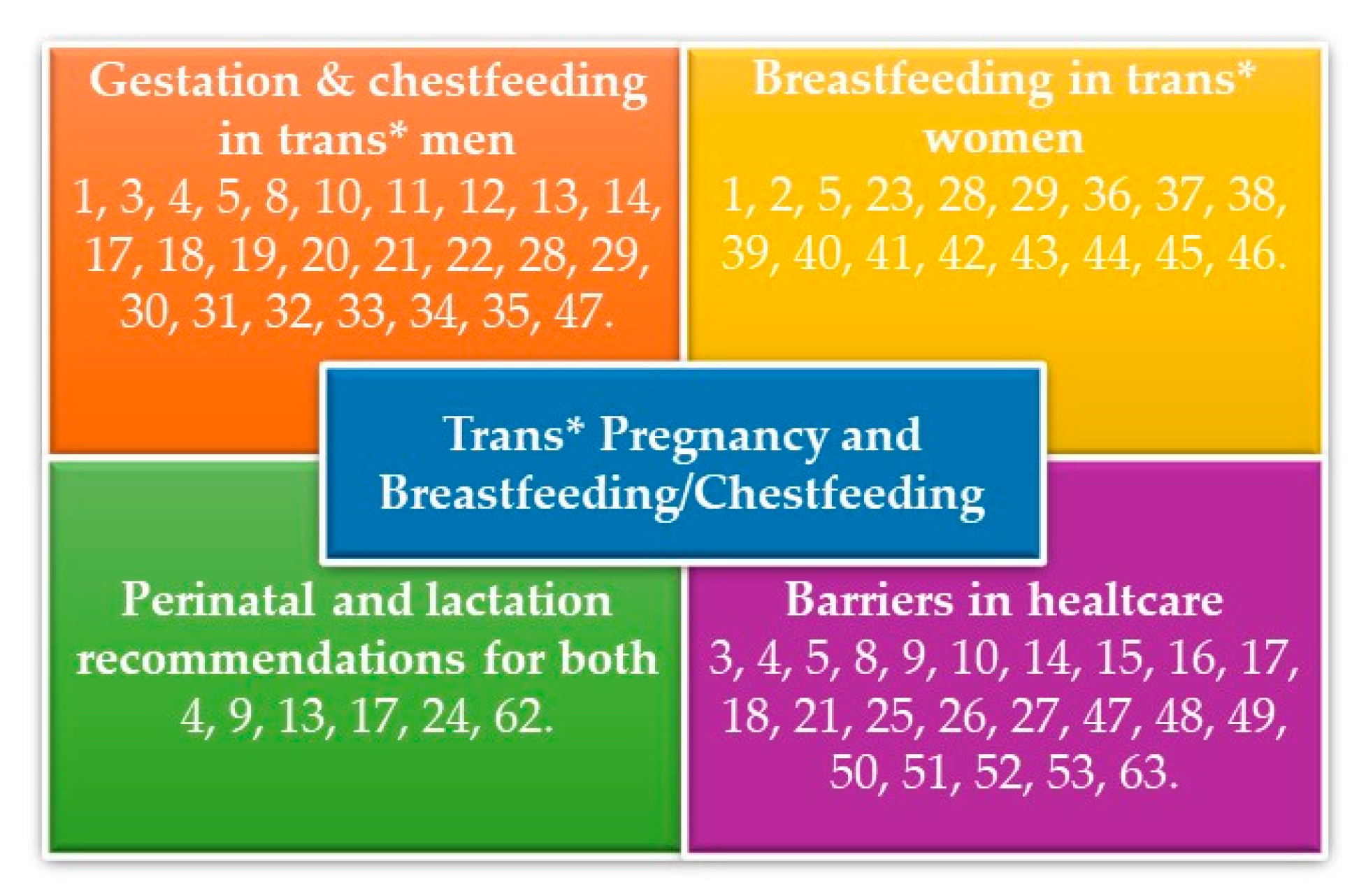
3. Results
3.1. Gestation and Chestfeeding in Trans* Men
3.2. The Breastfeeding Process in Trans* Women
3.3. Barriers in Healthcare
3.4. Recommendations on Perinatal Cares, Breastfeeding, and Chestfeeding
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Reisman, T.; Goldstein, Z.; Safer, J.D. A Review of Breast Development in Cisgender Women and Implications for Transgender Women. Endocr. Pract. 2019. [Google Scholar] [CrossRef]
- Sonnenblick, E.B.; Shah, A.D.; Goldstein, Z.; Reisman, T. Breast Imaging of Transgender Individuals: A Review. Curr. Radiol. Rep. 2018, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Castro-Peraza, M.-E.; García-Acosta, J.M.; Delgado-Rodriguez, N.; Sosa-Alvarez, M.I.; Llabrés-Solé, R.; Cardona-Llabrés, C.; Lorenzo-Rocha, N.D. Biological, Psychological, Social, and Legal Aspects of Trans Parenthood Based on a Real Case—A Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, T.; Noel-Weiss, J.; West, D.; Walks, M.; Biener, M.L.; Kibbe, A.; Myler, E. Transmasculine Individuals’ Experiences with Lactation, Chestfeeding, and Gender Identity: A Qualitative Study. BMC Pregnancy Childbirth 2016, 16, 106–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, E.; Bockting, W.; Botzer, M.; Cohen-Kettenis, G.; DeCuypere, J.; Feldman, L.; Fraser, L.; Green, J.; Knudson, G.; Meyer, W.J.; et al. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Int. J. Transgenderism 2012, 3, 165–232. [Google Scholar] [CrossRef]
- Winter, S.; Diamond, M.; Green, J.; Karasic, D.; Reed, T.; Whittle, S.; Wylie, K. Transgender People: Health at the Margins of Society. Lancet 2016, 388, 10042–10400. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM–5); American Psychiatric Association: Washintong, DC, USA, 2013; 947p. [Google Scholar]
