
Normo- or Hypo-Fractionated Photon or Proton Radiotherapy in the Management of Locally Advanced Unresectable Pancreatic Cancer: A Systematic Review
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Statistical Analysis
2.4. Bias Assessment
3. Results
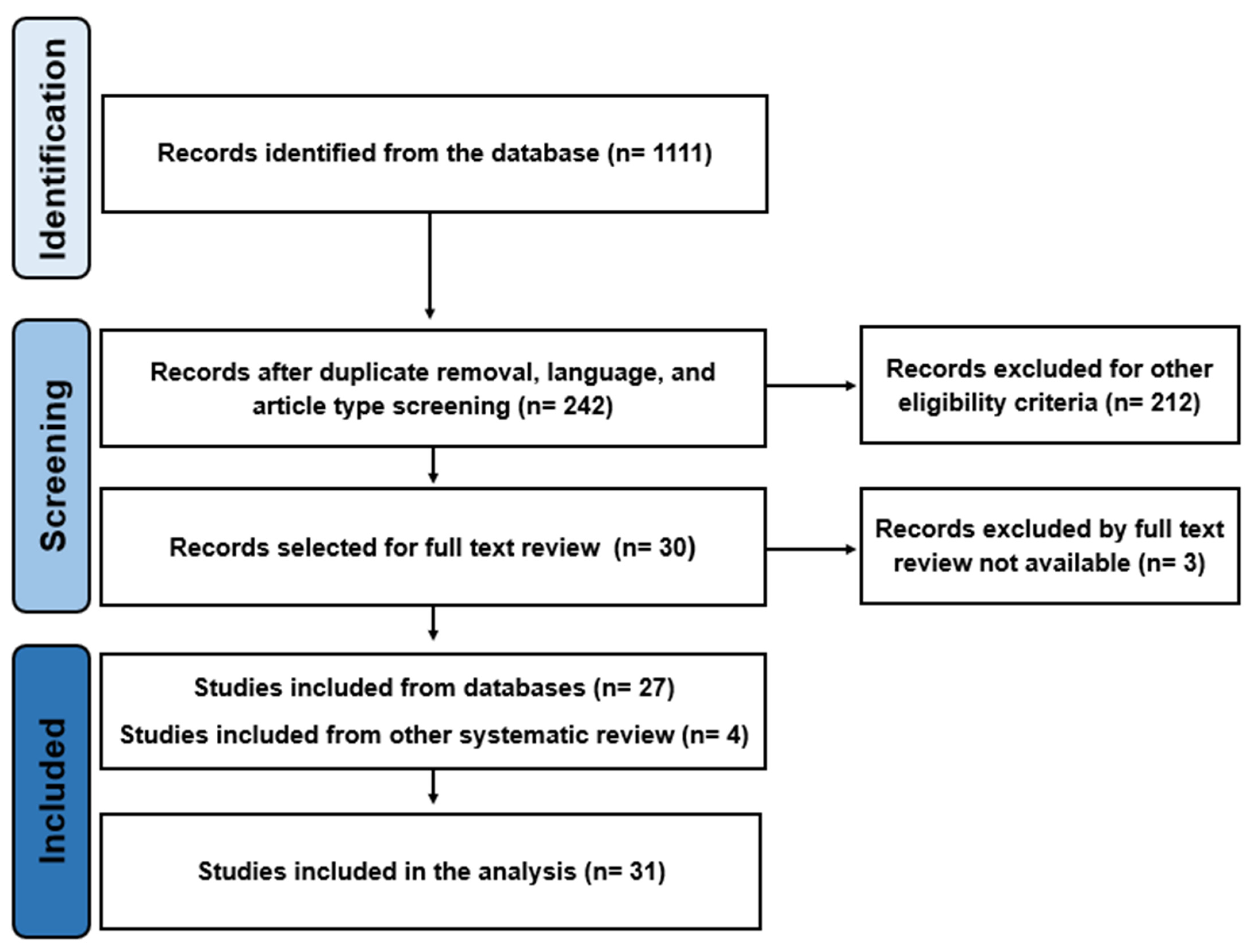
3.1. Search Results
3.2. Studies and Patient Characteristics
3.3. Radiation Therapy
3.4. Chemotherapy Regimens
3.5. Acute G3/G4 or Higher Toxicity
3.6. Late G3/4 or Higher Toxicity
3.7. Survival Outcomes
3.8. Overall Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Huguet, F.; Mukherjee, S.; Javle, M. Locally Advanced Pancreatic Cancer: The Role of Definitive Chemoradiotherapy. Clin. Oncol. 2014, 26, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Hansen, M.; Berendse, S.; Hamilton, W. Symptoms of Pancreatic Cancer in Primary Care: A Systematic Review. Pancreas 2016, 45, 814–818. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Chiaro, D.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef]
- Ng, I.W.; Soon, Y.Y.; Chen, D.; Tey, J.C.S. Chemoradiotherapy versus Chemotherapy for Locally Advanced Unresectable Pancreatic Cancer: A Systematic Review and Meta-Analysis. Asia-Pac. J. Clin. Oncol. 2018, 14, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Simoni, N.; Rossi, G.; Cellini, F.; Vitolo, V.; Orlandi, E.; Valentini, V.; Mazzarotto, R.; Sverzellati, N.; D’Abbiero, N. Ablative Radiotherapy (ART) for Locally Advanced Pancreatic Cancer (LAPC): Toward a New Paradigm? Life 2022, 12, 456. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.P.; Herman, J.M. Stereotactic Radiotherapy and Particle Therapy for Pancreatic Cancer. Cancers 2018, 10, 75. [Google Scholar] [CrossRef] [Green Version]
- Schneider, S.; Stefanowicz, S.; Jentsch, C.; Lohaus, F.; Thiele, J.; Haak, D.; Valentini, C.; Platzek, I.G.C.; Troost, E.; Hoffmann, A.L. Reduction of Intrafraction Pancreas Motion Using an Abdominal Corset Compatible with Proton Therapy and MRI. Clin. Transl. Radiat. Oncol. 2023, 38, 111–116. [Google Scholar] [CrossRef]
- Taniguchi, C.M.; Murphy, J.D.; Eclov, N.; Atwood, T.F.; Kielar, K.N.; Christman-Skieller, C.; Mok, E.; Xing, L.; Koong, A.C.; Chang, D.T. Dosimetric Analysis of Organs at Risk during Expiratory Gating in Stereotactic Body Radiation Therapy for Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1090–1095. [Google Scholar] [CrossRef]
- Rutenberg, M.S.; Nichols, R.C. Proton Beam Radiotherapy for Pancreas Cancer. J. Gastrointest. Oncol. 2020, 11, 166–175. [Google Scholar] [CrossRef]
- Tchelebi, L.T.; Lehrer, E.J.; Trifiletti, D.M.; Do, N.K.S.; Gusani, N.J.; Crane, C.H.; Zaorsky, N.G. Conventionally Fractionated Radiation Therapy versus Stereotactic Body Radiation Therapy for Locally Advanced Pancreatic Cancer (CRiSP): An International Systematic Review and Meta-Analysis. Cancer 2020, 126, 2120–2131. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kang, J.O. Basics of Particle Therapy II: Relative Biological Effectiveness. Radiat. Oncol. J. 2012, 30, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer: A Review. JAMA 2021, 326, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Starke, K.R.; Mauer, R.; Karskens, E.; Pretzsch, A.; Reissig, D.; Nienhaus, A.; Seidler, A.L.; Seidler, A. The Effect of Ambient Environmental Conditions on COVID-19 Mortality: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6665. [Google Scholar] [CrossRef]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.-L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Night-Shift Work and Breast Cancer—A Systematic Review and Meta-Analysis. Scand. J. Work. Environ. Health 2013, 39, 431–447. [Google Scholar] [CrossRef]
