Potential of Vibroacoustic Therapy in Persons with Cerebral Palsy: An Advanced Narrative Review



Abstract
:1. Introduction
2. Materials and Methods
- the age of the included people with CP;
- what measurement tools have been implemented in research on effects of VAT on motor function of people with spastic CP; and
- what low-frequency or types of low-sinusoidal stimulations have been used in research on the effects of VAT on motor function of people with spastic CP.
- PubMed,
- MEDLINE complete,
- Bibliographia Medica Čechoslovaca (the Medvik interface),
- EBSCO host,
- EBSCO discovery,
- ERIC,
- Wiley Online Library,
- EBM Reviews,
- ProQuest,
- Scopus,
- CINAHL Plus (with Full Text),
- Cochrane Library,
- JBI
- Prospero,
- MedNar, and
- Google Scholar.
3. Results
3.1. Results of Relevant Studies Applying VAT in Children with CP
3.2. Results of Studies Applying VAT in Adults with CP
4. Discussion
4.1. Recommendations for Future Research
- There have been few RCTs, and, specifically, double-blind and triple-blind studies are completely missing.
- Effects of VAT on adolescents and young adults with CP have not been explored yet.
- Using standardized measurement tools enables comparisons of results.
- It is advisable to include measuring spasticity (using MMAS).
- There is little knowledge on the possibly of different therapeutic outcomes of various frequencies or types of low-sinusoidal stimulation.
- There are other topics not addressed sufficiently in this review that would be worthy of further research (e.g., exploring the mechanisms of how VAT influences neuromuscular functions).
4.2. Reflection of the Review
5. Conclusions
Note
Author Contributions
Funding
Conflicts of Interest
References
- Bax, M.; Goldstein, M.; Rosenbaum, P.; Leviton, A.; Paneth, N.; Dan, B.; Jacobssen, B.; Damiano, D. Executive Committee for the definition of Cerebral Palsy. Proposed definition and classification of cerebral palsy, April 2005. Dev. Med. Child Neurol. 2005, 47, 571–576. [Google Scholar] [CrossRef]
- Panteliadis, C.P.; Hagel, C.; Karch, D.; Heinemann, K. Cerebral Palsy: A Lifelong Challenge Asks for Early Intervention. Open Neurol. J. 2015, 9, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colver, A.; Rapp, M.; Eisemann, N.; Ehlinger, V.; Thyen, U.; Dickinson, H.O.; Parkes, J.; Parkinson, K.; Nystrand, M.; Fauconnier, J.; et al. Self-reported quality of life of adolescents with cerebral palsy: A cross-sectional and longitudinal analysis. Lancet 2015, 385, 705–716. [Google Scholar] [CrossRef]
- Ritzmann, R.; Stark, C.; Krause, A. Vibration therapy in patients with cerebral palsy: A systematic review. Neuropsychiatr. Dis. Treat. 2018, 14, 1607–1625. [Google Scholar] [CrossRef] [PubMed]
- Neurosurgical Conditions and Treatments: Spasticity. Available online: https://www.aans.org/Patients/Neurosurgical-Conditions-and-Treatments/Spasticity (accessed on 7 September 2019).
