Health Seeking Behavior among Rural Left-Behind Children: Evidence from Shaanxi and Gansu Provinces in China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
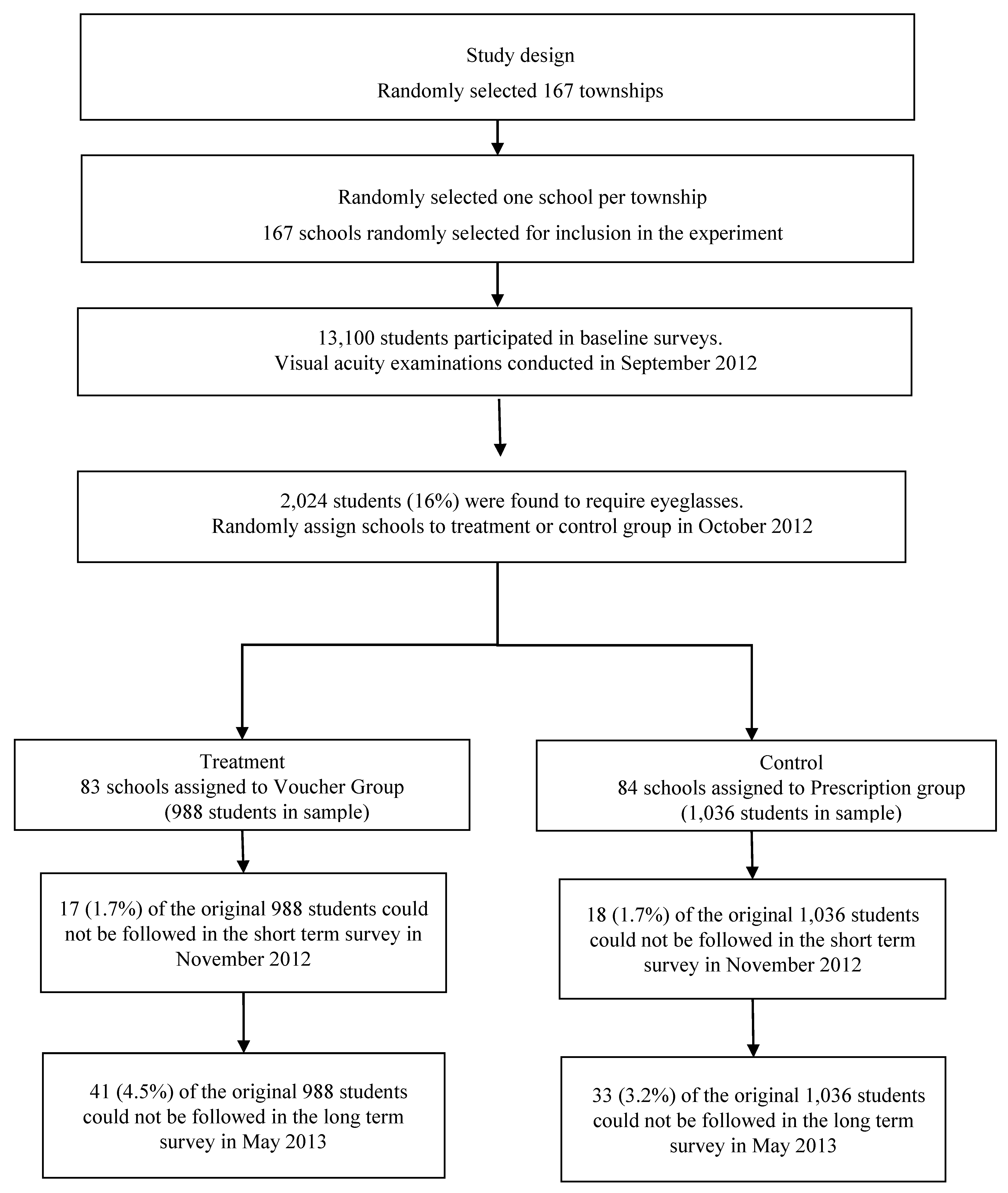
2.1. Study Area and Sampling Technique
2.2. Data Collection
2.2.1. Baseline Survey
2.2.2. Vision Examination
2.2.3. Eyeglasses Uptake and Usage
2.3. Experimental Design
