
Altered Gene Expression Encoding Cytochines, Grow Factors and Cell Cycle Regulators in the Endometrium of Women with Chronic Endometritis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Interventions
2.3. Gene Expression Profiling
3. Results
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Greenwood, S.M.; Moran, J.J. Chronic endometritis: Morphologic and clinical observations. Obstet. Gynecol. 1981, 58, 176–184. [Google Scholar]
- Cicinelli, E.; De Ziegler, D.; Nicoletti, R.; Colafiglio, G.; Saliani, N.; Resta, L.; Rizzi, D.; De Vito, D. Chronic endometritis: Correlation among hysteroscopic, histologic, and bacteriologic findings in a prospective trial with 2190 consecutive office hysteroscopies. Fertil. Steril. 2008, 89, 677–684. [Google Scholar] [CrossRef]
- Vitagliano, A.; Saccardi, C.; Noventa, M.; Di Spiezio Sardo, A.; Saccone, G.; Cicinelli, E.; Pizzi, S.; Andrisani, A.; Litta, P.S. Effects of chronic endometritis therapy on in vitro fertilization outcome in women with repeated implantation failure: A systematic review and meta-analysis. Fertil. Steril. 2018, 110, 103–112. [Google Scholar] [CrossRef]
- De Ziegler, D.; Pirtea, P.; Galliano, D.; Cicinelli, E.; Meldrum, D. Optimal uterine anatomy and physiology necessary for normal implantation and placentation. Fertil. Steril. 2016, 105, 844–854. [Google Scholar] [CrossRef] [Green Version]
- Cicinelli, E.; Matteo, M.; Tinelli, R.; Lepera, A.; Alfonso, R.; Indraccolo, U.; Marrocchella, S.; Greco, P.; Resta, L. Prevalence of chronic endometritis in repeated unexplained implantation failure and the IVF success rate after antibiotic therapy. Hum. Reprod. 2015, 30, 323–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston-MacAnanny, E.B.; Hartnett, J.; Engmann, L.L.; Nulsen, J.C.; Sanders, M.M.; Benadiva, C.A. Chronic endometritis is a frequent finding in women with recurrent implantation failure after in vitro fertilization. Fertil. Steril. 2010, 93, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, H.; Liu, Y.; Zheng, S.; Zhao, W.; Wu, D.; Lei, L.; Chen, G. Confirmation of chronic endometritis in repeated implantation failure and success outcome in IVF-ET after intrauterine delivery of the combined administration of antibiotic and dexamethasone. Am. J. Reprod. Immunol. 2019, 82. [Google Scholar] [CrossRef] [PubMed]
