4.1. Insights from PSS
The PSS framework was initially developed to analyze COVID-19 public sentiment towards reopening the economy for the purposes of catalyzing and augmenting public policy formulation [
5]. Samuel et al. highlighted the tremendous policy value of latent public sentiment and the need to capture it effectively for the purposes of influencing and contributing to the formulation of public policies at all relevant levels, including federal, state, and local governance. They carefully articulated the power of public sentiment, public perceptions, and public opinions and posited that the collective wisdom of mass, public, spontaneous, and continuous-stream social media posts are reflective of such public sentiments, perceptions, and opinions.
They also referenced a broad literature that demonstrates the use of social media analytics to gauge public opinion, and the power of public sentiment towards diverse issues, ranging from the stock market, to judicial processes, political agendas, technological innovation, crisis management policies, and the study of human behavior [
59,
60,
61,
62,
63].
Social media information is powerful and can pose contagion challenges owing to the virality of posts, as the information content and the format of feeds and posts have been shown to influence human sentiment and actions [
64,
65]. In the original PSS framework, the scenarios were presented as alternatives based on aggregate public sentiment conditions. In this study, we adapt the PSS theoretical framework and apply the concept to scenarios that may simultaneously emerge and coexist in different sub-populations. We use the PSS framework to structure our hypotheses for statistical analysis, and then to evaluate the public policy implications of the sentiment statistical analysis performed on vaccine tweets.
Scenario Analysis: 3 Significant Scenarios
The US is currently (May 2021) in an enviable position globally where, on any given day, it has more vaccines in stock than people willing to receive it. News reports have indicated increased public hesitancy towards the vaccine, partly due to the controversial federal government’s decision to implement a 10-day pause on the use of the Johnson & Johnson vaccine, to some attrition related to people who have already taken the first dose but do not appear to be returning for the second vaccine dose in a timely manner, and to a variety of other considerations.
We use the PSS framework to analyze the dominant sentiment in February and March 2021, and the two significant public sentiment changes—a change in positive sentiment from early February to late March, and change in negative sentiment from early February to late March. We do not dwell upon neutral sentiment in our analysis. The two changes do not automatically correlate negatively as may be intuitively perceived, because it is possible that both positive and negative sentiment counts or scores increase or decrease together at the expense of neutral sentiment. Hence, three scenarios are studied.
- (a)
Scenario 1: Positive public sentiment is dominant in February and in March 2021. Given this scenario, selected on the basis of descriptive analytics, we observe strong positive sentiment towards the vaccine. Illustrative tweets include celebratory posts, such as: “@PurelyNumbers Yay for vaccine!... ”; “@sprizee Happy birthday and congrats on the vaccine!”; “2nd dose ready. #vaccine #Happy”; “got a pfizer vaccine lined up for 4:20p on the afternoon before my birthday, nice nice nice nice”; “I love getting on Twitter / Instagram and seeing another friend, loved, or/and mutual receiving their vaccine. Just makes me so insanely happy" and "Got the vaccine! So thankful for God’s protection all around me!”.
These posts demonstrate positive public perceptions based on high levels of confidence that vast segments of the population have in vaccines. There is also a strong positive public perception on the operations and delivery of the vaccines: “Super shout out to everyone at the Moorestown Mall COVID-19 vaccine mega site. Unbelievably efficient & well run....really impressive...”; “Today I got my second dose of the Pfizer COVID-19 vaccine. Kudos to the Vermont National Guard for a job well done: well organized, smooth, courteous.”; “Best ‘day-date’ ever with @john_r_ratliff Our 1st vaccine dose is DONE. Thank you @UofLHealth for the massive undertaking, exceptional organization, and seamless process. #pfizercovid19vacccine #SeeYouIn3Weeks” and “Got my first COVID vaccine this morning administered by @NashvilleHealth. They are doing a phenomenal job with the logistics of rolling this out to our city. Everyone was friendly, helpful and efficient. Big thanks and kudos to all involved!!”.
These posts demonstrate public sentiment being driven by the vaccines and by their smooth delivery. An important takeaway from this for public policy is the emphasis on facilitating a comfortable and efficient vaccination process.
- (b)
Scenario 2: Positive public sentiment decreases from early February to late March 2021. Interestingly, we saw a decrease in positive public sentiment as indicated by the change in the proportion of positive tweets from early February to late March 2021. We do not speculate on the reasons for this but, instead, attempt to identify and discuss mass perceptions to help the public policy discourse.
Skepticism, both reasonable and unreasonable, appears to have increased, which may have toned some proportion of positive tweets into neutral or negative territory: “@Ironman_E @cruddydre_ @Ms_Jaydee But if your vaccinated and the vaccine works, what does it matter if im vaccinated? Youre safe right? Because the vaccine works right?”; “If we’re supposed to get the vaccine to protect other people but other people are supposed to get the vaccine to protect other people, who is it actually protecting? If the vaccine is already protecting those other people how does other people getting it further protect them?"; "excited to announce that i am not 30, therefore ineligible to receive a vaccine in the state of New York” and “@7_bunnies @TwixxBar07 @courtneymilan “Experts do not know how long” I’m protected by the antibodies I’ve acquired from infection. That’s fine. They don’t know how long the vaccine will protect, either, so we’ll all learn together. Meanwhile, I’ll stick to my own immune system’s protection”.
This change in sentiment, though minor, may be mitigated by a number of factors, such as a general loss of enthusiasm without a loss of confidence in the vaccines. Public policy can be quite useful in addressing such scenarios to prevent the erosion of positive public perceptions of vaccines and on the vaccination process—this can be achieved through appropriate communications and pronounced narrative development.
- (c)
Scenario 3: Negative public sentiment increases from early February to late March 2021. Multiple sentiment scoring methods affirmed the proportional increase in negative sentiment from early February to late March 2021. This is more alarming than the minor loss of positive sentiment across the same period: a loss of positive sentiment can be attributed to a number of factors and may not necessarily reflect a loss of confidence in vaccines; however, a proportional increase in negative sentiment over time could imply eroding confidence in vaccines based on rumors or inaccurate information. There could also be statistically disproportionate emphasis on some cases of people falling ill after taking the first or both dose/s of the vaccines, or outlier events, such as deaths following vaccination.
Illustrative tweets convey these concerns and negative sentiment quite effectively: “Whoa...when they say that the second vaccine might have strange side effects, the are NOT kidding.”; “Vaccine update: a day after shot one of the Pfizer vaccine I’m definitely feeling the arm pain, a headache, and kind of run down.”; “@onewiththesand Oh no. Feel better. Do you feel it is from your vaccine shot?” and “I would not have taken the vaccine if I knew it would make me sick... ”. While there is a general concern about some uneasiness, discomfort and pain post-vaccination, most people appear to accommodate that, as illustrated by many tweets along the lines of: “pretty achy and fatigued following my second vaccine dose yesterday. but still so grateful and hopeful. worth it 1000x over! #GetVaccinated ”.
Perhaps, the greater challenge is posed by some factual news on statistical outliers augmented by rumors of people being severely affected by vaccinations or even dying from the vaccine. This is illustrated by the deeply negative sentiment in some of the vaccine tweets in March of 2021: “@cruddydre_ My uncle got the vaccine and died a week or 2 later. I’m good bro yal can have that vaccine.”; “@DanMac2014 @Kayla_Grey @pfizer Wish one could request your vaccine, @moderna was a monster. Haveing had COVID recovered in 3 days with light fever/aches. Vaccine-1st dose F’d me up-5x worse then VID did. I wanted to crawl under a rock & die the past 3 days. Not sure I’ll go for 2nd...”; “Mom don’t be a cry baby. It doesn’t help that I have a sister that tried to have her not take it telling her that there’s people who died from the vaccine...I tell my mom that my sister isn’t well informed...directs mother to the daughter who has a PhD.”; “@princessnofrog Haven’t seen that yet they are not sure because it’s still in the experimental stage but there has been people that have died from the vaccine. Meaning it can be deadly” and “Maybe the vaccine will kill me since the virus didn’t”.
Such expressions of fear, despair and negativity tend to spread fast through social media and personal messaging and communications. Public policy is critical in such scenarios and proactive steps are required to build public confidence. Transparency on adverse events must not be compromised—post-vaccination illnesses and the rare cases of death must continue to be documented and such information must be made publicly available.
However, public policy must mandate resources for such information to be augmented and qualified by factual information truthfully highlighting the details along at least two lines of reasoning: (a) An emphasis on the rarity of extreme events such as vaccination induced deaths and (b) disassociation of vaccination as the cause of deaths after vaccination, where applicable, and clarity on the identified or potential causes of death.