2.4. Tests for Balance and Attrition Bias
2.5. Statistical Approach
3. Results
3.1. Eyeglasses Usage at the Time of Baseline among Left-Behind and Non-Left-Behind Students with Poor Vision
3.2. Average Impacts of Providing Voucher on Student Eyeglasses Uptake and Usage
3.3. Heterogeneous Effects on Left-Behind Children
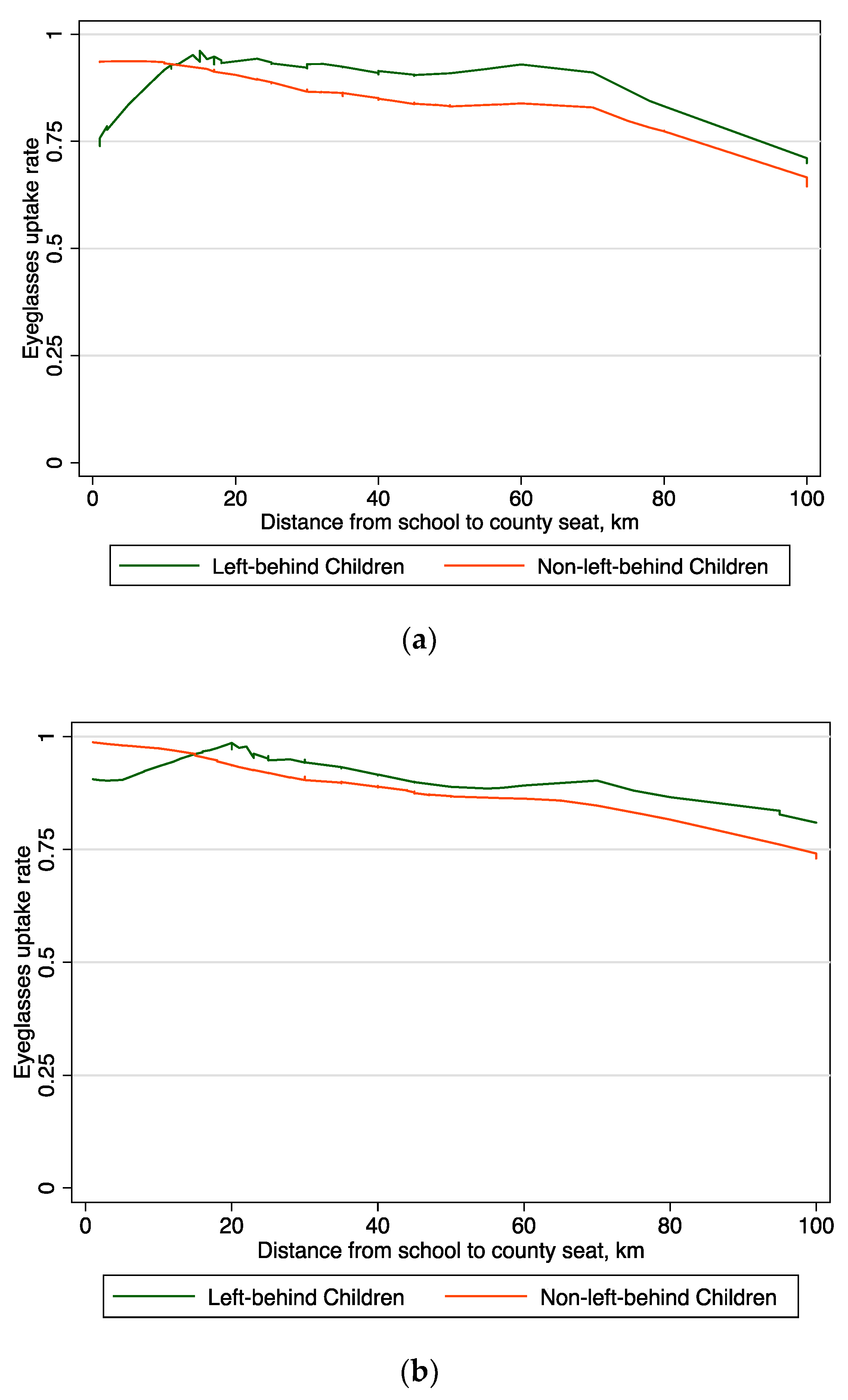
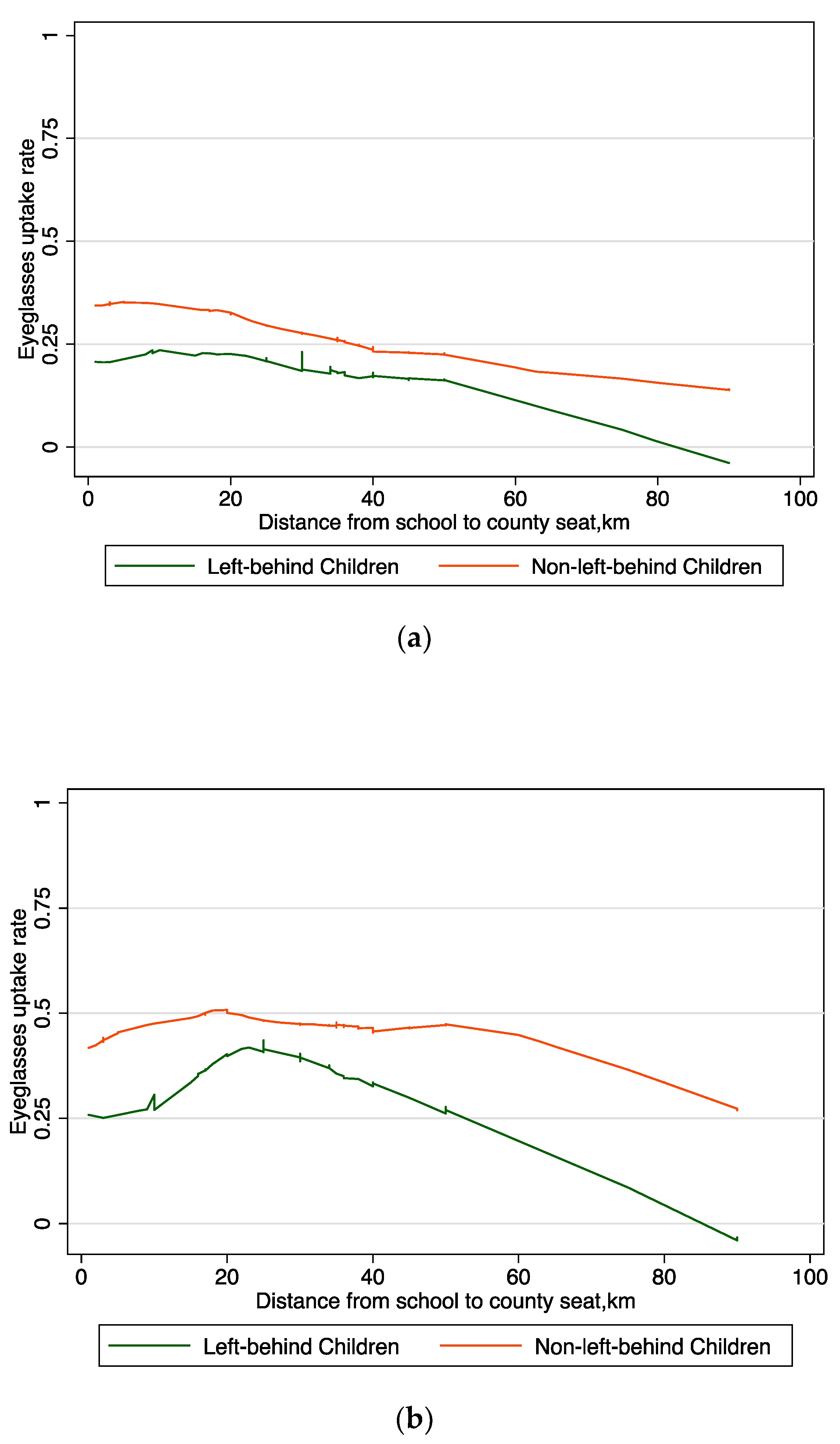
