
Anterior Chamber Angle in Adults Born Extremely, Very, and Moderately Preterm with and without Retinopathy of Prematurity—Results of the Gutenberg Prematurity Eye Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Assessment of Pre-, Peri- and Postnatal Medical History
2.3. Categorization
2.4. Ophthalmologic Examination
2.5. Scheimpflug Imaging
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Descriptive Ocular Geometric Parameters
3.3. Association Analysis
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Financial Disclosure
References
- Wu, W.C.; Lin, R.I.; Shih, C.P.; Wang, N.K.; Chen, Y.P.; Chao, A.N.; Chen, K.J.; Chen, T.L.; Hwang, Y.S.; Lai, C.C.; et al. Visual acuity, optical components, and macular abnormalities in patients with a history of retinopathy of prematurity. Ophthalmology 2012, 119, 1907–1916. [Google Scholar] [CrossRef]
- Fieß, A.; Kolb-Keerl, R.; Knuf, M.; Kirchhof, B.; Blecha, C.; Oberacher-Velten, I.; Muether, P.S.; Bauer, J. Axial Length and Anterior Segment Alterations in Former Preterm Infants and Full-Term Neonates Analyzed With Scheimpflug Imaging. Cornea 2017, 36, 821–827. [Google Scholar] [CrossRef]
- Cook, A.; White, S.; Batterbury, M.; Clark, D. Ocular growth and refractive error development in premature infants with or without retinopathy of prematurity. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5199–5207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fieß, A.; Schuster, A.K.; Pfeiffer, N.; Nickels, S. Association of birth weight with corneal power in early adolescence: Results from the National Health and Nutrition Examination Survey (NHANES) 1999–2008. PLoS ONE 2017, 12, e0186723. [Google Scholar] [CrossRef] [PubMed]
- Fieß, A.; Schuster, A.K.; Nickels, S.; Urschitz, M.S.; Elflein, H.M.; Schulz, A.; Münzel, T.; Wild, P.S.; Beutel, M.E.; Schmidtmann, I.; et al. Association of Low Birth Weight with Altered Corneal Geometry and Axial Length in Adulthood in the German Gutenberg Health Study. JAMA Ophthalmol. 2019, 137, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.K.; Pfeiffer, N.; Nickels, S.; Schulz, A.; Hohn, R.; Wild, P.S.; Binder, H.; Munzel, T.; Beutel, M.E.; Vossmerbaeumer, U. Distribution of Anterior Chamber Angle Width and Correlation With Age, Refraction, and Anterior Chamber Depth-The Gutenberg Health Study. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3740–3746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartnett, M.E.; Gilbert, M.M.; Richardson, T.M.; Krug, J.H., Jr.; Hirose, T. Anterior segment evaluation of infants with retinopathy of prematurity. Ophthalmology 1990, 97, 122–130. [Google Scholar] [CrossRef]