- Kolář, P. Dětská mozková obrna. In Rehabilitace v Klinické Praxi. [Rehabilitation in Clinical Practice], 1st ed.; Kolář, P., Ed.; Galén: Praha, Czech Republic, 2010; ISBN 9788072626571. [Google Scholar]
- Rosenbaum, P.L.; Walter, S.D.; Hanna, S.E.; Palisano, R.J.; Russell, D.J.; Raina, P.; Wood, E.; Bartlett, D.J.; Galuppi, B.E. Prognosis for gross motor function in cerebral palsy: Creation of motor development curves. JAMA 2002, 288, 1357–1363. [Google Scholar] [CrossRef]
- Jahnsen, R.; Villien, L.; Stanghelle, J.K.; Egeland, T. Locomotion skills in adults with cerebral palsy. Clin. Rehabil. 2004, 18, 309–316. [Google Scholar] [CrossRef]
- Hanna, S.E.; Rosenbaum, P.L.; Bartlett, D.J.; Palisano, R.J.; Walter, S.D.; Avery, L.; Russell, D.J. Stability and decline in gross motor function among children and youth with cerebral palsy aged 2 to 21 years. Dev. Med. Child Neurol. 2009, 51, 295–302. [Google Scholar] [CrossRef]
- Haak, P.; Lenski, M.; Hidecker, M.J.C.; Li, M.; Paneth, N. Cerebral palsy and aging. Dev. Med. Child Neurol. 2009, 51, 16–23. [Google Scholar] [CrossRef]
- Das, S.P.; Ganesh, G.S. Evidence-based Approach to Physical Therapy in Cerebral Palsy. Indian J. Orthop. 2019, 53, 20–34. [Google Scholar]
- Hoare, B.J.; Wallen, M.A.; Imms, C.; Villanueva, E.; Rawicki, H.B.; Carey, L. Botulinum toxin A as an adjunct to treatment in the management of the upper limb in children with spastic cerebral palsy (UPDATE). Cochrane Database Syst. Rev. 2010, CD003469. [Google Scholar] [CrossRef]
- Saquetto, M.; Carvalho, V.; Silva, C.; Conceição, C.; Gomes-Neto, M. The effects of whole body vibration on mobility and balance in children with cerebral palsy: A systematic review with meta-analysis. J. Musculoskelet. Neuronal Interact. 2015, 15, 137–144. [Google Scholar] [PubMed]
- Huang, M.; Liao, L.R.; Pang, M.Y. Effects of whole body vibration on muscle spasticity for people with central nervous system disorders: A systematic review. Clin. Rehabil. 2017, 31, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Pin, T.W.; Butler, P.B.; Purves, S. Use of whole body vibration therapy in individuals with moderate severity of cerebral palsy- a feasibility study. BMC Neurol. 2019, 19, 80. [Google Scholar] [CrossRef] [PubMed]
- Hooper, J. Is VA therapy, music therapy? Music Ther. Today 2002, 2, 24. [Google Scholar]
- Park, C.; Park, E.S.; Choi, J.Y.; Cho, Y.; Rha, D.-W. Immediate Effect of a Single Session of Whole Body Vibration on Spasticity in Children with Cerebral Palsy. Ann. Rehabil. Med. 2017, 41, 273–278. [Google Scholar] [CrossRef]
- Wigram, T. The Effects of Vibroacoustic Therapy on Clinical and Non-Clinical Populations. Ph.D. Thesis, London University, London, UK, 1996. [Google Scholar]
- Boyd-Brewer, C.H. Vibroacoustic Therapy: Sound Vibrations in Medicine. Altern. Complement. Ther. 2003, 9. [Google Scholar] [CrossRef]
- Chesky, K.S.; Michel, D.E. The Music Vibration Table (MVT): Developing a Technology and Conceptual Model for Pain Relief. Music Ther. Perspect. 1991, 9, 32–38. [Google Scholar] [CrossRef]
- Rüütel, E.; Vinkel, I.; Laanetu, M. Vibroacoustic Therapy and Development of a New Device: A Pilot Study in the Health Resort Environment. Univers. J. Public Health 2018, 6, 240–246. [Google Scholar] [CrossRef]
- MultivibTM. Available online: http://www.multivib.com/what-is-multivib/ (accessed on 3 October 2019).
- Vilímek, Z.; Kantor, J.; Chráska, M. Vliv vibroakustické stimulace na autonomní nervový systém. [Influence of vibroacoustic stimulation on autonomic nervous system]. In Tělo a Mysl. Proceedings of the PhD Existence, Palacky University in Olomouc, Olomouc, Czech Republic, 21–22 January 2019; University of Olomouc: Olomouc, Czech Republic, 2019; pp. 322–329. [Google Scholar]
- Nex Neuro Vibro-Acoustic Therapy. Available online: https://buynexneuro.weebly.com/ (accessed on 3 October 2019).
- VTS-1000 Vibroacoustic Therapy System. Available online: https://www.soundoasis.com/products/sleep-sound-therapy-systems/vibroacoustic-therapy-system/ (accessed on 4 October 2019).