4.3. Temporal Changes in Public Sentiments
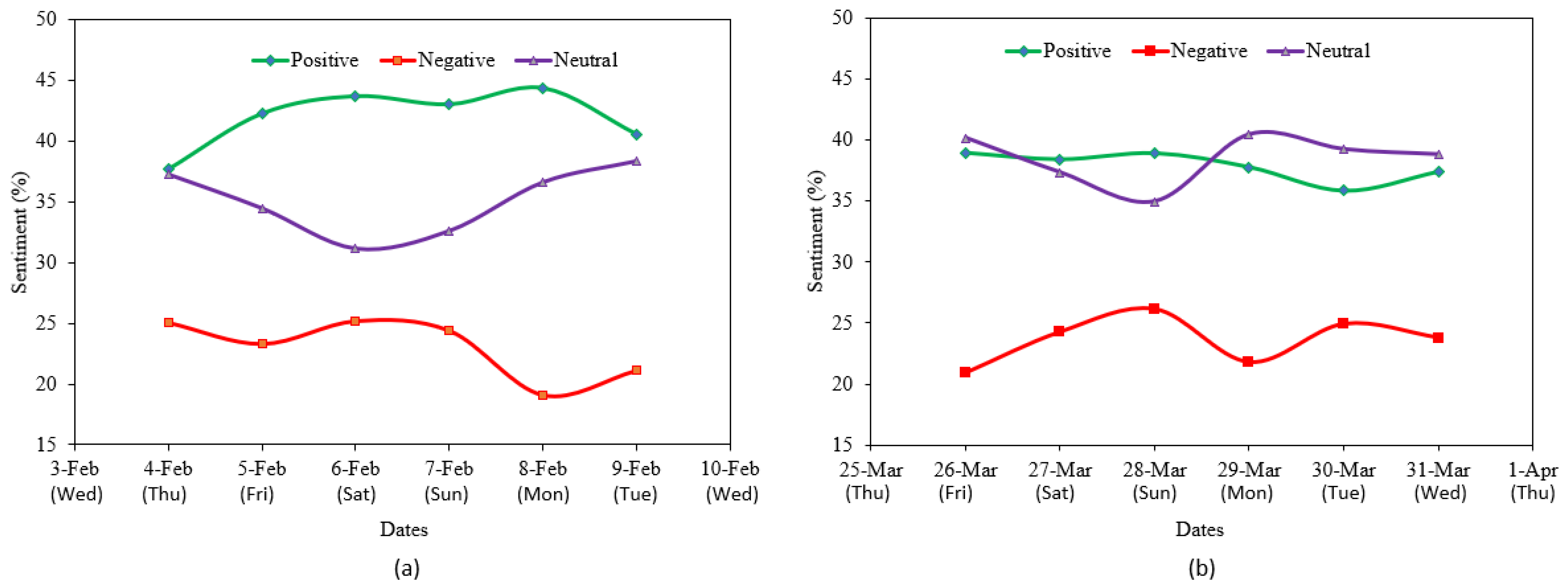
COVID-19 vaccine sentiments among Twitter users were observed and analyzed over a period of 6 days, both in the early February and the late March 2021 time frames. In the February time frame, an increasing positive sentiment trend, a decreasing negative sentiment trend, and stable neutral sentiment trend were found (
Figure 5a). On the other hand, in the March time frame, at the end of the week, no significant change was observed in the positive and neutral sentiment trends, but a slight increase is discernible in the negative sentiment trend (
Figure 5b). Apart from this, we also noted that the negative sentiment score was the lowest on Monday in both time frames. Negative scores were higher over the weekends compared to weekdays. Conversely, the neutral sentiment score was the lowest during the weekends. This suggests that people post more negative tweets during the weekends than on weekdays.
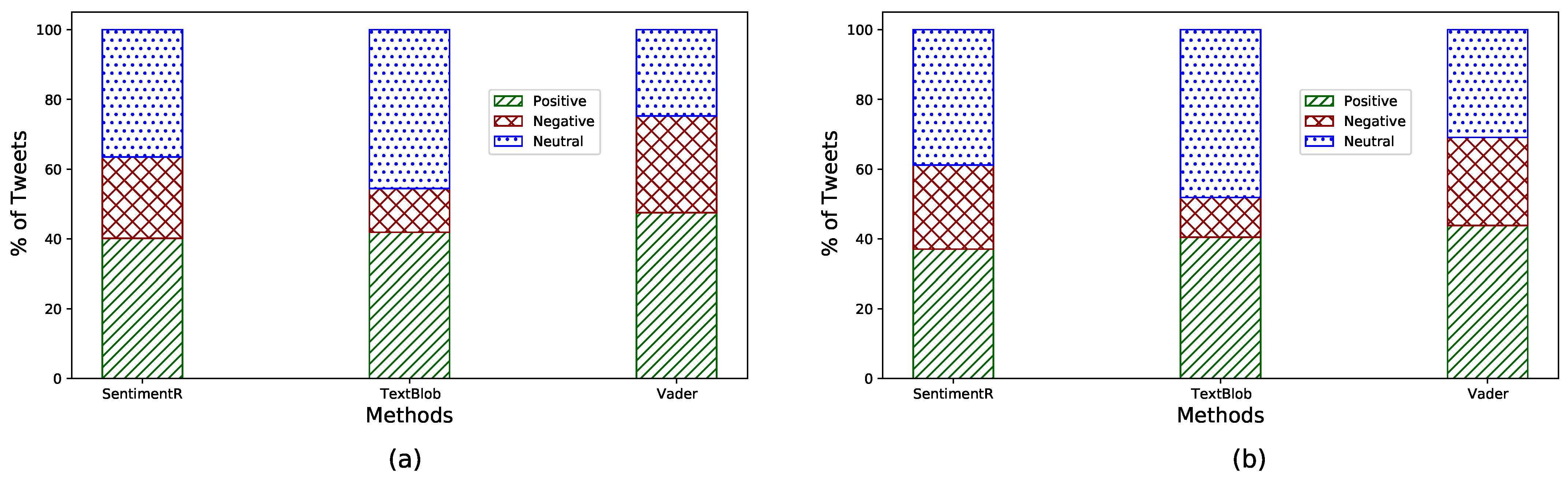
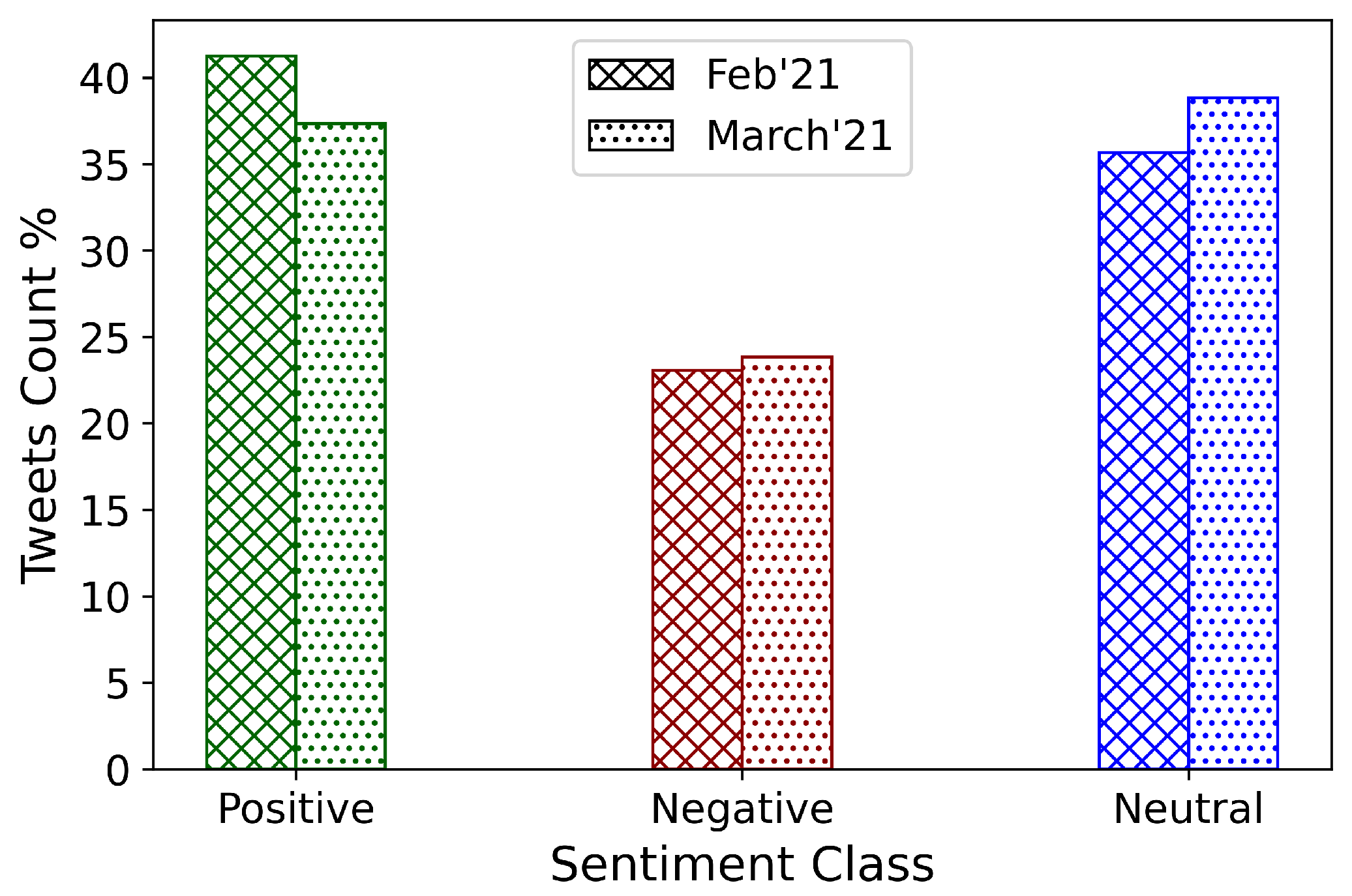
Overall, as depicted in
Figure 6, the share of positive sentiment tweets decreased over time (from early February to late March 2021). On the other hand, although the ratio of negative sentiment tweets did not change much, neutral sentiment increased noticeably. This indicates that, while COVID-19 vaccination was in full swing during February and March of 2021, public perceptions towards vaccination did not improve on the aggregate.