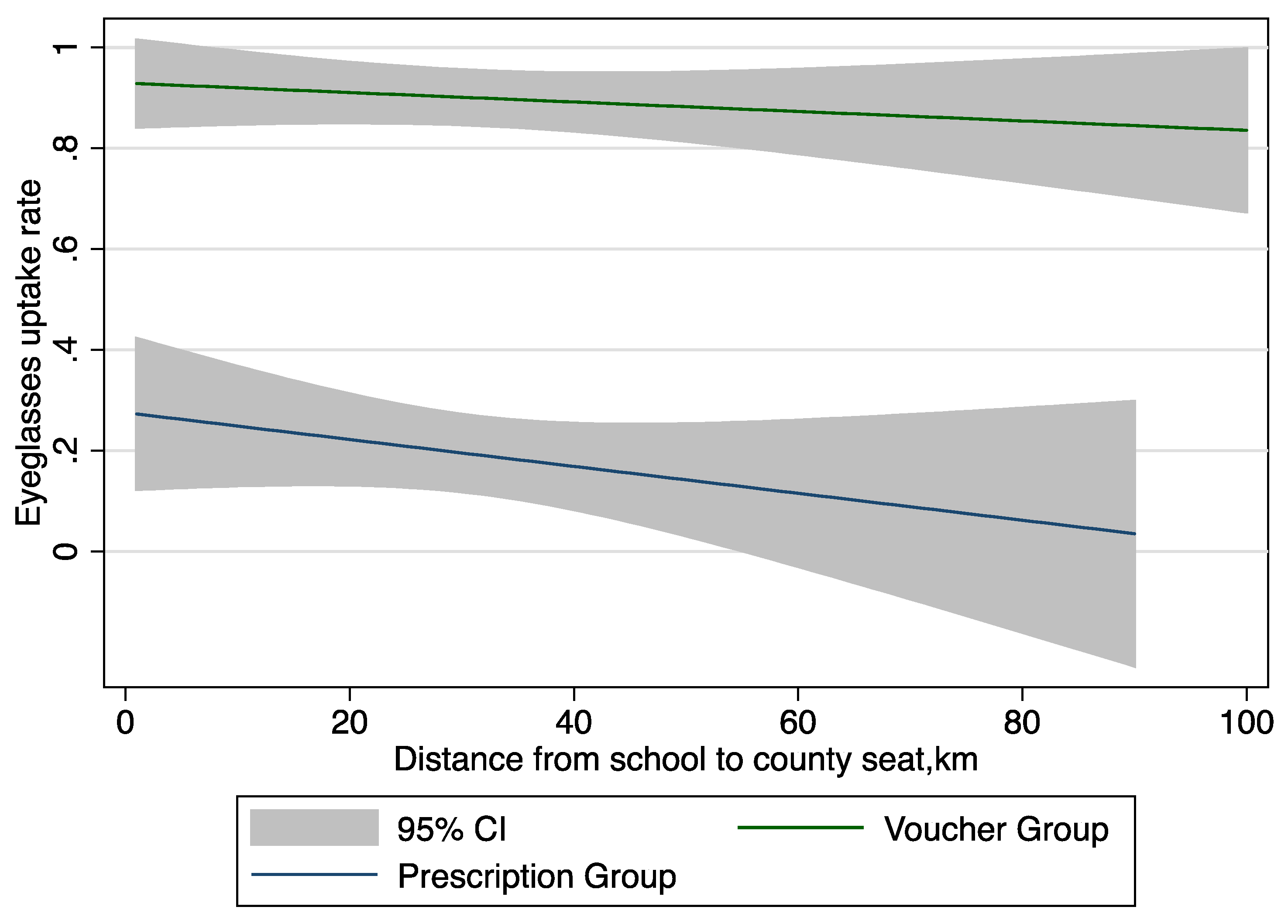
3.4. The Relationship between Distance and the Utilization among Rural Families
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Women’s Federation Report. A study of the conditions of left-behind children in rural China and migrant children in cities. Available online: http://acwf.people.com.cn/n/2013/0510/c99013-21437965.html (accessed on 30 March 2018).
