
PD-L1 Expression in Non-Small Cell Lung Cancer: Data from a Referral Center in Spain

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. PD-L1 Immunohistochemistry
2.3. Statistical Analysis
3. Results
3.1. Patient Cohort
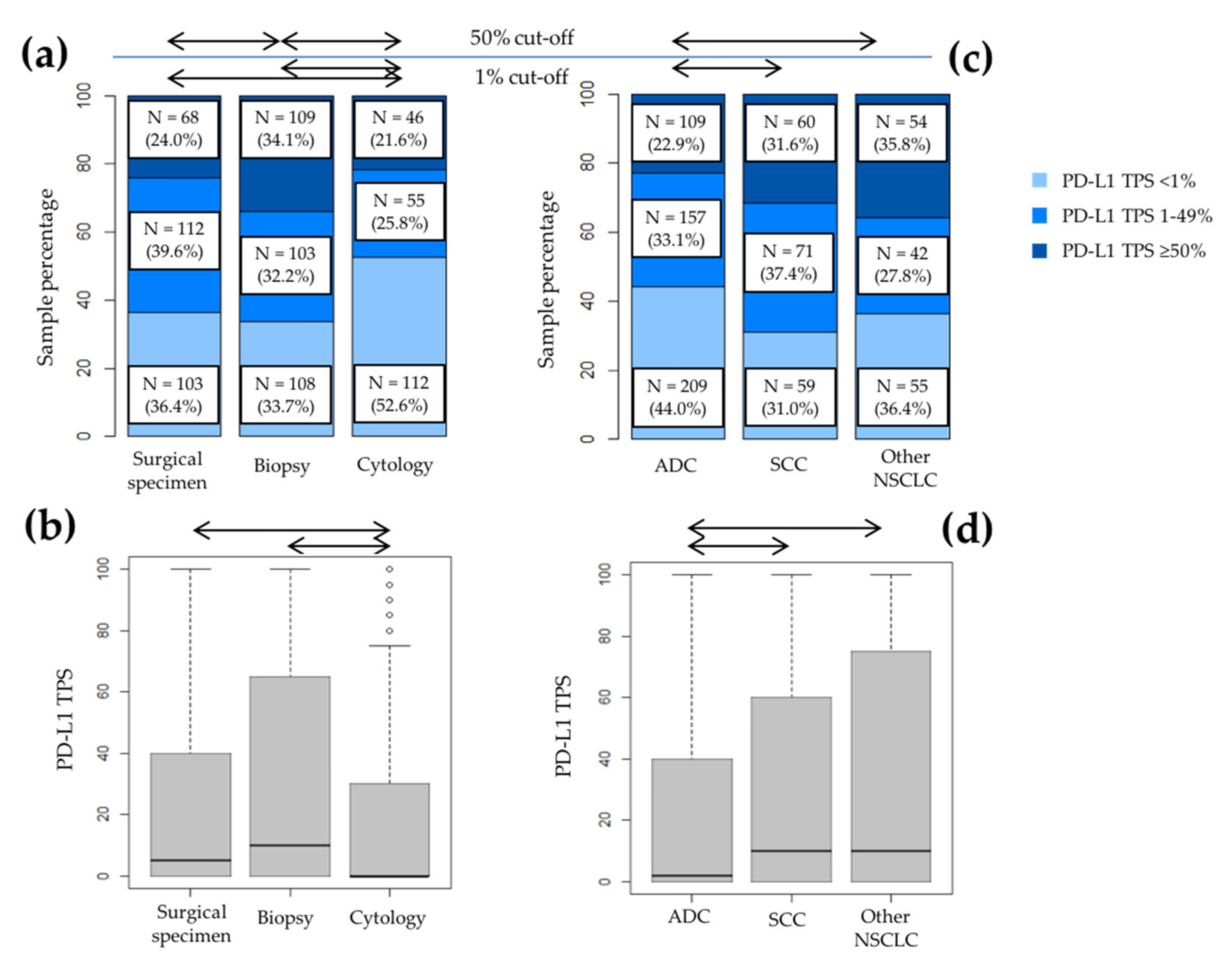
3.2. PD-L1 Expression and Patient Characteristics
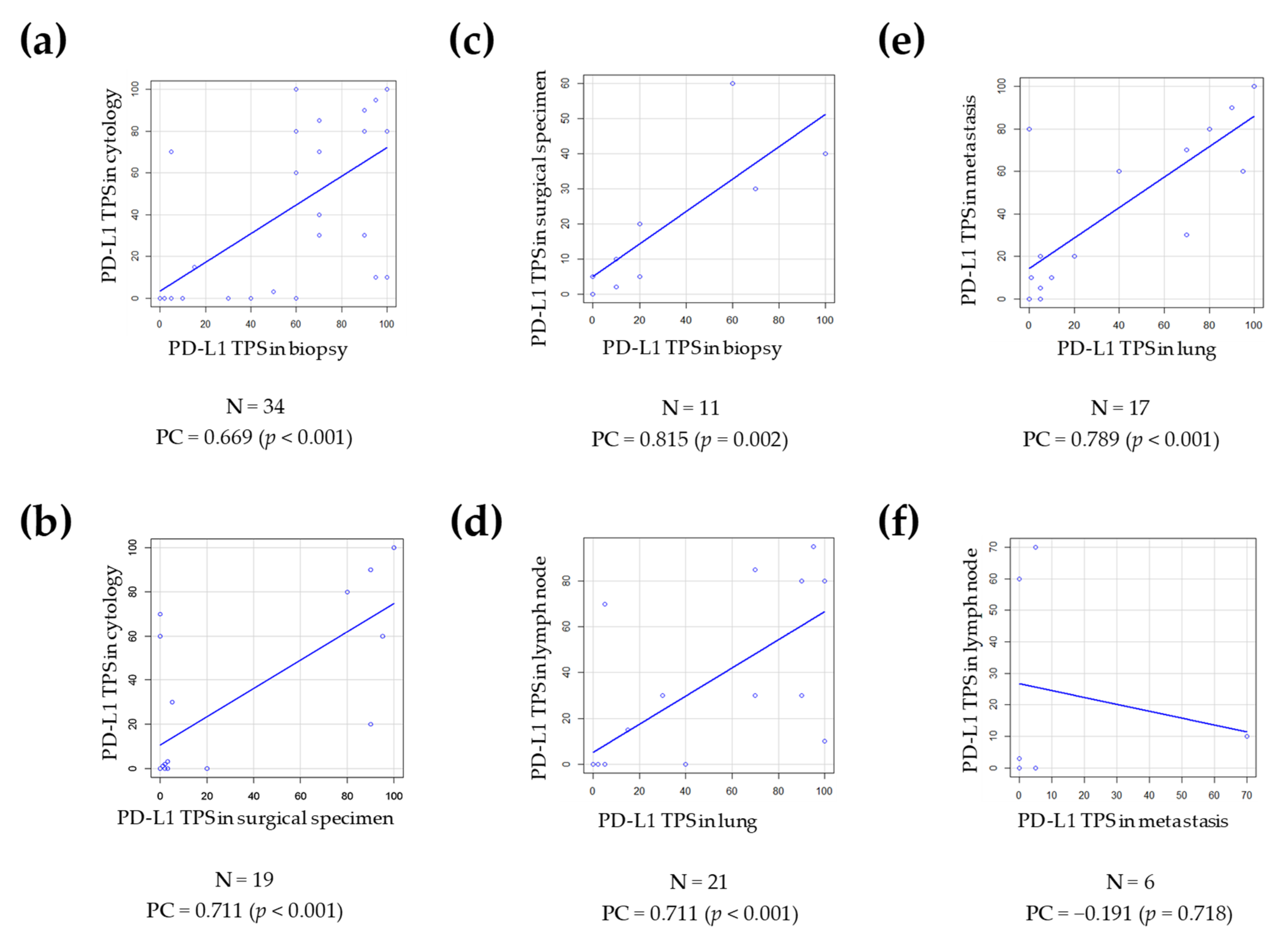
3.3. Agreement between the PD-L1 Results in Cases with More Than One Measurement in Different Samples
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brahmer, J.R.; Drake, C.G.; Wollner, I.; Powderly, J.D.; Picus, J.; Sharfman, W.H.; Stankevich, E.; Pons, A.; Salay, T.M.; McMiller, T.L.; et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 2010, 28, 3167–3175. [Google Scholar] [CrossRef]
- Davis, A.A.; Patel, V.G. The role of PD-L1 expression as a predictive biomarker: An analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 278. [Google Scholar] [CrossRef]
- Havel, J.J.; Chowell, D.; Chan, T.A. The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy. Nat. Rev. Cancer 2019, 19, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- Majem, M.; Juan, O.; Insa, A.; Reguart, N.; Trigo, J.M.; Carcereny, E.; García-Campelo, R.; García, Y.; Guirado, M.; Provencio, M. SEOM clinical guidelines for the treatment of non-small cell lung cancer (2018). Clin. Transl. Oncol. 2019, 21, 3–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, N.H.; Schneider, B.J.; Temin, S.; Baker, S.; Brahmer, J.; Ellis, P.M.; Gaspar, L.E.; Haddad, R.Y.; Hesketh, P.J.; Jain, D.; et al. Therapy for Stage IV Non-Small-Cell Lung Cancer Without Driver Alterations: ASCO and OH (CCO) Joint Guideline Update. J. Clin. Oncol. 2020, 38, 1608–1632. [Google Scholar] [CrossRef]
- Teixido, C.; Reguart, N. Using biomarkers to determine optimal combinations with immunotherapy (biomarker discovery perspective). Future Oncol. 2020, 16, 1677–1681. [Google Scholar] [CrossRef]