- What Is SUBPAC? Available online: https://subpac.com/what-is-the-subpac/ (accessed on 4 October 2019).
- Boyd-Brewer, C.; McCaffrey, R. Vibroacoustic sound therapy improves pain management and more. Holist. Nurs. Pract. 2004, 18, 111–118. [Google Scholar] [CrossRef]
- Ahonen, H. Low frequency research—Client populations and common frequencies used—Literature review. Laurier Centre Music Ther. Res. Newsl. 2007, 4, 1–5. [Google Scholar]
- Skille, O. Manual of Vibroacoustics; ISVA Publications: Levanger, Norway, 1986. [Google Scholar]
- Galambos, R.; Makeig, S.; Talmachoff, P.J. A 40-Hz auditory potential recorded from the human scalp. Proc. Natl. Acad. Sci. USA 1981, 78, 2643–2647. [Google Scholar] [CrossRef] [PubMed]
- Skille, O. VibroAcoustic Therapy. Music Ther. 1989, 8, 61–77. [Google Scholar] [CrossRef] [Green Version]
- Rüütel, E.; Vinkel, I.; & Eelmäe, P. The effect of short-term vibroacoustic treatment on spasticity and perceived health condition of patients with spinal cord and brain injuries. Music Med. 2017, 9, 202–208. [Google Scholar] [CrossRef]
- Guyatt, G.H. Evidence-based Medicine. ACP J. Club 1991, 114, A16. [Google Scholar] [CrossRef] [PubMed]
- Klugarová, J. Vyhledávání nejlepších dostupných vědeckých důkazů. [Searching for the Best Scientific Evidence]. In Evidence Based Healthcare: Zdravotnictví Založené na Vědeckých Důkazech, 1st ed.; Klugarová, J., Marečková, J., Eds.; Univerzita Palackého v Olomouci: Olomouc, Czech Republic, 2015; pp. 17–33. ISBN 978-80-244-4784-1. [Google Scholar]
- Wigram, T. The Effect of Vibroacoustic (VA) Therapy on Multiply Handicapped Adults with High Muscle Tone and Spasticity (4th chapter). The Effects of Vibroacoustic Therapy on Clinical and Non-Clinical Populations. Ph.D. Thesis, London University, London, UK, 1996; pp. 92–115. [Google Scholar]
- Wigram, T. The Effect of Vibroacoustic (VA) Therapy Compared with Music and Movement Based Physiotherapy on Multiply Handicapped Patients with High Muscle Tone and Spasticity (5th chapter). The Effects of Vibroacoustic Therapy on Clinical and Non-Clinical Populations. Ph.D. Thesis, London University, London, UK, 1996; pp. 116–144. [Google Scholar]
- Wigram, T.; Dileo, C. Music Vibration and Health, 1st ed.; Jeffrey Books: Cherry Hill, NJ, USA, 1997; pp. 57–86. [Google Scholar]
- Katusic, A. Učinak Zvučnih Vibracija Frekvencije 40 Hz na Spastičnost i Motoričke Funkcije u Djece sa Cerebralnom Paralizom [The Effect of 40 Hz Sound Wave Vibration on Spasticity and Motor Functions in Children with Cerebral Palsy]. Ph.D. Thesis, University of Zagreb Medical School Repository, Zagreb, Croatia, 2012. [Google Scholar]
- Katusic, A.; Alimovic, S.; Mejaski-Bosnjak, V. The effect of vibration therapy on spasticity and motor function in children with cerebral palsy: A randomized controlled trial. NeuroRehabilitation 2013, 32, 1–8. [Google Scholar] [PubMed]
- Liu, Z.; Zhang, L.; Zhao, Y. Effect of Vibroacoustic Therapy with Five Elements Music on Muscle Tone of Children with Cerebral Palsy. Chin. J. Rehabil. Theory Prac. 2013, 19, 771–774. [Google Scholar] [CrossRef]
