
Artificial Intelligence in Differential Diagnostics of Meningitis: A Nationwide Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients, Setting, Laboratory Testing, and Diagnosis
2.2. Predicting the Type of Meningitis
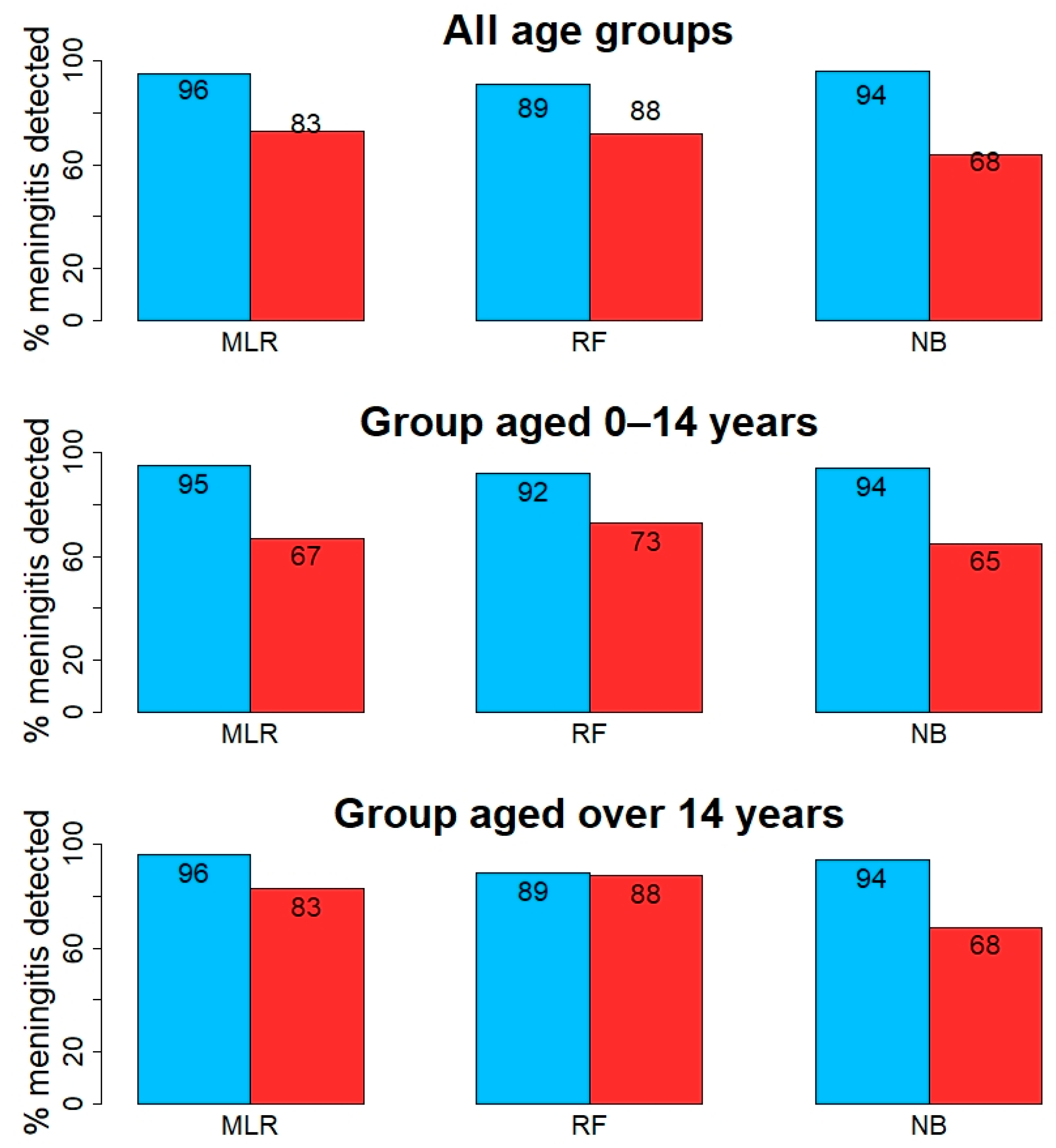
3. Results
3.1. Differential Diagnosis of Meningitis
3.1.1. Group Aged 0–14 Years
3.1.2. Age Group over 14 Years
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stephens, D.S.; Greenwood, B.; Brandtzaeg, P. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet 2007, 369, 2196–2210. [Google Scholar] [CrossRef]
- Black, S.; Pizza, M.; Nissum, M.; Rappuoli, R. Toward a meningitis-free world. Sci. Transl. Med. 2012, 4, 123ps125. [Google Scholar] [CrossRef]
- Harvala, H.; Simmonds, P. Viral meningitis: Epidemiology and diagnosis. Lancet Infect. Dis. 2016, 16, 1211–1212. [Google Scholar] [CrossRef]
- Reese, H.E.; Ronveaux, O.; Mwenda, J.M.; Bita, A.; Cohen, A.L.; Novak, R.T.; Fox, L.M.; Soeters, H.M. Invasive Meningococcal Disease in Africa’s Meningitis Belt: More Than Just Meningitis? J. Infect. Dis. 2019, 220, S263–S265. [Google Scholar] [CrossRef] [PubMed]
- Posnakoglou, L.; Siahanidou, T.; Syriopoulou, V.; Michos, A. Impact of cerebrospinal fluid syndromic testing in the management of children with suspected central nervous system infection. Eur. J. Clin. Microbiol. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Giulieri, S.; Chapuis-Taillard, C.; Jaton, K.; Cometta, A.; Chuard, C.; Hugli, O.; Du Pasquier, R.; Bille, J.; Meylan, P.; Manuel, O.; et al. CSF lactate for accurate diagnosis of community-acquired bacterial meningitis. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 2049–2055. [Google Scholar] [CrossRef]
- Brooks, J.A.; McCudden, C.; Breiner, A.; Bourque, P.R. Causes of albuminocytological dissociation and the impact of age-adjusted cerebrospinal fluid protein reference intervals: A retrospective chart review of 2627 samples collected at tertiary care centre. BMJ Open 2019, 9, e025348. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.R.; Sample, H.A.; Zorn, K.C.; Arevalo, S.; Yu, G.; Neuhaus, J.; Federman, S.; Stryke, D.; Briggs, B.; Langelier, C.; et al. Clinical Metagenomic Sequencing for Diagnosis of Meningitis and Encephalitis. N. Engl. J. Med. 2019, 380, 2327–2340. [Google Scholar] [CrossRef] [PubMed]
- Bartholomeus, E.; De Neuter, N.; Lemay, A.; Pattyn, L.; Tuerlinckx, D.; Weynants, D.; Van Lede, K.; van Berlaer, G.; Bulckaert, D.; Boiy, T.; et al. Diagnosing enterovirus meningitis via blood transcriptomics: An alternative for lumbar puncture? J. Transl. Med. 2019, 17, 282. [Google Scholar] [CrossRef] [Green Version]
