Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials

 ,
,  ,
,  , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Quality Assessment
2.3. Data Extraction
2.4. Outcomes
2.5. Statistical Analysis
3. Results
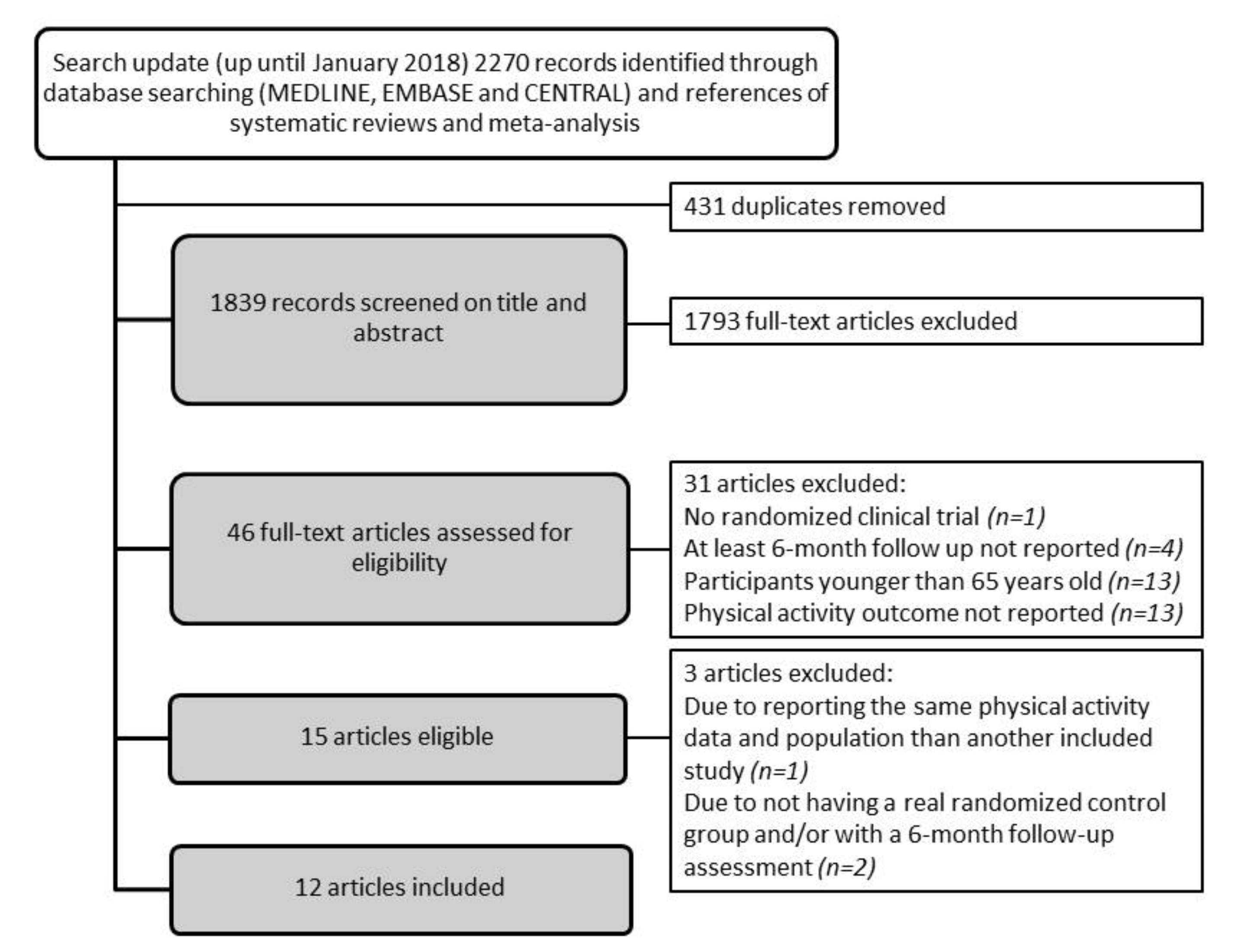
3.1. Description of Study Inclusion (Figure 1)
3.2. Characteristics of Exercise Arms Included in the Meta-Analysis
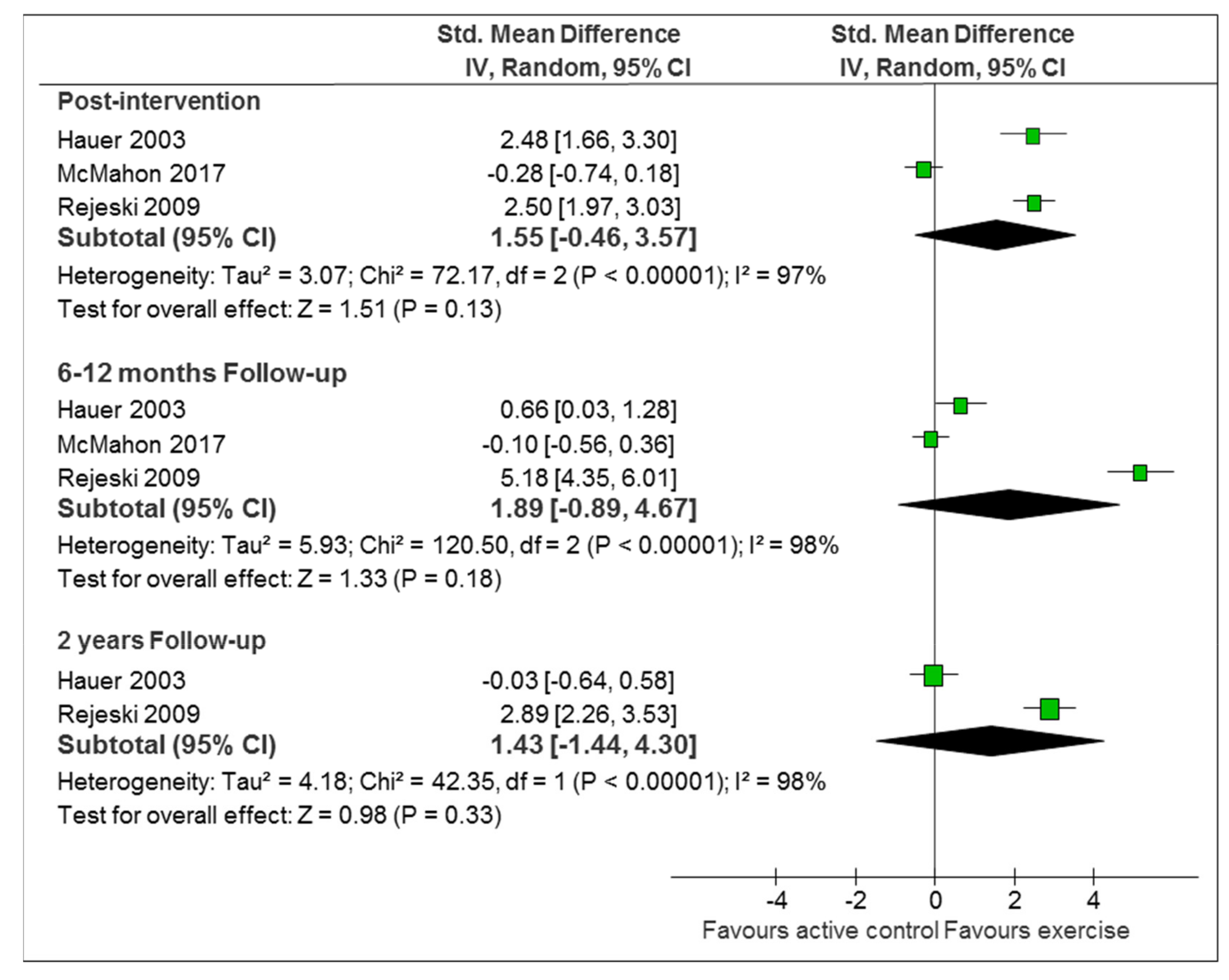
3.3. Comparison 1: Exercise-Based Intervention Versus Active Control
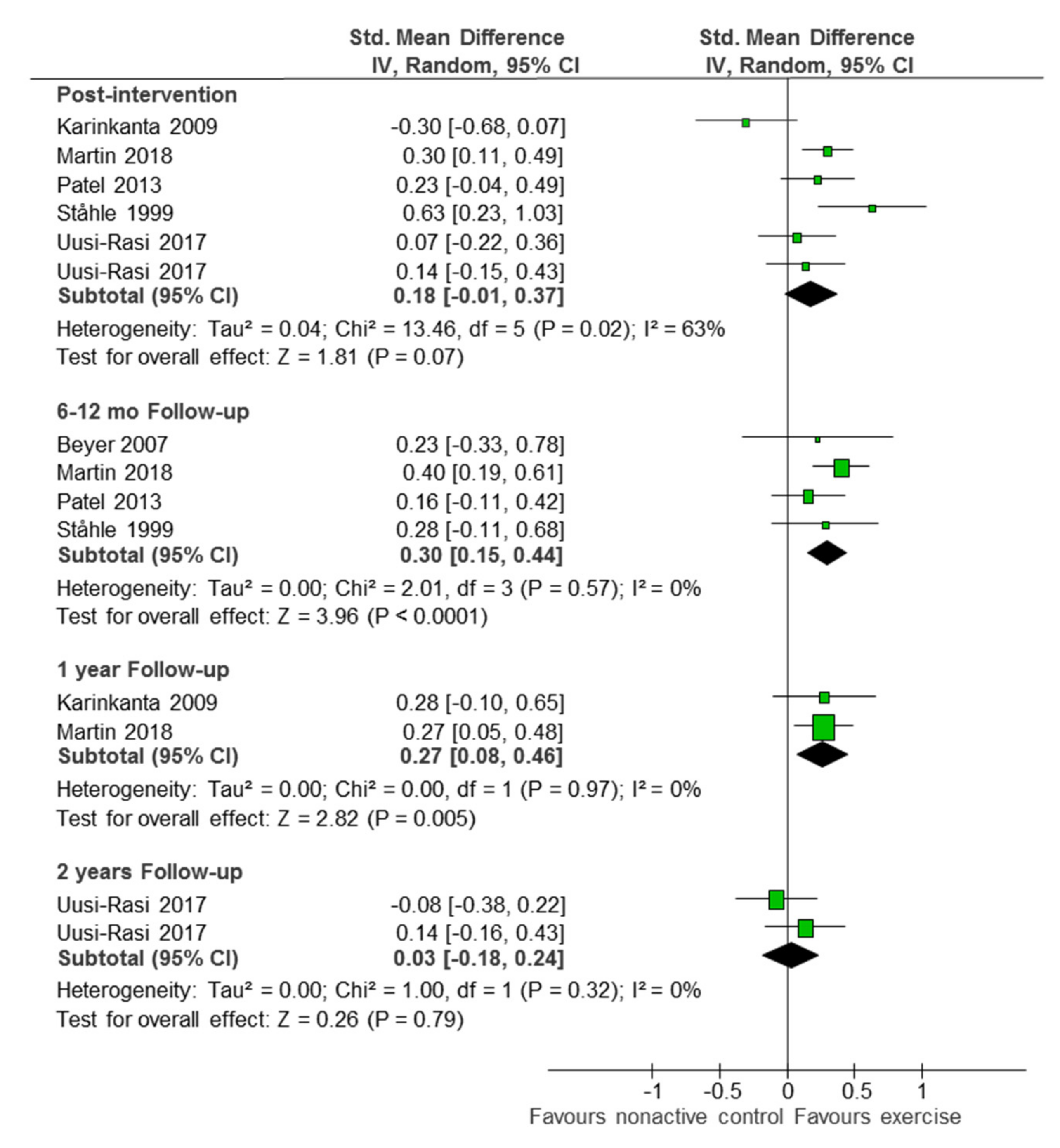
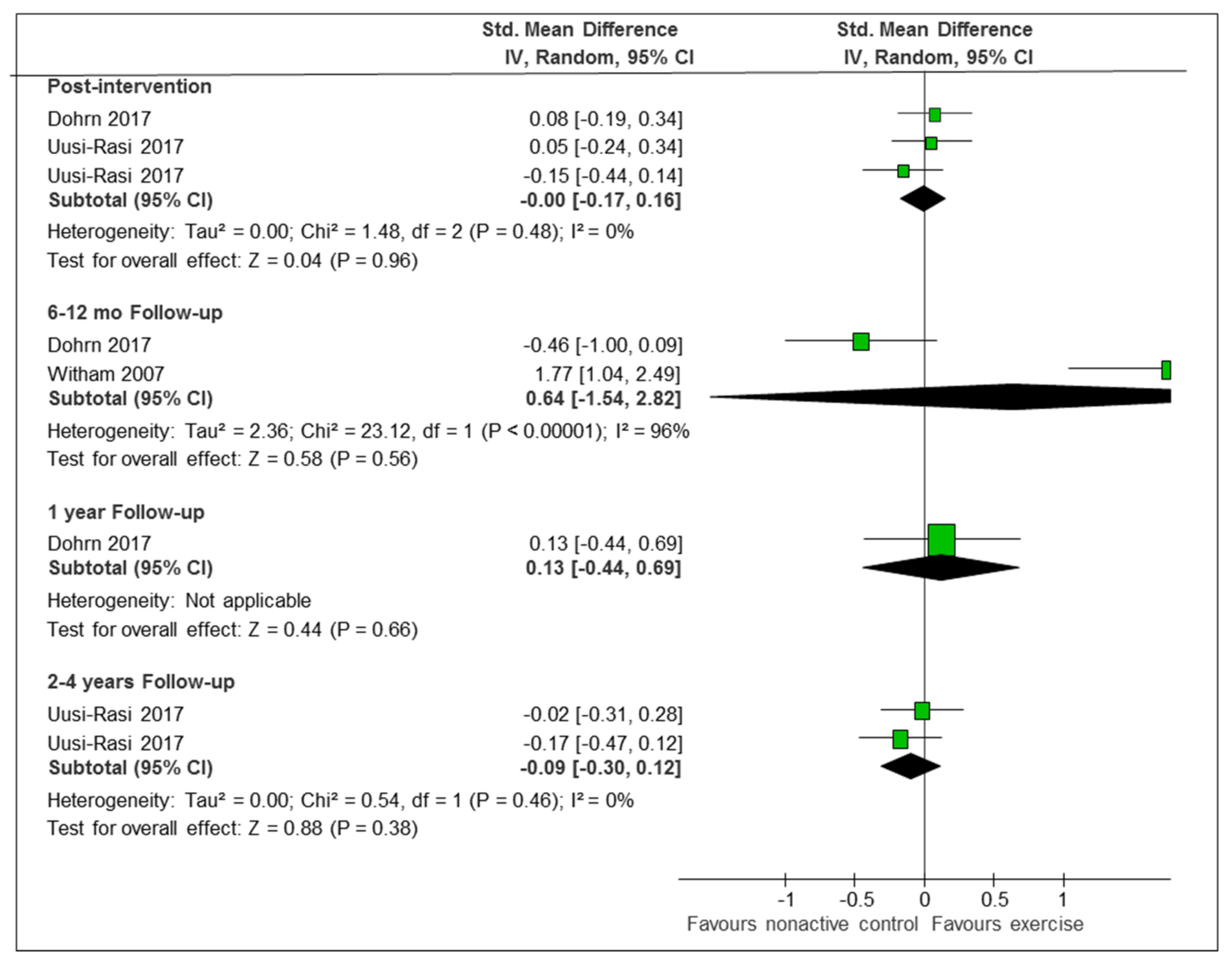
3.4. Comparison 2: Exercise-Based Intervention versus Non-Active Control
3.5. Reported Strategies to Enhance Long-Term Sustainable Maintenance of PA
4. Discussion
4.1. Mechanisms that Underpin our Main Finding
4.2. Strengths and Limitations
5. Conclusions
Data Statement