- Flemyng, E.; Dwan, K.; Moore, T.H.; Page, M.J.; Higgins, J.P. Risk of Bias 2 in Cochrane Reviews: A Phased Approach for the Introduction of New Methodology. Cochrane Database Syst. Rev. 2020, 2020, ED000148. [Google Scholar] [CrossRef]
- Liermann, J.; Munter, M.; Naumann, P.; Abdollahi, A.; Krempien, R.; Debus, J. Cetuximab, Gemcitabine and Radiotherapy in Locally Advanced Pancreatic Cancer: Long-Term Results of the Randomized Controlled Phase II PARC Trial. Clin. Transl. Radiat. Oncol. 2022, 34, 15–22. [Google Scholar] [CrossRef]
- Esnaola, N.F.; Chaudhary, U.B.; O’Brien, P.; Garrett-Mayer, E.; Camp, E.R.; Thomas, M.B.; Cole, D.J.; Montero, A.J.; Hoffman, B.J.; Romagnuolo, J.; et al. Phase 2 Trial of Induction Gemcitabine, Oxaliplatin, and Cetuximab Followed by Selective Capecitabine-Based Chemoradiation in Patients with Borderline Resectable or Unresectable Locally Advanced Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 837–844. [Google Scholar] [CrossRef] [Green Version]
- Hammel, P.; Huguet, F.; van Laethem, J.-L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouché, O.; Shannon, J.; André, T.; et al. Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients with Locally Advanced Pancreatic Cancer Controlled after 4 Months of Gemcitabine with or without Erlotinib. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef]
- Ducreux, M.; Giovannini, M.; Baey, C.; Llacer, C.; Bennouna, J.; Adenis, A.; Peiffert, D.; Mornex, F.; Abbas, M.; Boige, V.; et al. Radiation plus Docetaxel and Cisplatin in Locally Advanced Pancreatic Carcinoma: A Non-Comparative Randomized Phase II Trial. Dig. Liver Dis. 2014, 46, 950–955. [Google Scholar] [CrossRef]
- Combs, S.E.; Habermehl, D.; Kessel, K.; Bergmann, F.; Werner, J.; Brecht, I.; Schirmacher, P.; Jäger, D.; Büchler, M.W.; Debus, J. Intensity Modulated Radiotherapy as Neoadjuvant Chemoradiation for the Treatment of Patients with Locally Advanced Pancreatic Cancer: Outcome Analysis and Comparison with a 3D-Treated Patient Cohort. Strahlenther. Onkol. 2013, 198, 738–744. [Google Scholar] [CrossRef]
- Youl, M.; Hashem, S.; Brade, A.; Cummings, B.; Dawson, L.A.; Gallinger, S.; Hedley, D.; Jiang, H.; Kim, J.; Krzyzanowska, M.K.; et al. Induction Gemcitabine Plus Concurrent Gemcitabine and Radiotherapy for Locally Advanced Unresectable or Resected Pancreatic Cancer. Clin. Oncol. 2014, 26, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Hurt, C.N.; Bridgewater, J.; Falk, S.; Cummins, S.; Wasan, H.; Crosby, T.; Jephcott, C.; Roy, R.; Radhakrishna, G.; et al. Gemcitabine-Based or Capecitabine-Based Chemoradiotherapy for Locally Advanced Pancreatic Cancer (SCALOP): A Multicentre, Randomised, Phase 2 Trial. Lancet Oncol. 2013, 14, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CN, H.; Falk, S.; Crosby, T.; McDonald, A.; Ray, R.; Joseph, G.; Staffurth, J.; RA, A.; Griffiths, G.; Maughan, T.; et al. Long-Term Results and Recurrence Patterns from SCALOP: A Phase II Randomised Trial of Gemcitabine- or Capecitabine-Based Chemoradiation for Locally Advanced Pancreatic Cancer. Br. J. Cancer 2017, 116, 1264–1270. [Google Scholar] [CrossRef]
- Su, Y.Y.; Chiu, Y.F.; Li, C.P.; Yang, S.H.; Lin, J.; Lin, S.J.; Chang, P.Y.; Chiang, N.J.; Shan, Y.S.; Ch’ang, H.J.; et al. A Phase II Randomised Trial of Induction Chemotherapy Followed by Concurrent Chemoradiotherapy in Locally Advanced Pancreatic Cancer: The Taiwan Cooperative Oncology Group T2212 Study. Br. J. Cancer 2022, 126, 1018–1026. [Google Scholar] [CrossRef]