- Chang, S.H.L.; Lee, Y.S.; Wu, S.C.; See, L.C.; Chung, C.C.; Yang, M.L.; Lai, C.C.; Wu, W.C. Anterior Chamber Angle and Anterior Segment Structure of Eyes in Children With Early Stages of Retinopathy of Prematurity. Am. J. Ophthalmol. 2017, 179, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Cernichiaro-Espinosa, L.A.; Garcia-Huerta, M.M.; Giordano, V.E.; Salinas-Longoria, S.M.; Romero-Vera, R.; Garcia-Aguirre, G.; Salcedo-Villanueva, G.; Quiroz-Mercado, H.; Martinez-Castellanos, M.A. Comparison of iridocorneal angle in infants with retinopathy of prematurity and healthy infants using spectral domain optical coherence tomography. J. AAPOS Off. Publ. Am. Assoc. Pediatric Ophthalmol. Strabismus/Am. Assoc. Pediatric Ophthalmol. Strabismus 2014, 18, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Ecsedy, M.; Kovacs, I.; Mihaltz, K.; Recsan, Z.; Szigeti, A.; Juhasz, E.; Nemeth, J.; Nagy, Z.Z. Scheimpflug imaging for long-term evaluation of optical components in Hungarian children with a history of preterm birth. J. Pediatric Ophthalmol. Strabismus 2014, 51, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Lenis, T.L.; Gunzenhauser, R.C.; Fung, S.S.M.; Dhindsa, Y.K.; Sarraf, D.; Pineles, S.L.; Tsui, I. Myopia and anterior segment optical coherence tomography findings in laser-treated retinopathy of prematurity eyes. J. AAPOS Off. Publ. Am. Assoc. Pediatric Ophthalmol. Strabismus/Am. Assoc. Pediatric Ophthalmol. Strabismus 2020, 24, 86.e81–86.e87. [Google Scholar] [CrossRef] [PubMed]
- Voigt, M.; Fusch, C.; Olbertz, D. Analyse des Neugeborenenkollektivs der Bundesrepublik Deutschland 12. Mitteilung: Vorstellung engmaschiger Perzentilwerte (-kurven) für die Körpermaße Neugeborener. Geburtsh Frauenheilk 2006, 66, 956–970. [Google Scholar] [CrossRef]
- Scheie, H.G. Width and pigmentation of the angle of the anterior chamber; a system of grading by gonioscopy. AMA Arch. Ophthalmol. 1957, 58, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, G.L. The normal development of the human anterior chamber angle: A new system of descriptive grading. Trans. Ophthalmol. Soc. U. K. 1971, 91, 709–739. [Google Scholar] [PubMed]
