Sociodemographic Factors Associated with the Knowledge and Use of Birth Control Methods in Adolescents before and after Pregnancy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Subjects
2.2. Assessments
2.3. Operational Definitions
2.4. Ethical Considerations
2.5. Statistical Analyses
3. Results
3.1. Sample Characteristics
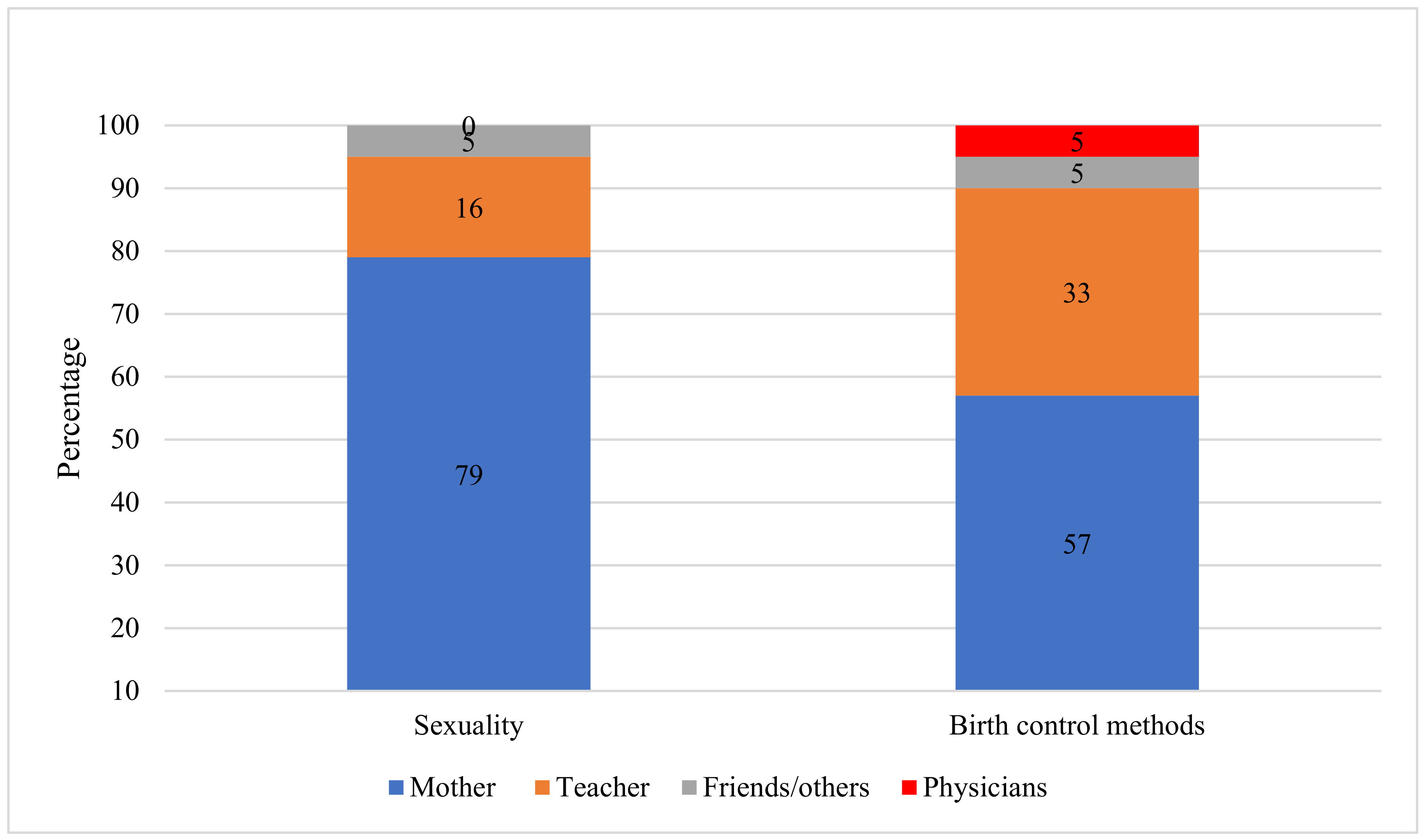
3.2. Knowledge about Sexuality and Birth Control Methods
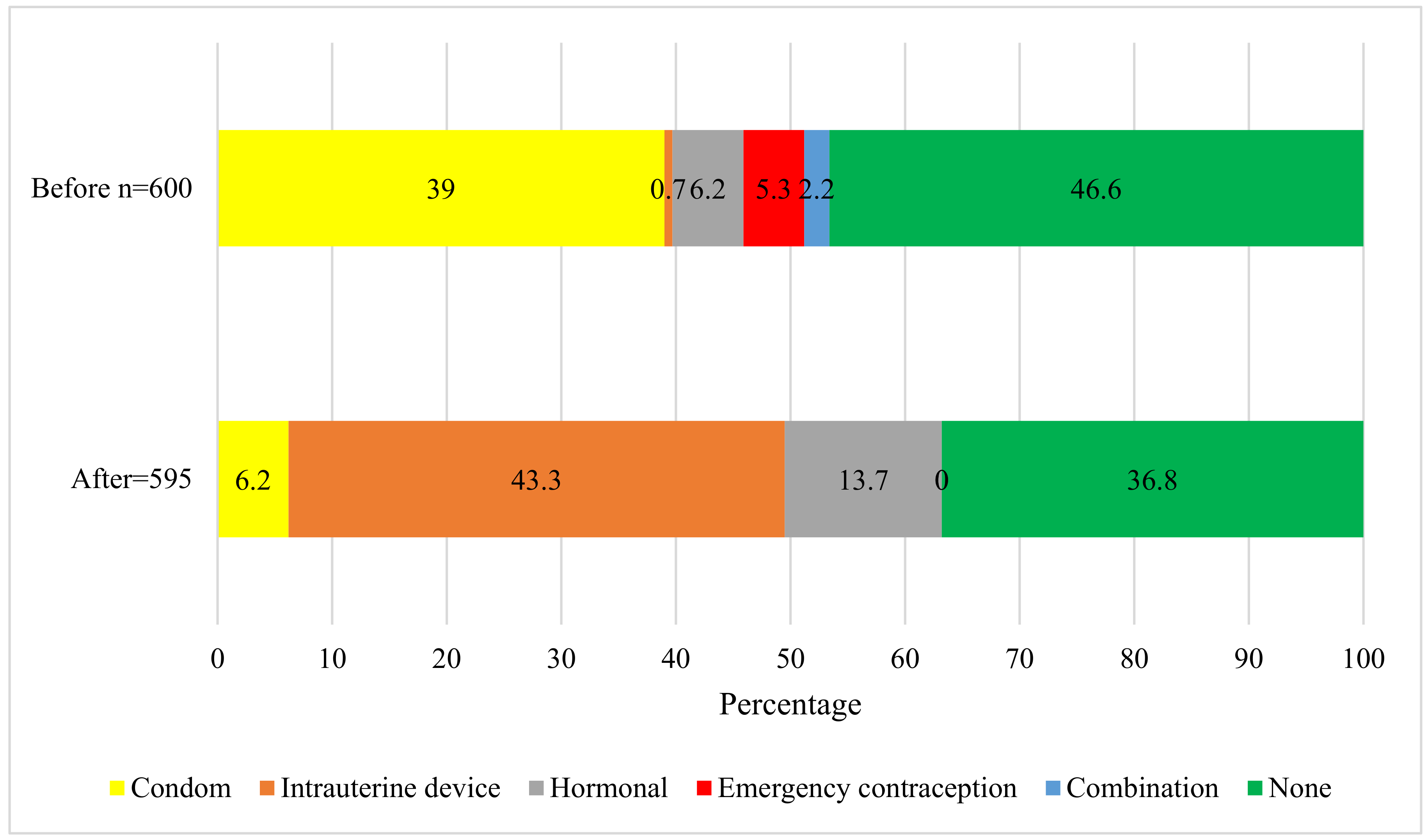
3.3. Use of Birth Control Methods before and after Pregnancy
4. Discussion
4.1. Sociodemographic and Initiation of Sexual Life
4.2. Information about Sexuality and Birth Control Methods
4.3. Use of Birth Control Methods
4.4. Postpartum Use of Birth Control Methods
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ENSANUT | Encuesta Nacional de Salud y Nutrición (National of Health and Nutrition Survey) |
| INPer | Instituto Nacional de Perinatología (National Institute of Perinatology) |
| WHO | World Health Organization |
| Ethics approval and consent to participate | Ethical approval for the study was granted by the National Institute of Perinatology Review Board (registration number 212250-49451). Written informed consent to participate in the study, was obtained before enrollment. |
References
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.B.; Gemmill, A.; Fat, DM.; Boerma, T.; Temmerman, M.; Mathers, C.; et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet 2016, 387, 462–474. [Google Scholar]
- Trends in Maternal Mortality: 1990 to 2015: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division; World Health Organization: Geneva, Switzerland, 2015.