- Keung Wong, D.F.; Li, C.Y.; Song, H.X. Rural migrant workers in urban China: Living a marginalised life. Int. J. Soc. Welf. 2007, 16, 32–40. [Google Scholar] [CrossRef]
- Ji, M.; Zhang, Y.; Zou, J.; Yuan, T.; Tang, A.; Deng, J.; Yang, L.; Li, M.; Chen, J.; Qin, H.; et al. Study on the Status of Health Service Utilization among Caregivers of Left-Behind Children in Poor Rural Areas of Hunan Province: A Baseline Survey. Int. J. Environ. Res. Public. Health 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Wen, M.; Lin, D. Child development in rural China: Children left behind by their migrant parents and children of nonmigrant families. Child. Dev. 2012, 83, 120–136. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhong, X.-N.; Li, Q.-Y.; Xu, D.; Zhang, X.-L.; Feng, C.; Yang, G.-X.; Bo, Y.-Y.; Deng, B. Health-related quality of life of the rural-China left-behind children or adolescents and influential factors: A cross-sectional study. Health Qual. Life Outcomes 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Peng, X.; Zong, R.; Yao, K.; Hu, R.; Du, Q.; Fang, J.; Zhu, M. The Status of Care and Nutrition of 774 Left-Behind Children in Rural Areas in China. Public Health Rep. 2008, 123, 382–389. [Google Scholar] [PubMed]
- Tian, X.; Ding, C.; Shen, C.; Wang, H. Does Parental Migration Have Negative Impact on the Growth of Left-Behind Children?—New Evidence from Longitudinal Data in Rural China. Int. J. Environ. Res. Public Health 2017, 14, 1308. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Sylvia, S.; Zhang, L.; Luo, R.; Yi, H.; Liu, C.; Shi, Y.; Loyalka, P.; Chu, J.; Medina, A.; et al. China’s Left-Behind Children: Impact Of Parental Migration On Health, Nutrition, And Educational Outcomes. Health Aff. 2015, 34, 1964–1971. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Chen, M.; Chan, K.L. A meta-analysis of the impacts of internal migration on child health outcomes in China. BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, X.; Ge, X. Left too early: The effects of age at separation from parents on Chinese rural children’s symptoms of anxiety and depression. Am. J. Public Health 2009, 99, 2049–2054. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Fan, J.; Liu, N.; Li, H.; Wang, Y.; Williams, J.; Wong, K. Depression risk of “left-behind children” in rural China. Psychiatry Res. 2012, 200, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Wang, L.; Rui, G. Depression among left-behind children in China. J. Health Psychol. 2017, 22, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Gao, J.; Liang, Z.; Wang, Y.; Du, Y.; Stallones, L. Parental migration patterns and risk of depression and anxiety disorder among rural children aged 10–18 years in China: A cross-sectional study. BMJ Open 2015, 5, e007802. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Lu, D.; Kang, M. Social capital and the mental health of children in rural China with different experiences of parental migration. Soc. Sci. Med. 2015, 132, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Mou, J.; Griffiths, S.M.; Fong, H.; Dawes, M.G. Health of China’s rural–urban migrants and their families: A review of literature from 2000 to 2012. Br. Med. Bull. 2013, 106, 19–43. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Liu, G. The Health Implications of Grandparents Caring for Grandchildren in China. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67B, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Biswas, P.; Kabir, Z.; Nilsson, J.; Zaman, S. Dynamics of Health Care Seeking Behaviour of Elderly People in Rural Bangladesh. Int. J. Ageing Later Life 2006, 1, 69–89. [Google Scholar] [CrossRef]
- Matovu, F.; Nanyiti, A.; Rutebemberwa, E. Household health care-seeking costs: Experiences from a randomized, controlled trial of community-based malaria and pneumonia treatment among under-fives in eastern Uganda. Malar. J. 2014, 13, 222. [Google Scholar] [CrossRef] [PubMed]
- Noordam, A.C.; Sharkey, A.B.; Hinssen, P.; Dinant, G.; Cals, J.W.L. Association between caregivers’ knowledge and care seeking behaviour for children with symptoms of pneumonia in six sub-Saharan African Countries. BMC Health Serv. Res. 2017, 17. [Google Scholar] [CrossRef] [PubMed]