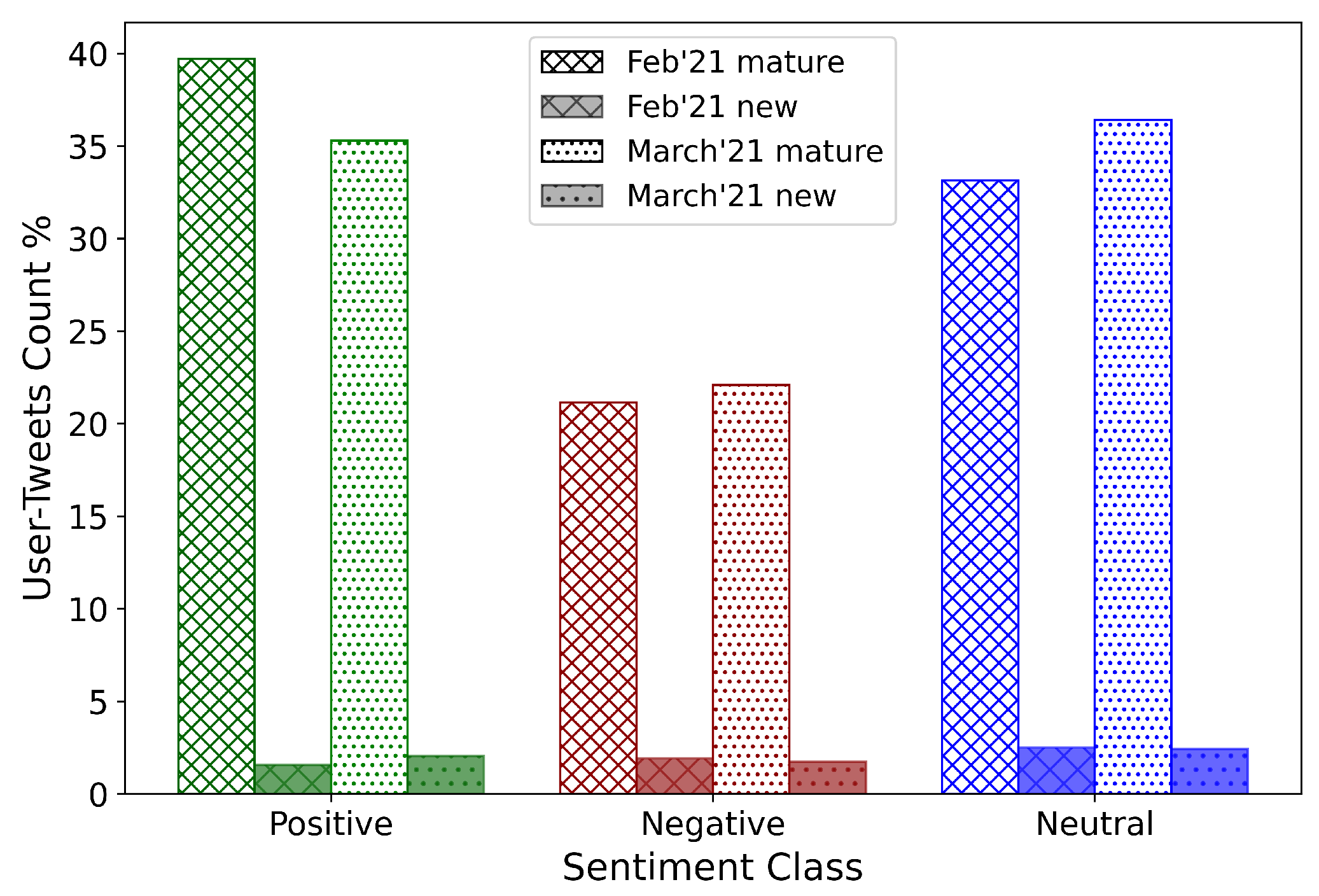
To understand the effect that the type of Twitter users may have had on the sentiment score, the Twitter accounts were divided into two groups based on the year of creation of the account. Accounts created before January 2020 form the mature group, while those created subsequently were categorized as the new group. The tweet sentiments based on these age groups were observed and plotted in
Figure 7. Of the total number of tweets, 6% and 6.21% were posted by new users in early February and late March 2021, respectively. These results indicate that tweets by new users neither dominated the overall narrative on COVID-19 vaccines nor, therefore, the public sentiments. Among the February tweets, about 40% were mature positive, 21.15% were mature negative, and 33.15% were mature neutral tweets.
On the other hand, in March 2021, 35.30% were mature positive, 22.09% were mature negative, and 36.40% were mature neutral tweets. It can be observed that, both among February and March tweets, positive sentiment was higher than negative sentiment among the mature users. Additionally, the percentage of neutral sentiment increased among the mature users from February to March. However, no such discernible change can be observed in the posts made by the new users. Sentiment changes in the Twitter discourse are entirely imputable to mature users.
4.4. Statistical Analysis of Sentiment Values
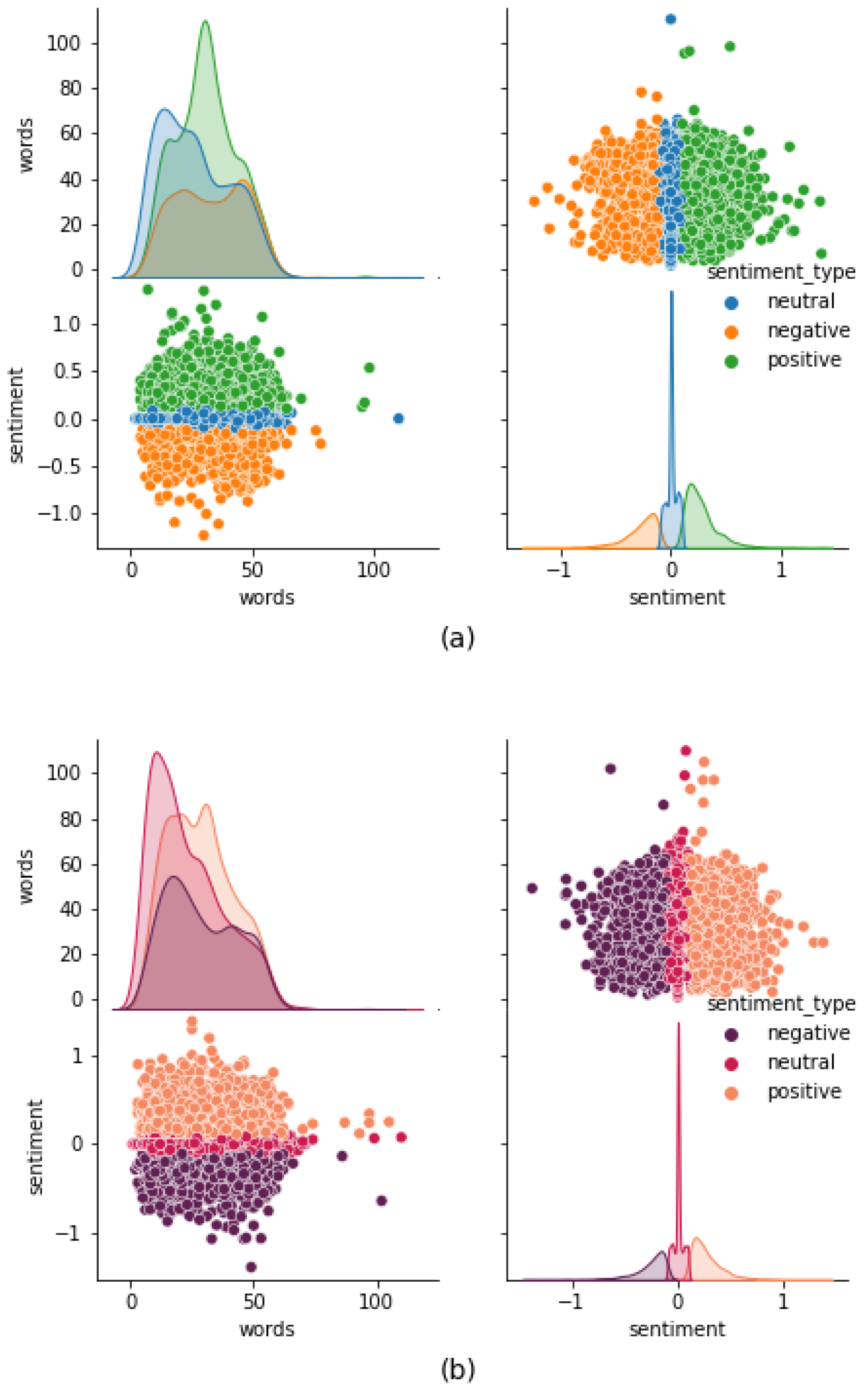
Various characteristics of the tweets were explored using descriptive analytics, and tweet length was found to have no significant correlation to sentiment scores (
Figure 2). Tweet lengths and sentiment scores displayed bimodal and skewed visually undetermined distributions. The majority of tweets were between 10 and 55 words in length, and most of the tweet sentiment scores fall in the range of −1 to 1. Our analysis of the sentiment scores shows that the percentage of tweets with positive sentiment was higher (daily as well as overall, in both datasets) compared to the percentage of tweets with negative sentiment (
Figure 5).