- Hoffkling, A.; Obedin-Maliver, J.; Sevelius, J. From Erasure to Opportunity: A Qualitative Study of the Experiences of Transgender Men around Pregnancy and Recommendations for Providers. BMC Pregnancy Childbirth 2017, 17 (Suppl. 2), 332. [Google Scholar] [CrossRef] [Green Version]
- Fein, L.A.; Salgado, C.J.; Alvarez, C.V.; Estes, C.M. Transitioning Transgender: Investigating the Important Aspects of the Transition: A Brief Report. Int. J. Sex. Health 2017, 29, 80–88. [Google Scholar] [CrossRef]
- Obedin-Maliver, J.; Makadon, H.J. Transgender Men and Pregnancy. Obstet. Med. 2016, 9, 4–8. [Google Scholar] [CrossRef]
- Beatie, T. Labor of Love: The Story of One Mans Extraordinary Pregnancy; Seal Press: Berkeley, CA, USA, 2008; 280p. [Google Scholar]
- De Sutter, P. Gender Reassignment and Assisted Reproduction: Present and Future Reproductive Options for Transsexual People. Hum. Reprod. 2001, 16, 612–614. [Google Scholar] [CrossRef]
- Macdonald, T. Lactancia: Apoyando a Hombres Transexuales. Available online: http://laligadelaleche.eu/wp-content/uploads/Apoyando-a-hombres-transexuales.pdf (accessed on 7 September 2019).
- MacDonald, T.K. Lactation Care for Transgender and Non-Binary Patients: Empowering Clients and Avoiding Aversives. J. Hum. Lact. 2019, 35, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Riggs, D.W. Transgender Men’s Self-Representations of Bearing Children Post-Transition. In Chasing Rainbows: Exploring Gender Fluid Parenting Practices; Green, F.J., Friedman, M., Eds.; Demeter Press: Toronto, ON, Canada, 2013; p. 200. Available online: https://dspace2.flinders.edu.au/xmlui/handle/2328/35786 (accessed on 13 September 2019).