- Smith, S.D.; Singh, K.; Lin, S.C.; Chen, P.P.; Chen, T.C.; Francis, B.A.; Jampel, H.D. Evaluation of the anterior chamber angle in glaucoma: A report by the american academy of ophthalmology. Ophthalmology 2013, 120, 1985–1997. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.E.; Dobson, V.; Siatkowski, R.M.; Hardy, R.J.; Kivlin, J.; Palmer, E.A.; Phelps, D.L.; Repka, M.X.; Summers, C.G.; Tung, B.; et al. Does cryotherapy affect refractive error? Results from treated versus control eyes in the cryotherapy for retinopathy of prematurity trial. Ophthalmology 2001, 108, 343–347. [Google Scholar] [CrossRef]
- Fielder, A.R.; Levene, M.I.; Russell-Eggitt, I.M.; Weale, R.A. Temperature—A factor in ocular development? Dev. Med. Child Neurol. 1986, 28, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Senthil, S.; Balijepalli, P.; Mohamed, A.; Rani, P.K.; Nayak, S.; Garudadri, C.; Mandal, A.K.; Jalali, S. Management outcomes of secondary glaucoma due to retinopathy of prematurity: A 19-year prospective study at a tertiary eye care Institute. The Indian Twin cities ROP Screening (ITCROPS) database report number 8. PLoS ONE 2020, 15, e0238633. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.S.; He, M. Anterior chamber angle assessment techniques. Surv. Ophthalmol. 2008, 53, 250–273. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | |
|---|---|---|---|---|---|---|
| Gestational Age | GA ≥ 37 | GA 33–36 | GA 29–32 | GA ≤ 28 | GA ≤ 32 | GA ≤ 32 |
| no ROP | no ROP | no ROP | ROP without Treatment |
ROP
with Treatment | ||
| Participants/eyes (n) | 113/182 | 100/160 | 61/101 | 11/18 | 28/45 | 6/10 |
| Sex (women) (%) | 68 (60.2) | 61 (61.0) | 34 (55.7) | 7 (63.6) | 15 (53.6) | 3 (50.0) |
| Age (y) | 30.0 ± 9.2 | 30.2 ± 9.3 | 27.5 ± 7.7 | 23.5 ± 7.5 | 25.1 ± 6.1 | 25.2 ± 4.6 |
| Birth weight (g) | 3421 ± 389 | 2112 ± 479 | 1563 ± 337 | 931 ± 215 | 1068 ± 380 | 708 ± 143 |
| Birth weight < 1500 g (yes) | 0 (0%) | 9 (9.0%) | 25 (41.0%) | 11 (100%) | 24 (85.7%) | 6 (100%) |
| Birth weight < 1000 g (yes) | 0 (0%) | 0 (0%) | 4 (6.6%) | 7 (63.6%) | 14 (50.0%) | 6 (100%) |
| Birth weight percentile | 49.2 ± 20.8 | 27.1 ± 24.4 | 42.9 ± 25.3 | 51.1 ± 25.8 | 35.0 ± 25.1 | 26.2 ± 30.5 |
| Gestational age (wks) | 39.3 ± 1.3 | 34.3 ± 0.9 | 30.8 ± 1.1 | 26.3 ± 1.7 | 28.1 ± 2.0 | 26.0 ± 1.9 |