- WHO/Adolescent Birth Rate. Global Health Observatory (GHO) Data. Globally, the Adolescent Birth Rate in 2015 Was 44.1 per 1000 Women Aged 15–19 years. Available online: http://www.who.int/gho/maternal_health/reproductive_health/adolescent_fertility/en/ (accessed on 25 October 2017).
- Rios-Zertuche, D.; Blanco, L.C.; Zúñiga-Brenes, P.; Palmisano, E.B.; Colombara, D.V.; Mokdad, A.H.; Iriarte, E. Contraceptive knowledge and use among women living in the poorest areas of five Mesoamerican countries. Contraception 2017, 95, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Maravilla, J.C.; Betts, K.S.; Couto, E.; Cruz, C.; Alati, R. Factors influencing repeated teenage pregnancy: A review and meta-analysis. Am. J. Obstet. Gynecol. 2017, 217, 527–545. [Google Scholar] [CrossRef] [PubMed]
- Borovac-Pinheiro, A.; Surita, F.G.; D’Annibale, A.; Pacagnella, R.C.; Pinto ESilva, J.L. Adolescent contraception before and after pregnancy-choices and challenges for the Future. Rev. Bras. Ginecol. Obstet. 2016, 38, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Shah, I.H.; Benova, L. A Fresh Look at the Level of Unmet Need for Family Planning in the Postpartum Period, Its Causes and Program Implications. Int. Perspect. Sex. Reprod. Health 2015, 41, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, G.R.; Bravo, P.E.; Vivaldi, M.I.M.; Manríquez, I.P.; Pérez, T.G. Adolescents’ access to contraception: Perceptions of health workers in Huechuraba, Chile. Rev. Panam. Salud Publica 2017, 41, e77. [Google Scholar] [PubMed]
- Yago Simón, T.; Tomás-Aznar, C. Sociodemographic and Clinical Data Predicting Unplanned Pregnancy in Young 13 to 24 Years, Spain. Rev. Esp. Salud Pública 2014, 88, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Villalobos-Hernández, A.; Campero, L.; Suárez-Lopez, L.; Atienzo, E.E.; Estrada, F.; De la Vara-Salazar, E. Teen pregnancy and educational gaps: Analysis of a national survey in Mexico. Salud Publica Mex. 2015, 57, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Almeida Mda, C.; Aquino, E.M. Adolescent pregnancy and completion of basic education: A study of young people in three state capital cities in Brazil. Cad Saude Publica 2011, 27, 2386–2400. [Google Scholar] [CrossRef]
- Finer, L.B.; Philbin, J.M. Sexual initiation, contraceptive use, and pregnancy among young adolescents. Pediatrics 2013, 131, 886–891. [Google Scholar] [CrossRef]
- Saavedra-Avendano, B.; Andrade-Romo, Z.; Rodriguez, M.I.; Darney, B.G. Adolescents and Long-Acting Reversible Contraception: Lessons from Mexico. Matern. Child Health J. 2017, 21, 1724–1733. [Google Scholar] [CrossRef] [PubMed]
- Muanda, M.; Gahungu Ndongo, P.; Taub, L.D.; Bertrand, J.T. Barriers to Modern Contraceptive Use in Kinshasa, DRC. PLoS ONE 2016, 11, e0167560. [Google Scholar] [CrossRef] [PubMed]
- Sedgh, G.; Finer, L.B.; Bankole, A.; Eilers, M.A.; Singh, S. Adolescent pregnancy, birth, and abortion rates across countries: Levels and recent trends. J. Adolesc. Health 2015, 56, 223–230. [Google Scholar] [CrossRef]
- Bongaarts, J.; Mensch, B.S.; Blanc, A.K. Trends in the age at reproductive transitions in the developing world: The role of education. Popul. Stud. (Camb) 2017, 71, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística y Geografía (INEGI). Natalidad. Porcentaje de nacimientos registrados de madres adolescentes (menores de 20 años). Available online: http://www.beta.inegi.org.mx/temas/natalidad/ (accessed on 25 October 2017).