- Liu, Z.H.; Zhang, L.H.; Yin, X.T. Clinical observation of the therapeutic effect of vibroacoustic therapy in relieving spasticity for children with cerebral palsy. Chin. Pediatr. Integr. Tradit. West. Med. 2010, 2, 27–29. [Google Scholar] [CrossRef]
- Kvam, M.H. The Effect of Vibroacoustic Therapy. Physiotherapy 1997, 83, 290–295. [Google Scholar] [CrossRef]
- Katusić, A.; Mejaski-Bosnjak, V. Effects of vibrotactile stimulation on the control of muscle tone and movement facilitation in children with cerebral injury. Coll. Antropol. 2011, 35, 57–63. [Google Scholar]
- Duquette, S.A.; Guiliano, A.M.; Starmer, D.J. Whole body vibration and cerebral palsy: A systematic review. J. Can. Chiropr. Assoc. 2015, 59, 245–252. [Google Scholar]
- Krause, A.; Schönau, E.; Gollhofer, A.; Duran, I.; Ferrari-Malik, A.; Freyler, K.; Ritzmann, R. Alleviation of Motor Impairments in Patients with Cerebral Palsy: Acute Effects of Whole-body Vibration on Stretch Reflex Response, Voluntary Muscle Activation and Mobility. Front. Neurol. 2017, 8, 416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tupimai, T.; Peungsuwan, P.; Prasertnoo, J.; Yamauchi, J. Effect of combining passive muscle stretching and whole body vibration on spasticity and physical performance of children and adolescents with cerebral palsy. J. Phys. Ther. Sci. 2016, 28, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ala-Ruona, A.; Punkanen, M.; Campbell, E. Vibroacoustic therapy: Conception, development, and future directions. Musiikkiterapia (Finish J. Music Ther.) 2015, 30, 48–71. [Google Scholar]
- Sokira, J.M. Physical Disabilities in School Children. In Guidelines for Music Therapy Practice in Developmental Health, 1st ed.; Hintz, M., Ed.; Barcelona Publishers: Gilsum, NH, USA, 2013; pp. 371–398. ISBN 978-1-937440-44-2. [Google Scholar]



{kind=link}
{kind=link}
| Primary search terms | |
| P | Spastic cerebral palsy |
| I | Vibroacoustic therapy |
| C | NA |
| O | Motor function |
| Primary search terms + synonyms + related terms | |
| P | “cerebral palsy“ OR “spastic paralysis“ OR quadriparesis OR diparesis OR hemiparesis |
| I | “vibroacoustic therapy“ OR “vibroacoustic music“ OR “vibroacoustic sound“ OR “somatosensory music therapy“ OR physioacoustic OR “physio acoustic sound” OR somatron OR “low-frequency sound stimulation” OR “vibrotactile stimulation” OR “music vibration table” |
| C | NA |
| O | “motor function” OR “range of motion“ OR “movement AND spasticity” |
| Database | Results for P (n) | Results for I (n) | Results for O (n) | Search Results (n) |
|---|---|---|---|---|
| PubMed | 31,713 | 333 | 265,208 | 1 |
| Medline | 25,671 | 292 | 310,806 | 1 |
| BMČ (Medvik) | 196 | 1 | 1572 | 0 |
| EBSCO discovery | 112,674 | 1547 | 2,905,734 | 8 |
| ERIC | 2980 | 255,974 | 1,673,393 | 0 |
| Wiley Online Library | 9980 | 0 | 2,300,473 | 0 |
| EBM Reviews | 4962 | 39 | 37,242 | 1 |
| ProQuest | 99,370 | 652 | 2,756,038 | 4 |
| Scopus | 59,723 | 2407 | 2,649,382 | 2 |
| CINAHL Plus | 8998 | 40 | 60,427 | 0 |
| Cochrane Library | 77 | 45 | 99 | 0 |
| JBI | 38 | 484 | 2 | 1 |