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Greenhalgh, T. How to Spread Good Ideas: A Systematic Review of the Literature on Diffusion, Dissemination, and Sustainability of Innovations in Health Service Delivery and Organization; Report for the National Coordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO); London University College: London, UK, 2004; p. 362. [Google Scholar]
- Scheirer, M.A.; Dearing, J.W. An Agenda for Research on the Sustainability of Public Health Programs. Am. J. Public Health 2011, 101, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Belala, N.; Clemson, L.; Boulton, E.; Hawley-Hague, H.; Becker, C.; Schwenk, M. Feasibility and Effectiveness of Intervention Programmes Integrating Functional Exercise into Daily Life of Older Adults: A Systematic Review. Gerontology 2018, 64, 172–187. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adherence to Long Term Therapies: Evidence for Action; World Health Organization Library: Geneva, Switzerland, 2003. [Google Scholar]
- Matthews, F.E.; Arthur, A.; Barnes, L.E.; Bond, J.; Jagger, C.; Robinson, L.; Brayne, C.; Medical Research Council Cognitive Function and Ageing Collaboration. A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: Results of the Cognitive Function and Ageing Study I and II. Lancet 2013, 382, 1405–1412. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef] [PubMed]
- Baumann, F.T.; Reike, A.; Reimer, V.; Schümann, M.; Hallek, M.; Taaffe, D.R.; Newton, R.U.; Galvao, D.A. Effects of physical exercise on breast cancer-related secondary lymphedema: A systematic review. Breast Cancer Res. Treat. 2018, 170, 1–13. [Google Scholar] [CrossRef]
- Stubbs, B.; Brefka, S.; Denkinger, M.D. What Works to Prevent Falls in Community-Dwelling Older Adults? Umbrella Review of Meta-analyses of Randomized Controlled Trials. Phys. Ther. 2015, 95, 1095–1110. [Google Scholar] [CrossRef] [Green Version]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Tada, A. Psychological effects of exercise on community-dwelling older adults. Clin. Interv. Aging 2018, 13, 271–276. [Google Scholar] [CrossRef]