- Gayet, C.; Gutiérrez, J.P. Sexual debut in Mexico: A comparison of household national surveys. Salud Publica Mex. 2014, 56, 638–647. [Google Scholar] [CrossRef]
- Blanquet-García, J.; Montoya-Cázarez, A.; Carranza-Lira, S. Sociodemographic characteristics of the pregnant adolescent in a high specialty hospital. Rev. Med. Inst. Mex. Seguro Soc. 2016, 54 (Suppl. 3), S238–S241. [Google Scholar] [PubMed]
- Chigona, A.; Chetty, R. Teen mothers and schooling: Lacunae and challenges. S. Afr. J. Educ. 2008, 28, 261–281. [Google Scholar]
- Rose, E.M.; Rajasingam, D.; Derkenne, R.C.; Mitchell, V.; Ramlall, A.A. Reproductive health knowledge, attitudes and practices of adolescents attending an obstetric unit in Georgetown, Guyana. J. Fam. Plan. Reprod. Health Care 2016, 42, 116–118. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs, Population Division. Trends in Contraceptive Use Worldwide 2015 (ST/ESA/SER.A/349). Available online: http://www.un.org/en/development/desa/population/publications/pdf/family/trendsContraceptiveUse2015Report.pdf (accessed on 25 October 2017).
- Gutiérrez, J.P.; Rivera-Dommarco, J.; Shamah-Levy, T.; Villalpando-Hernández, S.; Franco, A.; Cuevas-Nasu, L.; Romero-Martínez, M.; Hernández-Ávila, M. National Health and Nutrition Survey 2012. National Results; National Public Health Institute: Cuernavaca, Mexico, 2012; Available online: http://ensanut.insp.mx/informes/ENSANUT2012ResultadosNacionales.pdf (accessed on 25 October 2017).
- de Castro, F.; Place, J.M.; Allen-Leigh, B.; Barrientos-Gutierrez, T.; Dues, K.; Eternod Arámburu, M.; Hernández-Avila, M. Perceptions of adolescent’ simulated clients’ on barriers to seeking contraceptive services in health centers and pharmacies in Mexico. Sex. Reprod. Health 2018, 16, 118–123. [Google Scholar] [CrossRef]
- Schor, N.; Ferreira, A.F.; Machado, V.L.; França, A.P.; Pirotta, K.C.; Alvarenga, A.T.; Siqueira, A.A. Women and contraception: Knowledge and use of contraceptive methods. Cad Saude Publica 2000, 16, 377–384. [Google Scholar] [CrossRef]
- Espejo, X.; Tsunechiro, M.A.; Osis, M.J.; Duarte, G.A.; Bahamondese, L.; de Sousa, M.H. Knowledge adequacy on contraceptives among women in Campinas. Brazil. Rev. Saude Publica 2003, 37, 583–590. [Google Scholar] [CrossRef]
- Guzzo, K.B.; Hayford, S.R. Adolescent Reproductive and Contraceptive Knowledge and Attitudes and Adult Contraceptive Behavior. Matern. Child Health J. 2018, 22, 32–40. [Google Scholar] [CrossRef]
- Martins, L.B.; Costa-Paiva, L.; Osis, M.J.; Sousa, M.H.; Pinto Neto, A.M.; Tadini, V. Knowledge of contraceptive methods among adolescent students. Rev. Saude Publica 2006, 40, 57–64. [Google Scholar] [CrossRef]
- Persona, L.; Shimo, A.K.; Tarallo, M.C. Profile of adolescents with repeated pregnancies attended at a prenatal clinic. Revista Latino-Americana de Enfermagem 2004, 12, 745–750. [Google Scholar] [CrossRef]
- Sámano, R.; Martinez-Rojano, H.; Robichaux, D.; Rodríguez-Ventura, A.L.; Sánchez-Jiménez, B.; de la Luz Hoyuela, M.; Godínez, E.; Segovia, S. Family context and individual situation of teens before, during and after pregnancy in Mexico City. BMC Pregnancy Childbirth 2017, 17, 382. [Google Scholar] [CrossRef] [Green Version]
- Socioeconomic Level Index of the Mexican Association of Market Research and Public Opinion Agencies (AMAI) September 2014 AMAI Regulation NSE 8 × 7. Available online: www.amai.org/NSE/NivelSocioeconomicoAMAI.pdf (accessed on 25 October 2017).