- Nemet, G.F.; Bailey, A.J. Distance and health care utilization among the rural elderly. Soc. Sci. Med. 2000, 50, 1197–1208. [Google Scholar] [CrossRef]
- Thornton, R.L. The Demand for, and Impact of, Learning HIV Status. Am. Econ. Rev. 2008, 98, 1829–1863. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yip, W.; Zhang, L.; Wang, L.; Hsiao, W. Community-based health insurance in poor rural China: The distribution of net benefits. Health Policy Plan. 2005, 20, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, Q.; Lu, M.; Kwon, C.-S.; Quan, H. Rural and Urban Disparity in Health Services Utilization in China. Med. Care 2007, 45, 767. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.C.; Marmamula, S.; Rao, G.N. International Vision Care: Issues and Approaches. Annu. Rev. Vis. Sci. 2017, 3, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Murthy, G.V.S.; Gupta, S.K.; Ellwein, L.B.; Muñoz, S.R.; Pokharel, G.P.; Sanga, L.; Bachani, D. Refractive error in children in an urban population in New Delhi. Investig. Ophthalmol. Vis. Sci. 2002, 43, 623–631. [Google Scholar]
- Maul, E.; Barroso, S.; Munoz, S.R.; Sperduto, R.D.; Ellwein, L.B. Refractive Error Study in Children: Results from La Florida, Chile. Am. J. Ophthalmol. 2000, 129, 445–454. [Google Scholar] [CrossRef]
- He, M.; Huang, W.; Zheng, Y.; Huang, L.; Ellwein, L.B. Refractive error and visual impairment in school children in rural southern China. Ophthalmology 2007, 114, 374–382. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Sight Test and Glasses Could Dramatically Improve the Lives of 150 Million People with Poor Vision; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Bourne, R.R.A.; Dineen, B.P.; Huq, D.M.N.; Ali, S.M.; Johnson, G.J. Correction of Refractive Error in the Adult Population of Bangladesh: Meeting the Unmet Need. Investig. Ophthalmol. Vis. Sci. 2004, 45, 410–417. [Google Scholar] [CrossRef]
- Ramke, J.; du Toit, R.; Palagyi, A.; Brian, G.; Naduvilath, T. Correction of refractive error and presbyopia in Timor-Leste. Br. J. Ophthalmol. 2007, 91, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.; Zhang, L.; Ma, X.; Congdon, N.; Shi, Y.; Pang, X.; Zeng, J.; Wang, L.; Boswell, M.; Rozelle, S. Poor vision among China’s rural primary school students: Prevalence, correlates and consequences. China Econ. Rev. 2015, 33, 247–262. [Google Scholar] [CrossRef]
- Congdon, N.; Zheng, M.; Sharma, A.; Choi, K.; Song, Y.; Zhang, M.; Wang, M.; Zhou, Z.; Li, L.; Liu, X.; et al. Prevalence and determinants of spectacle nonwear among rural Chinese secondary schoolchildren: The Xichang Pediatric Refractive Error Study Report 3. Arch. Ophthalmol. 2008, 126, 1717–1723. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Zhou, Z.; Yi, H.; Pang, X.; Shi, Y.; Chen, Q.; Meltzer, M.E.; le Cessie, S.; He, M.; Rozelle, S.; et al. Effect of providing free glasses on children’s educational outcomes in China: Cluster randomized controlled trial. BMJ 2014, 349, g5740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Lam, J.; Lu, Y.; Ye, Y.; Lam, D.S.C.; Gao, Y.; Sharma, A.; Zhang, M.; Griffiths, S.; Congdon, N. Attitudes of Students, Parents, and Teachers Toward Glasses Use in Rural China. Arch. Ophthalmol. 2010, 128, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Glewwe, P.; Park, A.; Zhao, M. A better vision for development: Eyeglasses and academic performance in rural primary schools in China. J. Dev. Econ. 2016, 122, 170–182. [Google Scholar] [CrossRef]
- Krishnaratne, S.; White, H.; Carpenter, E. Quality Education for All Children?: What Works in Education in Developing Countries; International Initiative for Impact Evaluation: New Delhi, India, 2013. [Google Scholar]
- Bai, Y.; Yi, H.; Zhang, L.; Shi, Y.; Ma, X.; Congdon, N.; Zhou, Z.; Boswell, M.; Rozelle, S. An Investigation of Vision Problems and the Vision Care System in Rural China. Southeast Asian J. Trop. Med. Public Health 2014, 45, 1464–1473. [Google Scholar] [PubMed]