- Teixidó, C.; Vilariño, N.; Reyes, R.; Reguart, N. PD-L1 expression testing in non-small cell lung cancer. Ther. Adv. Med. Oncol. 2018, 10, 1758835918763493. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gumus, M.; Mazieres, J.; Hermes, B.; Cay Senler, F.; Csoszi, T.; Fulop, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Rodríguez-Abreu, D.; Powell, S.F.; Hochmair, M.J.; Gadgeel, S.; Esteban, E.; Felip, E.; Speranza, G.; De Angelis, F.; Dómine, M.; Cheng, S.Y.; et al. Pemetrexed Plus Platinum With or Without Pembrolizumab in Patients With Previously Untreated Metastatic Nonsquamous NSCLC: Protocol-Specified Final Analysis From KEYNOTE-189. Ann. Oncol. 2021, 32, 881–895. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Vicente, D.; Tafreshi, A.; Robinson, A.; Soto Parra, H.; Mazières, J.; Hermes, B.; Cicin, I.; Medgyasszay, B.; Rodríguez-Cid, J.; et al. A Randomized, Placebo-Controlled Trial of Pembrolizumab Plus Chemotherapy in Patients With Metastatic Squamous NSCLC: Protocol-Specified Final Analysis of KEYNOTE-407. J. Thorac. Oncol. 2020, 15, 1657–1669. [Google Scholar] [CrossRef]
- Reck, M.; Mok, T.S.K.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): Key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir. Med. 2019, 7, 387–401. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Vokes, E.E.; Ready, N.; Felip, E.; Horn, L.; Burgio, M.A.; Antonia, S.J.; Arén Frontera, O.; Gettinger, S.; Holgado, E.; Spigel, D.; et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann. Oncol. 2018, 29, 959–965. [Google Scholar] [CrossRef]
- Cheung, C.C.; Barnes, P.; Bigras, G.; Boerner, S.; Butany, J.; Calabrese, F.; Couture, C.; Deschenes, J.; El-Zimaity, H.; Fischer, G.; et al. Fit-For-Purpose PD-L1 Biomarker Testing For Patient Selection in Immuno-Oncology: Guidelines For Clinical Laboratories From the Canadian Association of Pathologists-Association Canadienne Des Pathologistes (CAP-ACP). Appl. Immunohistochem. Mol. Morphol. 2019, 27, 699–714. [Google Scholar] [CrossRef]
- Lantuejoul, S.; Sound-Tsao, M.; Cooper, W.A.; Girard, N.; Hirsch, F.R.; Roden, A.C.; Lopez-Rios, F.; Jain, D.; Chou, T.Y.; Motoi, N.; et al. PD-L1 Testing for Lung Cancer in 2019: Perspective From the IASLC Pathology Committee. J. Thorac. Oncol. 2020, 15, 499–519. [Google Scholar] [CrossRef]