- National Population Council (Mexico), Secretariat of the Interior (SEGOB) Mexico National Survey of Demographic Dynamics 2014—CONAPO. Available online: http://ghdx.healthdata.org/record/mexico-national-survey-demographic-dynamics-2014-conapo (accessed on 25 October 2017).
- Rengifo-Reina, H.A.; Córdoba-Espinal, A.; Serrano-Rodriguez, M. Adolescents’ sexual and reproductive health knowledge and Practice in a provincial Colombian town. Rev. Salud Publica 2012, 14, 558–569. [Google Scholar]
- Samandari, G.; Speizer, I.S. Adolescent sexual behavior and reproductive outcomes in Central America: Trends over the past two decades. Int. Perspect. Sex. Reprod. Health 2010, 36, 26–35. [Google Scholar] [CrossRef]
- Gilliam, M.L.; Neustadt, A.; Whitaker, A.; Kozloski, M. Familial, cultural and psychosocial influences of use of effective methods of contraception among Mexican-American adolescents and young adults. J. Pediatr. Adolesc. Gynecol. 2011, 24, 79–84. [Google Scholar] [CrossRef]
- Li, C.; Cheng, Z.; Wu, T.; Liang, X.; Gaoshan, J.; Li, L.; Hong, P.; Tang, K. The relationships of school-based sexuality education, sexual knowledge and sexual behaviors—A study of 18,000 Chinese college students. Reprod. Health 2017, 14, 103. [Google Scholar] [CrossRef]
- Kemigisha, E.; Bruce, K.; Nyakato, V.N.; Ruzaaza, G.N.; Ninsiima, A.B.; Mlahagwa, W.; Leye, E.; Coene, G.; Michielsen, K. Sexual health of very young adolescents in South Western Uganda: A cross-sectional assessment of sexual knowledge and behavior. Reprod. Health 2018, 15, 148. [Google Scholar] [CrossRef]
- Rodríguez-Vignoli, J.; Cavenaghi, S. Adolescent and Youth Fertility and Social Inequality in Latin America and the Caribbean: What Role Has Education Played? Genus 2014, 70, 1–25. [Google Scholar]
- Schaalma, H.P.; Abraham, C.; Gillmore, M.R.; Kok, G. Sex education as health promotion: What does it take? Arch. Sex. Behav. 2004, 33, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Lys, C.; Gesink, D.; Strike, C.; Larkin, J. Social Ecological Factors of Sexual Subjectivity and Contraceptive Use and Access Among Young Women in the Northwest Territories, Canada. J. Sex. Res. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Waluyanti, F.T.; Mulyadi, B.; Nursasi, A.Y. The influence of health training on teachers and students’ knowledge of adolescent reproductive health. Enferm. Clin. 2018, 28 (Suppl. 1), 332–336. [Google Scholar] [CrossRef]
- Atienzo, E.E.; Campero, L.; Estrada, F.; Rouse, C.; Walker, D. Interventions involving parents in order to impact adolescent sexual behavior. Salud Publica Mex. 2011, 53, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Swain, C.R.; Ackerman, L.K.; Ackerman, M.A. The influence of individual characteristics and contraceptive beliefs on parent-teen sexual communications: A structural model. J. Adolesc. Health 2006, 38, 753.e9–753.e18. [Google Scholar] [CrossRef]
- Grad, A.I.; Senilă, S.C.; Cosgarea, R.; Tataru, A.D.; Vesa, S.C.; Vica, M.L.; Matei, H.V.; Ungureanu, L. Sexual Behaviors, Attitudes, and Knowledge about Sexually Transmitted Infections: A Cross-sectional Study in Romania. Acta Dermatovenerol. Croat. 2018, 26, 25–32. [Google Scholar] [PubMed]
- Hamm, M.; Evans, M.; Miller, E.; Browne, M.; Bell, D.; Borrero, S. “It’s her body”: Low-income men’s perceptions of limited reproductive agency. Contraception 2018. [Google Scholar] [CrossRef] [PubMed]