| (min–max) | (37–43) | (33–36) | (29–32) | (23–28) | (24–32) | (24–32) |
| ROP stage (1/2/3) | 0/0/0 | 0/0/0 | 0/0/0 | 0/0/0 | 16/25/4 | 0/3/7 |
| Preeclampsia (yes) | 8 (7.1%) | 18 (18.0%) | 8 (13.1%) | 1 (9.1%) | 6 (21.4%) | 1 (16.7%) |
| Placental insufficiency (yes) | 2 (1.8%) | 10 (10.0%) | 2 (3.3%) | 0 (0%) | 0 (0%) | 0 (0%) |
| HELLP syndrome (yes) | 0 (0%) | 5 (5.0%) | 0 (0%) | 0 (0%) | 3 (10.7%) | 0 (0%) |
| Maternal smoking (eys) | 5 (4.4%) | 6 (6.0%) | 6 (9.8%) | 1 (9.1%) | 2 (7.1%) | 1 (16.7%) |
| Gestational diabetes (yes) | 1 (0.9%) | 5 (5.0%) | 1 (1.6%) | 0 (0.0%) | 1 (3.6%) | 0 (0%) |
| Breastfeeding (yes) | 59 (52.2%) | 55 (55.0%) | 33 (54.1%) | 4 (36.4%) | 13 (46.4%) | 2 (33.3%) |
| Ocular parameters | ||||||
| Spherical equivalent (diopter) OD | −0.24 ± 2.58 | −0.02 ± 3.15 | 0.16 ± 1.80 | 0.40 ± 1.26 | 0.50 ± 4.30 | 0.90 ± 2.40 |
| Spherical equivalent (diopter) OS | −0.23 ± 2.60 | −0.01 ± 3.10 | 0.17 ± 1.79 | 0.39 ± 1.24 | 0.49 ± 4.28 | 0.89 ± 4.38 |
| Intraocular pressure (mmHg) OD | 15.2 ± 2.8 | 14.7 ± 2.9 | 15.3 ± 3.3 | 16.6 ± 3.4 | 15.3 ± 4.3 | 16.8 ± 4.5 |
| Intraocular pressure (mmHg) OS | 15.1 ± 2.8 | 14.6 ± 2.8 | 15.2 ± 3.2 | 15.1 ±3.0 | 15.2 ± 4.2 | 16.7 ± 4.3 |
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | |
|---|---|---|---|---|---|---|
| Gestational Age | GA ≥ 37 | GA 33–36 | GA 29–32 | GA ≤ 28 | GA ≤ 32 | GA ≤ 32 |
| no ROP | no ROP | no ROP | ROP without Treatment |
ROP
with Treatment | ||
| § Participants/§eyes (n) OD + OS | 113/182 | 100/160 | 61/101 | 11/18 | 28/45 | 6/10 |
| Anterior chamber angle | ||||||
| Right eye | ||||||
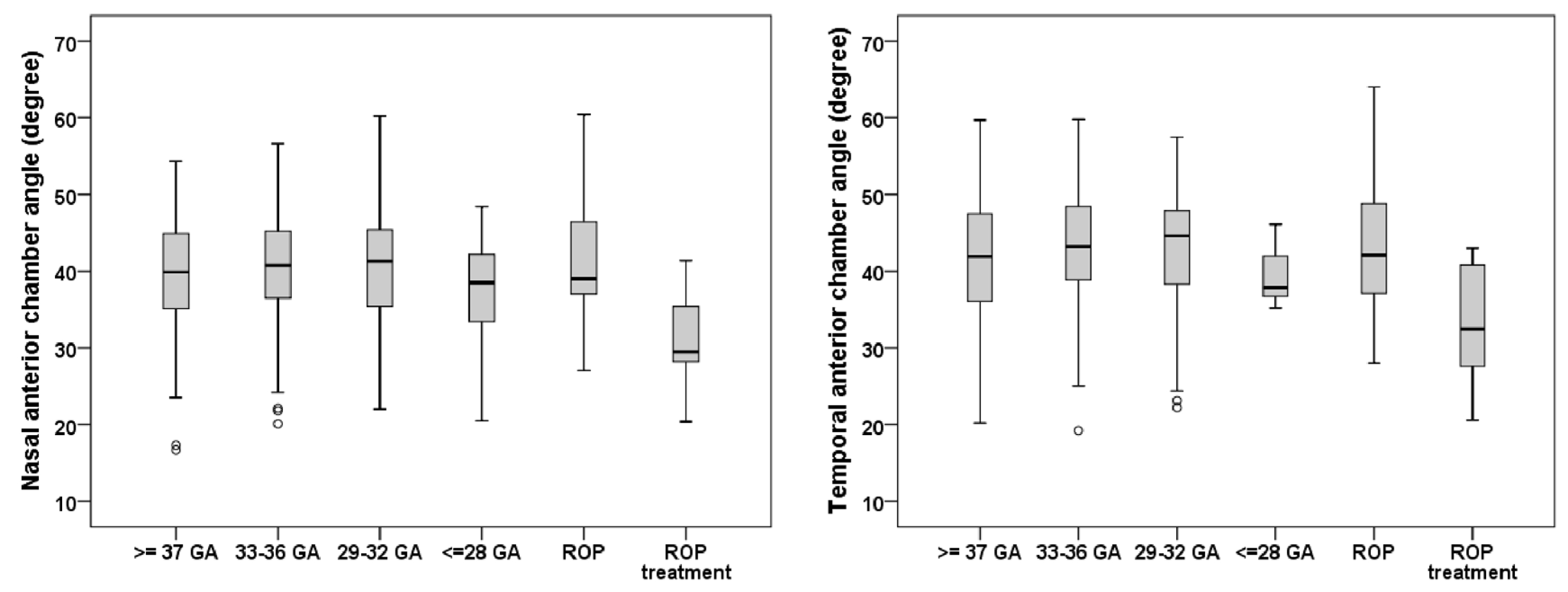
| Nasal (µm) OD | 40.1 ± 7.0 | 40.9 ± 7.0 | 40.7 ± 7.6 | 36.9 ± 4.7 | 42.5 ± 6.5 | 32.1 ± 6.3 ** |
| Valid measurements OD (participants/eyes) | 79/81 | 76/77 | 47/48 | 7/8 | 22/23 | 4/4 |
| Temporal (µm) OD | 41.8 ± 6.8 | 43.3 ± 6.8 | 43.0 ± 7.7 | 39.7 ± 3.0 | 42.5 ± 7.3 | 27.9 ± 0.4 ** |
| Valid measurements OD (participants/eyes) | 50/81 | 48/77 | 32/48 | 4/8 | 14/23 | 2/4 |
| Left eye | ||||||
| Nasal (µm) OS | 39.0 ± 6.7 | 40.7 ± 6.5 | 40.1 ± 7.2 | 37.0 ± 8.6 | 40.0 ± 6.9 | 30.2 ± 6.9 ** |
| Valid measurements OD (participants/eyes) | 99/101 | 82/83 | 53/53 | 10/10 | 22/22 | 6/6 |
| Temporal (µm) OS | 40.4 ± 7.7 | 44.8 ± 7.3 # | 42.1 ± 6.7 | 40.0 ± 3.7 | 44.4 ± 9.0 | 31.9 ± 9.0 # |