- Ma, X.; Congdon, N.; Yi, H.; Zhou, Z.; Pang, X.; Meltzer, M.E.; Shi, Y.; He, M.; Liu, Y.; Rozelle, S. Safety of Spectacles for Children’s Vision: A Cluster-Randomized Controlled Trial. Am. J. Ophthalmol. 2015, 160, 897–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camparini, M.; Cassinari, P.; Ferrigno, L.; Macaluso, C. ETDRS-Fast: Implementing Psychophysical Adaptive Methods to Standardized Visual Acuity Measurement with ETDRS Charts. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1226–1231. [Google Scholar]
- Bruhn, M.; McKenzie, D. In Pursuit of Balance: Randomization in Practice in Development Field Experiments. Am. Econ. J. Appl. Econ. 2009, 1, 200–232. [Google Scholar] [CrossRef]
- Grosvenor, T.; Grosvenor, T.P. Primary Care Optometry; Elsevier Health Sciences: New York, NY, USA, 2007; ISBN 978-0-7506-7575-8. [Google Scholar]
- Bailey, I.L.; Lovie, J.E. New Design Principles for Visual Acuity Letter Charts. Optom. Vis. Sci. 1976, 53, 740–745. [Google Scholar] [CrossRef]
- Cleveland, W.S. Robust Locally Weighted Regression and Smoothing Scatterplots. J. Am. Stat. Assoc. 1979, 74, 829–836. [Google Scholar] [CrossRef]
- Cleveland, W.S.; Devlin, S.J. Locally Weighted Regression: An Approach to Regression Analysis by Local Fitting. J. Am. Stat. Assoc. 1988, 83, 596–610. [Google Scholar] [CrossRef]
- Kremer, M.; Glennerster, R. Improving Health in Developing Countries: Evidence from Randomized Evaluations. In Handbook of Health Economics; Pauly, M.V., Mcguire, T.G., Barros, P.P., Eds.; Elsevier: New York, NY, USA, 2011; Volume 2, pp. 201–315. [Google Scholar]
- Ashraf, N.; Berry, J.; Shapiro, J.M. Can Higher Prices Stimulate Product Use? Evidence from a Field Experiment in Zambia. Am. Econ. Rev. 2010, 100, 2383–2413. [Google Scholar] [CrossRef]
- Cohen, J.; Dupas, P. Free Distribution or Cost-Sharing? Evidence from a Randomized Malaria Prevention Experiment. Q. J. Econ. 2010, 125, 1–45. [Google Scholar] [CrossRef]
- Grossman, M. The Human Capital Model; Elsevier: New York, NY, USA, 2000; pp. 347–408. [Google Scholar]
- Fischer, G.; Karlan, D.; McConnell, M.; Raffler, P. To Charge or Not to Charge: Evidence from a Health Products Experiment in Uganda; National Bureau of Economic Research: Cambridge, MA, USA, 2014. [Google Scholar]
- Miguel, E.; Kremer, M. Worms: Identifying Impacts on Education and Health in the Presence of Treatment Externalities. Econometrica 2004, 72, 159–217. [Google Scholar] [CrossRef]
- Qian, D.; Pong, R.W.; Yin, A.; Nagarajan, K.V.; Meng, Q. Determinants of health care demand in poor, rural China: The case of Gansu Province. Health Policy Plan. 2009, 24, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Wang, W.; Xu, L.; Li, Z.; Ding, Y.; Zhang, J.; Yan, F. Healthcare seeking behaviour among Chinese elderly. Int. J. Health Care Qual. Assur. 2017, 30, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.H.; Theoharides, C. Health-seeking behavior and hospital choice in China’s New Cooperative Medical System. Health Econ. 2009, 18, S47–S64. [Google Scholar] [CrossRef] [PubMed]
- Torgerson, D.J.; Donaldson, C.; Reid, D.M. Private versus social opportunity cost of time: Valuing time in the demand for health care. Health Econ. 1994, 3, 149–155. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Prescription Group | Voucher Group | Difference | p-Value |
|---|---|---|---|---|
| n = 1036 | n = 988 | |||
| (1) | (2) | (2)−(1) | ||
| 1. Age (Years) | 10.546 | 10.513 | −0.033 | 0.673 |
| (1.109) | (1.109) | |||
| 2. Male, 1 = yes | 0.499 | 0.480 | −0.019 | 0.379 |
| (0.500) | (0.500) | |||
| 3. Boarding at school, 1 = yes | 0.227 | 0.185 | −0.042 | 0.377 |
| (0.419) | (0.389) | |||
| 4. Grade four, 1 = yes | 0.404 | 0.385 | −0.020 | 0.380 |
| (0.491) | (0.487) | |||
| 5. Owns eyeglasses, 1 = yes | 0.139 | 0.140 | 0.001 | 0.973 |
| (0.346) | (0.347) | |||
| 6. Believe eyeglasses harm vision, 1 = yes | 0.415 | 0.364 | −0.051 | 0.114 |
| (0.493) | (0.481) | |||
| 7. Visual acuity of worse eye (LogMAR) | 0.647 | 0.621 | −0.027 | 0.104 |
| (0.215) | (0.210) | |||
| 8. Father has high school education or above, 1 = yes | 0.157 | 0.134 | −0.024 | 0.229 |
| (0.364) | (0.340) | |||
| 9. Mother has high school education or above, 1 = yes | 0.099 | 0.078 | −0.021 | 0.172 |
| (0.299) | (0.268) | |||
| 10. At least one family member wears glasses, 1 = yes | 0.347 | 0.325 | −0.022 | 0.322 |