- Walks, M. Masculine pregnancy: Butch lesbians’, trans men’s & genderqueer individuals’ experiences. In Natal Signs: Cultural Representations of Pregnancy, Birth, and Parenting; Demeter Press: Toronto, ON, Canada, 2015; pp. 41–57. [Google Scholar]
- Wolfe-Roubatis, E.; Spatz, D.L. Transgender Men and Lactation: What Nurses Need to Know. MCN Am. J. Matern./Child Nurs. 2015, 40, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Light, A.D.; Obedin-Maliver, J.; Sevelius, J.M.; Kerns, J.L. Transgender Men Who Experienced Pregnancy after Female-to-Male Gender Transitioning. Obstet. Gynecol. 2014, 124, 1120–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Doussa, H.; Power, J.; Riggs, D. Imagining Parenthood: The Possibilities and Experiences of Parenthood among Transgender People. Cult. Health Sex. 2015, 17, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- James-Abra, S.; Tarasoff, L.A.; Green, D.; Epstein, R.; Anderson, S.; Marvel, L.S.; Steele, L.S.; Ross, L.E. Trans People’s Experiences with Assisted Reproduction Services: A Qualitative Study. Hum. Reprod. 2015, 30, 1365–1374. [Google Scholar] [CrossRef]
- Charter, R.; Ussher, J.M.; Perz, J.; Robinson, K. The Transgender Parent: Experiences and Constructions of Pregnancy and Parenthood for Transgender Men in Australia. Int. J. Transgenderism 2018, 19, 64–77. [Google Scholar] [CrossRef]
- Ellis, S.A.; Wojnar, D.M.; Pettinato, M. Conception, Pregnancy, and Birth Experiences of Male and Gender Variant Gestational Parents: It’s How We Could Have a Family. J. Midwifery Women’s Health 2015, 60, 62–69. [Google Scholar] [CrossRef]
- Reisman, T.; Goldstein, Z. Case Report: Induced Lactation in a Transgender Woman. Transgender Health 2018, 3, 24–26. [Google Scholar] [CrossRef] [Green Version]
- Macdonald, T. Breastfeeding and Parenting from a Transgender Perspective FAQ. Milk Junkies (Answer to Question 7). 2016. Available online: http://www.milkjunkies.net/p/faq.html (accessed on 25 September 2019).
- Bradford, J.; Reisner, S.L.; Honnold, J.A.; Xavier, J. Experiences of Transgender-Related Discrimination and Implications for Health: Results from the Virginia Transgender Health Initiative Study. Am. J. Public Health 2013, 103, 1820–1829. [Google Scholar] [CrossRef]
- Safer, J.D.; Coleman, E.; Feldman, J.; Garofalo, R.; Hembree, W.; Radix, A.; Sevelius, J. Barriers to Healthcare for Transgender Individuals. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 168–171. [Google Scholar] [CrossRef] [Green Version]
- García-Acosta, J.M.; Castro-Peraza, M.E.; Arias Rodriguez, Á.; Luisa Perez-Cánovas, M.; Sosa-Alvarez, M.I.; Llabrés-Solé, R.; Perdomo-Hernández, A.M.; Lorenzo-Rocha, N.D. Impact of a Formative Program on Transgender Healthcare for Nursing Students and Health Professionals. Quasi-Experimental Intervention Study. Int. J. Environ. Res. Public Health 2019, 16, 3205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hembree, W.C.; Cohen-Kettenis, P.T.; Gooren, L.; Hannema, S.E.; Meyer, W.J.; Murad, M.H.; Rosenthal, S.M.; Safer, J.D.; Tangpricha, V.; T’Sjoen, G.G. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society∗Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 3869–3903. [Google Scholar] [CrossRef] [PubMed]
- Fabris, B.; Bernardi, S.; Trombetta, C. Cross-Sex Hormone Therapy for Gender Dysphoria. J. Endocrinol. Investig. 2015, 38, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Caanen, M.R.; Soleman, R.S.; Kuijper, E.A.; Kreukels, B.P.; De Roo, C.; Tilleman, K.; de Sutter, P.; van Trotsenburg, M.A.A.; Broekmans, F.J.; Lambalk, C.B. Antimüllerian Hormone Levels Decrease in Female-to-Male Transsexuals Using Testosterone as Cross-Sex Therapy. Fertil. Steril. 2015, 103, 1340–1345. [Google Scholar] [CrossRef]
- Loverro, G.; Resta, L.; Dellino, M.; Cascarano, M.A.; Loverro, M.; Mastrolia, S.A. Uterine and Ovarian Changes during Testosterone Administration in Young Female-to-Male Transsexuals. Taiwan J. Obstet. Gynecol. 2016, 55, 686–691. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.; Jones, T.; Ward, R.; Dixon, J.; Mitchell, A.; Hillier, L. From Blues to Rainbows: The Mental Health and Wellbeing of Gender Diverse and Transgender Young People in Australia. Australian Research Centre in Sex Health and Society. 2014. Available online: https://researchers.mq.edu.au/en/publications/from-blues-to-rainbows-the-mental-health-and-wellbeing-of-gender--2 (accessed on 13 September 2019).