- Fiore, M.; Ramella, S.; Valeri, S.; Caputo, D.; Floreno, B.; Trecca, P.; Trodella, L.E.; Trodella, L.; D’Angelillo, R.M.; Coppola, R. Phase II Study of Induction Chemotherapy Followed by Chemoradiotherapy in Patients with Borderline Resectable and Unresectable Locally Advanced Pancreatic Cancer. Sci. Rep. 2017, 7, 45845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.S.; Lim, J.H.; Kim, J.H.; Im, S.A.; Chie, E.K.; Hwang, J.H.; Kim, T.Y.; Bang, Y.J.; Ha, S.W.; Yoon, Y.B. Phase II Clinical Trial of Induction Chemotherapy with Fixed Dose Rate Gemcitabine and Cisplatin Followed by Concurrent Chemoradiotherapy with Capecitabine for Locally Advanced Pancreatic Cancer. Cancer Chemother. Pharmacol. 2012, 70, 381–389. [Google Scholar] [CrossRef]
- Sudo, K.; Hara, R.; Nakamura, K.; Kita, E.; Tsujimoto, A.; Yamaguchi, T. Phase II Study of Induction Gemcitabine and S-1 Followed by Chemoradiotherapy and Systemic Chemotherapy Using S-1 for Locally Advanced Pancreatic Cancer. Cancer Chemother. Pharmacol. 2017, 80, 195–202. [Google Scholar] [CrossRef]
- Ikeda, M.; Ioka, T.; Ito, Y.; Yonemoto, N.; Nagase, M.; Yamao, K.; Miyakawa, H.; Ishii, H.; Furuse, J.; Sato, K.; et al. A Multicenter Phase II Trial of S-1 with Concurrent Radiation Therapy for Locally Advanced Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 163–169. [Google Scholar] [CrossRef]
- Ioka, T.; Furuse, J.; Fukutomi, A.; Mizusawa, J.; Nakamura, S.; Hiraoka, N.; Ito, Y.; Katayama, H.; Ueno, M.; Ikeda, M.; et al. Randomized Phase II Study of Chemoradiotherapy with versus without Induction Chemotherapy for Locally Advanced Pancreatic Cancer: Japan Clinical Oncology Group Trial, JCOG1106. Jpn. J. Clin. Oncol. 2021, 51, 235–243. [Google Scholar] [CrossRef]
- Oh, E.S.; Kim, T.H.; Woo, S.M.; Lee, W.J.; Lee, J.H.; Youn, S.H.; Han, S.S.; Park, S.J.; Kim, D.Y. Effectiveness and Feasibility of Concurrent Chemoradiotherapy Using Simultaneous Integrated Boost-Intensity Modulated Radiotherapy with and without Induction Chemotherapy for Locally Advanced Pancreatic Cancer. Radiat. Oncol. J. 2018, 36, 200–209. [Google Scholar] [CrossRef] [Green Version]
- Quan, K.; Sutera, P.; Xu, K.; Bernard, M.E.; Burton, S.A.; Wegner, R.E.; Zeh, H.; Bahary, N.; Stoller, R.; Heron, D.E. Results of a Prospective Phase 2 Clinical Trial of Induction Gemcitabine/Capecitabine Followed by Stereotactic Ablative Radiation Therapy in Borderline Resectable or Locally Advanced Pancreatic Adenocarcinoma. Pract. Radiat. Oncol. 2018, 8, 95–106. [Google Scholar] [CrossRef]
- Zhu, X.; Cao, Y.; Lu, M.; Zhao, X.; Jiang, L.; Ye, Y.; Ju, X.; Zhang, H. Stereotactic Body Radiation Therapy with Sequential S-1 for Patients with Locally Advanced Pancreatic Cancer and Poor Performance Status: An Open-Label, Single-Arm, Phase 2 Trial. Radiother. Oncol. 2021, 162, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Moningi, S.; Dholakia, A.S.; Raman, S.P.; Blackford, A.; Cameron, J.L.; Le, D.T.; De Jesus-Acosta, A.M.C.; Hacker-Prietz, A.; Rosati, L.M.; Assadi, R.K.; et al. The Role of Stereotactic Body Radiation Therapy for Pancreatic Cancer: A Single-Institution Experience. Ann. Surg. Oncol. 2015, 22, 2352–2358. [Google Scholar] [CrossRef] [Green Version]
- Heerkens, H.D.; van Vulpen, M.; Erickson, B.; Reerink, O.; Intven, M.P.; van den Berg, C.A.; Molenaar, I.Q.; Vleggaar, F.P.; Meijer, G.J. MRI Guided Stereotactic Radiotherapy for Locally Advanced Pancreatic Cancer. Br. J. Radiol. 2018, 91, 20170563. [Google Scholar] [CrossRef] [PubMed]