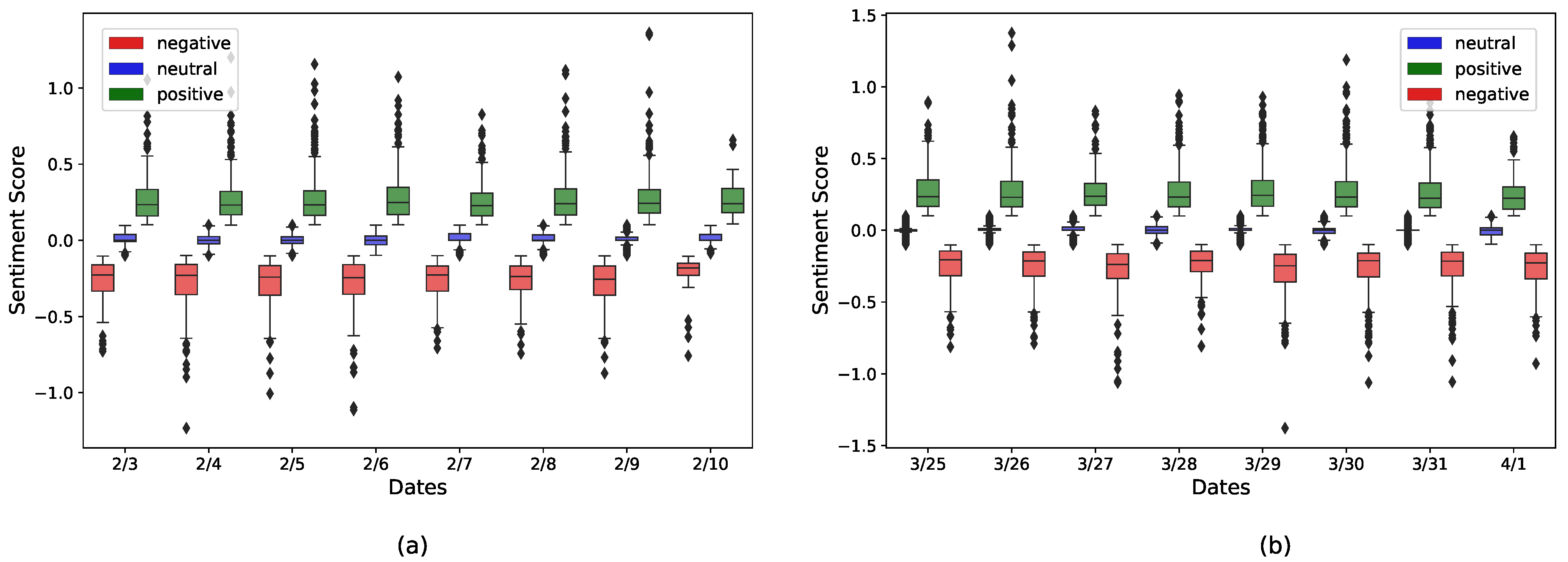
Figure 8 shows day-wise boxplots representing the distribution of sentiment scores in three classes (positive, negative, and neutral) based on the February dataset (
Figure 8a), and March dataset (
Figure 8b). It can be observed that the median values of the positive sentiment scores were equal or slightly greater than 0.25, whereas the maximum values were usually over 0.50. On the other hand, the median values for the negative sentiment scores were close to −0.25, and minimum values were usually under −0.50.
For both positive and negative sentiments, the median value was not located in the middle of IQR (interquartile range) of the boxplot, which implies that the sentiment scores were most likely not normally distributed. Additionally, we observe more outliers in positive sentiment boxplots than in negative sentiment boxplots (more tweets in extremely positive class than extremely negative). Descriptively, these boxplots indicate that the overall strength of positive sentiment was greater than that of the negative sentiment.
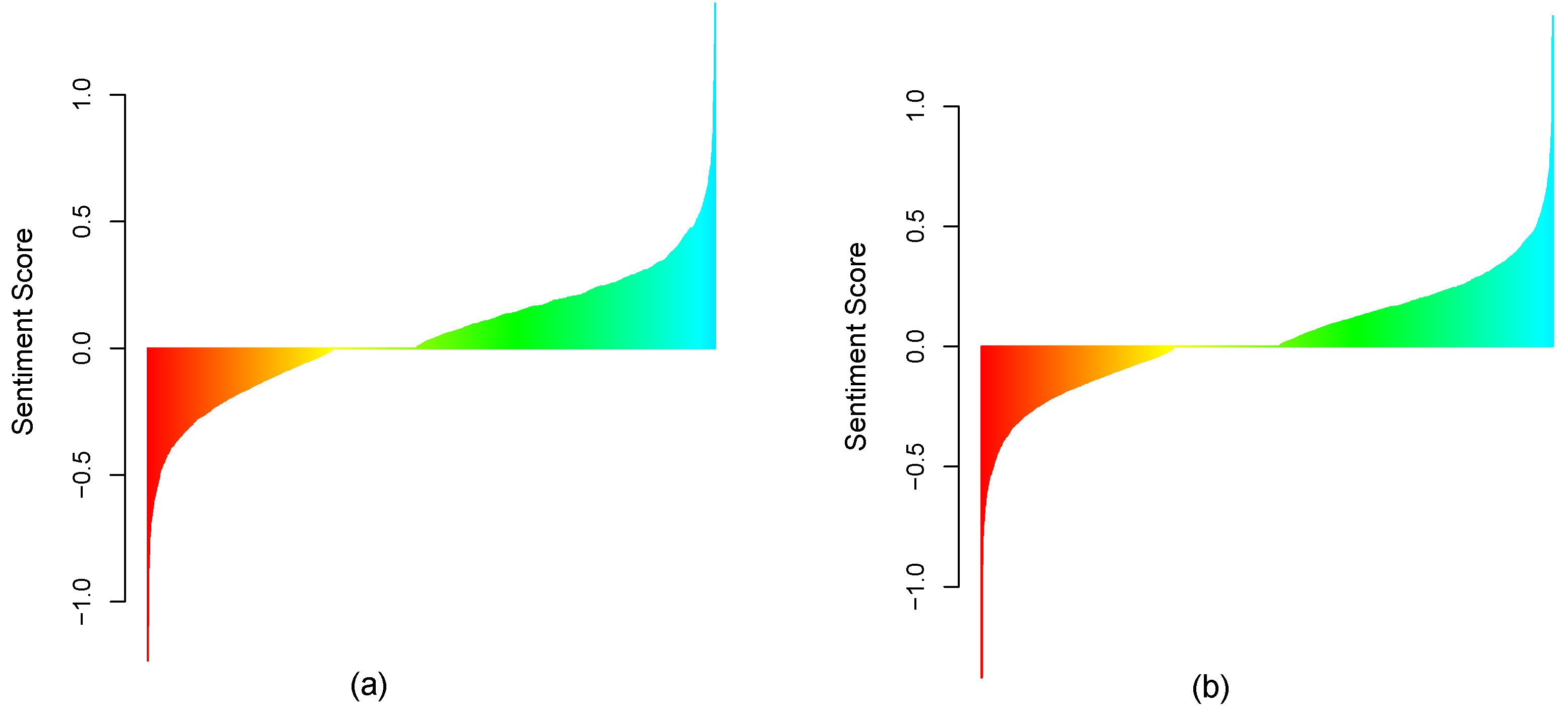
The descriptive analytics presented thus far provides strong support for a positive sentiment on vaccines that dominates the corresponding negative sentiment for both February and March 2021 (see
Figure 5 in particular). There is also some initial evidence of a decrease in positive sentiment between February and March, and evidence of an increase in negative sentiment between these time frames. The visual analysis of sorted sentiment scores for early February and late March 2021 (
Figure 9a,b) suggests the same.
However, this is insufficient from a statistical standpoint, and it is necessary to validate such descriptive findings. We validated the exploratory findings with a Proportion test on the ratio of positive tweets to negative tweets separately for early February and for late March, and further verified this by applying an Exact Binomial test as shown in
Table 2,
Table 3 and
Table 4.