- Sampson, D.; Yager, T.D.; Fox, B.; Shallcross, L.; McHugh, L.; Seldon, T.; Rapisarda, A.; Brandon, R.B.; Navalkar, K.; Simpson, N. Blood transcriptomic discrimination of bacterial and viral infections in the emergency department: A multi-cohort observational validation study. BMC Med. 2020, 18, 185. [Google Scholar]
- Luo, G.; Gao, Q.; Zhang, S.; Yan, B. Probing infectious disease by single-cell RNA sequencing: Progresses and perspectives. Comput. Struct. Biotechnol. J. 2020, 18, 2962–2971. [Google Scholar] [CrossRef]
- Mentis, A.F.; Kyprianou, M.A.; Xirogianni, A.; Kesanopoulos, K.; Tzanakaki, G. Neutrophil-to-lymphocyte ratio in the differential diagnosis of acute bacterial meningitis. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Mentis, A.A.; Kyprianou, M.A.; Tzanakaki, G. Age-specific application of neutrophil-to-lymphocyte ratio in meningitis: A nationwide study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1553–1557. [Google Scholar] [CrossRef]
- Tzanakaki, G.; Paparoupa, M.; Kyprianou, M.; Barbouni, A.; Eugen-Olsen, J.; Kourea-Kremastinou, J. Elevated soluble urokinase receptor values in CSF, age and bacterial meningitis infection are independent and additive risk factors of fatal outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Tzanakaki, G.; Tsopanomichalou, M.; Kesanopoulos, K.; Matzourani, R.; Sioumala, M.; Tabaki, A.; Kremastinou, J. Simultaneous single-tube PCR assay for the detection of Neisseria meningitidis, Haemophilus influenzae type b and Streptococcus pneumoniae. Clin. Microbiol. Infect. 2005, 11, 386–390. [Google Scholar] [CrossRef] [Green Version]
- Xirogianni, A.; Tzanakaki, G.; Karagianni, E.; Markoulatos, P.; Kourea-Kremastinou, J. Development of a single-tube polymerase chain reaction assay for the simultaneous detection of Haemophilus influenzae, Pseudomonas aeruginosa, Staphylococcus aureus, and Streptococcus spp. directly in clinical samples. Diagn. Microbiol. Infect. Dis. 2009, 63, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Ullah, W.; Basyal, B.; Tariq, S.; Almas, T.; Saeed, R.; Roomi, S.; Haq, S.; Madara, J.; Boigon, M.; Haas, D.C. Lymphocyte-to-C-Reactive Protein Ratio: A Novel Predictor of Adverse Outcomes in COVID-19. J. Clin. Med. Res. 2020, 12, 415–422. [Google Scholar] [CrossRef]
- Ford, B.A.; McElvania, E. Machine learning takes laboratory automation to the next level. J. Clin. Microbiol. 2020, 58, e00012-20. [Google Scholar] [CrossRef] [Green Version]