| Valid measurements OD (participants/eyes) | 58/101 | 46/83 | 34/53 | 7/10 | 15/22 | 4/6 |
| Univariate Analysis | ||
|---|---|---|
| B (95% CI) | p | |
| Nasal anterior chamber angle (in degrees) | ||
| Breastfeeding | 1.269 (−0.809; 3.348) | 0.23 |
| Placental insufficiency | −0.735 (−6.098; 4.629) | 0.79 |
| Preeclampsia | −1.098 (−3.175; 0.978) | 0.30 |
| Gestational age (weeks) | 0.038 (−0.139; 0.214) | 0.68 |
| Birth weight (gram) | 0.047 (−0.691; 0.784) | 0.90 |
| Birth weight percentile | 0.000 (−0.030; 0.029) | 0.97 |
| ROP (yes) | −0.351 (−3.059; 2.357) | 0.80 |
| ROP treatment (yes) | −9.6 (−14.7; −4.5) | <0.001 |
| Temporal anterior chamber angle (in degrees) | ||
| Placental insufficiency (yes) | 2.720 (−0.718; 6.158) | 0.021 |
| Preeclampsia (yes) | −1.211 (−4.320; 1.808) | 0.43 |
| Breastfeeding (yes) | 1.039 (−0.941; 3.018) | 0.30 |
| Gestational age (weeks) | 0.018 (−0.210; 0.247) | 0.87 |
| Birth weight (gram) | −0.249 (−1.242; 0.743) | 0.62 |
| Birth weight percentile | −0.015 (−0.056; 0.026) | 0.47 |
| ROP (yes) | −0.879 (−4.623; 2.864) | 0.65 |
| ROP treatment (yes) | −11.5 (−17.7; −5.3) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fieß, A.; Gißler, S.; Mildenberger, E.; Urschitz, M.S.; Fauer, A.; Elflein, H.M.; Zepp, F.; Stoffelns, B.; Pfeiffer, N.; Schuster, A.K. Anterior Chamber Angle in Adults Born Extremely, Very, and Moderately Preterm with and without Retinopathy of Prematurity—Results of the Gutenberg Prematurity Eye Study. Children 2022, 9, 281. https://doi.org/10.3390/children9020281
Fieß A, Gißler S, Mildenberger E, Urschitz MS, Fauer A, Elflein HM, Zepp F, Stoffelns B, Pfeiffer N, Schuster AK. Anterior Chamber Angle in Adults Born Extremely, Very, and Moderately Preterm with and without Retinopathy of Prematurity—Results of the Gutenberg Prematurity Eye Study. Children. 2022; 9(2):281. https://doi.org/10.3390/children9020281
Chicago/Turabian StyleFieß, Achim, Sandra Gißler, Eva Mildenberger, Michael S. Urschitz, Agnes Fauer, Heike M. Elflein, Fred Zepp, Bernhard Stoffelns, Norbert Pfeiffer, and Alexander K. Schuster. 2022. "Anterior Chamber Angle in Adults Born Extremely, Very, and Moderately Preterm with and without Retinopathy of Prematurity—Results of the Gutenberg Prematurity Eye Study" Children 9, no. 2: 281. https://doi.org/10.3390/children9020281