- Tsao, M.S.; Kerr, K.M.; Dacic, S.; Yatabe, Y.; Hirsch, F.R. IASLC Atlas of PD-L1 Immunohistochemistry Testing in Lung Cancer, 1st ed.; Editorial Rx Press: Aurora, CO, USA, 2017. [Google Scholar]
- Martin-Deleon, R.; Teixido, C.; Lucena, C.M.; Martinez, D.; Fontana, A.; Reyes, R.; García, M.; Viñolas, N.; Vollmer, I.; Sanchez, M.; et al. EBUS-TBNA Cytological Samples for Comprehensive Molecular Testing in Non-Small Cell Lung Cancer. Cancers 2021, 13, 2084. [Google Scholar] [CrossRef] [PubMed]
- Velcheti, V.; Patwardhan, P.D.; Liu, F.X.; Chen, X.; Cao, X.; Burke, T. Real-world PD-L1 testing and distribution of PD-L1 tumor expression by immunohistochemistry assay type among patients with metastatic non-small cell lung cancer in the United States. PLoS ONE 2018, 13, e0206370. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.; Negrao, M.V.; Dibaj, S.S.; Chen, R.; Reuben, A.; Bohac, J.M.; Liu, X.; Skoulidis, F.; Gay, C.M.; Cascone, T.; et al. Programmed Death-Ligand 1 Heterogeneity and Its Impact on Benefit From Immune Checkpoint Inhibitors in NSCLC. J. Thorac. Oncol. 2020, 15, 1449–1459. [Google Scholar] [CrossRef] [PubMed]
- Tsao, M.S.; Le Teuff, G.; Shepherd, F.A.; Landais, C.; Hainaut, P.; Filipits, M.; Pirker, R.; Le Chevalier, T.; Graziano, S.; Kratze, R.; et al. PD-L1 protein expression assessed by immunohistochemistry is neither prognostic nor predictive of benefit from adjuvant chemotherapy in resected non-small cell lung cancer. Ann. Oncol. 2017, 28, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Huang, Y.; Zeng, X.; Chen, X.; Shao, S.; Jin, Y.; Xue, Q.; Wang, Y.; Guo, Y.; Gu, B.; et al. Clinicopathological and molecular characteristics associated with PD-L1 expression in non-small cell lung cancer: A large-scale, multi-center, real-world study in China. J. Cancer Res. Clin. Oncol. 2021, 147, 1547–1556. [Google Scholar] [CrossRef] [PubMed]