- Allen-Leigh, B.; Villalobos-Hernández, A.; Hernández-Serrato, M.I.; Suárez, L.; De la Vara, E.; De Castro, F.; Schiavon-Ermani, R. Use of contraception and family planning in adolescent and adult women in Mexico. Salud Publica Mex. 2013, 55 (Suppl. 2), S235–S240. [Google Scholar] [CrossRef] [PubMed]
- Bahamondes, L.; Makuck my Monteiro, I.; Marin, V.; Lynen, R. Knowledge and attitudes of Latin American obstetricians and gynecologists regarding intrauterine contraceptives. Int. J. Women’s Health 2015, 16, 717–722. [Google Scholar] [CrossRef]
- Bahamondes, L.; Lira-Plascencia, J.; Martin, R.; Marin, V.; Makuch, M.Y. Knowledge and attitudes of Latin American gynecologists regarding unplanned pregnancy and use of combined oral contraceptives. Int. J. Womens Health 2015, 7, 485–491. [Google Scholar] [CrossRef] [Green Version]
- Shams, M.; Parhizkar, S.; Mousavizadeh, A.; Majdpour, M. Mothers’ views about sexual health education for their adolescent daughters: A qualitative study. Reprod. Health 2017, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Ministry of the Interior. National Strategy for the Prevention of Pregnancy in Adolescents. 2014. Available online: https://www.gob.mx/cms/uploads/attachment/file/55979/ENAPEA_0215.pdf (accessed on 25 October 2017).
- Abraham, M.; Zhao, Q.; Peipert, J.F. Young Age, Nulliparity, and Continuation of Long-Acting Reversible Contraceptive Methods. Obstet. Gynecol. 2015, 126, 823–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darney, B.G.; Sosa-Rubi, S.G.; Servan-Mori, E.; Rodriguez, M.I.; Walker, D.; Lozano, R. The relationship of age and place of delivery with postpartum contraception prior to discharge in Mexico: A retrospective cohort study. Contraception 2016, 93, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Users n = 318 | No Users n = 282 | p-Value | |
|---|---|---|---|---|
| Mean ± SD* | Min-max | |||
| Age (years) | 15.4 ± 1 | 15.2 ± 1 | 11–19 | 0.046 |
| Age at menarche (years) | 11.8 ± 1. | 11.6 ± 1 | 8–15 | 0.051 |
| Initiation of prenatal care (weeks of gestation) | 16.2 ± 5 | 12 (8–16) | 9–37 | 0.491 |
| Initiation of sexual life (years) | 14.5 ± 1.1 | 14.4 ± | 10–18 | 0.114 |
| Number of sexual partners ** | 1 (1,1) | 1 (1,1) | 1–5 | 0.694 |
| Age of the mother of the adolescent (years) ** | 39 (36–46) | 38(35–43) | 29–58 | 0.722 |
| Age of the father of the adolescent (years) ** | 41 (37–46) | 42 (37–46) | 29–68 | 0.709 |
| Age of the adolescent’s mother at her first pregnancy (years) ** | 20 (18–23) | 19 (17–23) | 14–39 | 0.799 |
| Age of the adolescent’s father at his first child (years) ** | 22 (19–25) | 23 (20–26) | 15–54 | 0.322 |
| Age of adolescent’s partner (years) ** | 18 (17–20) | 18 (16–19) | 17–43 | 0.063 |
| Users n = 318 (53%) | Non-Users n = 282 (47%) | p-Value * | Chi-Value | |
|---|---|---|---|---|
| Risk of pregnancy | 308 (97) | 265 (94) | 0.134 | 1.187 |
| The importance of self-care | 318 (100) | 265 (94) | 0.003 | 13.791 |
| The importance of being responsible | 318 (100) | 270 (96) | 0.001 | 15.588 |
| The possibility of infection by HIV | 308 (97) | 268 (95) | 0.001 | 16.306 |
| Birth control methods | 315 (99) | 26 (95) | 0.029 | 6.058 |
| Variables | Before Pregnancy | After Pregnancy | |||||
|---|---|---|---|---|---|---|---|
| Users n = 318 | Non-Users n = 282 | p-Value * | Users n = 382 | Non-Users n = 213 | p-Value * | ||