4.4.1. Dominant Positive Sentiment for February and March 2021
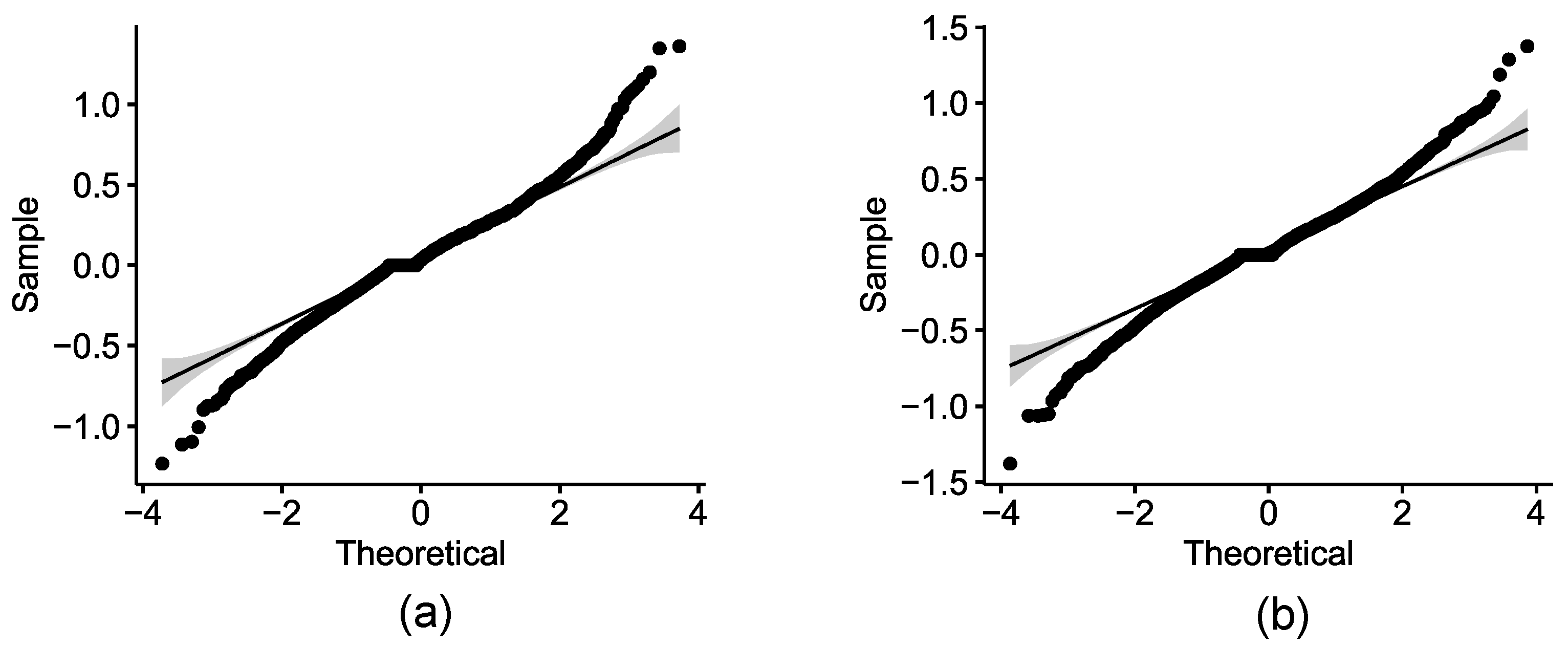
We first tested for the normal distribution of the sentiment scores. For this purpose, we applied the Shapiro–Wilk normality test on the sentiment scores computed for February 2021 (
Table 2) and for March 2021 (
Table 3). The tests concluded that the sentiment scores were not normally distributed. These results were also supported by the Q-Q plots indicating departure from normality (
Figure 10). We therefore employed the same validation approach used for the PSS framework by Samuel et al., which involved applying the non-parametric Proportion Test and Exact Binomial Test [
5].
The results of the Proportion Test, with the null hypothesis indicating that the proportional count of negative tweets is equal to or greater than that of positive tweets, inferred that the null hypothesis could safely be rejected with a p-Value significantly <0.0001 on both the February and March samples. The Proportion Test results, thus, validated the alternative hypothesis for the positive sentiment proportion being significantly greater than the corresponding negative sentiment. The Exact Binomial tests confirmed the same results.
Finally, the Wilcoxon signed rank test was used to confirm the findings, as the sentiment scores were not normally distributed. Thus, the dominance of the positive sentiment scores for both February and March were supported both by the Proportion Test, as well as by the Exact Binomial Test.
4.4.2. February-March: Lower Positivity and Higher Negativity
Although, as demonstrated above, positive sentiment for both February and March remained stronger than corresponding negative sentiment, our analysis of relative changes highlighted important insights: the relative proportion of positive sentiment decreased from February to March, and the relative proportion of negative sentiment increased from February to March 2021. Here again, we employed the Proportion Test and further validated it using the Exact Binomial Test. Our null hypothesis was that positive sentiment remained in the same relative proportion or increased from February to March.
The results, as shown in
Table 4, indicate that the null hypothesis can be fairly rejected in favor of the alternate hypothesis that relative proportion of positive sentiment decreased from February to March. In a similar way, we statistically tested that the relative proportion of negative sentiment increased from February to March. The original PSS framework applied these methods in a cross sectional manner, with data collected for one period of time [
5]. In this study, we extended the PSS framework to contrast Public Sentiment Scenarios across two time periods, namely February and March 2021.
4.5. State-Wise Sentiment Analysis in the US
In this subsection, we explore the progression in COVID-19 vaccination sentiment on a state by state basis from early February to late March 2021. It should be noted that, because of the limitations of geo-location of Twitter posts, some states may have rather small sample sizes, and therefore inference should proceed with caution. This is particularly the case of Idaho, South Dakota, Vermont, and Wyoming in February and of Alaska and Wyoming in March.
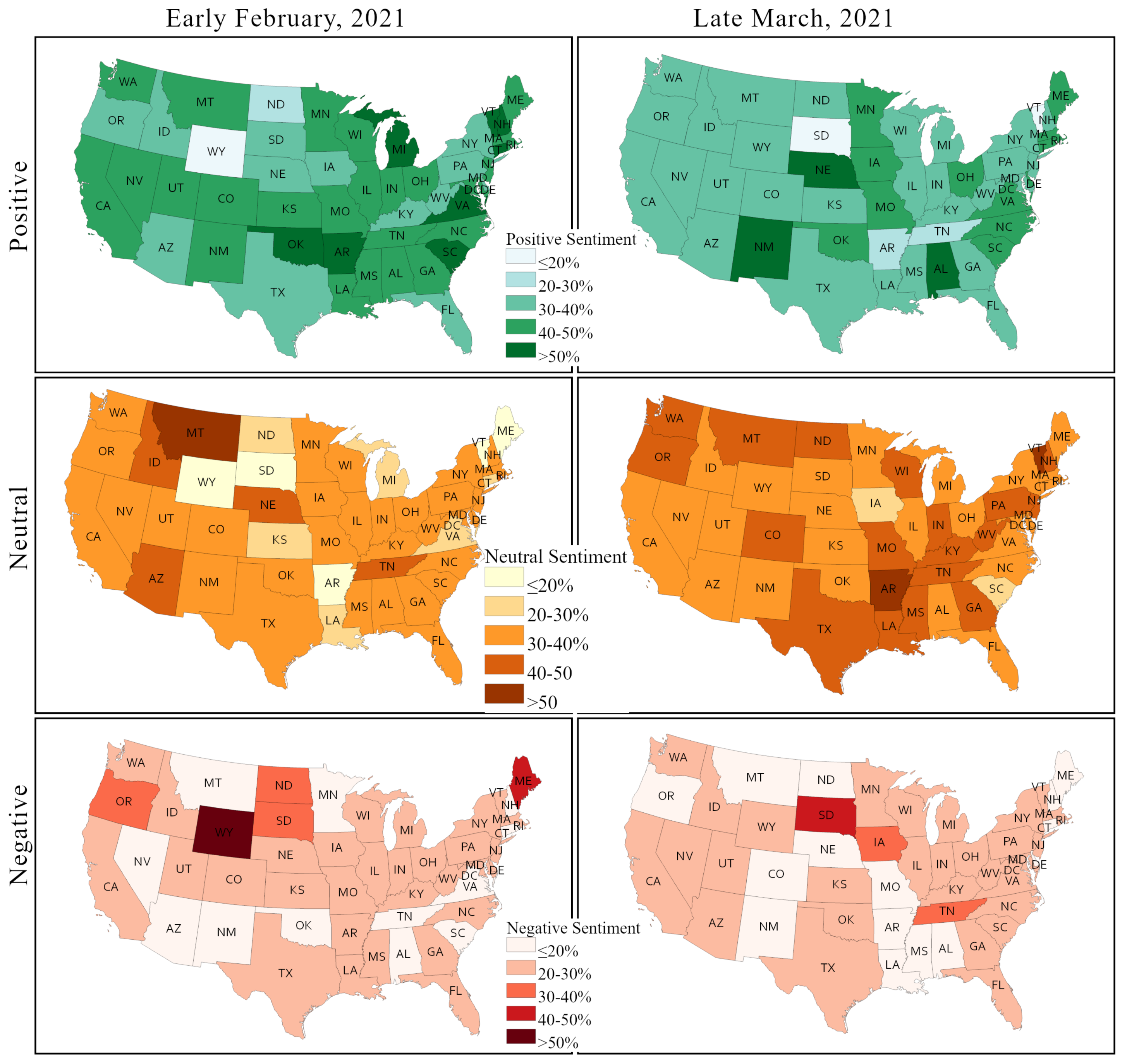
Figure 11 depicts the percentage of positive, negative, and neutral sentiment across states in early February and in late March. The positive sentiment is decreased in most states, except for a handful, namely New Mexico, Nebraska, Iowa, North Dakota, and Alabama. In the latter states, the positive sentiment is increased by as much as 10%. The largest decline in positive sentiment is observed in Vermont and Arkansas, from more than 50% to below 20% and 20–30%, respectively. A few states have around 20% decline in positive sentiment including New Hampshire, Michigan, South Dakota, and Tennessee, whereas South Dakota and Tennessee have a significant increase in negative sentiment. Most of the states have no or very little change in negative sentiments.
A significant decline in negative sentiments is observed in only four states: Wyoming, North Dakota, Oregon, and Maine. A significant decline in both positive and negative sentiments in Arkansas results in a sharp rise of neutral sentiments. In contrast, both positive and negative sentiments are increased in a few states, while neutral sentiment is decreased, as in the case of Iowa.