- Comito, T.; Cozzi, L.; Clerici, E.; Franzese, C.; Tozzi, A.; Iftode, C.; Navarria, P.; D’Agostino, G.; Rimassa, L.; Carnaghi, C.; et al. Can Stereotactic Body Radiation Therapy Be a Viable and Efficient Therapeutic Option for Unresectable Locally Advanced Pancreatic Adenocarcinoma? Results of a Phase 2 Study. Technol. Cancer Res. Treat. 2017, 16, 295–301. [Google Scholar] [CrossRef]
- MA, T.; Loi, M.; Suker, M.; Falm, E.; van Eijck, C.H.J.; Nuyttens, J.J. A Phase II Study of Stereotactic Radiotherapy after FOLFIRINOX for Locally Advanced Pancreatic Cancer (LAPC-1 Trial): Long-Term Outcome. Radiother. Oncol. 2021, 155, 232–236. [Google Scholar] [CrossRef]
- Herman, J.M.; Chang, D.T.; Goodman, K.A.; Dholakia, A.S.; Raman, S.P.; Hacker-Prietz, A.; Iacobuzio-Donahue, C.A.; Griffith, M.E.; Pawlik, T.M.; Pai, J.S.; et al. Phase 2 Multi-Institutional Trial Evaluating Gemcitabine and Stereotactic Body Radiotherapy for Patients with Locally Advanced Unresectable Pancreatic Adenocarcinoma. Cancer 2015, 121, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Chuong, M.D.; Springett, G.M.; Freilich, J.M.; Park, C.K.; Weber, J.M.; Mellon, E.A.; Hodul, P.J.; Malafa, M.P.; Meredith, K.L.; Hoffe, S.E.; et al. Stereotactic Body Radiation Therapy for Locally Advanced and Borderline Resectable Pancreatic Cancer Is Effective and Well Tolerated. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 516–522. [Google Scholar] [CrossRef]
- Song, Y.; Yuan, Z.; Li, F.; Dong, Y.; Zhuang, H.; Wang, J.; Chen, H.; Wang, P. Analysis of Clinical Efficacy of CyberKnife(®) Treatment for Locally Advanced Pancreatic Cancer. Onco. Targets. Ther. 2015, 8, 1427–1431. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.-C.; Jen, Y.-M.; Li, M.-H.; Chao, H.-L.; Tsai, J.-T. Comparing Outcomes of Stereotactic Body Radiotherapy with Intensity-Modulated Radiotherapy for Patients with Locally Advanced Unresectable Pancreatic Cancer. Eur. J. Gastroenterol. Hepatol. 2015, 27, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Lee, W.J.; Woo, S.M.; Oh, E.S.; Youn, S.H.; Jang, H.Y.; Han, S.S.; Park, S.J.; Suh, Y.G.; Moon, S.H.; et al. Efficacy and Feasibility of Proton Beam Radiotherapy Using the Simultaneous Integrated Boost Technique for Locally Advanced Pancreatic Cancer. Sci. Rep. 2020, 10, 21712. [Google Scholar] [CrossRef] [PubMed]
- Terashima, K.; Demizu, Y.; Hashimoto, N.; Jin, D.; Mima, M.; Fujii, O.; Niwa, Y.; Takatori, K.; Kitajima, N.; Sirakawa, S.; et al. A Phase I/II Study of Gemcitabine-Concurrent Proton Radiotherapy for Locally Advanced Pancreatic Cancer without Distant Metastasis. Radiother. Oncol. 2012, 103, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Nichols, R.C.; George, T.J.; Zaiden, R.A.; Awad, Z.T.; Asbun, H.J.; Huh, S.; Ho, M.W.; Mendenhall, N.P.; Morris, C.G.; Hoppe, B.S. Proton Therapy with Concomitant Capecitabine for Pancreatic and Ampullary Cancers Is Associated with a Low Incidence of Gastrointestinal Toxicity. Acta Oncol. 2013, 52, 498–505. [Google Scholar] [CrossRef]
- Sachsman, S.; Nichols, R.C., Jr.; Morris, C.G.; Zaiden, R.; Johnson, E.A.; Awad, Z.; Bose, D.; Ho, M.W.; Huh, S.N.; Li, Z.; et al. Proton Therapy and Concomitant Capecitabine for Non-Metastatic Unresectable Pancreatic Adenocarcinoma. Int. J. Part. Ther. 2014, 1, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Ogura, Y.; Terashima, K.; Nanno, Y.; Park, S.; Suga, M.; Takahashi, D.; Matsuo, Y.; Sulaiman, N.S.; Tokumaru, S.; Okimoto, T.; et al. Factors Associated with Long-Term Survival in Gemcitabine-Concurrent Proton Radiotherapy for Non-Metastatic Locally Advanced Pancreatic Cancer: A Single-Center Retrospective Study. Radiat. Oncol. 2022, 17, 32. [Google Scholar] [CrossRef]