- Vita, R.; Settineri, S.; Liotta, M.; Benvenga, S.; Trimarchi, F. Changes in Hormonal and Metabolic Parameters in Transgender Subjects on Cross-Sex Hormone Therapy: A Cohort Study. Maturitas 2018, 107, 92–96. [Google Scholar] [CrossRef]
- De Roo, C.; Tilleman, K.; T’Sjoen, G.; De Sutter, P. Fertility options in transgender people. Int. Rev. Psychiatry 2016, 28, 112–119. [Google Scholar] [CrossRef]
- Riggs, D.W. What Makes a Man? Thomas Beatie, Embodiment, and “Mundane Transphobia”. Fem Psychol. 2014, 24, 157–171. [Google Scholar]
- De Blok, C.J.M.; Klaver, M.; Wiepjes, C.M.; Nota, N.M.; Heijboer, A.C.; Fisher, A.D.; Schreiner, T.; T’Sjoen, G.; den Heijer, M. Breast Development in Transwomen after 1 Year of Cross-Sex Hormone Therapy: Results of a Prospective Multicenter Study. J. Clin. Endocrinol. Metab. 2018, 103, 532–538. [Google Scholar] [CrossRef] [Green Version]
- Wierckx, K.; Gooren, L.; T’Sjoen, G. Clinical Review: Breast Development in Trans Women Receiving Cross-Sex Hormones. J. Sex. Med. 2014, 11, 1240–1247. [Google Scholar] [CrossRef]
- Kanhai, R.C.; Hage, J.J.; Van Diest, P.J.; Bloemena, E.; Mulder, J.W. Short-Term and Long-Term Histologic Effects of Castration and Estrogen Treatment on Breast Tissue of 14 Male-to-Female Transsexuals in Comparison with Two Chemically Castrated Men. Am. J. Surg. Pathol. 2000, 24, 74. [Google Scholar] [CrossRef] [PubMed]
- Breastfeeding Inc. Keeping Breastfeeding Simple, just as It Was Meant to be…. 2019. Available online: https://www.breastfeedinginc.ca/ (accessed on 13 October 2019).
- Newman, J. Breastfeeding Online 2019. Available online: http://www.breastfeedingonline.com/newman.shtml#sthash.j7VkbULN.dpbs (accessed on 13 October 2019).
- Newman, J.; Pitman, T. The Ultimate Breastfeeding Book of Answers: The Most Comprehensive Problem-Solution Guide to Breastfeeding from the Foremost Expert in North America; Prima Publishing: Roseville, CA, USA, 2000; 441p. [Google Scholar]
- Goldfarb, L.; Newman, J. Newman-Goldfarb Protocols for Induced Lactation Decision Tool. J. Hum. Lact. 2008, 24, 102. [Google Scholar]
- Padró, A. Cómo se Puede Inducir la Lactancia Materna Alba Lactancia Materna. 2019. Available online: https://albalactanciamaterna.org/lactancia/tema-2-como-superar-dificultades/como-relactar-o-inducir-una-lactancia/ (accessed on 10 October 2019).
- Farhadi, R.; Philip, R.K. Induction of Lactation in the Biological Mother after Gestational Surrogacy of Twins: A Novel Approach and Review of Literature. Breastfeed. Med. 2017, 12, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.; Perrin, M.T.; Fogleman, A.; Chetwynd, E. The intricacies of induced lactation for same-sex mothers of an adopted child. J. Hum. Lact. 2015, 31, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research. Information by Drug Class—FDA Talk Paper: FDA Warns against Women Using Unapproved Drug, Domperidone, to Increase Milk Production. U.S. Food & Drug Administration. 2016. Available online: https://www.fda.gov/drugs/information-drug-class/fda-talk-paper-fda-warns-against-women-using-unapproved-drug-domperidone-increase-milk-production (accessed on 7 October 2019).
- Dodgson, J.E. Non-Conforming: Aren’t We All in One Way or Another? J. Hum. Lact. 2019, 35, 212–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byron, P.; Rasmussen, S.; Wright Toussaint, D.; Lobo, R.; Robinson, K.H.; Paradise, B. Learn from Each Other LGBTIQ Young People’s Mental Health Help-Seeking and the RAD Australia Online Directory. 2017. Available online: https://researchdirect.westernsydney.edu.au/islandora/object/uws:38815/ (accessed on 23 July 2019).