| (0.476) | (0.469) | |||
| 11. Household assets (index) | −0.053 | −0.064 | −0.011 | 0.923 |
| (1.275) | (1.280) | |||
| 12. Distance from school to the county seat (Km) | 34.871 | 32.212 | −2.659 | 0.515 |
| (19.758) | (23.826) | |||
| 13. Both parents at home, 1 = yes | 0.509 | 0.487 | −0.022 | 0.511 |
| (0.500) | (0.500) | |||
| 14. Both parents migrated, 1 = yes | 0.100 | 0.124 | 0.024 | 0.138 |
| (0.301) | (0.330) |
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (Years) | Male, 1 = yes | Boarding at School, 1 = yes | Grade Four, 1 = yes | Owns Eyeglasses, 1 = yes | Believe Eyeglasses Harm Vision, 1 = yes | Visual Acuity of Worse Eye (LogMAR) | Father Has High School Education or Above, 1 = yes | Mother Has High School Education or Above, 1 = yes | At Least One Family Member Wears Glasses, 1 = yes | Household Assets (Index) | Distance from School to the County Seat. km | Both Parents at Home, 1 = yes | Both Parents Migrated, 1 = yes | |
| Panel A: Balance between Voucher and Prescription group accounting for attrition in short term | ||||||||||||||
| Voucher Group Dummy | −0.038 | −0.019 | −0.039 | −0.020 | 0.001 | −0.044 | −0.027 | −0.020 | −0.019 | −0.022 | −0.014 | −2.546 | −0.022 | 0.021 |
| (0.080) | (0.022) | (0.047) | (0.023) | (0.020) | (0.032) | (0.017) | (0.019) | (0.015) | (0.022) | (0.111) | (4.089) | (0.034) | (0.016) | |
| Attrition short term | 0.162 | 0.227 ** | 0.108 | −0.016 | −0.028 | 0.313 ** | −0.014 | 0.179 | 0.125 | 0.156 | 0.116 | 4.146 | −0.122 | −0.102 *** |
| (0.262) | (0.092) | (0.131) | (0.131) | (0.063) | (0.120) | (0.064) | (0.167) | (0.082) | (0.117) | (0.730) | (5.371) | (0.097) | (0.011) | |
| Voucher × Short term attrition | 0.273 | 0.003 | −0.177 | −0.016 | 0.006 | −0.384 ** | 0.035 | −0.195 | −0.144 | −0.007 | 0.174 | −6.516 | −0.014 | 0.155 |
| (0.341) | (0.165) | (0.153) | (0.183) | (0.104) | (0.166) | (0.071) | (0.182) | (0.101) | (0.163) | (0.804) | (7.865) | (0.150) | (0.100) | |
| Constant | 10.544 *** | 0.495 *** | 0.225 *** | 0.405 *** | 0.139 *** | 0.410 *** | 0.648 *** | 0.154 *** | 0.097 *** | 0.344 *** | −0.055 | 34.799 *** | 0.511 *** | 0.102 *** |
| (0.059) | (0.016) | (0.035) | (0.016) | (0.014) | (0.021) | (0.011) | (0.013) | (0.011) | (0.015) | (0.081) | (2.617) | (0.026) | (0.011) | |
| R2 | 0.002 | 0.004 | 0.004 | 0.000 | 0.000 | 0.006 | 0.004 | 0.003 | 0.003 | 0.002 | 0.001 | 0.004 | 0.002 | 0.003 |
| Panel B: Balance between Voucher and Prescription group accounting for attrition in long term | ||||||||||||||
| Voucher Group Dummy | −0.034 | −0.024 | −0.042 | −0.020 | 0.004 | −0.046 | −0.027 | −0.023 | −0.023 | −0.026 | −0.013 | −2.624 | −0.018 | 0.022 |
| (0.078) | (0.022) | (0.046) | (0.023) | (0.020) | (0.032) | (0.017) | (0.020) | (0.016) | (0.023) | (0.114) | (4.034) | (0.035) | (0.016) | |
| Attrition long term | −0.048 | −0.140 | 0.203 *** | 0.083 | 0.076 | 0.041 | −0.005 | 0.088 | 0.085 | −0.014 | −0.134 | 5.736 | −0.525 *** | 0.272 *** |
| (0.258) | (0.092) | (0.071) | (0.087) | (0.063) | (0.098) | (0.043) | (0.072) | (0.068) | (0.084) | (0.294) | (4.114) | (0.026) | (0.085) | |
| Voucher × Long term attrition | 0.021 | 0.148 | −0.041 | −0.026 | −0.094 | −0.116 | 0.017 | −0.049 | 0.012 | 0.083 | 0.082 | −2.191 | 0.018 | −0.020 |
| (0.345) | (0.117) | (0.104) | (0.118) | (0.077) | (0.123) | (0.051) | (0.103) | (0.091) | (0.106) | (0.364) | (6.322) | (0.035) | (0.124) | |
| Constant | 10.548 *** | 0.503 *** | 0.221 *** | 0.402 *** | 0.137 *** | 0.414 *** | 0.648 *** | 0.155 *** | 0.097 *** | 0.348 *** | −0.048 | 34.688 *** | 0.525 *** | 0.092 *** |
| (0.058) | (0.016) | (0.035) | (0.017) | (0.014) | (0.021) | (0.012) | (0.014) | (0.012) | (0.016) | (0.083) | (2.607) | (0.026) | (0.012) | |
| R2 | 0.000 | 0.002 | 0.010 | 0.001 | 0.001 | 0.003 | 0.004 | 0.002 | 0.005 | 0.001 | 0.000 | 0.005 | 0.038 | 0.026 |
| Variables | Non-Left-Behind | Left-Behind | Difference | p-Value |
|---|---|---|---|---|
| n = 1797 | n = 227 | |||
| (1) | (2) | (2)−(1) | ||
| 1. Age (Years) | 10.530 | 10.535 | 0.006 | 0.940 |
| (1.087) | (1.276) | |||
| 2. Male, 1 = yes | 0.494 | 0.458 | −0.035 | 0.314 |