- Motl, R.W.; McAuley, E. Physical Activity, Disability, and Quality of Life in Older Adults. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 299–308. [Google Scholar] [CrossRef]
- Santanasto, A.J.; Glynn, N.W.; Lovato, L.C.; Blair, S.N.; Fielding, R.A.; Gill, T.M.; Guralnik, J.M.; Hsu, F.-C.; King, A.C.; Strotmeyer, E.S.; et al. Effect of Physical Activity versus Health Education on Physical Function, Grip Strength and Mobility. J. Am. Geriatr. Soc. 2017, 65, 1427–1433. [Google Scholar] [CrossRef]
- Daskalopoulou, C.; Stubbs, B.; Kralj, C.; Koukounari, A.; Prince, M.; Prina, A. Physical activity and healthy ageing: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res. Rev. 2017, 38, 6–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bembom, O.; Van Der Laan, M.; Haight, T.; Tager, I. Leisure-time Physical Activity and All-cause Mortality in an Elderly Cohort. Epidemiology 2009, 20, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Ward, H.A.; Norat, T.; Luan, J.; May, A.M.; Weiderpass, E.; Sharp, S.J.; Overvad, K.; Østergaard, J.N.; Tjønneland, A.; et al. Physical activity and all-cause mortality across levels of overall and abdominal adiposity in European men and women: The European Prospective Investigation into Cancer and Nutrition Study (EPIC). Am. J. Clin. Nutr. 2015, 101, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Horton, R. Rethinking our approach to physical activity. Lancet 2012, 380, 189–190. [Google Scholar] [CrossRef]
- Hallal, P.C.; Bauman, A.E.; Heath, G.W.; Kohl, H.W., 3rd; Lee, I.M.; Pratt, M. Physical activity: More of the same is not enough. Lancet 2012, 380, 190–191. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Rethinking Development and Health: Findings from the Global Burden of Disease Study. Seattle. 2016. Available online: http://www.healthdata.org/policy-report/rethinking-development-and-health-findings-global-burden-disease-study (accessed on 21 October 2018).