| Prospero | 598 | 0 | 92 | 0 |
| MedNar * | 1388 | 313 | 2385 | 344 |
| Google Scholar * | cca 550,000 | cca 8990 | cca 5,560,000 | 461 |
| Research Design | Randomized Controlled Trial, Single-Blinded |
|---|---|
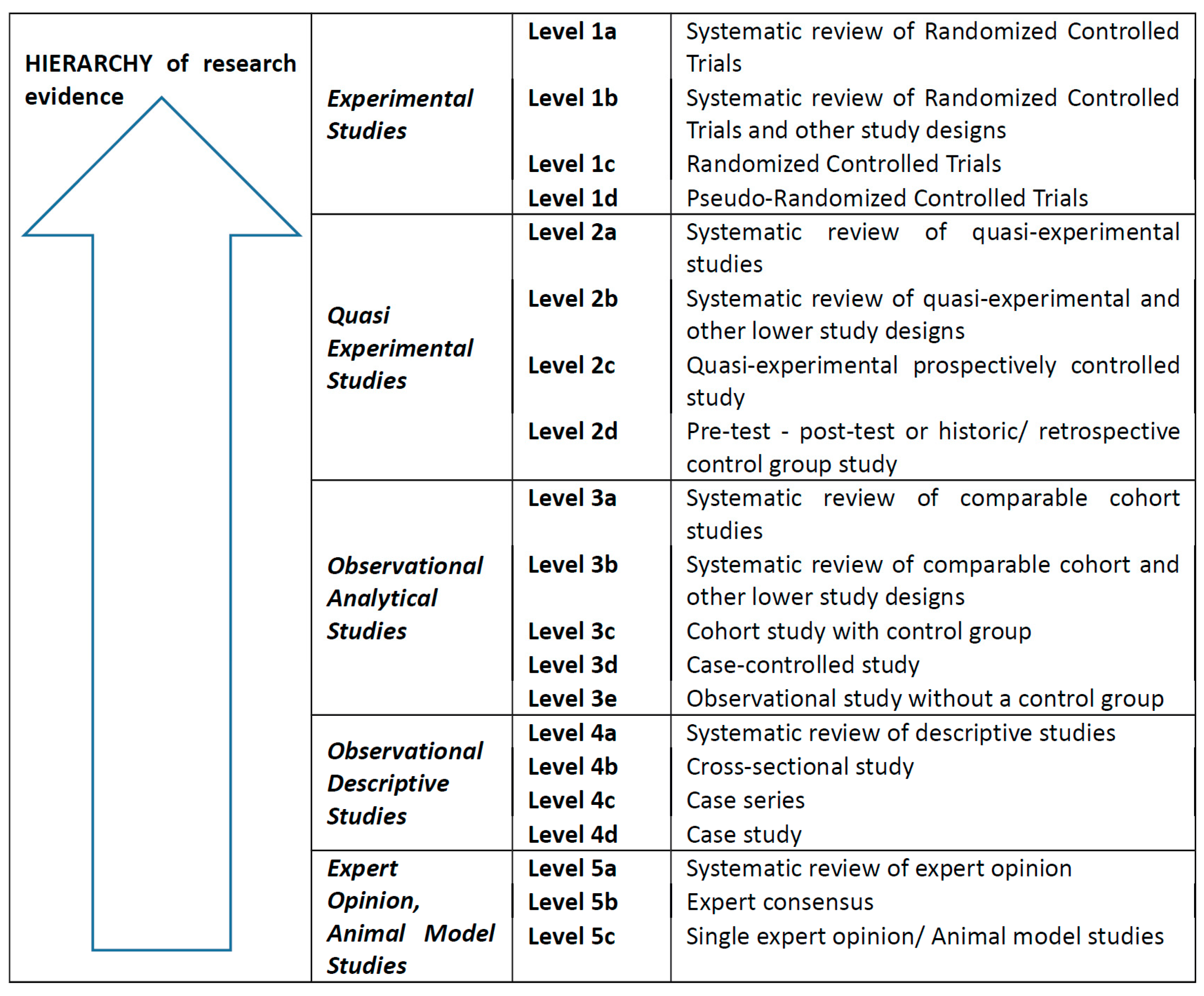
| JBI level of evidence | 1c |
| Objective(s) stated in the study | To determine the effects of VAT on spasticity and motor function in children with CP (age 4–6) undergoing physiotherapy compared to physiotherapy alone |
| Sample | 89 children (age 4–6) with spastic CP from a daycare center for rehabilitation were randomized into conventional therapy or conventional + VAT. |
| Randomization | Stratified according to GMFCS level |
| Intervention | Experimental group: VAT (on top of conventional therapy) twice a week for 12 weeks (40 Hz with sinusoidal amplitude variations −6.8 s between peaks). Control group: physiotherapy 3 times a week for 40 min. |
| Measurements | Pre- and post-12-week period MMAS spasticity, GMFM-88 by blinded evaluators. Statistical methods: non-parametric Wilcoxon matched pairs test and Mann–Whitney U test. |
| Results | The 12-week-change MMAS total score showed that spasticity level decreased more in the VAT group (p < 0.001). GMFM-88 significantly improved more in the VAT group (p < 0.001). |
| Research Design | Quasi-Experimental Prospective Study |
|---|---|
| JBI level of evidence | 2c |
| Objective(s) stated in the study | To determine the effects of VAT on muscle tension and range of motion in children with spastic CP (age 1–6) compared with physiotherapy and placebo. |
| Sample | 90 children (age 1–6) from Nanhai Affiliated Maternity and Children’s Hospital of Guangzhou University of Traditional Chinese Medicine allocated equally into three groups: conventional therapy, placebo, and VAT. The study does not specify how participants were allocated into groups. There was no significant difference between the groups for gender, age, and for some of the muscle tone and range of motion measurements (p > 0.05). |
| Intervention | Conventional therapy group—physical therapy, massage, and Chinese herb bath (once a day for 20 d). Experimental group—conventional therapy + VAT (60 Hz with Jiao music). Control group—conventional therapy + Jiao music. Interventions for both groups: 30 min a day for 20 d. |
| Measurements | An average of 3 measurements of muscle tone and range of motion (before, midway, and after treatment) were used, muscle tone assessed by MMAS, and statistical methods used included matching t test and variance. |
| Results | There was no statistically significant difference for the conventional group after 20 d of treatment. Listening (placebo) group had a decrease in muscle tone (p < 0.05). In the VAT group, the range of motion of hips, knees, and ankles improved, and muscle tone decreased (p < 0.05). 89 children (age 4–6) with spastic CP from a daycare center for rehabilitation were randomized into conventional therapy or conventional + VAT. |
| Research Design | Pretest–Post-Test Quasiexperimental Study |
|---|---|
| JBI level of evidence | 2d |