- Rivera, S.C.; Liu, X.; Chan, A.-W.; Denniston, A.K.; Calvert, M.J. Guidelines for clinical trial protocols for interventions involving artificial intelligence: The SPIRIT-AI extension. BMJ 2020, 370. [Google Scholar] [CrossRef]
- Cupp, M.A.; Cariolou, M.; Tzoulaki, I.; Aune, D.; Evangelou, E.; Berlanga-Taylor, A.J. Neutrophil to lymphocyte ratio and cancer prognosis: An umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020, 18, 360. [Google Scholar] [CrossRef]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Kavakiotis, I.; Tsave, O.; Salifoglou, A.; Maglaveras, N.; Vlahavas, I.; Chouvarda, I. Machine learning and data mining methods in diabetes research. Comput. Struct. Biotechnol. J. 2017, 15, 104–116. [Google Scholar] [CrossRef]
- Bravo-Merodio, L.; Acharjee, A.; Hazeldine, J.; Bentley, C.; Foster, M.; Gkoutos, G.V.; Lord, J.M. Machine learning for the detection of early immunological markers as predictors of multi-organ dysfunction. Sci. Data 2019, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uddin, S.; Khan, A.; Hossain, M.E.; Moni, M.A. Comparing different supervised machine learning algorithms for disease prediction. BMC Med. Inf. Decis. Mak. 2019, 19, 281. [Google Scholar] [CrossRef] [PubMed]
- Ramgopal, S.; Horvat, C.M.; Yanamala, N.; Alpern, E.R. Machine learning to predict serious bacterial infections in young febrile infants. Pediatrics 2020, 146, e20194096. [Google Scholar] [CrossRef]
- Flores, M.; Glusman, G.; Brogaard, K.; Price, N.D.; Hood, L. P4 medicine: How systems medicine will transform the healthcare sector and society. Pers. Med. 2013, 10, 565–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mentis, A.-F.A.; Pantelidi, K.; Dardiotis, E.; Hadjigeorgiou, G.M.; Petinaki, E. Precision medicine and global health: The good, the bad, and the ugly. Front. Med. 2018, 5, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aschenbrenner, A.C.; Mouktaroudi, M.; Kraemer, B.; Oestreich, M.; Antonakos, N.; Nuesch-Germano, M.; Gkizeli, K.; Bonaguro, L.; Reusch, N.; Baßler, K. Disease severity-specific neutrophil signatures in blood transcriptomes stratify COVID-19 patients. Genome Med. 2021, 13, 7. [Google Scholar] [CrossRef]


{kind=link}
| Covariates | Total Number of Cases | Viral Cases | Bacterial Cases |
|---|---|---|---|
| G1 = CSF Neutrophils + CSF Lymphocytes | 1860 | 1005 (54%) | 855 (46%) |
| G2 = G1 + CSF NLR | 1844 | 1002 (54%) | 842 (46%) |
| G3 = G2 + Blood Albumin | 1684 | 932 (55%) | 752 (45%) |