- Federal Interagency Forum on Aging-Related Statistics. Older Americans 2016: Key Indicators of Well-Being; CreateSpace Independent Publishing Platform: Washington, DC, USA, 2016. [Google Scholar]
- Gomes, M.; Figueiredo, D.; Teixeira, L.; Poveda, V.; Paúl, C.; Santos-Silva, A.; Costa, E. Physical inactivity among older adults across Europe based on the SHARE database. Age Ageing 2017, 46, 71–77. [Google Scholar] [CrossRef]
- Sørensen, J.B.; Skovgaard, T.; Puggaard, L. Exercise on prescription in general practice: A systematic review. Scand. J. Prim. Health Care 2006, 24, 69–74. [Google Scholar] [CrossRef]
- Williams, N.H.; Hendry, M.; France, B.; Lewis, R.; Wilkinson, C. Effectiveness of exercise-referral schemes to promote physical activity in adults: Systematic review. Br. J. Gen. Pr. 2007, 57, 979–986. [Google Scholar] [CrossRef]
- Richards, J.; Hillsdon, M.; Thorogood, M. Face-to-face interventions for promoting physical activity. Cochrane Database Syst. Rev. 2013, 30, CD010392. [Google Scholar] [CrossRef]
- Morelhao, P.K.; Oliveira, C.B.; Franco, M.R. Interventions to increase physical activity among older adults (PEDro synthesis). Br. J. Sports Med. 2017, 51, 1375–1376. [Google Scholar] [CrossRef] [PubMed]
- Chase, J.A. Interventions to Increase Physical Activity among Older Adults: A Meta-Analysis. Gerontologist 2015, 55, 706–718. [Google Scholar] [CrossRef] [PubMed]
- Zubala, A.; MacGillivray, S.; Frost, H.; Kroll, T.; Skelton, D.A.; Gavine, A.; Gray, N.M.; Toma, M.; Morris, J. Promotion of physical activity interventions for community dwelling older adults: A systematic review of reviews. PLoS ONE 2017, 12, e0180902. [Google Scholar] [CrossRef] [PubMed]
- Chao, D.; Foy, C.G.; Farmer, D. Exercise adherence among older adults: Challenges and strategies. Control. Clin. Trials 2000, 21, 212–217. [Google Scholar] [CrossRef]
- Velicer, W.F.; Prochaska, J.O. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar]
- Bandura, A. Social Cognitive Theory: An Agentic Perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochrane-handbook.org (accessed on 15 July 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Hauer, K.; Pfisterer, M.; Schuler, M.; Bärtsch, P.; Oster, P. Two years later: A prospective long-term follow-up of a training intervention in geriatric patients with a history of severe falls. Arch. Phys. Med. Rehabil. 2003, 84, 1426–1432. [Google Scholar] [CrossRef]
- Karinkanta, S.; Heinonen, A.; Sievänen, H.; Uusi-Rasi, K.; Fogelholm, M.; Kannus, P. Maintenance of exercise-induced benefits in physical functioning and bone among elderly women. Osteoporos. Int. 2009, 20, 665–674. [Google Scholar] [CrossRef]
- McMahon, S.K.; Lewis, B.; Oakes, J.M.; Wyman, J.F.; Guan, W.; Rothman, A.J. Assessing the effects of interpersonal and intrapersonal behavior change strategies on physical activity in older adults: A factorial experiment. Ann. Behav. Med. 2017, 51, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Dohrn, I.-M.; Hagströmer, M.; Hellénius, M.-L.; Ståhle, A. Short- and Long-Term Effects of Balance Training on Physical Activity in Older Adults with Osteoporosis: A Randomized Controlled Trial. J. Geriatr. Phys. Ther. 2017, 40, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Uusi-Rasi, K.; Patil, R.; Karinkanta, S.; Kannus, P.; Tokola, K.; Lamberg-Allardt, C.; Sievänen, H. A 2-Year Follow-Up after a 2-Year RCT with Vitamin D and Exercise: Effects on Falls, Injurious Falls and Physical Functioning among Older Women. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2017, 72, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, E.; Unden, A.-L.; Ståhle, A.; Rydén, L.; Nordlander, R. Improved physical fitness and quality of life following training of elderly patients after acute coronary events. A 1 year follow-up randomized controlled study. Eur. Heart J. 1999, 20, 1475–1484. [Google Scholar] [Green Version]