| Objective(s) stated in the study | To determine the effects of VAT on spasticity and motor function in children with spastic CP (age 3–4) |
| Sample | 13 children (age 3–4) from a daycare center for rehabilitation. |
| Intervention | VAT once a week for 12 weeks, 20 min (40 Hz sine wave with sinusoidal amplitude variation, 6.8 s between peaks). |
| Measurements | Pre- and post-12 week treatment GMFM-88, GMFCS standardised assessments, non-parametric Wilcoxon matched pairs test and Pearson c 2-test. |
| Results | Significant improvement in motor function. There was a significant improvement in total GMFM score (z = 3.17, p = 0.00), as well as on dimension A (lying and rolling, z = 3.05, p = 0.00) and dimension B (sitting, z = 2.80, p = 0.00). There was a significant difference between GMFCS levels of children before and after intervention (df = 6, p = 0.00). |
| Research Design | Pretest–Post-Test Quasiexperimental Study |
|---|---|
| JBI level of evidence | 2d |
| Objective(s) stated in the study | To determine effects of VAT on muscle tension and range of motion in children with spastic CP (age 2–8) |
| Sample | 36 children (2–8 years) with spastic cerebral palsy in outpatient and hospitalized care at children´s rehabilitation hospital clinic. |
| Intervention | Application of vibroacoustic therapy (16–150 Hz) with Jiao music 30 min each time. No mention of length of therapy. |
| Measurements | Measuring range of motion, muscle tension: MMAS. Statistical methods used: t test. |
| Results | After VAT, the adductor angle, popliteal fossa angle, food dorsiflexion angle, and muscle tone improved (p < 0.05). |
| Research Design | Double-Blind Randomized Controlled Trial |
|---|---|
| JBI level of evidence | 1c |
| Objective(s) stated in the study | To determine effects of VAT in adults with CP (age 27–48) on gross and fine movements compared to placebo |
| Sample | From 1 sheltered workshop of 14 workers, 12 had CP and were included. |
| Randomization | Stratified randomization of sample size 12: 6 pairs were created based on similarities in age, level of communication, physical functioning, and level of independence. One member of each pair was randomly selected for the experimental group. |
| Intervention | Experimental group: application of VAT (40–80 Hz) twice weekly for 9 weeks. Control group: application of music only, no vibrations, twice weekly for 9 weeks. |
| Measurements | Videotapes of gross and fine movements and drawing/writing tests (Swedish test by Bille) blind evaluation by 4 assessors, AND post-trial interviews. Statistical methods used: non-parametric one-tailed Wilcoxon signed rank test for matched pairs, inter-rater reliability of the test was 90% and of the drawing test 92%. |
| Results | All experimental participants showed greater improvement after treatment in motor test, and most participants were also better in drawing tests than those in the control group. In the area of hand–eye coordination, there was a statistically significant improvement (p = 0.034), and improvement in fine movements was quite significant (p = 0.069). In the final interviews with participants, the experimental group was more positive as to the effect of the treatment (p = 0.054) and more certain of their desire to continue (statistically significant, p = 0.034). No participant results were worse after the treatment. |