- Maemura, K.; Mataki, Y.; Kurahara, H.; Kawasaki, Y.; Iino, S.; Sakoda, M.; Ueno, S.; Arimura, T.; Higashi, R.; Yoshiura, T.; et al. Comparison of Proton Beam Radiotherapy and Hyper-Fractionated Accelerated Chemoradiotherapy for Locally Advanced Pancreatic Cancer. Pancreatology 2017, 17, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Chao, S.T.; Dad, L.K.; Dawson, L.A.; Desai, N.B.; Pacella, M.; Rengan, R.; Xiao, Y.; Yenice, K.M.; Rosenthal, S.A.; Hartford, A. ACR–ASTRO Practice Parameter for the Performance of Stereotactic Body Radiation Therapy. Am. J. Clin. Oncol. 2020, 43, 545–552. [Google Scholar] [CrossRef]
- Chang, D.T.; Schellenberg, D.; Shen, J.; Kim, J.; Goodman, K.A.; Fisher, G.A.; Ford, J.M.; Desser, T.; Quon, A.; Koong, A.C. Stereotactic Radiotherapy for Unresectable Adenocarcinoma of the Pancreas. Cancer 2009, 115, 665–672. [Google Scholar] [CrossRef]
- Hoyer, M.; Roed, H.; Sengelov, L.; Traberg, A.; Ohlhuis, L.; Pedersen, J.; Nellemann, H.; Berthelsen, A.K.; Eberholst, F.; Engelholm, S.A.; et al. Phase-II Study on Stereotactic Radiotherapy of Locally Advanced Pancreatic Carcinoma. Radiother. Oncol. 2005, 76, 48–53. [Google Scholar] [CrossRef]
- Paganetti, H. Relative Biological Effectiveness (RBE) Values for Proton Beam Therapy. Variations as a Function of Biological Endpoint, Dose, and Linear Energy Transfer. Phys. Med. Biol. 2014, 59, R419–R472. [Google Scholar] [CrossRef]
- Phillips, M.H.; Pedroni, E.; Blattmann, H.; Boehringer, T.; Coray, A.; Scheib, S. Effects of Respiratory Motion on Dose Uniformity with a Charged Particle Scanning Method. Phys. Med. Biol. 1992, 37, 223. [Google Scholar] [CrossRef] [PubMed]
- Henke, L.; Kashani, R.; Yang, D.; Zhao, T.; Green, O.; Olsen, L.; Rodriguez, V.; Wooten, H.O.; Li, H.H.; Hu, Y.; et al. Simulated Online Adaptive Magnetic Resonance-Guided Stereotactic Body Radiation Therapy for the Treatment of Oligometastatic Disease of the Abdomen and Central Thorax: Characterization of Potential Advantages. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 1078–1086. [Google Scholar] [CrossRef] [Green Version]
- Bohoudi, O.; Bruynzeel, A.M.E.; Senan, S.; Cuijpers, J.P.; Slotman, B.J.; Lagerwaard, F.J.; Palacios, M.A. Fast and Robust Online Adaptive Planning in Stereotactic MR-Guided Adaptive Radiation Therapy (SMART) for Pancreatic Cancer. Radiother. Oncol. 2017, 125, 439–444. [Google Scholar] [CrossRef]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; Faris, J.E.; Mellon, E.A.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. FOLFIRINOX for Locally Advanced Pancreatic Cancer: A Systematic Review and Patient-Level Meta-Analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnan, S.; Rana, V.; Janjan, N.A.; Varadhachary, G.R.; Abbruzzese, J.L.; Das, P.; Delclos, M.E.; Gould, M.S.; Evans, D.B.; Wolff, R.A.; et al. Induction Chemotherapy Selects Patients with Locally Advanced, Unresectable Pancreatic Cancer for Optimal Benefit from Consolidative Chemoradiation Therapy. Cancer 2007, 110, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the Pancreas: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26 (Suppl. S5), v56–v68. [Google Scholar] [CrossRef] [PubMed]

 ), SBRT (
), SBRT ( ), and proton beam therapy groups (
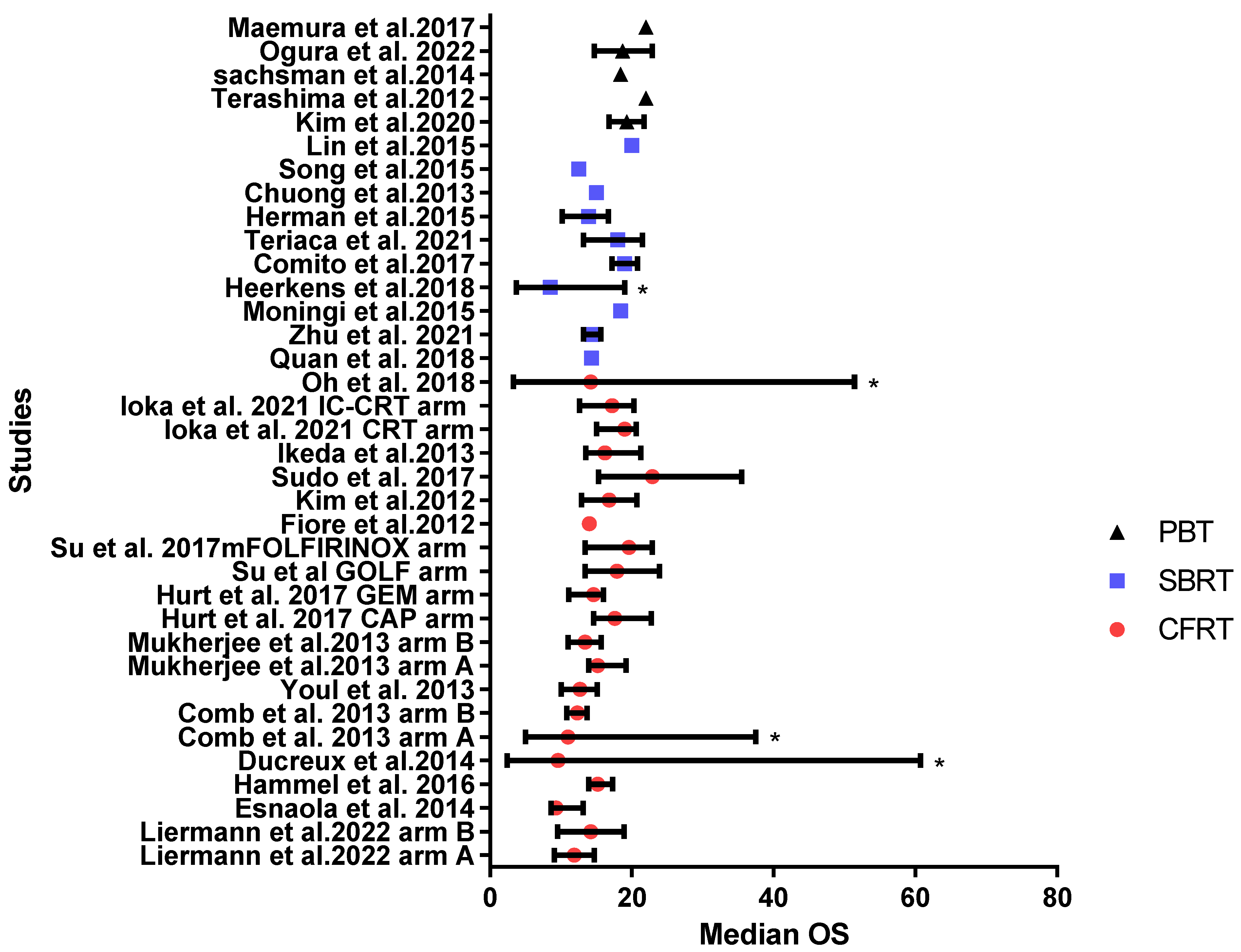
), and proton beam therapy groups ( ). Bars represent 95% CI or range (range marked by *) [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,45,46,47].