- McQueen, D.B.; Perfetto, C.O.; Hazard, F.K.; Lathi, R.B. Pregnancy outcomes in women with chronic endometritis and recurrent pregnancy loss. Fertil. Steril. 2015, 104, 927–931. [Google Scholar] [CrossRef] [Green Version]
- Kitaya, K.; Takeuchi, T.; Mizuta, S.; Matsubayashi, H.; Ishikawa, T. Endometritis: New time, new concepts. Fertil. Steril. 2018, 110, 344–350. [Google Scholar] [CrossRef]
- Cicinelli, E.; Vitagliano, A.; Kumar, A.; Lasmar, R.B.; Bettocchi, S.; Haimovich, S.; International Working Group for Standardization of Chronic Endometritis Diagnosis. Unified diagnostic criteria for chronic endometritis at fluid hysteroscopy: Proposal and reliability evaluation through an international randomized-controlled observer study. Fertil. Steril. 2019, 112, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Kitaya, K.; Yasuo, T. Immunohistochemistrical and clinicopathological characterization of chronic endometritis. Am. J. Reprod. Immunol. 2011, 66, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, E.; Bettocchi, S.; De Ziegler, D.; Loizzi, V.; Cormio, G.; Marinaccio, M.; Trojano, G.; Crupano, F.M.; Francescato, R.; Vitagliano, A.; et al. Chronic Endometritis, a Common Disease Hidden Behind Endometrial Polyps in Premenopausal Women: First Evidence from a Case-Control Study. J. Minim. Invasive Gynecol. 2019, 26, 1346–1350. [Google Scholar] [CrossRef]
- Crusz, S.M.; Balkwill, F.R. Inflammation and cancer: Advances and new agents. Nat. Rev. Clin. Oncol. 2015, 12, 584–596. [Google Scholar] [CrossRef]
- Di Pietro, C.; Cicinelli, E.; Guglielmino, M.R.; Ragusa, M.; Farina, M.; Palumbo, M.A.; Cianci, A. Altered transcriptional regulation of cytokines, growth factors, and apoptotic proteins in the endometrium of infertile women with chronic endometritis. Am. J. Reprod. Immunol. 2013, 69, 509–517. [Google Scholar] [CrossRef]
- Cicinelli, E.; Tinelli, R.; Lepera, A.; Pinto, V.; Fucci, M.; Resta, L. Correspondence between hysteroscopic and histologic findings in women with chronic endometritis. Acta Obstet. Gynecol. Scand. 2010, 89, 1061–1065. [Google Scholar] [CrossRef]
- Kitaya, K.; Tada, Y.; Taguchi, S.; Funabiki, M.; Hayashi, T.; Nakamura, Y. Local mononuclear cell infiltrates in infertile patients with endometrial macropolyps versus micropolyps. Hum. Reprod. 2012, 27, 3474–3480. [Google Scholar] [CrossRef]