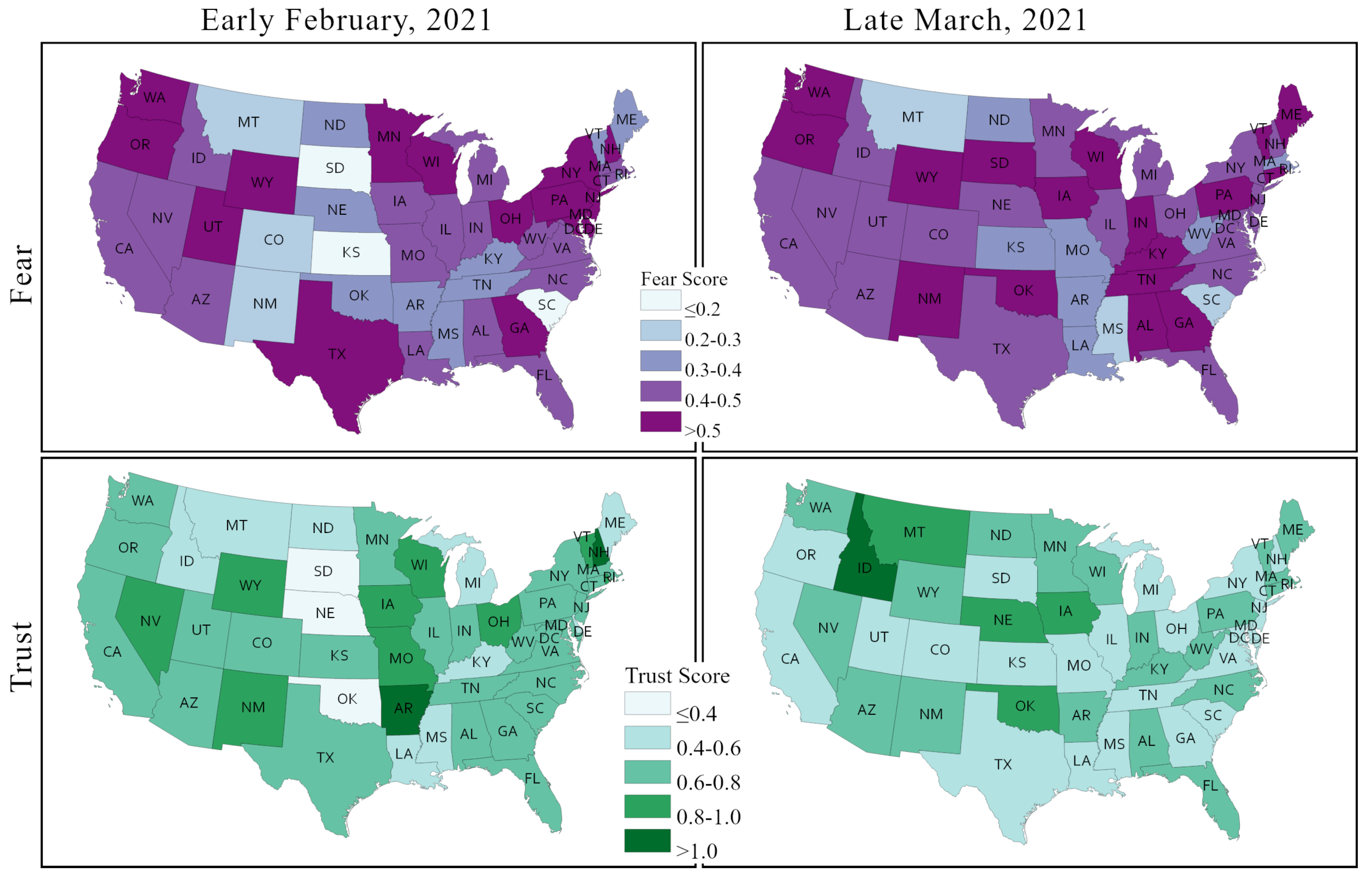
Figure 12 depicts the changes in two sentiments that feature prominently in the context of the COVID-19 pandemic and of the health policy responses, including the vaccination campaign, –fear and trust– between early February and late March across US states. The fear sentiment vis à vis COVID-19 vaccination is very strong in most states, and this sentiment gained even further strength in most cases over time. Nearly two thirds of the contiguous US states showed an overall fear score over 0.4 in early February. This number increased to 38 (about 80%) by late March. Generally, the fear sentiment remained unchanged in the Northwest and the West regions, but it increased in many states of the Southwest, the Southeast, and the Midwest. Fear sentiments decreased or remained unchanged in several large states, including Texas, New York, California, Arizona, and Florida.
Most of the states showed relatively moderate to low score in trust sentiments in early February. However, in contrast to the fear sentiment, the trust sentiment dropped further in a majority of states, except for a few, such as South Dakota, Nebraska, Oklahoma, Idaho, Arkansas, and North Dakota. Trust in vaccines decreased the most in Arkansas. Although, fear sentiment remained largely unchanged in large states, trust sentiment decreased in California, Texas, and New York.
4.6. Discussion
Considering the criticality of vaccination to secure public health and the high ambition of the stated national goal, we sought to identify the states that could be regarded as leaders and laggers in the pursuit of vaccination, and to assess how the differentiation among states on this basis intersected with state-wise public sentiments. To this end, we used the state-wise actual rate of vaccinations sourced from the US CDC [
12]. We observed that the vaccination rates varied considerably from one state to another. We will discuss state-wise sentiment assessed from the Twitter posts in relation to these vaccination rates and vice versa.
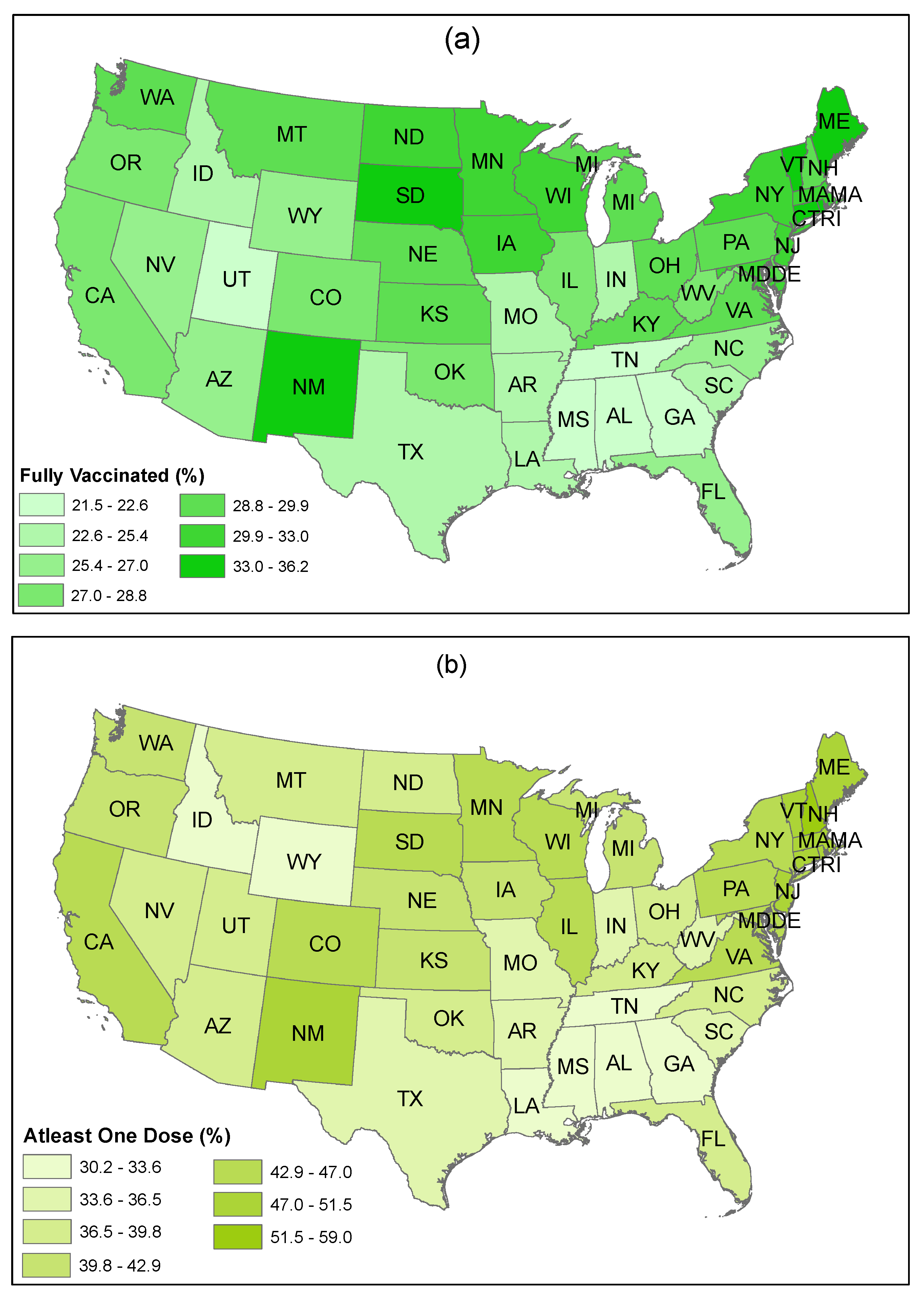
Figure 13 shows the rate of fully vaccinated people and of people who have received at least one dose of vaccine (%) in US states as of 28 April. The figure indicates that people living in the Northeast (e.g., Maine, New Hampshire, Connecticut, Rhode Island, Vermont, New Jersey, Massachusetts, New York, Pennsylvania, Delaware, the District of Columbia, and Maryland) have a higher rate of vaccine uptake. In contrast, a lower rate of vaccine uptake is observed in the South (e.g., Alabama, Georgia, Louisiana, Mississippi, Tennessee, Arkansas, South Carolina, and Texas).