- Gagné, A.; Wang, E.; Bastien, N.; Orain, M.; Desmeules, P.; Pagé, S.; Trahan, S.; Couture, C.; Joubert, D.; Joubert, P. Impact of Specimen Characteristics on PD-L1 Testing in Non-Small Cell Lung Cancer: Validation of the IASLC PD-L1 Testing Recommendations. J. Thorac. Oncol. 2019, 14, 2062–2070. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, F.; Nankivell, M.; Adizie, J.B.; Maqsood, U.; Elshafi, M.; Jafri, S.; Lerner, A.D.; Woolhouse, I.; Munavvar, M.; Evison, M.; et al. Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration for PD-L1 Testing in Non-small Cell Lung Cancer. Chest 2020, 158, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, T.; Marushima, H.; Saji, H.; Kojima, K.; Hoshikawa, M.; Takagi, M.; Nakamura, H. PD-L1 Expression in Non-Small-Cell Lung Cancer Including Various Adenocarcinoma Subtypes. Ann. Thorac. Cardiovasc. Surg. 2019, 25, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosney, J.R.; Boothman, A.M.; Ratcliffe, M.; Kerr, K.M. Cytology for PD-L1 testing: A systematic review. Lung Cancer 2020, 141, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Koomen, B.M.; van der Starre-Gaal, J.; Vonk, J.M.; von der Thüsen, J.H.; van der Meij, J.J.C.; Monkhorst, K.; Willems, S.M.; Timens, W.; ’t Hart, N.A. Formalin fixation for optimal concordance of programmed death-ligand 1 immunostaining between cytologic and histologic specimens from patients with non-small cell lung cancer. Cancer Cytopathol. 2021, 129, 304–317. [Google Scholar] [CrossRef]
- Gradecki, S.E.; Grange, J.S.; Stelow, E.B. Concordance of PD-L1 Expression Between Core Biopsy and Resection Specimens of Non-Small Cell Lung Cancer. Am. J. Surg. Pathol. 2018, 42, 1090–1094. [Google Scholar] [CrossRef]
- Giunchi, F.; Degiovanni, A.; Daddi, N.; Trisolini, R.; Dell’Amore, A.; Agostinelli, C.; Ardizzoni, A.; Fiorentino, M. Fading With Time of PD-L1 Immunoreactivity in Non-Small Cells Lung Cancer Tissues: A Methodological Study. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 489–494. [Google Scholar] [CrossRef]
- Cho, J.H.; Sorensen, S.F.; Choi, Y.L.; Feng, Y.; Kim, T.E.; Choi, H.; Georgsen, J.B.; Dolled-Filhart, M.; Emancipator, K.; Meldgaard, P.; et al. Programmed Death Ligand 1 Expression in Paired Non-Small Cell Lung Cancer Tumor Samples. Clin. Lung Cancer 2017, 18, e473–e479. [Google Scholar] [CrossRef]