- Lal, N.; Puri, K.; Rodrigues, B. Vascular Endothelial Growth Factor B and Its Signaling. Front. Cardiovasc. Med. 2018, 5, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibuya, M. Vascular Endothelial Growth Factor (VEGF) and Its Receptor (VEGFR) Signaling in Angiogenesis: A Crucial Target for Anti- and Pro-Angiogenic Therapies. Genes Cancer 2011, 2, 1097–1105. [Google Scholar] [CrossRef]
- Fukumura, D.; Gohongi, T.; Kadambi, A.; Izumi, Y.; Ang, J.; Yun, C.O.; Buerk, D.G.; Huang, P.L.; Jain, R.K. Predominant role of endothelial nitric oxide synthase in vascular endothelial growth factor-induced angiogenesis and vascular permeability. Proc. Natl. Acad. Sci. USA. 2001, 98, 2604–2609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerber, H.P.; McMurtrey, A.; Kowalski, J.; Yan, M.; Keyt, B.A.; Dixit, V.; Ferrara, N. Vascular endothelial growth factor regulates endothelial cell survival through the phosphatidylinositol 3′-kinase/Akt signal transduction pathway. Requirement for Flk-1/KDR activation. J. Biol. Chem. 1998, 273, 30336–30343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arjunan, P.; Lin, X.; Tang, Z.; Du, Y.; Kumar, A.; Liu, L.; Yin, X.; Huang, L.; Chen, W.; Chen, Q.; et al. VEGF-B is a potent antioxidant. Proc. Natl. Acad. Sci. USA 2018, 115, 10351–10356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bausero, P.; Cavaillé, F.; Méduri, G.; Freitas, S.; Perrot-Applanat, M. Paracrine action of vascular endothelial growth factor in the human endometrium: Production and target sites, and hormonal regulation. Angiogenesis 1998, 2, 167–182. [Google Scholar] [CrossRef]
- Sanderson, M.P.; Dempsey, P.J.; Dunbar, A.J. Control of ErbB signaling through metalloprotease mediated ectodomain shedding of EGF-like factors. Growth Factors 2006, 24, 121–136. [Google Scholar] [CrossRef]
- Herbst, R.S. Review of epidermal growth factor receptor biology. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 21–26. [Google Scholar] [CrossRef]
- Möller, B.; Rasmussen, C.; Lindblom, B.; Olovsson, M. Expression of the angiogenic growth factors VEGF, FGF-2, EGF and their receptors in normal human endometrium during the menstrual cycle. Mol. Hum. Reprod. 2001, 7, 65–72. [Google Scholar]
- Islam, M.R.; Yamagami, K.; Yoshii, Y.; Yamauchi, N. Growth factor induced proliferation, migration, and lumen formation of rat endometrial epithelial cells in vitro. J. Reprod. Dev. 2016, 62, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Locksley, R.M.; Killeen, N.; Lenardo, M.J. The TNF and TNF receptor superfamilies: Integrating mammalian biology. Cell 2001, 104, 487–501. [Google Scholar] [CrossRef] [Green Version]