). Bars represent 95% CI or range (range marked by *) [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,45,46,47].

{kind=link}
{kind=link}
| Study | Study Type | N | Dose/Gy | Technique | Chemotherapy | Median OS, Months | 1-Year OS Rate, % | 2-Year OS Rate, % | Local Control | Acute G3/4 Toxicity | Late G3/4 Toxicity |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Liermann et al., 2022, arm A [17] | (Long-term results of phase II PARC trial) | 35 | 45 Gy/25 fractions with SIB to 54 Gy | IMRT | Concurrent gemcitabine/cetuximab followed by maintenance gemcitabine | 11.9 | 47% | 14.7% | 1-year LC rate approximately 65% (from figure) | G3 nausea: 4% G3/4 leucopenia: 37% G3/4 anemia: 14% | Not observed |
| Liermann et al., 2022, arm B [17] | (Long-term results of phase II PARC trial) | 33 | 45 Gy/25 fractions with SIB to 54 Gy | IMRT | Concurrent gemcitabine/cetuximab followed by maintenance gemcitabine/cetuximab | 14.2 | 60.6% | 27% | 1-year LC rate approximately 85% (from figure) | G3 nausea: 9% G3/4 leucopenia: 25% G3/4 anemia: 9% | G3 ileus: 3% G3 GIT Hge: 1% |
| Esnaola et al., 2014 [18] | Phase II | 19 | 45.9 Gy/30 fractions with SIB to 54 Gy | IMRT | Induction gemcitabine/oxaliplatin /cetuximab + concurrent capecitabine | 9.3 | NR | NR | 8.3% underwent R0 resection | Combined with BRPC patients | NR |
| Hammel et al., 2016, CRT arm [19] | Phase III | 133 | 54 Gy/30 fractions | 3DCRT | Concurrent capecitabine, either induction gemcitabine alone or gemcitabine + erlotinib followed by maintenance therapy | 15.2 | NR | NR | Loco-regional progression rate: 32% | Total hematological toxicity: 3.9% Total non-hematological toxicity: 23.1% | NR |
| Ducreux et al., 2014 [20] | Phase II | 51 | Median dose 54 Gy/30 fractions | 3DCRT | Concurrent docetaxel/cisplatin | 9.6 | 41% | NR | CR + PR: 27% SD: 51% PD: 14% (8% not evaluated) | GIT toxicity: 43% hematological toxicity: 8% | NR |
| Comb et al., 2013, arm A [21] | Phase II | 57 | A median total dose of 45 Gy/25 fractions with SIB to 54 Gy | IMRT | Concurrent and adjuvant gemcitabine | 11 | 36% | 8% | SD: 88% PD: 5% PR: 7% | Not observed | NR |
| Comb et al., 2013, arm B [21] | 198 | Median dose of 52.2 Gy/28 fractions | 3DCRT | Concurrent and adjuvant gemcitabine | 12.3 | NR | NR | SD: 80% PD: 11% PR: 9% | Not observed | NR | |
| Youl et al., 2013 [22] | Retrospective | 74 | Median total dose of 52.5 Gy/30 fractions | 3DCRT or IMRT | Induction and concurrent gemcitabine | 12.7 | 53.6% | 14.7% | SD: 60.8% PD: 22.9% | NR | NR |
| Mukherjee et al., 2013, capecitabine arm (SCALOP trial) [23] | Phase II | 36 | Median total dose of 50.4 Gy/28 fractions | 3DCRT or IMRT | Induction gemcitabine/capecitabine + concurrent capecitabine | 15.2 | 79.2% | NR | CR: 6% PR: 17% SD: 63% PD: 14% | Both hematological and non-hematological: 12% | NR |
| Mukherjee et al., 2013, gemcitabine arm (SCALOP trial) [23] | Phase II | 38 | Median total dose of 50.4 Gy/28 fractions | 3DCRT or IMRT | Induction gemcitabine/capecitabine + concurrent gemcitabine | 13.4 | 64.2% | NR | CR: 0% PR: 19% SD: 67% PD: 14% | Both hematological and non-hematological: 37% | NR |
| Hurt et al., 2017 [24] | (Long-term results of SCALOP trial) | Capecitabine arm: 17.6 Gemcitabine arm: 14.6 | |||||||||
| Su et al., 2022, GOLF arm [25] | Phase II | 17 | 50.4 Gy/28 fractions | IMRT | Induction GOLF followed by concurrent gemcitabine | 17.9 | 82.1% | 31.8% | PR: 24% SD: 65% PD: 11% | G3/4 leukopenia: 29.4% | NR |
| Su et al., 2022, mFOLFIRINOX arm [25] | Phase II | 21 | 50.4 Gy/28 fractions | IMRT | Induction m FOLFIRINOX followed by concurrent 5-FU | 19.6 | 88.9% | 29.6% | PR: 29%, SD: 33% PD: 38% | G3/4 leukopenia: 0% | NR |
| Fiore et al., 2017 [26] | Phase II | 27 | 59.4 Gy/33 fractions | 3DCRT | IC gemcitabine/oxaliplatin then concurrent gemcitabine | 14 | Combined with BRPC patients | Combined with BRPC patients | 40.7% became resectable | Combined with BRPC patients | NR |
| Kim et al., 2012 [27] | Phase II | 25 | Median total dose of 54 Gy/30 fractions | 3DCRT | Induction gemcitabine/cisplatin—concurrent capecitabine followed by gemcitabine | 16.8 | 69.1% | 16.1% | PD: 14.3% | G3 neutropenia: 4% G3 anemia: 4% G3 nausea/vomiting: 4% G3 diarrhea: 8% | NR |
| Sudo et al., 2017 [28] | Phase II | 23 | 50.4 Gy/28 fractions | 3DCRT | Induction gemcitabine/S1 then CRT with S1 followed by maintenance therapy with S1 | 22.9 | 82.6% | 43.5% | Significant reduction in tumor size (median size, from 41 to 32 mm) | G3 neutropenia: 4.3% G3 biliary tract infection: 8.7% | NR |