- Kim, S.; Koh, J.; Kwon, D.; Keam, B.; Go, H.; Kim, Y.A.; Jeon, Y.K.; Chung, D.H. Comparative analysis of PD-L1 expression between primary and metastatic pulmonary adenocarcinomas. Eur. J. Cancer 2017, 75, 141–149. [Google Scholar] [CrossRef]
- Mansfield, A.S.; Aubry, M.C.; Moser, J.C.; Harrington, S.M.; Dronca, R.S.; Park, S.S.; Dong, H. Temporal and spatial discordance of programmed cell death-ligand 1 expression and lymphocyte tumor infiltration between paired primary lesions and brain metastases in lung cancer. Ann. Oncol. 2016, 27, 1953–1958. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristic | N (%) | PD-L1 TPS | p-Value | |||
|---|---|---|---|---|---|---|
| <1% (%) | 1–49% (%) | ≥50% (%) | ||||
| Gender | Men | 569 (69.73) | 233 (40.9) | 182 (32.0) | 154 (27.1) | 0.444 |
| Women | 247 (30.27) | 90 (36.5) | 883 (35.6) | 69 (27.9) | ||
| Age | ≤65 years | 353 (43.26) | 145 (41.1) | 114 (32.3) | 94 (26.6) | 0.748 |
| >65 years | 463 (56.74) | 178 (38.4) | 156 (33.7) | 129 (27.9) | ||
| Sample type | Surgical specimen | 283 (34.68) | 103 (36.4) | 112 (39.6) | 68 (24.0) | <0.001 |
| Biopsy | 320 (39.22) | 108 (33.7) | 103 (32.2) | 109 (34.1) | ||
| Cytology | 213 (26.10) | 112 (52.6) | 55 (25.8) | 46 (21.6) | ||
| Site of sample | Lung—bronchus | 541 (66.30) | 207 (38.3) | 180 (33.3) | 154 (28.5) | 0.458 |
| Lymph node | 115 (14.09) | 54 (47.0) | 33 (28.7) | 28 (24.3) | ||
| Distant metastasis | 160 (19.61) | 62 (38.8) | 57 (35.6) | 41 (25.6) | ||
| Histology | Adenocarcinoma | 475 (58.21) | 209 (44.0) | 157 (33.1) | 109 (22.9) | 0.002 |
| Squamous carcinoma | 190 (23.28) | 59 (31.1) | 71 (37.4) | 60 (31.6) | ||
| Other NSCLC | 151 (18.51) | 55 (36.4) | 42 (27.8) | 54 (35.8) | ||
| Clinical Characteristic | As a Continuous Variable | PD-L1 TPS 1% Cut-Off | PD-L1 TPS 50% Cut-Off | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | Mean | p-Value | <1 N (%) | ≥1 N (%) | p-Value | <50 N (%) | ≥50 N (%) | p-Value | ||