- Tortorella, C.; Piazzolla, G.; Matteo, M.; Pinto, V.; Tinelli, R.; Sabbà, C.; Fanelli, M.; Cicinelli, E. Interleukin-6, interleukin-1β, and tumor necrosis factor α in menstrual effluents as biomarkers of chronic endometritis. Fertil. Steril. 2014, 101, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Nichols, J.E.; Valdez, R.; Mendelson, C.R.; Simpson, E.R. Tumor necrosis factor-alpha stimulates aromatase gene expression in human adipose stromal cells through use of an activating protein-1 binding site upstream of promoter 1.4. Mol. Endocrinol. 1996, 10, 1350–1357. [Google Scholar] [CrossRef] [Green Version]
- Chen, W. Tregs in immunotherapy: Opportunities and challenges. Immunotherapy 2011, 3, 911–914. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, A.S.; Schumacher, A. The T helper type 17/regulatory T cell paradigm in pregnancy. Immunology 2016, 148, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzaki, E.; Kouimtzoglou, E.; Margioris, A.N.; Gravanis, A. Transforming growth factor beta1 exerts an autocrine regulatory effect on human endometrial stromal cell apoptosis, involving the FasL and Bcl-2 apoptotic pathways. Mol. Hum. Reprod. 2003, 9, 91–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.J.; Zhang, H.; Chen, Z.Q.; Zhang, W.; Liu, X.M.; Fang, J.Y.; Liu, F.J.; Kwak-Kim, J. Endometrial TGF-β, IL-10, IL-17 and autophagy are dysregulated in women with recurrent implantation failure with chronic endometritis. Reprod. Biol. Endocrinol. 2019, 17, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroder, K.; Hertzog, P.J.; Ravasi, T.; Hume, D.A. Interferon-gamma: An overview of signals, mechanisms and functions. J. Leukoc. Biol. 2004, 75, 163–189. [Google Scholar] [CrossRef]
- Rodríguez, N.; Peláez, A.; Barderas, R.; Domínguez, G. Clinical implications of the deregulated TP73 isoforms expression in cancer. Clin. Transl. Oncol. 2018, 20, 827–836. [Google Scholar] [CrossRef]
- Costanzo, A.; Pediconi, N.; Narcisi, A.; Guerrieri, F.; Belloni, L.; Fausti, F.; Botti, E.; Levrero, M. TP63 and TP73 in cancer, an unresolved “family” puzzle of complexity, redundancy and hierarchy. FEBS Lett. 2014, 588, 2590–2599. [Google Scholar] [CrossRef] [Green Version]