| Level of education | Low | 154 (52) | 214 (71) | 0.001 | 224 (59) | 143 (67) | 0.041 |
| High | 143 (48) | 82 (29) | 158 (41) | 70 (33) | |||
| Educational lag | No | 212 (71) | 155 (51) | 0.001 | 253 (66) | 113 (53) | 0.002 |
| Yes | 85 (29) | 148 (49) | 129 (34) | 100 (47) | |||
| Student | Yes | 102 (34) | 43 (14) | 0.001 | 119 (31) | 26 (12) | 0.001 |
| No | 195 (66) | 260 (86) | 263 (68) | 187 (88) | |||
| Source of information about birth control methods | Mother | 190 (60) | 147 (52) | 0.034 | 221 (58) | 117 (55) | 0.490 |
| Other | 127 (40) | 135 (48) | 161 (42) | 96 (45) | |||
| Occupation of the mother | Housewife | 168 (58) | 139 (51) | 0.042 | 215 (56) | 110 (52) | 0.276 |
| Employee | 119 (41) | 134 (49) | 167 (44) | 103 (48) | |||
| Socioeconomic level | Average or slightly below | 214 (67) | 177 (63) | 0.141 | 265 (69) | 124 (58) | 0.004 |
| Low | 104 (32) | 105 (37) | 117 (31) | 89 (42) | |||
| Family structure | Nuclear | 207 (65) | 166 (59) | 0.093 | 242 (63) | 126 (59) | 0.312 |
| Other | 111 (35) | 122 (41) | 140 (37) | 87 (41) | |||
| Age of initiation of sexual life | ≥15 years | 181 (57) | 146 (52) | 0.137 | 209 (55) | 101 (47) | 0.088 |
| <15 years | 136 (43) | 135 (48) | 173 (45) | 112 (53) | |||
| Age | ≥15 years | 197 (62) | 124 (44) | 0.001 | 199 (52) | 106 (50) | 0.323 |
| <15 years | 121 (38) | 158 (56) | 183 (48) | 107 (50) | |||
| Planned pregnancy | 64 (22) | 62 (19) | 0.171 | 81 (79) | 45 (21) | 0.981 | |
| Variables | Before Pregnancy | After Pregnancy | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| <15 years old | 1.950 | 1.284–2.973 | 0.002 | 1.084 | 0.701–1.679 | 0.716 |
| Low level of education | 1.578 | 1.033–2.410 | 0.035 | 1.173 | 0.717–1.842 | 0.489 |
| Drop-out of school | 2.824 | 1.796–4.440 | <0.001 | 2.823 | 1667–4.780 | <0.001 |
| Educational lag | 2.157 | 1.442–3.227 | <0.001 | 1.362 | 0.952–2.056 | 0.141 |
| Information from someone different to the mother about birth control methods | 1.054 | 1.009–1.102 | 0.019 | 0.994 | 0.994–1.039 | 0.799 |
| Did not use a birth control method before pregnancy | 2.392 | 1.599–3.578 | <0.001 | |||
| Constant | 0.019 | <0.001 | 0.116 | <0.001 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sámano, R.; Martínez-Rojano, H.; Chico-Barba, G.; Sánchez-Jiménez, B.; Sam-Soto, S.; Rodríguez-Ventura, A.L.; Mejía-Luna, L.; Sclavo-Melo, S. Sociodemographic Factors Associated with the Knowledge and Use of Birth Control Methods in Adolescents before and after Pregnancy. Int. J. Environ. Res. Public Health 2019, 16, 1022. https://doi.org/10.3390/ijerph16061022
Sámano R, Martínez-Rojano H, Chico-Barba G, Sánchez-Jiménez B, Sam-Soto S, Rodríguez-Ventura AL, Mejía-Luna L, Sclavo-Melo S. Sociodemographic Factors Associated with the Knowledge and Use of Birth Control Methods in Adolescents before and after Pregnancy. International Journal of Environmental Research and Public Health. 2019; 16(6):1022. https://doi.org/10.3390/ijerph16061022
Chicago/Turabian StyleSámano, Reyna, Hugo Martínez-Rojano, Gabriela Chico-Barba, Bernarda Sánchez-Jiménez, Selene Sam-Soto, Ana Lilia Rodríguez-Ventura, Laura Mejía-Luna, and Sylvia Sclavo-Melo. 2019. "Sociodemographic Factors Associated with the Knowledge and Use of Birth Control Methods in Adolescents before and after Pregnancy" International Journal of Environmental Research and Public Health 16, no. 6: 1022. https://doi.org/10.3390/ijerph16061022