| Gender | Male | 3 | 25.17 | 0.157 | 233 (40.9) | 336 (59.1) | 0.226 | 415 (72.9) | 154 (27.1) | 0.798 |
| Female | 5 | 27.83 | 90 (36.4) | 157 (63.6) | 178 (72.1) | 69 (27.9) | ||||
| Age | ≤65 years | 3 | 25.95 | 0.619 | 145 (41.1) | 208 (58.9) | 0.446 | 259 (73.4) | 94 (26.6) | 0.695 |
| >65 years | 5 | 26.00 | 178 (38.4) | 285 (61.6) | 334 (72.1) | 129 (27.9) | ||||
| Sample type | Surgical specimen | 5 | 24.61 | <0.001 | 103(36.4) | 180 (63.6) | <0.001 | 215(76.0) | 68 (24.0) | 0.002 |
| Biopsy | 10 | 31.47 | 108 (33.8) | 212 (66.2) | 211 (65.9) | 109 (34.1) | ||||
| Cytology | 0 | 19.55 | 112 (52.6) | 101 (47.4) | 167 (78.4) | 46 (21.6) | ||||
| Site of sample | Lung—bronchus | 5 | 26.70 | 0.359 | 207 (38.3) | 334 (61.7) | 0.217 | 387 (71.5) | 154 (28.5) | 0.577 |
| Lymph node | 2 | 23.22 | 54 (47.0) | 61 (53.0) | 87 (75.7) | 28 (24.3) | ||||
| Distant metastasis | 5 | 25.52 | 62 (38.8) | 98 (61.2) | 119 (74.4) | 41 (25.6) | ||||
| Histology | Adenocarcinoma | 2 | 22.16 | 0.001 | 209 (44.0) | 266 (56.0) | 0.006 | 366 (77.1) | 109 (22.9) | 0.003 |
| Squamous carcinoma | 10 | 29.51 | 59 (31.1) | 131 (68.9) | 130 (68.4) | 60 (31.6) | ||||
| Other NSCLC | 10 | 33.55 | 55 (36.4) | 96 (63.6) | 97 (64.2) | 54 (35.8) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saez de Gordoa, K.; Lopez, I.; Marginet, M.; Coloma, B.; Frigola, G.; Vega, N.; Martinez, D.; Teixido, C. PD-L1 Expression in Non-Small Cell Lung Cancer: Data from a Referral Center in Spain. Diagnostics 2021, 11, 1452. https://doi.org/10.3390/diagnostics11081452
Saez de Gordoa K, Lopez I, Marginet M, Coloma B, Frigola G, Vega N, Martinez D, Teixido C. PD-L1 Expression in Non-Small Cell Lung Cancer: Data from a Referral Center in Spain. Diagnostics. 2021; 11(8):1452. https://doi.org/10.3390/diagnostics11081452
Chicago/Turabian StyleSaez de Gordoa, Karmele, Ingrid Lopez, Marta Marginet, Berta Coloma, Gerard Frigola, Naiara Vega, Daniel Martinez, and Cristina Teixido. 2021. "PD-L1 Expression in Non-Small Cell Lung Cancer: Data from a Referral Center in Spain" Diagnostics 11, no. 8: 1452. https://doi.org/10.3390/diagnostics11081452