- Hage, C.; Mattsson, E.; Ståhle, A. Long term effects of exercise training on physical activity level and quality of life in elderly coronary patients—A three- to six-year follow-up. Physiother. Res. Int. 2003, 8, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Beyer, N.; Simonsen, L.; Bülow, J.; Lorenzen, T.; Jensen, D.V.; Larsen, L.; Rasmussen, U.; Rennie, M.; Kjær, M. Old women with a recent fall history show improved muscle strength and function sustained for six months after finishing training. Aging Clin. Exp. Res. 2007, 19, 300–309. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Morris, K.S.; Motl, R.W.; Hu, L.; Konopack, J.F.; Elavsky, S. Long-term follow-up of physical activity behavior in older adults. Health Psychol. 2007, 26, 375–380. [Google Scholar] [CrossRef]
- Witham, M.D.; Argo, I.S.; Johnston, D.W.; Struthers, A.D.; McMurdo, M.E.T. Long-Term Follow-Up of Very Old Heart Failure Patients Enrolled in a Trial of Exercise Training. Am. J. Geriatr. Cardiol. 2007, 16, 243–248. [Google Scholar] [CrossRef]
- Rejeski, W.J.; Marsh, A.P.; Chmelo, E.; Prescott, A.J.; Dobrosielski, M.; Walkup, M.P.; Espeland, M.; Miller, M.E.; Kritchevsky, S. The Lifestyle Interventions and Independence for Elders Pilot (LIFE-P): 2-Year Follow-up. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2009, 64, 462–467. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Keogh, J.W.; Kolt, G.S.; Schofield, G.M. The long-term effects of a primary care physical activity intervention on mental health in low-active, community-dwelling older adults. Aging Ment. Health 2013, 17, 766–772. [Google Scholar] [CrossRef]
- Hars, M.; Herrmann, F.R.; Fielding, R.A.; Reid, K.F.; Rizzoli, R.; Trombetti, A. Long-Term Exercise in Older Adults: 4-Year Outcomes of Music-Based Multitask Training. Calcif. Tissue Int. 2014, 95, 393–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, N.M.; Staal, J.B.; van der Wees, P.J.; Adang, E.M.; Akkermans, R.; Olde Rikkert, M.G.; Nijhuis-van der Sanden, M.W. Patient-centred physical therapy is (cost-) effective in increasing physical activity and reducing frailty in older adults with mobility problems: A randomized controlled trial with 6 months follow-up. J. Cachexia Sarcopenia Muscle 2016, 7, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Martin-Borràs, C.; Giné-Garriga, M.; Puig-Ribera, A.; Martin, C.; Solà, M.; Cuesta-Vargas, A.I.; Losada, J.A.; Albarrilla, E.; Muñoz, M.; Castillo, E.; et al. A new model of exercise referral scheme in primary care: Is the effect on adherence to physical activity sustainable in the long term? A 15-month randomised controlled trial. BMJ Open 2018, 8, e017211. [Google Scholar] [CrossRef] [PubMed]
- Patil, R.; Karinkanta, S.; Tokola, K.; Kannus, P.; Sievänen, H.; Uusi-Rasi, K. Effects of Vitamin D and Exercise on the Wellbeing of Older Community-Dwelling Women: A Randomized Controlled Trial. Gerontology 2016, 62, 401–408. [Google Scholar] [CrossRef]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef]
- Finegood, D.; Johnston, L.; Steinberg, M.; Matteson, C.L.; Deck, P. Complexity, systems thinking, and health behavior change. In Health Behavior Change in Populations; Kahan, S., Gielen, A.C., Fagan, P.J., Lawrence, W.G., Eds.; Oxford University Press: New York, NY, USA, 2011; pp. 208–236. [Google Scholar]
- Green, L.W.; O’Neill, M.; Westphal, M.; Morisky, D.; Editors, G. The Challenges of Participatory Action Research for Health Promotion. Promot. Educ. 1996, 3, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef]
- Conn, V.S.; Minor, M.A.; Burks, K.J.; Rantz, M.J.; Pomeroy, S.H. Integrative Review of Physical Activity Intervention Research with Aging Adults. J. Am. Geriatr. Soc. 2003, 51, 1159–1168. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Cohen, J.S.; Edmunds, J.M.; Brodman, D.M.; Benjamin, C.L.; Kendall, P.C.; Wolk, C.B. Using Self-Monitoring: Implementation of Collaborative Empiricism in Cognitive-Behavioral Therapy. Cogn. Behav. Pr. 2013, 20, 419–428. [Google Scholar] [CrossRef]