- Giannone, G.; Tuninetti, V.; Ghisoni, E.; Genta, S.; Scotto, G.; Mittica, G.; Valabrega, G. Role of Cyclin-Dependent Kinase Inhibitors in Endometrial Cancer. Int. J. Mol. Sci. 2019, 20, 2353. [Google Scholar] [CrossRef] [Green Version]
- Horrée, N.; van Diest, P.J.; van der Groep, P.; Sie-Go, D.M.; Heintz, A.P. Progressive derailment of cell cycle regulators in endometrial carcinogenesis. J. Clin. Pathol. 2008, 61, 36–42. [Google Scholar] [CrossRef]
- Crosby, M.E. Cell Cycle: Principles of Control. Yale J. Biol. Med. 2007, 80, 141–142. [Google Scholar]
- Enserink, J.M.; Kolodner, R.D. An overview of Cdk1-controlled targets and processes. Cell Divis. 2010, 13, 1–41. [Google Scholar] [CrossRef] [Green Version]
- Shiozawa, T.; Li, S.F.; Nakayama, K.; Nikaido, T.; Fujii, S. Relationship between the expression of cyclins/cyclin-dependent kinases and sex-steroid receptors/Ki67 in normal human endometrial glands and stroma during the menstrual cycle. Mol. Hum. Reprod. 1996, 2, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Zhang, Y.; Pan, H.; Luo, Q.; Zhu, X.M.; Dong, M.Y.; Leung, P.C.; Sheng, J.Z.; Huang, H.F. Involvement of cyclin B1 in progesterone-mediated cell growth inhibition, G2/M cell cycle arrest, and apoptosis in human endometrial cell. Reprod. Biol. Endocrinol. 2009, 7, 144. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | CE Group (n = 7) | Control Group (n = 6) | p Value |
|---|---|---|---|
| Age (years) | 24–39, 30.5 | 27–35, 30 | NS |
| BMI (kg/cm2) | 24–35, 29.5 | 23–33, 29.5 | NS |
| Parity (n) | 1–2, 1 | 1–2, 1 | NS |
| AUB (n) | 3 | 1 | NS |
| Smoking (n) | 0 | 1 | NS |
| Previous intrauterine instrumentation | 0 | 0 | NS |
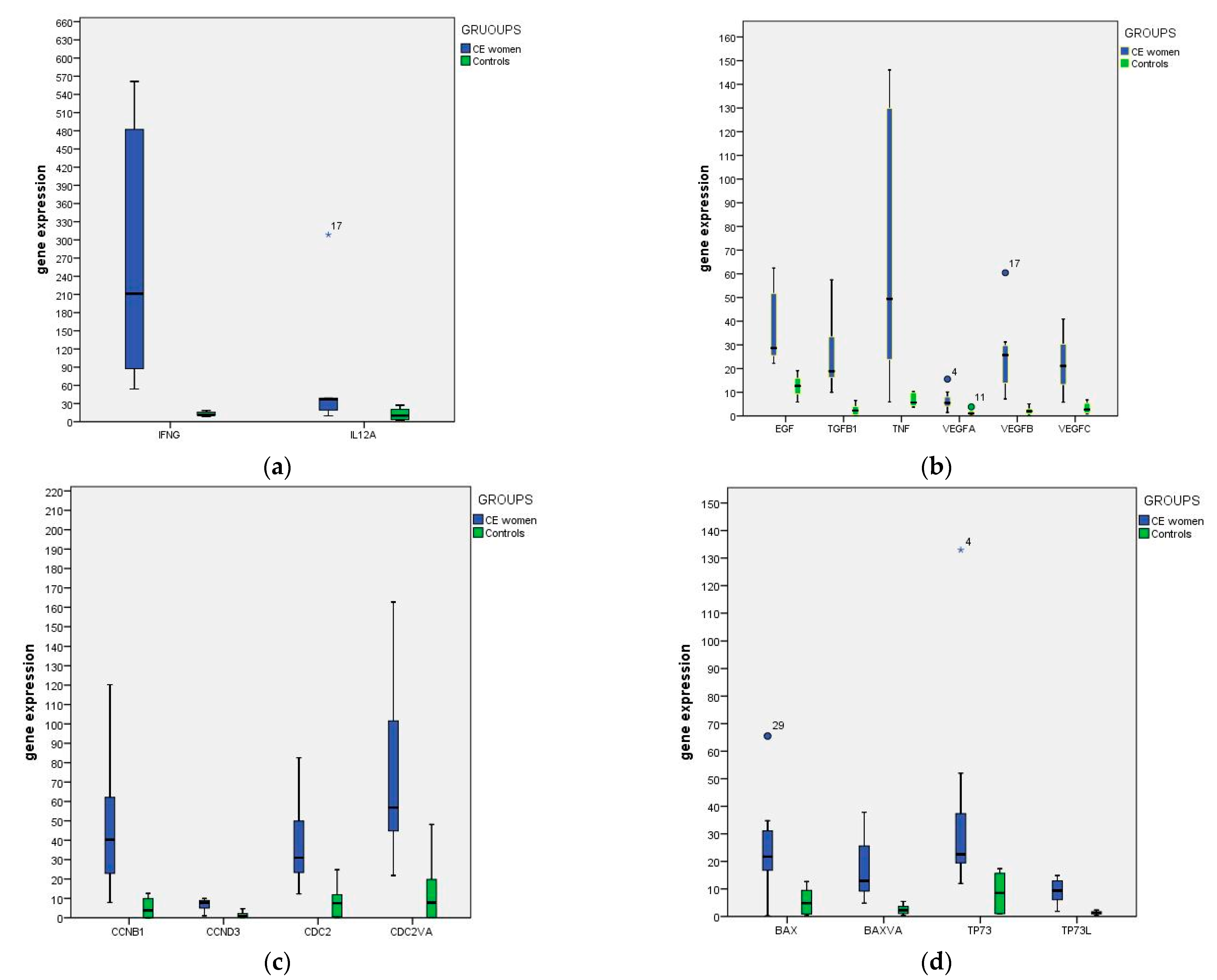
| Endometrial Expression | |||||||||
|---|---|---|---|---|---|---|---|---|---|
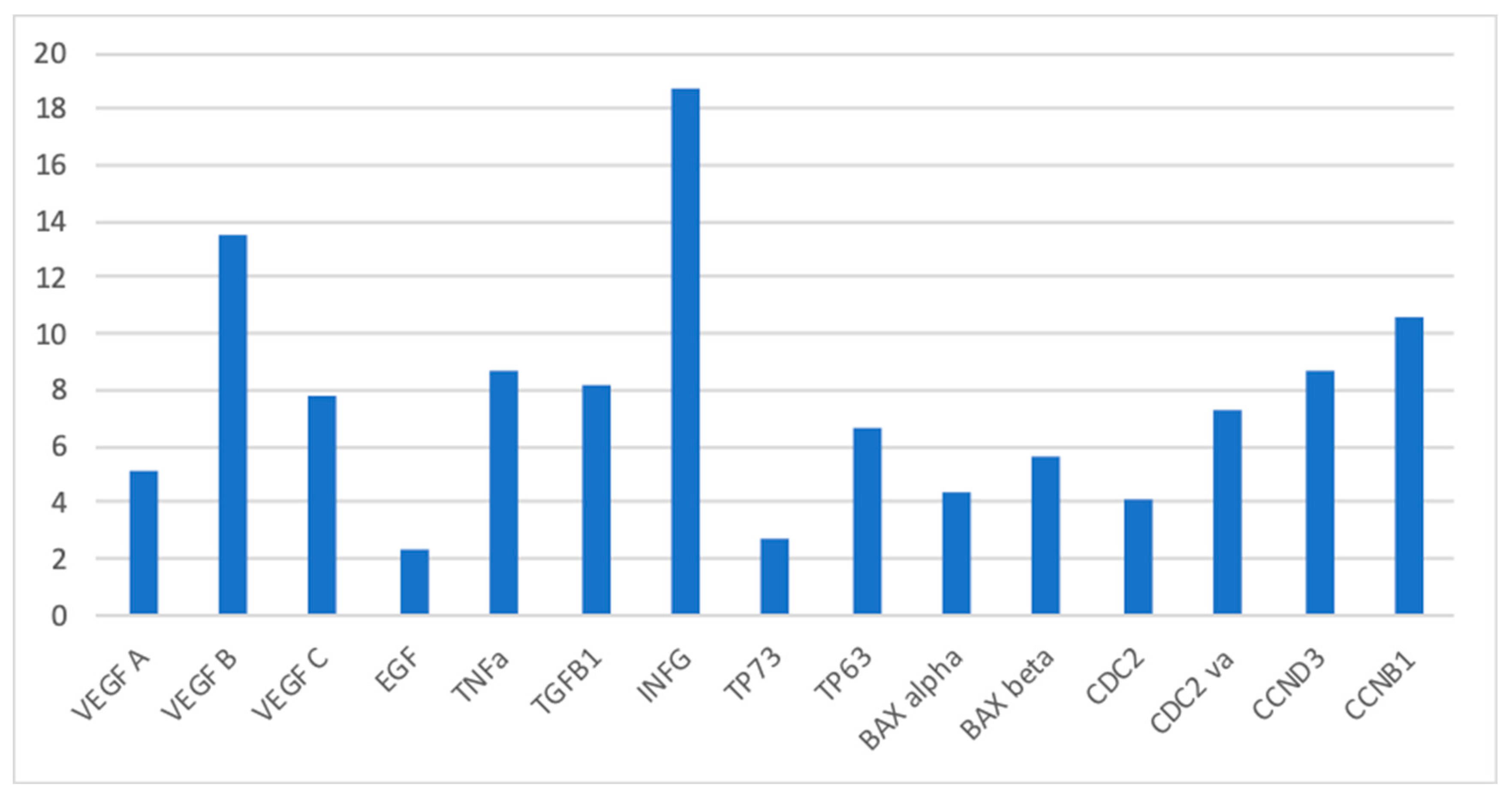
| Full Name | CE Women | Controls | Median Ratio (CE Women/Controls) | p Value | |||||
| Median | Min | Max | Median | Min | Max | ||||
| IL12A | INTERLEUKIN 12A | 36.45 | 9.79 | 308.44 | 10.17 | 2.53 | 27.24 | 3.6 | 0.151 |
| IFNG | INTERFERON GAMMA | 211.32 | 53,91 | 561,42 | 11,27 | 8.56 | 18.52 | 18.75 | 0.001 * |
| TGFB1 | TRANSFORMING GROWTH FATOR B | 18.89 | 9.97 | 57.48 | 2.27 | 0.16 | 6.55 | 8.2 | 0.001 * |
| TNF | TUMOR NECROSIS FACTOR (TNF SUPERFAMILY, MEMBER 2) | 49.4 | 5.9 | 146.05 | 5.67 | 3.76 | 10.27 | 8.7 | 0.015 * |