| Ikeda et al., 2013 [29] | Phase II | 53 | 50.4 Gy/28 fractions | 3DCRT | Concurrent S1 followed by maintenance S1 | 16.2 | 72% | 26% | PR: 27%, SD: 67% | G3 leukocytopenia: 10% G3 gastric ulcer: 2% | NR |
| Ioka et al., 2021, CRT arm [30] | Phase II | 50 | 50.4 Gy/28 fractions | 3DCRT | Concurrent S1 + maintenance gemcitabine | 19 | 66.7% | 36.9%, | NR | G3 leucopenia: 60% G3 anorexia: 16% G3 biliary infection: 18% | NR |
| Ioka et al., 2021, IC-CRT arm [30] | Phase II | 34 | 50.4 Gy/28 fractions | 3DCRT | Induction gemcitabine then CRT + maintenance gemcitabine | 17.2 | 69.3% | 18.9% | NR | G3 leucopenia: 59% G3 anorexia: 4% G3 biliary infection: 27% | NR |
| Oh et al., 2018 [31] | Retrospective | 47 | 44 Gy/22 fractions with SIB to 55 Gy | IMRT | Concurrent chemotherapy, with gemcitabine (n = 37) and capecitabine (n = 10) with or without induction chemotherapy | 14.2 | NR | NR | PR: 61.7% SD: 38.3% | G3 hematological toxicity: 12.8% G3 GIT toxicity: 2.1% | G3 anemia: 2.1% |
| Study | Study Type | N | Total Dose/Gy | Chemotherapy | Median OS, Months | 1-Year OS Rate, % | 2-Year OS Rate, % | Local Control | Acute G3/4 Toxicity | Late Toxicity |
|---|---|---|---|---|---|---|---|---|---|---|
| Quan et al., 2018 [32] | Phase II | 16 | 36 Gy/3 fractions | Induction gemcitabine/capecitabine ± adjuvant chemotherapy | 14.3 | 60% | 16% | m LPFS: 28.1 months 1-year LPFS rate: 78% 2-year LPFS rate: 52% | Not observed | NR |
| Zhu et al., 2021 [33] | Phase II | 63 | 35–40 Gy/5 fractions | Sequential S1 one month after SBRT | 14.4 | 73% | NR | Local recurrence rate: 15.9% regional recurrences: 30.2% | Total G3 toxicity: 14.3% | Total G3 toxicity: 4.8% |
| Moningi et al., 2015 [34] | Retrospective | Unresectable: 74 | 25–33 Gy/5 fractions | Different IC regimens followed by post SBRT chemotherapy | 18.4 | Reported combined with BRPC patients | Reported combined with BRPC patients | 15 patients underwent surgery, LPFS combined with BRPC patients | Reported combined with BRPC patients | reported combined with BRPC patients |
| Heerkens et al., 2018 [35] | Phase II | 20 | 24 Gy/3 fractions | ±Post SBRT gemcitabine/nab-paclitaxel or FOLFIRINOX | 8.5 | NR | NR | SD: 39% PD: 61% CR or PR: 0% | Not observed | Not observed |
| Comito et al., 2017 [36] | Phase II | 45 | 45 Gy/6 fractions | Pre or post SBRT different chemotherapy regimens | 19 months from diagnosis | 85% from diagnosis | 33% from diagnosis | m FFLP: 26 months | Not observed | Not observed |
| Teriaca et al., 2021 [37] | Phase II | 39 | 40 Gy/8 fractions | IC FOLFIRINOX | 18 | 77% | NR | 1-year LC rate: 80%, 3-year LC rate: 53% | Not observed | G3 toxicity or higher: 10% |
| Herman et al., 2015 [38] | Phase II | 49 | 33 Gy/5 fractions | Induction and post SBRT Gemcitabine | 13.9 | 59% | 18% | 1-year FFLP rate: 78% | G3 or more gastric ulcer: 2% G3 lymphopenia: 8.2% | G3 or more gastric ulcer: 6.4% |
| Chuong et al., 2013 [39] | Retrospective | 16 | 35–50 Gy/5 fractions | Induction gemcitabine followed by SBRT | 15 | 68.1% | NR | Surgical resection: 12.5% (other LC parameters were combined with BRPC) | Not observed | Total G3 toxicity: 5.3% |
| Song et al., 2015 [40] | Retrospective | 59 | Median total dose of 45 Gy/5 fractions | 90% of patients received chemotherapy before or after treatment | 12.5 | 53.9% | 35.1% | 1-year FFLP rate was 90.8% | Not observed | G3 GIT reaction: 1 patient |
| Lin et al., 2015, SBRT arm [41] | Retrospective | 20 | 35–45 Gy/5 fractions | Different concurrent chemotherapy regimens | 20 | 80% | NR | 1-year LDFS approximately 70% (from the figure) | Not observed | NR |
| Study | Study Type | N Patients | Total Dose Gy (RBE) | Technique | Chemotherapy | Median OS, Months | 1-Year OS Rate, % | 2-Year OS Rate, % | Local Control | Acute G3/4 Toxicity | Late G3/4 Toxicity |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kim et al., 2020 [42] | Retrospective | 81 | PTV1: 45 or 50 Gy PTV2: 30 Gy/10 fractions | Passive scattered proton beams | Upfront or maintenance chemotherapy or neither ± concurrent fluoropyrimidine chemotherapy | 19.3 | NR | NR | PR: 6.% SD: 80% PD: 14% | Not observed | Not observed |
| Terashima et al., 2012 [43] | Phase I/II | 5 | 50 Gy/25 fractions | NR | Concurrent and adjuvant gemcitabine | NR | NR | NR | NR | G3 leukopenia: 20% G3 neutropenia: 20% G3 fatigue: 20% G3 anorexia: 20% | NR |
| Terashima et al., 2012 [43] | Phase I/II | 5 | 70.2 Gy/26 fractions | NR | Concurrent and adjuvant gemcitabine | NR | NR | NR | NR | G3 leukopenia: 60% G3 neutropenia: 40% G3 anorexia: 20% | G3 GIT: 20% |