A somewhat mixed response to vaccination can be noticed among the residents in the Midwest and in the West (i.e., some states have a higher vaccination rate, while some have a lower rate). People living in the West, particularly in California, New Mexico, Arizona, and Colorado showed a higher willingness accompanied with a higher rate of vaccination. However, residents from Wyoming and Idaho showed a reluctance to accept vaccines, and, as a consequence, a lower rate of vaccination is observed in these two states.
Although a higher use of distributed vaccines is observed in Utah, overall vaccine administration is low in this state. The states in the Midwest also have a higher rate of vaccine uptake. More specifically, people in South Dakota, North Dakota, Wisconsin, Iowa, Kansas, and Minnesota have a higher rate of vaccination. On the other hand, Missouri and Indiana have a lower rate of overall vaccine administration.
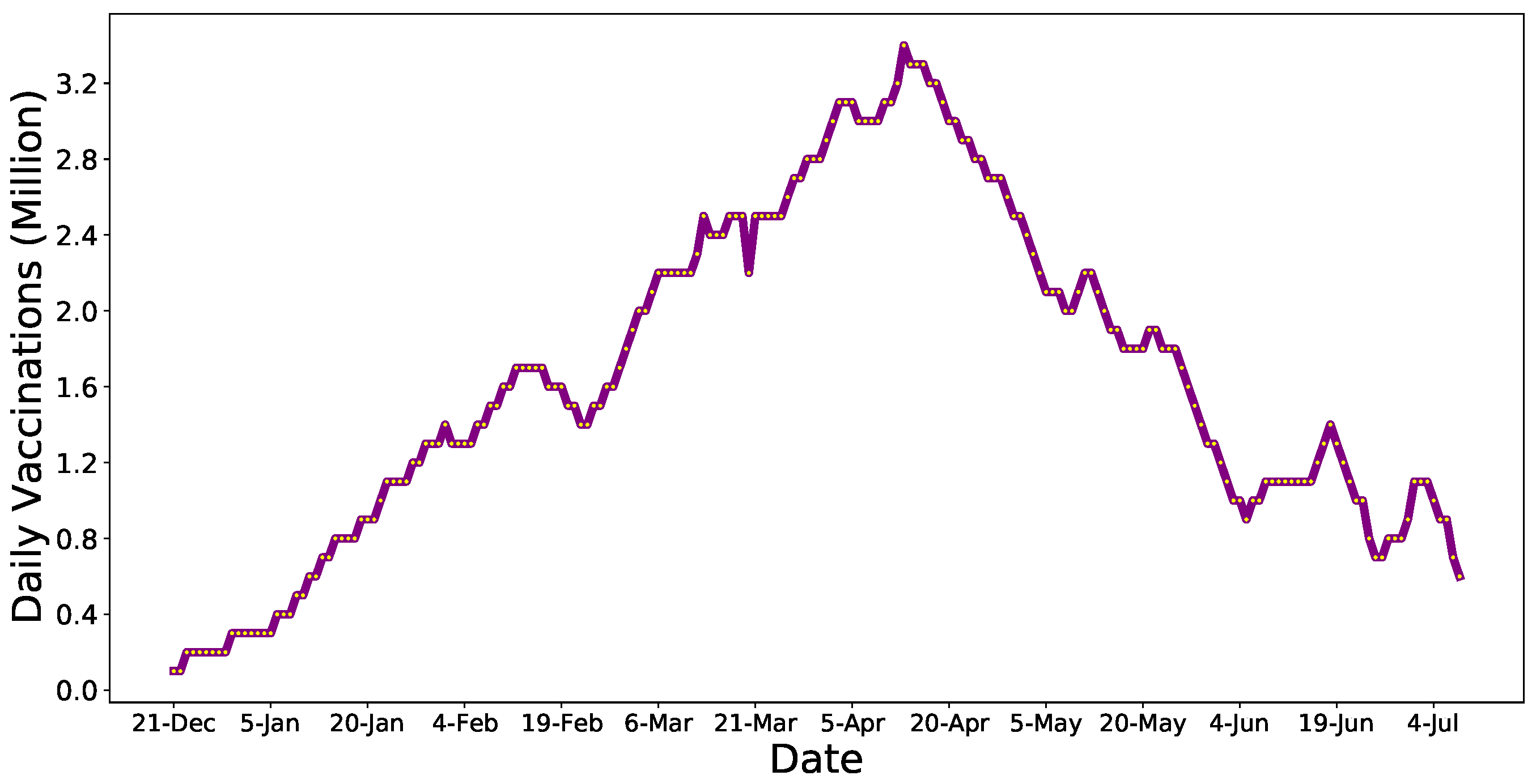
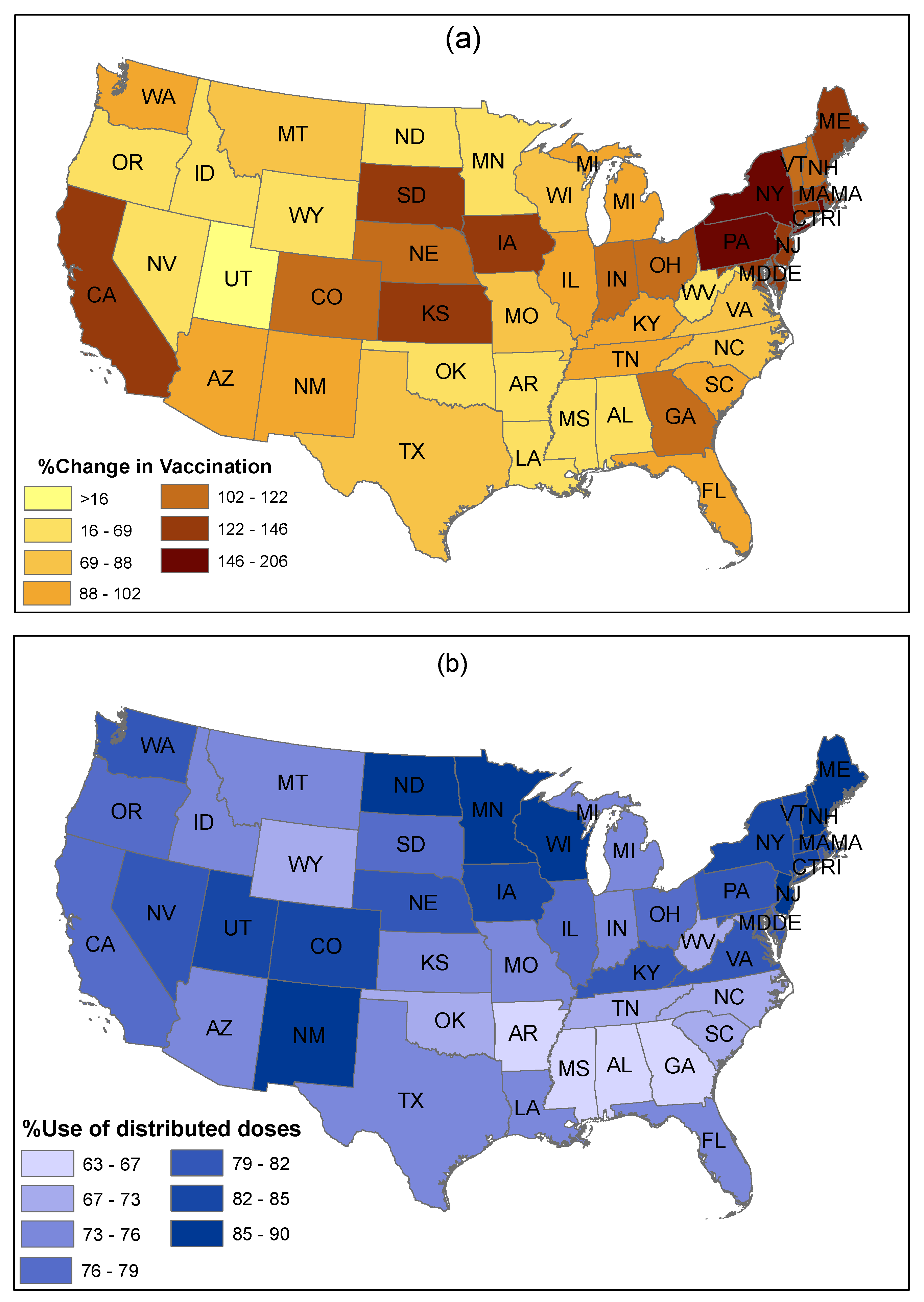
To more directly compare state-wise vaccination propensities with our tweet sentiment analytics, we also investigated the changes in vaccination uptake in the US by collecting average daily vaccination data from the same time frames, that is 3 to 10 February and 25 March to 1 April (
Figure 14a). The figure shows that most states achieved a significant increase in vaccination in late March, when compared to early February. The highest increase in vaccination is observed in the Northeast regions of the US.
Similarly, a significant increase in vaccination is also observed in some Midwestern states (e.g., Kansas, Iowa, and South Dakota), despite a low increase in vaccination in North Dakota and Minnesota. In contrast, the lowest increase in vaccination is noticed in parts of the West region (e.g., Utah, Idaho, and Wyoming). However, California achieved a higher increase in vaccination from early February to late March. Finally, many Southern states (e.g., Mississippi, Louisiana, Alabama, Oklahoma, Arkansas, and West Virginia) achieved a relatively low increase in vaccination between the two time frames. Sparsely populated states and less populous states achieved a higher rate of vaccination in comparison to more populated states.