| G4 = G3 + Gender + Group | 1668 | 918 (55%) | 750 (45%) |
| G5 = G4 + Blood Glucose | 1606 | 911 (57%) | 695 (43%) |
| G6 = G5 + Blood CRP | 955 | 553 (58%) | 402 (42%) |
| G7 = G6 + Blood suPAR | 125 | 69 (55%) | 56 (45%) |
| G8 = G7 + LCR | 125 | 69 (55%) | 56 (45%) |
| ML Algorithm | Percentage of Viral Meningitis Detected: Mean Value and CI (95%) | Percentage of Bacterial Meningitis Detected: Mean Value and CI (95%) | Most Important Predictor |
|---|---|---|---|
| Table 2a | |||
| MLR | 96% (92%, 99%) | 49% (40%, 58%) | CSF Neutrophils |
| RF | 86% (79%, 90%) | 61% (51%, 70%) | CSF Neutrophils |
| NB | 96% (94%, 99%) | 44% (35%, 54%) | NA |
| Table 2b | |||
| MLR | 95% (91%, 97%) | 68% (61%, 75%) | NLR |
| RF | 87% (81%, 90%) | 78% (70%, 82%) | CSF Neutrophils |
| NB | 96% (92%, 98%) | 60% (50%, 68%) | NA |
| Table 2c | |||
| MLR | 96% (93%, 99%) | 66% (58%, 74%) | NLR |
| RF | 91% (86%, 65%) | 72% (65%, 79%) | CSF Neutrophils |
| NB | 95% (91%, 98%) | 63% (53%, 71%) | NA |
| Table 2d | |||
| MLR | 95% (92%, 98%) | 73% (66%, 79%) | NLR |
| RF | 90% (85%, 93%) | 71% (64%, 79%) | CSF Neutrophils |
| NB | 96% (93%, 99%) | 64% (56%, 73%) | NA |
| Table 2e | |||
| MLR | 95% (92%, 98%) | 73% (66%, 79%) | NLR |
| RF | 90% (85%, 93%) | 78% (72%, 84%) | CSF Neutrophils |
| NB | 95% (92%, 98%) | 66% (59%, 74%) | NA |
| Table 2f | |||
| MLR | 95% (90%, 99%) | 62% (50%, 74%) | NLR |
| RF | 91% (86%, 95%) | 76% (70%, 83%) | NLR |
| NB | 96% (92%, 100%) | 52% (38%, 66%) | NA |
| Table 2g | |||
| MLR | 86% (63%, 100%) | 72% (43%, 100%) | NLR |
| RF | 93% (87%, 97%) | 69% (57%, 81%) | NLR |
| NB | 88% (67%, 100%) | 64% (22%, 89%) | NA |
| ML Algorithm | Percentage of Viral Meningitis Detected: Mean Value and CI (95%) | Percentage of Bacterial Meningitis Detected: Mean Value and CI (95%) | Most important predictor |
|---|---|---|---|
| Table 3a | |||
| MLR | 97% (94%, 99%) | 56% (46%, 66%) | CSF Neutrophils |
| RF | 89% (83%, 94%) | 67% (56%, 76%) | CSF Neutrophils |
| NB | 96% (93%, 99%) | 42% (32%, 52%) | NA |
| Table 3b | |||
| MLR | 96% (93% 99%) | 61% (50%, 72%) | NLR |
| RF | 89% (83%, 94%) | 66% (55%, 76%) | CSF Neutrophils |
| NB | 95% (92%, 98%) | 55% (44%, 65%) | NA |
| Table 3c | |||
| MLR | 96% (93%, 99%) | 63% (53%, 74%) | NLR |
| RF | 90% (85%, 95%) | 67% (57%, 77%) | CSF Neutrophils |
| NB | 95% (91%, 98%) | 60% (50%, 71%) | NA |
| Table 3d | |||
| MLR | 95% (90%, 98%) | 63% (53%, 74%) | CSF Neutrophils |
| RF | 90% (85%, 95%) | 67% (57%, 77%) | CSF Neutrophils |