- Grant, J.M.; Mottet, L.; Tanis, J.E.; Harrison, J.; Herman, J.; Keisling, M. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey; National Center for Transgender Equality: Washington, DC, USA, 2011. [Google Scholar]
- Obedin-maliver, J.; Goldsmith, E.S.; Stewart, L.; White, W.; Tran, E.; Brenman, S.; Wells, M.; Fetterman, D.M.; Garcia, G.; Lunn, M.R. Lesbian, Gay, Bisexual, and Transgender–Related Content in Undergraduate Medical Education. JAMA 2011, 306, 971–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, N.F.; Rabatin, J.; Sanchez, J.P.; Hubbard, S.; Kalet, A. Medical Students’ Ability to Care for Lesbian, Gay, Bisexual, and Transgendered Patients. Fam. Med. 2006, 38, 21–27. [Google Scholar] [PubMed]
- Snelgrove, J.W.; Jasudavisius, A.M.; Rowe, B.W.; Head, E.M.; Bauer, G.R. “Completely out-at-Sea” with “Two-Gender Medicine”: A Qualitative Analysis of Physician-Side Barriers to Providing Healthcare for Transgender Patients. BMC Health Serv. Res. 2012, 12, 110. [Google Scholar] [CrossRef] [Green Version]
- Duckett, L.J.; Ruud, M. Affirming Language Use When Providing Health Care for and Writing about Childbearing Families Who Identify as LGBTQI+. J. Hum. Lact. 2019, 35, 227–232. [Google Scholar] [CrossRef]
- World Health Organization. ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS) 2018 Version 2018. Available online: https://icd.who.int/browse11/l-m/en (accessed on 13 September 2019).
- Downing, J.B. Transgender-Parent Families. In LGBT-Parent Families; Springer: New York, NY, USA, 2013; pp. 105–115. Available online: https://link.springer.com/chapter/10.1007/978-1-4614-4556-2_7 (accessed on 18 September 2019).
- Oswald, R.F.; Blume, L.B.; Marks, S.R. Decentering Heteronormativity: A Model for Family Studies. Sourceb. Fam. Theory Res. 2005, 143–165. [Google Scholar]
- Ryan, C. Supportive Families, Healthy Children: Helping Families with Lesbian, Gay, Bisexual & Transgender Children; Family Acceptance Project; San Francisco State University: San Francisco, CA, USA, 2009. [Google Scholar]
- Ryan, M. The Gender of Pregnancy: Masculine Lesbians Talk about Reproduction. J. Lesbian Stud. 2013, 17, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Arenz, S.; Rückerl, R.; Koletzko, B.; Von Kries, R. Breast-Feeding and Childhood Obesity—A Systematic Review. Int. J. Obes. 2004, 28, 1247–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, J.; Kernerman, E. Breastfeeding Your Adopted Baby or Baby Born by Surrogate/Gestational Carrier Canadian Breastfeeding Foundation. 2009. Available online: https://www.canadianbreastfeedingfoundation.org/induced/adoptive_breastfeeding.shtml (accessed on 27 September 2019).
- López Granados, L.; Serrano Reynal, A.; Mora, C.C. Inducción de la Lactancia sin Gestación. Rev. Pediatr. Aten. Primaria 2018, 20, 113–115. [Google Scholar]
- Adams, E.D. If Transmen Can Have Babies, How Will Perinatal Nursing Adapt? MCN Am. J. Matern./Child Nurs. 2010, 35, 26–32. [Google Scholar] [CrossRef]
- Poteat, T.; German, D.; Kerrigan, D. Managing Uncertainty: A Grounded Theory of Stigma in Transgender Health Care Encounters. Soc. Sci. Med. 2013, 84, 22–29. [Google Scholar] [CrossRef]
- Thomas, R.; Pega, F.; Khosla, R.; Verster, A.; Hana, T.; Say, L. Ensuring an inclusive global health agenda for transgender people. Bull. World Health Organ. 2017, 95, 154. [Google Scholar] [CrossRef]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Acosta, J.M.; San Juan-Valdivia, R.M.; Fernández-Martínez, A.D.; Lorenzo-Rocha, N.D.; Castro-Peraza, M.E. Trans* Pregnancy and Lactation: A Literature Review from a Nursing Perspective. Int. J. Environ. Res. Public Health 2020, 17, 44. https://doi.org/10.3390/ijerph17010044
García-Acosta JM, San Juan-Valdivia RM, Fernández-Martínez AD, Lorenzo-Rocha ND, Castro-Peraza ME. Trans* Pregnancy and Lactation: A Literature Review from a Nursing Perspective. International Journal of Environmental Research and Public Health. 2020; 17(1):44. https://doi.org/10.3390/ijerph17010044
Chicago/Turabian StyleGarcía-Acosta, Jesús Manuel, Rosa María San Juan-Valdivia, Alfredo David Fernández-Martínez, Nieves Doria Lorenzo-Rocha, and Maria Elisa Castro-Peraza. 2020. "Trans* Pregnancy and Lactation: A Literature Review from a Nursing Perspective" International Journal of Environmental Research and Public Health 17, no. 1: 44. https://doi.org/10.3390/ijerph17010044