Extant studies have mentioned that one of the main reasons for a low acceptance of vaccines is the inadequate supply and distribution of vaccines and low accessibility to vaccines. Considering this issue, we investigated the share of vaccine doses used from the actual distribution in different states of the US to gauge the status of vaccine dose utilization, as of 28 April (
Figure 14b). This figure shows a comparative scenario of differences between vaccine used and vaccine distributed across states.
This evidence verifies that Northeastern states have a higher percent usage of the distributed vaccines. Similarly, a significant use of distributed vaccine is observed in Western and Midwestern states. In contrast, Southern states showed a lower percent use of the distributed vaccine, which is consistent with the lower rate of vaccination uptake in these states as shown in
Figure 13.
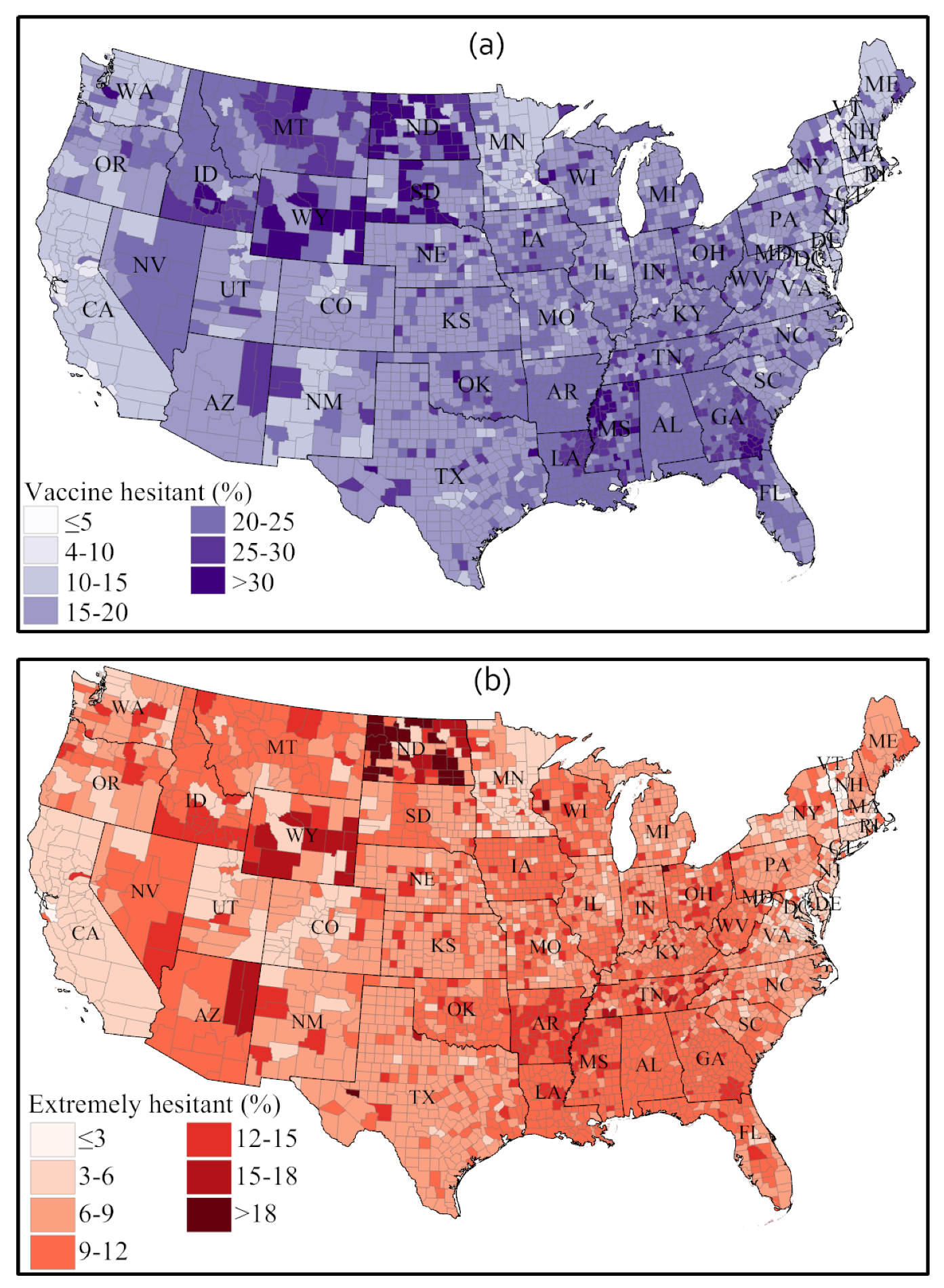
To understand the root causes of vaccine hesitancy among Americans, a recent nationwide Household Pulse Survey (HPS) conducted by the US Census Bureau (from 14 April to 26 April 2021) investigated the status of COVID-19 vaccine hesitancy at the county level of each state [
13]. Survey participants were asked the following question: “Once a vaccine to prevent COVID-19 is available to you, would you get a vaccine?” with following four options proposed as answers: (1) “definitely get a vaccine”, (2) “probably get a vaccine”, (3) “probably not get a vaccine”, and (4) “definitely not get a vaccine”.
The survey took the “probably not” and “definitely not” responses for vaccine hesitancy, while the “definitely not” option is defined as extreme vaccine hesitancy. The spatial representation of vaccine hesitancy in
Figure 15 indicates that many counties in Western states, parts of the Midwest, and parts of the South have a higher incidence of vaccine hesitancy and extreme vaccine hesitancy. Consistently with these survey results, a lower rate of vaccination was observed in most of these states.
Table 5 shows the prominent reasons for COVID-19 vaccine hesitancy reported in the HPS survey [
13]. The possible side effects of vaccines is reported as the main reason nationally (20.86%), whereas safety (17.04%) and trust (12.55%) of vaccines are the other two important reasons why Americans are hesitant to take the COVID-19 vaccine. Almost 10% of respondents also said they declined vaccination due to a lack of trust in the government.
In another study, the YouGov market research and data analytics firm, in association with the Institute of Global Health Innovation (IGHI) at Imperial College London (ICL), conducted surveys in 29 countries to gather global insights on people’s behaviors in response to COVID-19 [
66]. Respondents, who did not receive a COVID-19 vaccine, were asked to provide their responses on a scale of 1 (i.e., strongly agree) to 5 (i.e., strongly disagree) to the question: “If a COVID-19 vaccine were made available to me this week, I would definitely get it”.
Only 34.5% of US respondents expressed their willingness to receive a COVID-19 vaccine, which validates our findings from Twitter sentiment analysis (i.e., roughly 37% of US Twitter users expressed positive sentiment on the COVID-19 vaccine (
Figure 6)). As a point of comparison, in this international survey, UK residents had the highest positive responses overall (67.2%), followed by residents of Denmark (66.8%), Norway (58.5%), Germany (58%), and Italy (57.3%).
From our PSS-framework-based sentiment analysis of Twitter posts over two time periods in early 2021 (
Figure 11 and
Figure 12) and from the US state-wise actual vaccination scenarios over the same periods (
Figure 13,
Figure 14 and
Figure 15), we identified significant changes in sentiment from February to March and found that both the public sentiment and vaccination administration scenarios varied from one state to another state and have a strong correlation with population density and agglomeration, and with geographic location. Some of the notable key points are stated below.
Sentiments towards vaccination vary considerably across states and other place-based communities, like counties, and so do vaccination rates and hesitancy. We observed that less populous states and more sparsely populated states tend to have a higher vaccination rate; some of these states also have a strongly positive vaccination sentiment, but some also exhibit high vaccination hesitancy and less positive sentiments.
The Northeast region has a higher vaccination acceptance than other regions of the US. The strongest vaccine hesitancy is found across a number of southern states, such as Alabama, Georgia, Mississippi, Tennessee, and Arkansas. The Midwest and the West show mixed vaccine acceptance scenarios. Notably, Wyoming and Idaho show lower vaccine acceptance. In contrast, California, New Mexico, Arizona, and Colorado show a higher vaccination acceptance. The HPS survey found that side effects, trust in vaccine and in authority, safety, and efficiency are the main reasons for lower vaccination acceptance in these states.
Although positive sentiment declined and neutral sentiment increased in most states from February to March 2021, we found that most states improved their actual vaccine administration rate. We argued that this can be imputed to the increasing state-wise vaccine availability as time progresses.
Among the specific negative sentiments isolated from the Twitter corpus (including fear, which was discussed explicitly, but also sadness, anger, and disgust), fear is the sentiment that strengthened the most over time in most states.
The fear sentiment remained unchanged (between early February and late March) in populous states, like California, Texas, and New York), whereas a slight decline in trust sentiment was observed in these states.
Changes in sentiments were very abrupt among less populous states in the central parts of the US, including Wyoming, South Dakota, Kansas, New Mexico, and Arkansas.
In summary, as vaccine hesitancy exhibits significant variability from one state to another, state-wise policies need to be sensitive to these variations instead of adopting a “one size fits all” approach to increase the vaccination uptake. In
Section 5, we apply the PSS framework logic to propose public policies that could be adopted by local, state and federal governments to provide increased sensitivity to the masses and responsiveness to public sentiment, in the pursuit of herd immunity.


 ,
, 















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}