| NB | 95% (91%, 98%) | 60% (50%, 71%) | NA |
| Table 3e | |||
| MLR | 95% (91%, 99%) | 67% (56%, 78%) | NLR |
| RF | 90% (83%, 96%) | 70% (58%, 81%) | CSF Neutrophils |
| NB | 94% (89%, 99%) | 65% (53%, 77%) | NA |
| Table 3f | |||
| MLR | 89%% (73%, 100%) | 67% (33%, 100%) | NLR |
| RF | 84%% (58%, 100%) | 69%% (33%, 97%) | NLR |
| NB | 86% (64%, 97%) | 61% (29%, 97%) | NA |
| Table 3g | |||
| MLR | 86% (64%, 100%) | 61% (29%, 97%) | NLR |
| RF | 92% (77%, 100%) | 73% (41%, 97%) | NLR |
| NB | 85%% (61%, 100%) | 66% (33%, 97%) | NA |
| ML Algorithm | Percentage of Viral Meningitis Detected: Mean Value and CI (95%) | Percentage of Bacterial Meningitis Detected: Mean Value and CI (95%) | Most Important Predictor |
|---|---|---|---|
| Table 4a | |||
| MLR | 97% (94%, 100%) | 75% (67%, 82%) | CSF Neutrophils |
| RF | 82% (71%, 91%) | 86% (79%, 92%) | CSF Neutrophils |
| NB | 97% (91%, 100%) | 51% (40%, 65%) | NA |
| Table 4b | |||
| MLR | 96% (91%, 100%) | 83% (75%, 90%) | NLR |
| RF | 84% (75%, 92%) | 85% (78%, 91%) | CSF Neutrophils |
| NB | 96% (90%, 100%) | 65% (53%, 79%) | NA |
| Table 4c | |||
| MLR | 95% (89%, 100%) | 83% (75%, 90%) | NLR |
| RF | 87% (78%, 95%) | 87% (80%, 93%) | CSF Neutrophils |
| NB | 94% (89%, 98%) | 68% (58%, 81%) | NA |
| Table 4d | |||
| MLR | 95% (89%, 100%) | 81% (74%, 89%) | CSF Neutrophils |
| RF | 89% (80%, 96%) | 88% (80%, 94%) | CSF Neutrophils |
| NB | 94% (88%, 100%) | 65% (51%, 79%) | NA |
| Table 4e | |||
| MLR | 94% (84%, 100%) | 82% (70%, 93%) | NLR |
| RF | 89% (76%, 100%) | 87% (73%, 97%) | CSF Neutrophils |
| NB | 95% (84%, 100%) | 59% (37%, 82%) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mentis, A.-F.A.; Garcia, I.; Jiménez, J.; Paparoupa, M.; Xirogianni, A.; Papandreou, A.; Tzanakaki, G. Artificial Intelligence in Differential Diagnostics of Meningitis: A Nationwide Study. Diagnostics 2021, 11, 602. https://doi.org/10.3390/diagnostics11040602
Mentis A-FA, Garcia I, Jiménez J, Paparoupa M, Xirogianni A, Papandreou A, Tzanakaki G. Artificial Intelligence in Differential Diagnostics of Meningitis: A Nationwide Study. Diagnostics. 2021; 11(4):602. https://doi.org/10.3390/diagnostics11040602
Chicago/Turabian StyleMentis, Alexios-Fotios A., Irene Garcia, Juan Jiménez, Maria Paparoupa, Athanasia Xirogianni, Anastasia Papandreou, and Georgina Tzanakaki. 2021. "Artificial Intelligence in Differential Diagnostics of Meningitis: A Nationwide Study" Diagnostics 11, no. 4: 602. https://doi.org/10.3390/diagnostics11040602