| Research Design | Pretest–Post-Test Quasiexperimental Study (Included Subjects Studied with a Single Blind Evaluation) |
|---|---|
| JBI level of evidence | 2d |
| Objective(s) stated in the study | To determine effects of VAT on range of motion in adults (age 28–77) with CP and high muscle tone compared with placebo (only music) |
| Sample | 10 residents of a large mental hospital took part in the trials (28–77 years), with severe disorder with spastic cerebral palsy, with high muscle tone. |
| Intervention | All 10 subjects received 6 sessions of 30 min VAT (44 Hz) as well as 6 only music (no vibrations) sessions, randomly ordered, 2 times a week over 6 weeks. |
| Measurements | Blind evaluation of spinal mobility and limb flexion and extension using tape measures of range of movement before and after each session. Statistics: Wilcoxon matched pairs signed rank test. |
| Results | VAT treatment showed significantly improved range of movement than placebo (no vibrations), p = 0.0051. |
| Research Design | Pretest–Post-Test Quasiexperimental Study |
|---|---|
| JBI level of evidence | 2d |
| Objective(s) stated in the study | To determine effects of VAT on range of motion in adults (age 24–68) with high muscle tone compared to placebo |
| Sample | 10 participants were randomly chosen from a group of 27 residents of a large mental hospital (24–68 years) all with high muscle tone who were included in a different part of the same study. |
| Intervention | Three 30 min VAT sessions using 44 Hz and three music (placebo) sessions in each of the 10 participants administered blindly. |
| Measurements | Range of motion, extension of arms and legs in centimeters measured before and after each treatment, statistics: Wilcoxon matched pairs signed rank test. |
| Results | All 10 participants had improved motor function after VAT compared with a placebo (only music) with a significant difference p = 0.0051. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kantor, J.; Kantorová, L.; Marečková, J.; Peng, D.; Vilímek, Z. Potential of Vibroacoustic Therapy in Persons with Cerebral Palsy: An Advanced Narrative Review. Int. J. Environ. Res. Public Health 2019, 16, 3940. https://doi.org/10.3390/ijerph16203940
Kantor J, Kantorová L, Marečková J, Peng D, Vilímek Z. Potential of Vibroacoustic Therapy in Persons with Cerebral Palsy: An Advanced Narrative Review. International Journal of Environmental Research and Public Health. 2019; 16(20):3940. https://doi.org/10.3390/ijerph16203940
Chicago/Turabian StyleKantor, Jiří, Lucia Kantorová, Jana Marečková, Danping Peng, and Zdeněk Vilímek. 2019. "Potential of Vibroacoustic Therapy in Persons with Cerebral Palsy: An Advanced Narrative Review" International Journal of Environmental Research and Public Health 16, no. 20: 3940. https://doi.org/10.3390/ijerph16203940