| (0.500) | (0.499) | |||
| 3. Boarding at school, 1 = yes | 0.206 | 0.212 | 0.006 | 0.827 |
| (0.405) | (0.410) | |||
| 4. Grade four, 1 = yes | 0.390 | 0.436 | 0.047 | 0.176 |
| (0.488) | (0.497) | |||
| 5. Owns eyeglasses, 1 = yes | 0.141 | 0.128 | −0.013 | 0.593 |
| (0.348) | (0.335) | |||
| 6. Believe eyeglasses harm vision, 1 = yes | 0.393 | 0.370 | −0.023 | 0.507 |
| (0.489) | (0.484) | |||
| 7. Visual acuity of worse eye (LogMAR) | 0.634 | 0.637 | 0.003 | 0.850 |
| (0.211) | (0.224) | |||
| 8. Father has high school education or above, 1 = yes | 0.145 | 0.150 | 0.005 | 0.855 |
| (0.352) | (0.358) | |||
| 9. Mother has high school education or above | 0.081 | 0.150 | 0.069 *** | 0.001 |
| (0.273) | (0.358) | |||
| 10. At least one family member wears glasses | 0.337 | 0.332 | −0.005 | 0.881 |
| (0.473) | (0.472) | |||
| 11. Household assets (Index) | −0.019 | −0.364 | −0.345 *** | 0.000 |
| (1.273) | (1.268) | |||
| 12. Distance from school to the county seat. km | 33.866 | 31.247 | −2.620 | 0.089 |
| (21.868) | (21.823) |
| Variables | Eyeglasses Uptake | Eyeglasses Usage | ||||||
|---|---|---|---|---|---|---|---|---|
| Short Term | Long Term | Short Term | Long Term | |||||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | |
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |
| Voucher | 0.606 *** | 0.611 *** | 0.447 *** | 0.454 *** | 0.446 *** | 0.454 *** | 0.246 *** | 0.265 *** |
| (0.022) | (0.020) | (0.024) | (0.024) | (0.025) | (0.022) | (0.027) | (0.025) | |
| Controls | Yes | Yes | Yes | Yes | ||||
| Constant | 0.262 *** | 0.091 | 0.456 *** | 0.074 | 0.227 *** | −0.080 | 0.379 *** | 0.043 |
| (0.015) | (0.113) | (0.019) | (0.126) | (0.016) | (0.122) | (0.019) | (0.153) | |
| Observations | 1989 | 1980 | 1950 | 1941 | 1989 | 1980 | 1950 | 1941 |
| R2 | 0.411 | 0.527 | 0.262 | 0.332 | 0.258 | 0.390 | 0.122 | 0.231 |
| Mean in prescription group | 0.248 | 0.427 | 0.210 | 0.345 | ||||
| Eyeglasses Uptake | Eyeglasses Usage | |||||||
|---|---|---|---|---|---|---|---|---|
| Short term | Long term | Short term | Long term | |||||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | |
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |
| 1. Voucher Group | 0.597 *** | 0.603 *** | 0.435 *** | 0.442 *** | 0.437 *** | 0.445 *** | 0.233 *** | 0.251 *** |
| (0.022) | (0.020) | (0.025) | (0.025) | (0.026) | (0.024) | (0.029) | (0.026) | |
| 2. Left-behind children | −0.065 * | −0.050 * | −0.109 ** | −0.098 ** | −0.056 | −0.044 | −0.131 *** | −0.120 *** |
| (0.034) | (0.028) | (0.051) | (0.049) | (0.036) | (0.033) | (0.045) | (0.044) | |
| 3. Voucher * Left-behind | 0.084 ** | 0.068 * | 0.131 ** | 0.118 ** | 0.076 | 0.072 | 0.146 ** | 0.137 ** |
| (0.042) | (0.040) | (0.056) | (0.056) | (0.054) | (0.054) | (0.063) | (0.062) | |
| Baseline controls | YES | YES | YES | YES | ||||
| Constant | 0.269 *** | 0.096 | 0.466 *** | 0.080 | 0.233 *** | −0.075 | 0.391 *** | 0.050 |
| (0.015) | (0.113) | (0.020) | (0.125) | (0.017) | (0.122) | (0.020) | (0.151) | |
| Observations | 1989 | 1980 | 1950 | 1941 | 1989 | 1980 | 1950 | 1941 |
| R2 | 0.411 | 0.527 | 0.264 | 0.333 | 0.258 | 0.390 | 0.124 | 0.232 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guan, H.; Wang, H.; Huang, J.; Du, K.; Zhao, J.; Boswell, M.; Shi, Y.; Iyer, M.; Rozelle, S. Health Seeking Behavior among Rural Left-Behind Children: Evidence from Shaanxi and Gansu Provinces in China. Int. J. Environ. Res. Public Health 2018, 15, 883. https://doi.org/10.3390/ijerph15050883
Guan H, Wang H, Huang J, Du K, Zhao J, Boswell M, Shi Y, Iyer M, Rozelle S. Health Seeking Behavior among Rural Left-Behind Children: Evidence from Shaanxi and Gansu Provinces in China. International Journal of Environmental Research and Public Health. 2018; 15(5):883. https://doi.org/10.3390/ijerph15050883
Chicago/Turabian StyleGuan, Hongyu, Huan Wang, Juerong Huang, Kang Du, Jin Zhao, Matthew Boswell, Yaojiang Shi, Mony Iyer, and Scott Rozelle. 2018. "Health Seeking Behavior among Rural Left-Behind Children: Evidence from Shaanxi and Gansu Provinces in China" International Journal of Environmental Research and Public Health 15, no. 5: 883. https://doi.org/10.3390/ijerph15050883