- Pearson, E.S. Goal setting as a health behavior change strategy in overweight and obese adults: A systematic literature review examining intervention components. Patient Educ. Couns. 2012, 87, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Chase, J.D. Methodological challenges in physical activity research among older adults. West J. Nurs. Res. 2013, 35, 76–97. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Bull, S.S.; Piette, J.D.; Steiner, J. Interactive behavior change technology: A partial solution to the competing demands of primary care. Am. J. Prev. Med. 2004, 27 (Suppl. 2), 80–87. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, R.T.; Deyo, R.A.; LoGerfo, J.P. Prompting primary care providers to increase community exercise referrals for older adults: A randomized trial. J. Am. Geriatr. Soc. 2005, 53, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Green, B. Effectiveness of telephone support in increasing physical activity levels in primary care patients. Am. J. Prev. Med. 2002, 22, 177–183. [Google Scholar] [CrossRef]
- Piwek, L.; Ellis, D.A.; Andrews, S.; Joinson, A. The Rise of Consumer Health Wearables: Promises and Barriers. PLoS Med. 2016, 13, e1001953. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Davis, K.K.; Rogers, R.J.; King, W.C.; Marcus, M.D.; Helsel, D.; Rickman, A.D.; Wahed, A.S.; Belle, S.H. Effect of Wearable Technology Combined with a Lifestyle Intervention on Long-Term Weight Loss: The IDEA Randomized Clinical Trial. JAMA 2016, 316, 1161–1171. [Google Scholar] [CrossRef]
- Brawley, L.R.; Rejeski, W.; King, A.C. Promoting physical activity for older adults: The challenges for changing behavior. Am. J. Prev. Med. 2003, 25, 172–183. [Google Scholar] [CrossRef]
- Sartini, C.; Wannamethee, S.G.; Iliffe, S.; Morris, R.W.; Ash, S.; Lennon, L.; Whincup, P.H.; Jefferis, B.J. Diurnal patterns of objectively measured physical activity and sedentary behaviour in older men. BMC Public Health 2015, 15, 609. [Google Scholar] [CrossRef]
- Clemson, L.; Fiatarone Singh, M.A.; Bundy, A.; Cumming, R.G.; Manollaras, K.; O’Loughlin, P.; Black, D. Integration of balance and strength training into daily life activity to reduce rate of falls in older people (the LiFE study): Randomised parallel trial. BMJ 2012, 345, e4547. [Google Scholar] [CrossRef]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; Dimatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar] [PubMed]
- Cumming, R.G.; Klineberg, R.J. A study of the reproducibility of long-term recall in the elderly. Epidemiology 1994, 5, 116–119. [Google Scholar] [CrossRef] [PubMed]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sansano-Nadal, O.; Giné-Garriga, M.; Brach, J.S.; Wert, D.M.; Jerez-Roig, J.; Guerra-Balic, M.; Oviedo, G.; Fortuño, J.; Gómara-Toldrà, N.; Soto-Bagaria, L.; et al. Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Environ. Res. Public Health 2019, 16, 2527. https://doi.org/10.3390/ijerph16142527
Sansano-Nadal O, Giné-Garriga M, Brach JS, Wert DM, Jerez-Roig J, Guerra-Balic M, Oviedo G, Fortuño J, Gómara-Toldrà N, Soto-Bagaria L, et al. Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. International Journal of Environmental Research and Public Health. 2019; 16(14):2527. https://doi.org/10.3390/ijerph16142527
Chicago/Turabian StyleSansano-Nadal, Oriol, Maria Giné-Garriga, Jennifer S. Brach, David M. Wert, Javier Jerez-Roig, Myriam Guerra-Balic, Guillermo Oviedo, Jesús Fortuño, Natàlia Gómara-Toldrà, Luis Soto-Bagaria, and et al. 2019. "Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" International Journal of Environmental Research and Public Health 16, no. 14: 2527. https://doi.org/10.3390/ijerph16142527