| VEGFA | VASCULAR ENDOTHELIAL GROWTH FACTOR A | 5.53 | 1.46 | 15.54 | 1.05 | 0.72 | 3.83 | 5.2 | 0.008 * |
| VEGF B | VASCULAR ENDOTHELIAL GROWTH FACTOR B | 25.71 | 7.14 | 60.44 | 1.98 | 0.2 | 5.1 | 13.5 | 0.001 * |
| VEGF C | VASCULAR ENDOTHELIAL GROWTH FACTOR C | 21.13 | 5.8 | 40.92 | 2.71 | 0.85 | 6.79 | 7.8 | 0.005 * |
| EGF | EPIDERMAL GROWTH FACTOR | 28.65 | 22.2 | 62.43 | 12.67 | 5.84 | 19.14 | 2.4 | 0.017 * |
| CDC2 | CELL DIVISION CONTROL 2 | 30.94 | 12.32 | 82.55 | 7.49 | 0.09 | 24.77 | 4.1 | 0.005 * |
| CDC2 va | CELL DIVISION CONTROL 2 VARIANT | 56.86 | 21.82 | 162.69 | 7.79 | 0.18 | 48.12 | 7.3 | 0.008 * |
| CCND3 | CYCLIN D3 | 7.77 | 1.01 | 10 | 0.88 | 0.15 | 4.65 | 8.7 | 0.014 * |
| CCNB1 | CYCLIN B1 | 40.24 | 7.91 | 120.24 | 3.78 | 0.06 | 12.6 | 10.6 | 0.005 * |
| TP73 | TUMOR PROTEIN P73 | 22.55 | 11.96 | 132.95 | 8.53 | 0.94 | 17.35 | 2.64 | 0.005 * |
| TP73L | TUMOR PROTEIN P73 | 9.39 | 1.87 | 14.88 | 1.4 | 0.29 | 2.34 | 6.71 | 0.004 * |
| BAX | BCL2-ASSOCIATED X PROTEIN | 21.73 | 0.22 | 65.51 | 4.87 | 0.28 | 12.69 | 4.46 | 0.051 |
| BAX va | BCL2-ASSOCIATED X PROTEIN VARIANT | 12.91 | 4.83 | 37.83 | 2.26 | 0.32 | 5.46 | 5.71 | 0.002 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicinelli, E.; Vitagliano, A.; Loizzi, V.; De Ziegler, D.; Fanelli, M.; Bettocchi, S.; Nardelli, C.; Trojano, G.; Cicinelli, R.; Minervini, C.F.; et al. Altered Gene Expression Encoding Cytochines, Grow Factors and Cell Cycle Regulators in the Endometrium of Women with Chronic Endometritis. Diagnostics 2021, 11, 471. https://doi.org/10.3390/diagnostics11030471
Cicinelli E, Vitagliano A, Loizzi V, De Ziegler D, Fanelli M, Bettocchi S, Nardelli C, Trojano G, Cicinelli R, Minervini CF, et al. Altered Gene Expression Encoding Cytochines, Grow Factors and Cell Cycle Regulators in the Endometrium of Women with Chronic Endometritis. Diagnostics. 2021; 11(3):471. https://doi.org/10.3390/diagnostics11030471
Chicago/Turabian StyleCicinelli, Ettore, Amerigo Vitagliano, Vera Loizzi, Dominique De Ziegler, Margherita Fanelli, Stefano Bettocchi, Claudia Nardelli, Giuseppe Trojano, Rossana Cicinelli, Crescenzio Francesco Minervini, and et al. 2021. "Altered Gene Expression Encoding Cytochines, Grow Factors and Cell Cycle Regulators in the Endometrium of Women with Chronic Endometritis" Diagnostics 11, no. 3: 471. https://doi.org/10.3390/diagnostics11030471