| Terashima et al., 2012 [43] | Phase I/II | 40 | 67.5 Gy/25 fractions | NR | Concurrent and adjuvant gemcitabine | NR | 78.8% | NR | 1-year FFLP: 79.9% | G3 hematological toxicity: 66% G4: 7.5%, G3 GIT toxicity: 21% | G3 anorexia: 3%, G3 gastric ulcer: 8% G3 fatigue: 3% G5 gastric ulcer: 3% |
| Terashima et al., 2012 [43] | Phase I/II | 50 | 50–70.2 Gy/ 25–26 | NR | Concurrent and adjuvant gemcitabine | 22 (from the curve) | 76.8% | NR | 1-year FFLP: 81.7% | ||
| Nichols et al., 2013 [44] | Prospective single institute | Unresectable: 12 | Medan dose 59.4 Gy/33 fractions | NR | Concurrent capecitabine | 8.8 | NR | NR | NR | Not observed | NR |
| Sachsman et al., 2014 [45] | Prospective single institute | 11 | 59.4 Gy/33 fractions | Passive scattering proton beams | Concomitant capecitabine | 18.4 | 61% | 31% | 1- and 2-year FFLP: 86% and 6% | Not observed | NR |
| Ogura et al., 2022 [46] | Retrospective | 123 | 67.5 Gy/25 fractions | NR | Concurrent and adjuvant gemcitabine | 18.7 | 70.4% | 35.7% | 1-year LPFS: 78.2% 2-year LPFS: 59% | All are hematological: G3: 42% G4: 2% | GIT toxicity: G3: 5% G4: 2% G5: 2% |
| Maemura et al., 2017, PT arm [47] | Prospective non-randomized | 10 | 50 Gy or 67.5 Gy/25 fractions | NR | IC followed by concurrent S1 + maintenance S1 | 22.3 | 80% | 45% | PR: 20% SD: 60% PD: 20% | One patient developed G3 ulcer | NR |
| Study | Major Domains | Minor Domains | |||||
|---|---|---|---|---|---|---|---|
| Selection of Participants | Clarification of Intervention | Measurements of Outcomes | Missing Data | Funding | Conflict of Interest | Overall | |
| Liermann et al., 2022 [17] |  | | | |  | | |
| Esnaola et al., 2014 [18] | | | |  | | | |
| Hammel et al., 2016 [19] | | | | | | | |
| Ducreux et al., 2014 [20] | | | | | | | |
| Comb et al., 2013 [21] | | | | | | | |
| Youl et al., 2013 [22] | | | | | | | |
| Mukherjee et al., 2013 [23] | | | | | | | |
| Hurt et al., 2017 [24] | | | | | | | |
| Su et al., 2022 [25] | | | | | | | |
| Fiore et al., 2017 [26] | | | | | | | |
| Kim et al., 2012 [27] | | | | | | | |
| Sudo et al., 2017 [28] | | | | | | | |
| Ikeda et al., 2013 [29] | | | | | | | |
| Ioka et al., 2021 [30] | | | | | | | |
| Oh et al., 2018 [31] | | | | | | | |
: Low risk; : High risk; : Unclear risk.| Study | Major Domains | Minor Domains | |||||
|---|---|---|---|---|---|---|---|
| Selection of Participants | Clarification of Intervention | Measurements of Outcomes | Missing Data | Funding | Conflict of Interest | Overall | |
| Quan et al., 2018 [32] | | | | | | | |
| Zhu et al., 2021 [33] | | | | | | | |
| Moningi et al., 2015 [34] | | | | | | | |
| Heerkens et al., 2018 [35] | | | | | | | |
| Comito et al., 2017 [36] | | | | | | | |
| Teriaca et al., 2021 [37] | | | | | | | |
| Herman et al., 2015 [38] | | | | | | | |
| Chuong et al., 2013 [39] | | | | | | | |
| Song et al., 2015 [40] | | | | | | | |
| Lin et al., 2015 [41] | | | | | | | |
: Low risk; : High risk; : Unclear risk.| Study | Major Domains | Minor Domains | |||||
|---|---|---|---|---|---|---|---|
| Selection of Participants | Clarification of Intervention | Measurements of Outcomes | Missing Data | Funding | Conflict of Interest | Overall | |
| Kim et al., 2020 [42] | | | | | | | |
| Terashima et al., 2012 [43] | | | | | | | |
| Nicolas et al., 2013 [44] | | | | | | | |
| Sachsman et al., 2014 [45] | | | | | | | |
| Ogura et al., 2022 [46] | | | | | | | |
| Maemura et al., 2017 [47] | | | | | | | |
: Low risk; : High risk; : Unclear risk.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elkhamisy, S.A.; Valentini, C.; Lattermann, A.; Radhakrishna, G.; Künzel, L.A.; Löck, S.; Troost, E.G.C. Normo- or Hypo-Fractionated Photon or Proton Radiotherapy in the Management of Locally Advanced Unresectable Pancreatic Cancer: A Systematic Review. Cancers 2023, 15, 3771. https://doi.org/10.3390/cancers15153771
Elkhamisy SA, Valentini C, Lattermann A, Radhakrishna G, Künzel LA, Löck S, Troost EGC. Normo- or Hypo-Fractionated Photon or Proton Radiotherapy in the Management of Locally Advanced Unresectable Pancreatic Cancer: A Systematic Review. Cancers. 2023; 15(15):3771. https://doi.org/10.3390/cancers15153771
Chicago/Turabian StyleElkhamisy, Sally A., Chiara Valentini, Annika Lattermann, Ganesh Radhakrishna, Luise A. Künzel, Steffen Löck, and Esther G. C. Troost. 2023. "Normo- or Hypo-Fractionated Photon or Proton Radiotherapy in the Management of Locally Advanced Unresectable Pancreatic Cancer: A Systematic Review" Cancers 15, no. 15: 3771. https://doi.org/10.3390/cancers15153771